Adrenal Gland diagram
advertisement

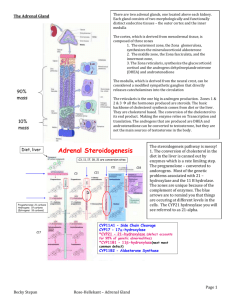
1 Adrenal Gland diagram Adam Bein 1/22/2014 6:02 PM 1) Zona Glomerulosa 2) Zona Fasciculata ACTH from the Ant. Pit. goes to here when stimulated by fasting or exercise. This stims the rel. of Cortisol/ Hydrocortisone. 3) Zona Reticularis Disorder: Etiology: S/S: Tests: Interventions: Nursing: Adrenal Gland Adrenal Cortex Secretes steroid hormones: 1) ‘Mineralocorticoids’ (Aldosterone) which reg. minerals & energy. 2) ‘Glucocorticoids’ (Cortisol/ Hydrocortisone) which reg. metabolism of glucose, 3) Androgens. Mineralocorticoids. Aldosterone: 1) It’s target organ is the kidney. It is the most abundant mineralocorticoid. 2) Regulates: Na & K (stimulates reabsorbtion of Na and excreation of K in the kidney’s distal tubule). 3) As Na is reabsorbed, H is excreted. This l/t alkalosis/less acidosis/prevention of acidosis. 4) As Na is reabsorbed, bicarb follows too. 5) Aldosterone release is stim. by: 1) Low blood Na lvl. 2) High blood K lvls. 3) Lower BP (d/t loss of blood or dehydration) 1) Low BP activates RAA in the kids l/t Angiotensin II l/t increased secretion of aldosterone. 6) Aldosterone non-release: When BP rises the atria secretes ANP. That inhibits the rel. of aldosterone (renin) l/t the kids elim. Na l/t water following the Na, l/t BP going down. Glucocorticoids. Cortisol/Hydrocortisone: Is the most abundant ot Glucocorticoids. It stims. glucogenesis (the conversion of secondary energy sources to glucose). Cortisol/Hydrocortisone: 1) Stims metabolism of carbs. 2) Regs glucose metabolism. 3) Inhibits the immune system (synthetic cortisol/steroids are given to trt inflammation & organ rejection). 4) Is secreted in diurnal rhythm (more in the early a.m.). 5) Is secreted during times of stress. Hypersecretion of Cortisol/Hydrocortisone manifests as ‘Cushing Syndrome’. Hyposecretion of Cortisol/Hydrocortisone manifests as ‘Addison’s Disease’. Gender steroids/androgens. Make precursors of testosterone and estrogen & supplement the gonads’ release of their hormones. No zones Adrenal Medulla Secrete the Catacholamine hormones (they help the SNS) Epinepherine & Norepinephrine. Epinepherine (stims metabolism of carbs.) & Norepinephrine. Hypersecretion: S/S of typical SNS stim. Hypersecretion d/t a tumor. Called ‘Pheochromocytoma’. Hyposecretion: Rare. Increased Epinepherine & Norepinephrine: 1) Are in a ratio of 4:1 Hypersecretion of Cortisol/Hydrocortisone manifests as ‘Cushing Hyposecretion of Cortisol/Hydrocortisone, Aldosterone, or both manifests as Hypersecretion of Epinepherine & Norepinepherine d/t a tumor is called ‘Pheochromocytoma’. Syndrome’. ‘Addison’s Disease’. 1) This hypersecretion is occuring w/o regards to stress or time of day. 1) It is autoimmune in nature. 2) When Cortisol/Hydrocortisone lvls are very high, effects r/t excess 2) It can be Primary or Secondary. Aldosterone & Androgens are also seen. Primary: ACTH from the Pit is elevated (in an attempt to stim. the Adrenal Cortex to synthesize more hormones). 3) D/t hypersecretion of ACTH by the: Pituitary gland (probably d/t a tumor ie: Secondary: Deficient ACTH fails to stim. Adrenal steroid synthesis. A benign pituitary adenoma), a lung tumor, or a tumor elsewhere. 3) The Adrenal glands are atrophied, small, misshapen, & are unable to produce adeq. amts of hormones. 