RENAL DISEASES
advertisement

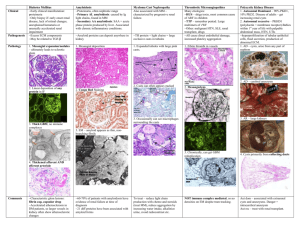
Renal Diseases Renal cysts and Tumors CYSTIC DISEASES OF THE KIDNEY Fluid filled spaces within the kidney May involve cortex or medulla or both May be unilateral or bilateral May be unilocular or multilocular May be congenital or acquired May be sporadic or genetically determined Clinical significance may be trivial or grave CLASSIFICATIONS OF RENAL CYSTIC DISEASES Polycystic kidney diseases: 1. Autosomal recessive (ARPKD) classic infantile polycystic disease with congenital hepatic fibrosis 2. Autosomal dominant (ADPKD) Simple renal cysts Acquired renal cystic disease Autosomal Recessive Polycystic Kidney Disease ( ARPKD ) Rare, 1:6-14000 live births Abnormal gene located on chromosome 6p21 May be still born or neonatal death due to pulmonary insufficiency Progressive renal failure Low specific gravity, mild proteinuria, urine concentrating defect, anemia, hypertension CCF Bilaterally symmetrical enlargement of kidneys Smooth surface with innumerable 1-2 mm cysts Diffuse fusiform dilatation of the collecting ducts ARPKD ( Cont. ) Enlarged but normally shaped pelvi-calyceal system Normal reniform shape complete with fetal lobation & normal sized (undilated) ureter Normal glomeruli and tubules Normal interstitium and no dysplasia Congenital hepatic fibrosis is almost always present Normal numbers of nephrons, no interstitial fibrosis and no dysplasia Autosomal Dominant Polycystic Kidney Disease (ADPKD ) World wide, 1:1000 in general population Accounting for 6% of patients in dialysis and transplant program Abnormal gene on short arm of chromosome 16 i.e. 16p13.3(PKD-1). 4q12-22(PKD-2), 3rd locus found Present in 3rd-5th decade Dull loin pain, flank masses. azotemia, positive family history, hypertension, hematuria, colic etc. Prograssive renal failure anemia & GFR, Ur & Cr ADPKD (CONT.) Associated cysts in liver of biliary type, in pancreas (10%), spleen,thyroid & seminal vesicle Vascular anomalies including Berry aneurysms(33%), aortic aneurysm, aortic root dilatation and mitral valve prolapse Diverticular disease of the colon (80%) ADPKD- Pathological Features Bilaterally enlarged kidneys (up to 4000 gms) Diffuse cystic (1-2% cystic nephrons) change with uninvolved intervening parenchyma Varying sized, numerous to innumerable generally spherical unilocular cysts, distributed in cortex and medulla obscuring normal reniform shape and corticomedullary junction, containing yellowish to turbid to brown to black colored fluid Distorted pelvi-calyceal system Cysts arising from any part of nephron or collecting duct ADPKD- PATHOLOGICAL FEATURES Cysts lined by single layer of cuboidal epithelium Neoplastic change - uncommon Simple Renal Cysts Extremely common as age advances Incompletely understood pathogenesis Commonly associated with scarred kidneys Asymptomatic with normal renal function May be solitary/multiple/unilateral/bilateral Generally unilocular, round to oval of varying sizes SIMPLE RENAL CYSTS (Cont.) Arises as dilated tubules or collecting ducts Thin, translucent fibrous wall containing clear or amber colored serous fluid ACQUIRED RENAL CYSTIC DISEASE Secondary to end-stage renal disease as well as prolonged dialysis ( 9 months -7 yrs.) Kidneys are generally small but may be normal or even enlarged Common in cortex Seems to be arising in either proximal or distal tubules Neoplastic change are common RENAL TUMOURS In infants and children : • Nephroblastoma ( Wilms’ tumour ) In adults : • Renal cell carcinoma • Renal cell adenoma • Renal oncocytoma NEPHROBLASTOMA ( Wilms’ tumour ) Embryonal tumour arising from nephrogenic blastemal cells • can differentiate in to several cell lines - blastemal, epithelial and stromal • many replicate developing kidneys Common in young children / uncommon in neonates and infants 90% in < 6yrs. old ( mean: 3yrs. in boys and 3.5yrs. in girls ) NEPHROBLASTOMA Etiology and Pathogenesis Generally unknown World wide i.e. … No environmental factors Variable incidence in racial groups : • blacks> whites> Orientals Familial tendencies: 1% autosomal dominant with variable penetrance & expressivity Genetic predispositions • WT-1 gene (11p13); WT-2 gene (11p15.5) NEPHROBLASTOMA Clinical Features Most common genitourinary cancer Age: 1-3yrs., 98% in <10yrs Abdominal mass, pain, & hematuria Usually unicentric, may be multicentric (7%) or bilateral (5%) Imaging technique to reveal smaller lesions No specific tumor markers identified NEPHROBLASTOMA Pathologic findings (gross) Usually solitary, sharply (well) defined masses with pseudocapsule Variable size & weight (60-6350 gms. with a mean of 550 gms.) Uniform, pale gray to tan, divided by prominent fibrous septa in to lobules May be cystic, hemorrhagic or necrotic No specific location NEPHROBLASTOMA Microscopic findings Generally triphasic pattern : • blastemal, epithelial and stromal cell type may contains heterologous elements “favorable” or “unfavorable” histology on the bases of nuclear anaplasia i.e. . . . • marked nuclear enlargement (3x) • abnormal mitoses i.e. . . . increased DNA NEPHROBLASTOMA - Spread Local Regional Distant • lungs • liver : i.e. . . lymphatic NEPHROBLASTOMA prognosis and treatment Depends upon : • stage, age and histology Surgery with chemotherapy for : • stage I & II with favorable histology • surgery with chemotherapy and radiotherapy for higher stages and unfavorable histology RENAL CELL CARCINOMA Hypernephroma / Grawitz’s tumour 3% of all adult malignancies world wide, no racial predispositions M:F = 1.6:1, 6th decade (mean 55 yrs) seems to be arising from mature renal tubules tobacco - smoked / chewed RENAL CELL CARCINOMA ( Cont. ) Chromosomal abnormalities : • 3p13 - clear or granular cell type • trisomy 17/ tri-or tetrasomy 7 - papillary type Rare familial association Associated with acquired cysts and / or in patients on chronic hemodialysis RENAL CELL CARCINOMA Clinical Features & Diagnosis classic triad : • hematuria, flank pain and abdominal mass may be clinically occult, 30% presents with metastatic lesion Polycythemia due to erythropoietin constitutional symptoms imaging techniques - useful RENAL CELL CARCINOMA mode of dissemination Direct extension Vascular Lymphatic Lungs, lymph nodes, liver, bone brain, skin etc. RENAL CELL CARCINOMA prognosis Influenced by multiple factors : • tumour size • infiltrative margins • histological type • tumour stage - most important Can be expressed in terms of histological types RENAL CELL ADENOMA Incidental findings at autopsy (22%) Well demarcated, unencapsulated Pale yellow-gray, discrete cortical mass Up to 2 cms. in maximum dimension