Mary T. Dorritie, PhD
Mark Ruiz, Ph.D.
Objectives
Learn to obtain a client’s military service background
Understand the goals of military medicine
Understand the importance of rank and structure
Understanding the “Us vs. them” mentality
Identify important resources
OIF/OND: Fatalities = 4,491; Wounded= 32,243
OEF: Fatalities = 2,345; Wounded= 19,996
A caveat…
Although vets all share their service
and certain experiences in
common, there are distinct
differences between the services.
Today, you’ll be hearing things
mostly from the Army perspective.
Don’t be afraid to ask questions!
Most Vets/Troops will appreciate
your willingness to ask and NOT
ASSUME.
Afghanistan Parking Lot
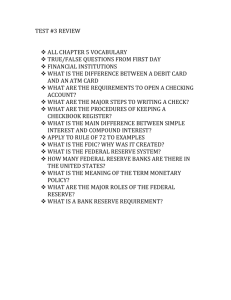
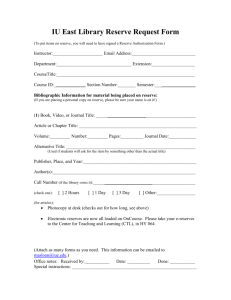
Military Structure
Department of
Defense (DOD)
(CINC PRESIDENT)
ARMY
Reserve
NAVY
Reserve
AIR FORCE
Reserve
National Guard
National Guard
(CINC Governor)
(CINC Governor)
MARINES
Reserve
COAST GUARD
Reserve
Rank & Structure
It’s all about DISCIPLINE
We know EXACTLY where and how we fit into the
organizational structure
Interchangeable parts
Your uniform is your resume
Normal tension between officers and enlisted
Role of the officer vs. role of the NCO and other enlisted
We call NCO’s the ‘backbone of the Army’
Many vets often choose post-military careers in law
enforcement, corrections, firefighting, EMT, etc.
Increased concerns about privacy due to employment.
Reality of Security Clearance procedures
“Us vs. Them”
Team work and “Esprit de corps”
Many vets, particularly combat vets, view themselves as different from civilians
If you fail to acknowledge this or ‘brush it aside,’ vet will typically write you off
Several reasons:
Perceived lack of discipline in civilian society/workplaces
Views on life and death, what’s important
“Mission first” mindset
Treatment many vets received from civilians upon redeployment
Lack of knowledge/awareness in civilians
“I didn’t realize we had people in Afghanistan.” “What is OIF?”
Insensitive questions, un-invited political commentary
“How many people did you kill.”
“We should stop using drones, they are killing too many civilians.”
Over concern from others
Tactical awareness versus Hyper-vigilance; Lethally armed versus Locked and Loaded
1 year re-adjustment period for every year deployed (Walter Reed Army Institute of Research)
Different (unofficial) norms for appropriate behavior within the military
“Us vs. Them” cont.
How do we deal with this when
working with Veterans?
Acknowledge it. If you’ve had a
family member in the military,
share that with the Vet.
Don’t pretend to
understand/know terminology,
tactics, ‘what it was like.’
ASK if you don’t know what
something means, Vets are usually
glad to explain.
The Military Family/Unit Cohesion
Traditional nuclear structure, but with
an increasing number of single parents,
dual military couples, and couples in
which the wife is the military member
Military member typically works long
hours- 8-hour days are almost unheard of
Non-military spouse bears most of the
childcare duties, attends school
functions, often takes care of financial
management (this is even more
pronounced during deployments)
Because of frequent PCS’ing, non-military
spouse often can’t find a job at each new
post
Kids tend to be pretty resilient, used to
moving and having to make new friends
Active vs. Guard/Reserve
Active- move around a lot, don’t get to stay with the same troops
for more than 2-3 years, usually.
Guard/Reserve- often serve with the same people for YEARS.
They get to know each other’s families, kids go to school
together, they may work in civilian jobs together, etc.
