Ludwing_06212011IntelligentMedicine
advertisement

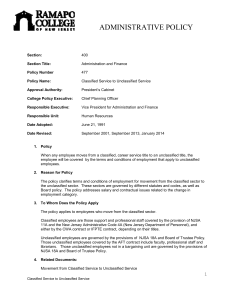
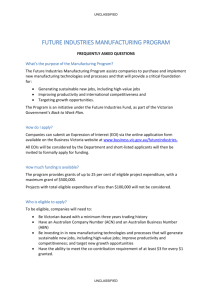
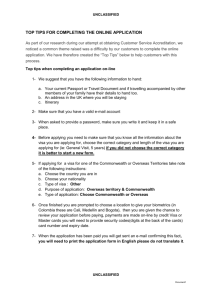
Armed Forces Health Surveillance Center: Medical Intelligence or Intelligent Medicine 21 June 2011 Sharon L. Ludwig, MD, MPH, MA CAPT, USPHS/USCG Division Chief Epidemiology and Analysis UNCLASSIFIED Disclaimer The views expressed in this presentation are those of the author and do not necessarily reflect the official policy or position of the US Army, Department of Defense, Coast Guard, or the Public Health Service. UNCLASSIFIED Briefing Outline 1. Intelligence and Surveillance 2. Introduction to AFHSC 3. Data & Analysis 4. Public Health Practice vs Research 5. Intelligent Medicine UNCLASSIFIED Military Intelligence • Military Intelligence: • • “information and knowledge obtained through observation, investigation, analysis, or understanding Surveillance: systematic observation* for whatever data are available Reconnaissance: specific mission to obtain specific data * of aerospace, surface, or subsurface areas, places, persons, or things, by visual, aural, electronic, photographic, or other means UNCLASSIFIED Military Medical Intelligence • Tracking/assessing full range of global health issues, • • specifically those that could negatively impact U.S. military and civilian health Uses medical/public health surveillance information National Center for Medical Intelligence (NCMI) UNCLASSIFIED Public Health Surveillance • Ongoing, systematic collection, analysis, interpretation, • • • and reporting of health related data Purposes of detecting, characterizing, and countering threats to the health, well-being, and performance of defined populations [Military Services] Followed by timely dissemination and public health action to prevent, treat, or control disease & injury Includes – Medical Surveillance – Occ/Env Health Surv – [Military Force Health Protection] UNCLASSIFIED AFHSC Established Feb 2008 DASD(HA) Force Health Protection & Readiness DoD Global Emerging Infections Surveillance & Response System Global Health Surveillance Capability Area UNCLASSIFIED Army Medical Surveillance Activity Defense Medical Surveillance System (DMSS) & DoD Serum Repository (DoDSR) AFHSC Governance USD (Personnel &Readiness) ASD (Health Affairs) Army Exec Agent Force Health Protection Council Armed Forces Health Surveillance Center UNCLASSIFIED Functional Oversight AFHSC Relationships National (CDC) Armed Forces Health Surveillance Center DoD HQ,USCG State Health Depts PHC(P) POPM NMCPHC BUMED County /Metro Depts USAFSAM AFMSA Service Public Health Ctrs MTFs UNCLASSIFIED AFHSC Mission & Vision • Mission: To promote, maintain, and enhance the health of military and military-associated populations by providing relevant, timely, actionable, and comprehensive health surveillance information and support. • Vision: To be the central epidemiological resource for the US Armed Forces and the Military Health System. UNCLASSIFIED AFHSC Scope of Responsibility IAW CONOPS What We Shouldn’t Do What We Should Do • Strategic level surveillance • Improve decision-making and • Direct installation surveillance effectiveness – Acquire, analyze, interpret, recommend and disseminate information – Develop, refine, and improve standardized surveillance methods – Serve as focal point for sharing health surveillance products, expertise and information • • • • support Healthcare systems analysis Evaluation of the quality of care at the individual provider-patient level Clinical research In-house laboratory services UNCLASSIFIED AFHSC Structure Director Science Advisor HQ Staff Deputy Director