treating ex-offenders: barriers to treatment
advertisement

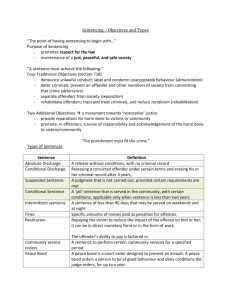
Treating Ex-offenders: Barriers to Treatment Tom Granucci, LCSW Supervisory U. S. Probation Officer United States District Court Central District of California & Peter Getoff, LCSW Supervising Psychiatric Social Worker California Department of Corrections and Rehabilitation Parole Outpatient Clinic Today’s Workshop • Overview of USPO and CDCR POC • Current Data on: • • The offender population • Mentally ill offenders • Substance Abuse in the offender population • COD in the offender population Trends in community supervision of offenders Today’s Workshop • Barriers to Treatment for Offenders: • Offender Characteristics • Lack of Motivated and Qualified Providers • Evidence-based practice in: • • • Mental Health, Substance Abuse, Co-occurring Disorders, and Correctional Treatment Underfunded Public Mental Health System Collaboration: Integrated Treatment and Community Corrections U.S. Probation • Established by Congress in 1925 • 94 Federal Districts • Central District of California • 7 Counties: Los Angeles, Orange, Riverside, San Bernardino, Ventura, Santa Barbara, San Luis Obispo CD-CA • 12 Field Offices, 120 Supervision Officers, 40 Pre-sentence Officers, 3 Federal Courthouses • Crimes: Bank Robbery, Drug Trafficking, Credit Card Fraud,White Collar Fraud, Cyber Crime, Sex Offenses • Diversity of Offenders Caseload/workload • General Caseloads = 55-65 • Drug Specialists = 45 • MH Specialists = 35-40 • Sex Offender Specialists = 25 U.S. Probation Goals • Provide objective, verified information and recommendations to assist the court in making fair decisions • Ensure offender compliance with court-ordered conditions through community-based supervision and partnerships • Protect the community through the use of controlling and correctional strategies designed to assess and manage risk • Facilitate long-term, positive changes in offenders through proactive interventions • Promote the fair, impartial, and just treatment of offenders U.S. Probation Values • Integrity • Effective stewards of public resources • Treat everyone with dignity and respect • Fairness in process and excellence in service • Work together to foster a collegial environment • Responsible and accountable • Parole abolished November 1, 1987 • Supervised Release (76%) • Probation (22%) • Parole (<2%) • Military Parole (<1%) • Conditional Release (<1%) • Federal Law Enforcement Officers and Officers of the Court Reentry • in 2001, 1,600 state and federal prisoners released per day • Residential Reentry Centers (RRCs) California Department of Corrections and Rehabilitation • State prison population is 174,000 felons • California: one of the highest recidivism rates in the country • 70% within 3 years • Average yearly cost: $35,587 per inmate; $4,338 per parolee • 33 state prisons California Department of Corrections and Rehabilitation • Los Angeles County - 40,000 parolees • Largest population of all counties • 125,000 parolees statewide Parole Outpatient Clinic POC • 1954: Established by the California Department of Corrections • To assist parolees with mental health problems • To reduce recidivism POC • Caseloads: 80-200 POC Outcomes • UCLA Integrated Substance Abuse Program contracted by CDCR to conduct program evaluation • The greater # of contacts a parolee has with clinic clinicians, the less likely to be returned to prison • 17.4% of parolees with at least 9 POC contacts recidivated within 12 months vs. 70.6% of parolees w/ no POC contact Co-occurring Disorders at the POC • Estimated at 75-85% at Region III’s POC Reentry • Dr. Joan Petersilia proponent of prisoner reentry programs but only where practitioners and researchers work together to create services, both clinically and administratively effective The Offender Population The Numbers • At midyear 2006: One in every 133 U.S. residents in prison or jail National State & Federal Prison Population Mentally Ill Offenders The Numbers • “There are three kinds of lies: lies, damned lies, and statistics” (Benjamin Disraeli) The Numbers • 7% of Federal Inmates • 16% in state prisons, local jails, and on probation Department of Justice, Bureau of Justice Statistics, 1999 More Numbers • DOJ, BJS 2006: 50% • Change in Methodology • Our current MH = 17% Mental Illness in the Forensic Population • Psychotic Disorders and Major Depression 2-4x more common than in the general population Personality Disorders in the Forensic Population • Anti-social personality disorder 10x more common than in the general population Substance Abuse in the Forensic Population • Across studies: 55% - 72% Co-occurring Disorders The Numbers • General MH Population: 20-80% of severely mentally ill abusing substances • Substance abuse treatment: 30-70% of addicts have a mental disorder Co-occurring Disorders Forensic Numbers • Across studies: 56% - 75% (85% for alcohol) Trends Our Numbers • MH doubled from 2000 to 2004 • Drug cases = 57% • Co-Occurring = > 70%? More Trends • More Sex Offenders: Internet Child Pornography and Lurers/Travelers More Trends • More High Risk • Axis I: Clinical Disorders, especially Psychotic Disorders and Mood Disorders + • Axis I: Substance Abuse/Dependence + • Axis II: Personality Disorders, especially Borderline, Narcissistic, and Antisocial My Forensic Formula • Axis I + Axis II + Substance Abuse = Trouble Our Response: Specialized Caseloads • Mental Health and Sex Offenders in 2000 • Further Specialization of Sex Offenders in 2007 Specialized Caseloads • Council of State Governments, Criminal Justice/Mental Health Consensus Project in 2002 www.consensusproject.org Specialty vs. Traditional Agencies • Specialized Caseloads • Reduced Caseloads • Sustained Officer Training • Integration of Internal and External Resources • Problem Solving vs. Traditional Barriers to Treatment The First Problem: The Offender Recidivism: Are they really “ex”? • From Inmate to Offender to Inmate? • Numbers are Frightening and Depressing: 50-70% Recidivism within 3 years; 70% in California or • From Inmate to Offender to Ex-Offender: Law-abiding, drug free, productive, tax-paying citizen • Federal Supervision Numbers: 70% Succeeded, 30% Revoked • Why? Speculation, no data. • Low risk/rehabilitation of some offenders • Sophistication of other offenders Outcomes • My Snapshot: January 2007 September 2007 n=13 • 31% Successful without violations • 38% Revoked (1 for technical violations; 2 for drug use; 2 for new criminal conduct) • 31% Violations without revocation • 62% Overall success rate Mental Illness and Supervision Failure • Research indicates mentally ill offenders are more likely to fail on supervision • In my experience, due to substance abuse and new criminal conduct; not due to mental illness or mental health noncompliance Outcomes • My Officers’ Snapshot: October 1, 2007 - January 14, 2008 • n= 33 • 55% Successful without violations • 27% Revoked (1 for technical violations; 3 for drug use; 5 for new criminal conduct) • 18% Violations without revocation • 73% Overall success rate Characteristics of the Forensic MH Population • Mandated/Involuntary = Unmotivated • Deceptive • Criminal Lifestyle • Dangerousness • Substance Abuse • Co-occurring Disorders PLUS Antisocial Personality Disorder and/or Psychopathy Motivation: Stages of Change • Pre-contemplation • Contemplation • Determination • Action • Maintenance • Relapse Motivation • A lot of precontemplation going on! Motivation • My version of motivational interviewing: Prison or residential treatment? • Move directly from precontemplation to action. • Research: Drug treatment outcomes as good for mandated clients as voluntary clients The Second Barrier: The Providers • Lack of Integrated Co-Occurring Disorders Treatment and Lack of Qualified Forensic Mental Health Providers: Motivation, Training, and Experience History of MH Treatment vs. SA Treatment • Two separate programs in the public health system • Separate, unequal funding sources • Treatment by providers with two different training backgrounds and treatment philosophies • Treatment provided in two separate places History of MH Treatment vs. SA Treatment • MH Diagnosis Primary vs. SA Dx Primary • MH accepts limited recovery vs. SA: recovery and lifetime abstinence always possible • MH: Medication accepted vs. SA: Clean and Sober required. • MH: Supportive and Non-Directive vs. SA: Confrontive History of MH Treatment vs. SA Treatment • MH: Professionals only vs. SA: Recovering clients and professionals • MH: Scientific and process oriented vs. SA: Spiritual and outcome oriented • MH: Prevent decompensation vs. SA: Hitting bottom OK Untreated Co-occurring Disorders • In 2002, 52% of adults with cooccurring disorders did not receive mental health treatment or substance abuse treatment. • Of the 48% who received treatment: • 34% received MH treatment only • 2% received SA treatment only • 12% received both MH and SA treatment Treatment of Co-occurring Disorders • “The more things change, the more they remain the same” Jean-Baptiste Alphonse Karr, 1849 • "Those who cannot remember the past are condemned to repeat it." George Santayana, 1905 Treatment of Co-occurring Disorders • Attitudinal Change: MH vs. SA providers