OEF/OIF – Largest mobilization of Guard/Reserve since WWII.
This is a primary reason that Active troops often view Guard/Reserve as
having “slack” discipline.
Variable discipline across units (line combat units vs. highly skilled medical units).
Typically older than active component.
Deployment differences- very different
homecomings/readjustment periods.
Increased rates of mental health problems between 3-12 months post
deployment (Milliken et al., 2007).
Military Medicine
“Mission First” vs. Patient Centered Treatment
Use of sick call
Lack of autonomy/Institutionalized mindset
Needs of the Army
Soldier Readiness Program (SRP)
Vaccinations
Lack of Confidentiality
Command’s “Need to Know”
The role of the Chaplain.
More accepted source of help.
Military History
What branch of service were you in?
What was your time in service (TIS)?
What was your MOS (the job you did)?
Level of security clearance
Confidential, Secret, Top Secret, TS-SCI
Types of Discharge (Form DD214)
Honorable
General
Other than honorable
Dishonorable/Bad Conduct
Character of discharge impacts access to benefits &
services.
Any Honorable discharge qualifies a veteran for many
services.
Military decorations (awards)
Congressional Medal of Honor
Purple Heart
Valor Awards–Examples-Silver Star, Navy Cross.
Military History cont.
Deployments and Associated Health Concerns
Combat
WWII – Cold injuries, chemical warfare experiments, exposure to nuclear weapons,
malnutrition and related ailments
Korea- Cold injuries, diabetes, peripheral vascular disease, malnutrition and related
ailments
Vietnam- Agent Orange exposure-www.va.gov/agentorange, PTSD, Hepatitis C
Desert Shield/Desert Storm (Saudi Arabia/Kuwait/Iraq)- Depleted Uranium, chemical
and biological agent exposure, leishmaniasis
OEF (Operating Enduring Freedom- Afghanistan)
OIF (Operation Iraqi Freedom)
OND (Operation New Dawn- as we were leaving Iraq)
For all of these- PTSD, Traumatic Brain Injury (TBI), blast exposure, amputations,
exposure to burn pits, orthopedic injuries from carrying heavy gear
Peacekeeping- not a large body of research on health effects of these operations
Bosnia/Kosovo
Somalia
Hurricane Katrina
West Africa (fight against Ebola)
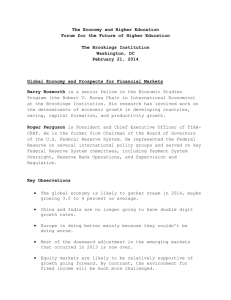
Resources for Signature Conditions
• VA Trauma Recovery Clinic
• VA Post-Deployment Clinic
• PTSD Residential Treatment
(Bay Pines, Miami)
• Vet Centers
• VA Women’s Center
• Trauma Recovery
Clinic
• Residential MST
program (Bay Pines)
Post
Traumatic
Stress
Disorder
(PTSD)
Substance
Abuse
• ADATP program
(Tampa)
• SARRTP (Bay Pines,
Miami, Gainesville,
Orlando)
Military
Sexual
Trauma
(MST)
Traumatic
Brain Injury
(TBI)
• VA Polytrauma
Treatment and
Rehabilitation.
• SCI
Increased rates of mental health problems between 3-12
months after deployment (Milliken et al., 2007).
Conclusion
Military society is its own subculture.
There are norms and mores that differ from
those of civilian society, often leading
military members and families to feel like
they ‘don’t belong.’
Few people in our country have a direct
connection to the military.
Military is becoming increasingly diverse
and offers opportunities to excel for anyone
with the skills and drive necessary,
regardless of race, gender, or ethnicity.
Important resources:
http://www.ebenefits.va.gov
http://www.va.gov
http://www.tampa.va.gov
Further training
http://www.deploymentpsych.org/military-culture
This is a FREE online training developed jointly by VA
and DoD.
4 modules, 2 CE’s each (again, FOR FREE!)
Questions?
 0
0