4) D/t excess cortisol secretion d/t a problem in the adrenal gland (an adrenal 4) D/t: TB, fungal infection, AIDS, cancer, Hashimotot’s Thyroiditis, bilateral adrenalectomy. Secondary d/t: dysfunction of the Pit or Hypothalamus, prolonged use of adenoma or adrenal carcinoma). corticosteroids reduces the man. of hormones (ie: Pts using long term cort. ther. being dc’d abruptly). 1) Wt. gain, Na & water retention, buffalo hump (fat), moon face (fat), 1) Sodium loss and water loss. Since the Mineralocorticoid Aldosterone causes Pts show exaggerated fight or flight symptoms constantly or sporadically. Htn, tachycardia hyperglycemia, wt gain, central obesity w/thin arms & legs. the kidneys to retain Na, water follows the Na. If there is no Aldosterone, the Na (>100bpm), palpitations, tremor, diaphoresis, apprehension, severe pounding headache, n/v, > blood 2) Hyperpigmentation of the skin, acne, facial hair growth, amenorrhea. leaves & the water leaves as well. This causes a decrease in the blood pressure. glucose d/t catecholamines inhibiting insulin rel. from the pancreas, constipation. The most 3) D.M. (secondary) (d/t: Cortisol causes insulin resistance & stims. Hypotension is the most signficant sign of Addison’s Disease. The body prominent characteristic is intermittent unstable htn. Diastolic BP > 115, unctrld htn & tachycardia. gluconeogeneis which results in glucose intolerance). responds by increasing the HR. The Pt craves Na. Pt is at risk for: stroke, heart attack, heart failure, viz changes, seizures, organ damage, psychosis. 4) Cortisol’s catabolic effect on tissue l/t: Muscle wasting, thin skin w/purple 2) Since Cortisol stims the metabolism/breakdown of carbs, low Cortisol l/t striae, osteoporosis, pathological fx, compression fx of the vertebrae. hypoglycemia & lower blood sugar, which leads to weakness, fatigue, wt. loss, 5) Infection (Cortisol inhibits anti-inflamm. & immunosuppressive action). confusion, psychosis, anorexia, n/v (which l/t electrolyte imbalances). 6) Steroid Psychosis (mental status changes: Irritability to psychosis). 7) Hypokalemia. Viz of the Pt’s Cushingoid appearance. Hx of taking steroid meds. Serum Cortisol. Urine Cortisol. 1) 24 hr urine test: Metanephrines (an end products of metabolism of catecholamine). Serum, Urine,Saliva, 24 Hr Urine test for Cortisol. 2) 24 hr urine test: VMA (Vanillylmandelic Acid) (an end product of metabolism of Plasma ACTH catecholamine). Serum K 3) Blood test for Metanephrines. No caffeine or meds for 2 days before the tests. Dexamethasone Suppression Test 4) CT or MRI. Surgery if it’s d/t a tumor. Alter steroid therapy (lower the dose, 1x/day in the a.m., every other day). Glucocorticoid replacement. 1) Remove one or both Adrenal glands. Radiation of the Pit. gland. Removal of the Adrenal glands. Radiation of the Adrenal glands. Mineralocorticoid replacement. 2) Alpha Blockers. Phenoxybenzamine/Dibenzyline) to dilate blood vessels to ctrl acute htn. Ketoconazole: Blocks prod. of adrenal steroids. 3) Beta Blockers-block the heart & lungs beta adrenergic receptor/ reduce fight-or-flight s/s. Excess fluid risk, Unstable blood glucose lvl risk. Infection. Deficient fluid volume. If both Adrenal glands have been removed the Pt will req. lifelong replacement hormones. Diet ordered: High K, K supplements, high protein, low Na diet. Injury: Htn. Monitor: v/s, fluid & Na excess complications, lungs for crackles (d/t fluid overload), edema in the extremeties, capillary glucose, skin integrity, infections.