and vice versa • On MH side: Starts in the professional schools Forensic MH: Shortage of Motivated Providers • Professional Prejudice • Resistance to change = untreatable • “Undignified” target population • Countertransference • Fear Forensic MH: Shortage of Qualified Providers • Cross Training: MH-SA; SA-MH and Forensic • Basic Competence and Teams Evidenced-Based Practice • Best Practices • What Works • EBP What Works in Mental Health Treatment • The Relationship • Cognitive Behavioral • Medication • Assertive Community Treatment (ACT) Models What Works in Substance Abuse Treatment • Motivational Interviewing • Cognitive-behavioral treatment: relapse prevention • Contingency Management • The Matrix Model • Medication • 90 days minimum effective dose What Works for Co-occurring Disorders • Integrated Treatment = • Co-located • Cross trained staff • Adequate staffing: low staff to client ratios for intensive case management (ACT model) • Individualized screening • Flexible • Peer support • Comprehensive services: housing, employment, HIV/AIDS, Hepatitis EBP in Correctional Treatment • Risk Principle • Needs Principle • Responsivity Principle EBP in Correctional Treatment • Any other treatment is “correctional quackery” Dynamic Risk Factors Criminogenic Needs • Antisocial Attitudes • Antisocial Associations • Antisocial Personality • Substance Abuse • Lack of Empathy • Low Self-Control/Impulsive Behavior • Dysfunctional Family Ties • Employment/Education EBP for Treating Offenders • Cognitive-Behavioral Curriculum-Based Group Therapy • Examples: Thinking For a Change (T4C) www.nicic.org and Moral Reconation Therapy (MRT) www. moral-reconation-therapy.com Evidence-Influenced Treatment • Address Instant Offense and Criminal History • Confront Anti-social Attitudes • Eliminate/reduce Anti-social Associations • Encourage Pro-social thinking and behavior • Abstinence from alcohol and drugs • Develop/increase empathy • Eliminate/decrease impulsive behavior • Develop/improve life skills Co-occurring Disorders Treatment at the POC • Reality • Dynamic • Cognitive-behavioral • Medication management • Interactional • Integrated team approach • Parole and Residential Treatment Therapeutic Confrontation • Effectiveness • Timing • Empathy • Feedback, not judgement Common Defense Mechanisms of Offenders • Denial Common Defense Mechanisms of Offenders • Rationalization Common Defense Mechanisms of Offenders • Minimization Common Defense Mechanisms of Offenders • Projection • Sorry, no cartoon. What Does Not Work with Offenders • Non-Directive • Targeting Self-Esteem Sex Offender Specific Treatment • Note: Even fewer qualified specialists in sex offender treatment The Third Barrier: Limited Public Mental Health Resources • State and Federal policy is to use community resources Collaboration • Non-contracted: AB2034 Criteria: • Serious Mental Illness • Homeless • At risk of homelessness or incarceration Current Collaborations • Contracted: Residential Co-Occurring Disorders Treatment: Tarzana Treatment Centers and BHS/Pacifica House • Non-Contracted: DMH The Case for Collaboration • Mutual Clients: • Offenders are in the community • Severely Mentally Ill • Have SSI or SSI Eligible = Medi-Cal The Case for Collaboration • State and Federal have gaps in continuum of care; public mental health has a full continuum of care. • Clients will require mental health/substance abuse services beyond the period of supervision. Future Collaborations • Full Service Partnerships (FSPs) • Criteria: • Homeless • Criminal Justice contact • Frequent utilization Future Collaborations • Staff training in forensic mental health needed Moving Forward • If cannot co-locate, then collaborate • Regional collaborations: mental health, substance abuse, and community corrections References • Berman, G., Bowen, P., and Mansky, A. (2007). Trial and Error: Failure and Innovation in Criminal Justice Reform. Executive Exchange, Summer 2007. • Best, J.. Damned lies and statistics: untangling numbers from the media, politicians, and activists (2001). University of California Press, Berkeley and Los Angeles, California. • Center for Substance Abuse Treatment. Substance Abuse Treatment for Persons With CoOccurring Disorders. Treatment Improvement Protocol (TIP) Series 42. DHHS Publication No. (SMA) 05-3992. Rockville, MD: Substance Abuse and Mental Health Services Administration, 2005. • Cohen, W. and Inaba, D. (1991). The Haight-Ashbury Training Series. Volume IV. Dual Diagnosis. The Mentally Ill Drug Abuser. Training Manual. CNS Productions. • DeMichelle, M. (2007). Probation and Parole’s Growing Caseloads and Workload