3-adrenal wael
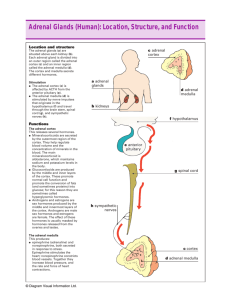
advertisement

Disorders Of Adrenal Glands Dr. Wael H.Mansy, MD Assistant Professor College of Pharmacy King Saud University 1 Adrenal Glands The adrenal glands are small, triangular structures that lie on top of the kidneys. 2 Adrenal Glands Anatomically, the adrenal glands may be divided into two parts: 1. The adrenal medulla, and, 2. The adrenal cortex. The adrenal medulla contains cells that secrete: the catecholamines, epinephrine and norepinephrine. Cells of the adrenal cortex secrete the Glucocorticoids (mainly cortisol), the Mineralcorticoids (mainly aldosterone) and some testosterone. 3 Physiologic functions of the adrenal hormones Catecholamines Epinephrine and norepinephrine Involved in: • the “fight or flight response”: • Interact with α and β receptors in the body • Increase heart and respiratory rate • Increase energy availability; stimulate glycogenolysis in the liver as well as plasma levels of free fatty acids • Reduce gastrointestinal activity 4 Physiologic functions of the adrenal hormones Adrenal Cortex I) Glucocorticoids: Cortisol, corticosterone, cortisol??? •Stimulate the synthesis and storage of glycogen •Increase gluconeogenesis and blood glucose levels •Exert catabolic effects in muscle and fat tissue •Anti-inflammatory action; used clinically as anti-inflammatory agents II) Mineralcorticoids: Aldosterone • act on the distal tubules and collecting ducts of the kidney to increase reabsorption of sodium •Increase plasma volume •Increase renal excretion of potassium 5 Adrenal Cortex: I) Glucocorticoids Control of Cortisol Secretion: Feedback Loops 6 Adrenal Cortex: I) Glucocorticoids Hyposecretion of Adrenal Glands Congenital Adrenal Hypoplasia • An autosomal recessive disorder in which the enzymes necessary for cortisol synthesis are deficient. • Lack of cortisol-negative feedback on the pituitary gland leads to excess ACTH production, which in turn increases the synthesis and release of androgens from the adrenal cortex. • Aldosterone production may also be altered depending on the specific enzyme(s) lacking. 7 Adrenal Cortex: I) Glucocorticoids Hyposecretion of Adrenal Glands Congenital Adrenal Hypoplasia Manifestations • Masculinization of the female external genitals (pseudohemaphroditism). • Short stature due to premature fusion of the epiphyseal growth plate in the long bones. • With certain forms of CAH, a lack of aldosterone production may lead to significant “salt wasting” (sodium losses). 8 Adrenal Cortex: I) Glucocorticoids Hyposecretion of Adrenal Glands Congenital Adrenal Hypoplasia Treatment • Administration of cortisone/hydrocortisone will reduce ACTH levels and block the subsequent production of excess androgens. • Serum electrolyte levels should be closely monitored and corrected, particularly in the salt-wasting form of CAH. • Reconstructive surgery of the genitals may be necessary in females to alter the obvious male characteristics. 9 Adrenal Cortex: I) Glucocorticoids Hyposecretion of Adrenal Glands Addison’s disease • A primary condition associated with atrophy of the adrenal glands. • The majority of cases arise from autoimmune destruction of the adrenal glands. • Some cases may occur as a result of adrenal gland injury as a result of infection or tumors. • Decreased production of cortisol, aldosterone and androgens from the adrenal glands. 10 Adrenal Cortex: I) Glucocorticoids Hyposecretion of Adrenal Glands Addison’s disease Manifestations • Weakness and fatigue. • Increased pigmentation of the skin due to an ACTH-induced increase in Melanocyte (skin pigment cell) activity. • Weight loss, anorexia, hypometabolism, cold intolerance. • Cardiovascular changes: Hypotension up to orthostatic hypotension. • Changes in electroencephalogram and mental function. • Although androgen production from the adrenal glands is reduced, androgen production from other sites in the body (testis) is sufficient to maintain normal sexual function and development11 12 Adrenal Cortex: I) Glucocorticoids Hyposecretion of Adrenal Glands Addison’s disease Treatment As the manifestations of Addison’s disease are due to deficiency of all three hormone groups produced by the adrenal gland (glucocorticoids, mineralcorticoids and androgens), Treatment will be Lifelong replacement therapy with glucocorticoids (cortisone/hydrocortisone) and mineralcorticoids (aldosterone). 13 Adrenal Cortex: I) Glucocorticoids Hyposecretion of Adrenal Glands Adrenal Crisis An episode of severe hypotension, vascular collapse, acute renal failure and hypothermia caused by a combined lack of cortisol and aldosterone. It may be precipitated by infection, trauma and dehydration in individuals with Addison’s disease and can be life-threatening. 14 Adrenal Cortex: I) Glucocorticoids Hypersecretion of Adrenal Glands Cushing's disease • Characterized by excess circulating levels of cortisol. • May be caused by excess ACTH secretion due to pituitary tumors or a tumor of the adrenal gland itself. In rare instances, ACTH or cortisol-producing tumors may occur in the body outside the pituitary or adrenal glands themselves. 15 Adrenal Cortex: I) Glucocorticoids Hypersecretion of Adrenal Glands Cushing's disease Manifestations: • Characteristic “moon face” and “buffalo hump” patterns of fat distribution. • Glucose intolerance and possible diabetes mellitus. • Thin skin, poor wound healing, impaired immune function. • Hypertension. • Muscle weakness and wasting. • Reduced bone density, hypercalciuria with possible development of renal calculi. • Alterations in mental function and personality. • Increased androgen levels in females with possible “virilization.” • Mortality is approximately 50% within 5 years if left untreated. 16 The most common symptom of Cushing's syndrome is sudden weight gain, usually manifested by central obesity. 17 Adrenal Cortex: I) Glucocorticoids Hypersecretion of Adrenal Glands Cushing's disease Treatment: • Surgical removal of tumors. • Radiation therapy. • Chemotherapy if tumor is inoperable. Mitotane is a compound that is structurally similar to the insecticide DDT. It is used because of its selective toxicity for cells of the adrenal cortex to treat tumors arising in this tissue 18 Adrenal Medulla: Pheochromocytoma • A tumor (usually benign) that arises in the chromaffin cells of the adrenal medulla that produce the catecholamines. • Symptoms are those of excess catecholamine production and can be life-threatening. • Excess catecholamine production may be continual or occur in episodes (“bursts”). 19 Adrenal Medulla: Pheochromocytoma Manifestations: Hypertension Tachycardia Severe headache Nausea and vomiting Excess sweating (diaphoresis) Palpitations Anxiety Risk of stroke due to marked hypertension 20 Types of Pheochromocytoma Paroxysmal Type: *The tumor secretion occurs in bouts. *Manifestations occurs only during bouts. *In-between bouts the patient is completely normal. Sustained Type: *The tumor secretion is continuous. *The manifestations begins with the start of tumor secretion, 21 Adrenal Medulla: Pheochromocytoma Treatment: β-Blocking and α-blocking drugs to blunt catecholamine effects Surgical removal of tumor 22