Allocation: Strategies For Managerial Decision Making. The American Probation and Parole Association. • Ditton, P. M. (1999). U. S. Department of Justice, Office of Justice Programs. Bureau of Justice Statistics Special Report. Mental Health and Treatment of Inmates and Probationers. References • Dual Diagnosis: Part I. The Harvard Mental Health Letter, Volume 20, Number 2, August 2003. • Fazel, S. and Danesh, J. (2002). Serious Mental Illness in 23,000 Prisoners: A Systematic Review of 62 Surveys. The Lancet; 359(9306):545-550. • Flores, A. W., Russell, A. L., Latessa, E. J., and Travis III, L. F. (December 2005). Evidence of Professionalism or Quackery: Measuring Practitioner Awareness of Risk/Need Factors and Effective Treatment Strategies. Federal Probation. • Hills, H. A. (March 2000). Creating Effective Treatment Programs for Persons with CoOccurring Disorders in the Justice System. The National GAINS Center for People with CoOccurring Disorders in the Justice System. • Latessa, E. J. and Lowenkamp, C., What are Criminogenic Needs and Why are they Important? Community Corrections: Research and Best Practices, Ohio Judicial Conference, For the Record, 4th Quarter 2005. • James, D. J. and Glaze, L. E. (2006). U. S. Department of Justice, Office of Justice Programs. Bureau of Justice Statistics Special Report. Mental Health and Treatment of Inmates and Probationers References • Latessa, E. J. (1999). What Works in Correctional Treatment, Southern Illinois University Law Journal Volume 23. • Massaro, J. (2004). Working with People with Mental Illness Involved in the Criminal Justice System: What Mental Health Service Providers Need to Know (2nd ed.). Delmar, NY: Technical Assistance and Policy Analysis Center for Jail Diversion. • Mendel, P. and Fuentes, S. (December 2006). Partnering for Mental Health and Substance Needs in Los Angeles: A Community Feedback Report. Summary of the Community Feedback Conference for the Health Care for Communities Partnership Initiative, Los Angeles, July 7, 2006. • National Institute on Drug Abuse. NIDA Notes, Court-Mandated Treatment Works as Well as Voluntary, Vol. 20, No 6. (July 2006) • National Institute on Drug Abuse. Principles of Drug Abuse Treatment for Criminal Justice Populations. A Research-Based Guide. NIH Publication No. 06-5316. July 2006. • Peck, J. A. (June 8, 2007). Evidence-Based Interventions for Substance Abuse. Advances in Addiction Treatment: Theory, Research, and Practice Conference, Bel Air, CA. References • Petersilia, J. (2003). When Prisoners Come Home: Parole and Prisoner Reentry (Studies in Crime and Public Policy). Oxford University Press, New York, New York. • Peters, R. H., Hills, H. A. Intervention Strategies for Offenders with Co-Occurring Disorders: What Works? The National GAINS Center for People with Co-Occurring Disorders in the Justice System. December 1997 • Public Safety Performance Project. A Project of the Pew Charitable Trusts. www.pewpublicsafety.org. 2007 • Sabol, W. J. and Harrison, P.M. (2007). U. S. Department of Justice, Office of Justice Programs. Bureau of Justice Statistics Bulletin. Prison and Jail Inmates at Midyear 2006. • Skeem, J. L. and Louden, J. E. (March 2006). Toward Evidence-Based Practice for Probationers and Parolees Mandated to Mental Health Treatment. Psychiatric Services, Vol. 57 No. 3 • Skeem, J. L., Monahan, J., and Mulvey, E. P. (December 2002). Psychopathy, Treatment Involvement, and Subsequent Violence Among Civil Psychiatric Patients. Law and Human Behavior, Vol. 26, No. 6. References • Taxman, F., Shephardson, E., & Byrne, J. (2004). Tools of the Trade: A Guide to Incorporating Science into Practice. National Institute of Corrections, U. S. Department of Justice, Office of Justice Programs. • Travis, J., Solomon A. L., and Waul, M. (2001). From Prison to Home - The Dimensions and Consequences of Prisoner Reentry. Urban Institute. • U. S. Department of Health and Human Services, Substance Abuse and Mental Health Services Administration (SAMHSA), Report to Congress on the Prevention and Treatment of Co-Occurring Substance Abuse Disorders and Mental Disorders, November 2002. • U. S. Department of Health and Human Services, Office of Applied Studies, Substance Abuse and Mental Health Services Administration (SAMHSA) (June 2004). The National Survey on Drug Use and Health Report. Adults with Co-Occurring Serious Mental Illness and a Substance Use Disorder. • U. S. Department of Justice, National Institute of Corrections. Crime & Justice Institute (April 2004). Implementing Evidence-Based Practices in Community Corrections: The Principles of Effective Intervention.