Communications, Standards, & Training Division Data Management & Tech Support Division Epidemiology & Analysis Division PERSONNEL Uniformed: 17 FederalCiv: 4 Contract: 63 UNCLASSIFIED GEIS Operations Division AFHSC Divisions Communications, Standards & Training Director Science Advisor HQ Staff Deputy Director Communications, Standards, & Training Division Data Management & Tech Support Division Epidemiology & Analysis Division PERSONNEL Uniformed: 17 FederalCiv: 4 Contract: 63 UNCLASSIFIED GEIS Operations Division AFHSC Divisions Communications, Standards & Training UNCLASSIFIED AFHSC Divisions Communications, Standards & Training Medical Surveillance Monthly Report • • • • • Longitudinal surveillance of health & fitness of Service members > 100 issues Online and mailed each month Annual DoD summaries Promulgation of DOD standard case definitions www.afhsc.mil UNCLASSIFIED AFHSC Divisions Communications, Standards & Training AFHSC Surveillance Standards • Part of AFHSC mission to provide guidelines and standardization for epidemiological purposes across DoD • AFHSC maintains the Tri-Service Reportable Medical Events Guidelines and Case Definitions • New “surveillance case definitions” are among first formal efforts to document methods unique to AFHSC/Defense Medical Surveillance System UNCLASSIFIED AFHSC Divisions Communications, Standards & Training UNCLASSIFIED AFHSC Divisions Communications, Standards & Training Resident Rotations at AFHSC • Preventive and Occupational Medicine residents – Walter Reed Army Institute of Research (WRAIR) – Uniformed Services University of the Health Sciences (USUHS) • 4-6 week rotation w/data analysis project using DMSS UNCLASSIFIED AFHSC Divisions GEIS Operations Director Science Advisor HQ Staff Deputy Director Communications, Standards, & Training Division Data Management & Tech Support Division Epidemiology & Analysis Division PERSONNEL Uniformed: 17 FederalCiv: 4 Contract: 63 UNCLASSIFIED GEIS Operations Division AFHSC Divisions GEIS Operations Strategic Goals and Priority Pillars RI = Respiratory Infection GI = Gastrointestinal Infection FVBI = Febrile & Vectorborne Infection AR = Antimicrobial Resistance STI = Sexually Transmitted Infection STI STI DRO AR FVBI GI GI ARD RI Force Health Protection Surveillance and Response Training and Capacity Building Research, Innovation and Integration Assessment and Communication of Value Added UNCLASSIFIED AFHSC Divisions GEIS Operations WRAIR/NMRC DoD Partners USAPHC (Prov) Germany NHRC Korea Egypt USAFSAM Thailand NMCPHC Kenya Peru Pacific UNCLASSIFIED AFHSC Divisions Data Management & Tech Support Director Science Advisor HQ Staff Deputy Director Communications, Standards, & Training Division Data Management & Tech Support Division Epidemiology & Analysis Division PERSONNEL Uniformed: 17 FederalCiv: 4 Contract: 63 UNCLASSIFIED GEIS Operations Division AFHSC Divisions Data Management & Tech Support • Maintain Defense Medical Surveillance System (DMSS) • Archive HIV test results • Maintain DOD Serum Repository • Support AFHSC IM/IT Needs UNCLASSIFIED AFHSC Divisions Data Management & Tech Support DMSS—Longitudinal Database >1.5B Records MEPS 12.1 million persons 26.6 M records Personnel Data 9.4 M persons 111.7 M records Serum 58.2 M specimens 38.9 HIV test results Hospitalizations 2.5 M records Pre / Post-Deployment Health Assessments 8.5M Discharge or Death Accession Process Immunizations 86.9 M records Reportable Diseases 276 K records Deployments 4.9 million records Casualty Data 49 K Deaths Ambulatory Data 211.7 M records As of Feb 2011 UNCLASSIFIED AFHSC Divisions Data Management & Tech Support DMSS Data Inputs / Frequency Table Source Frequency Person DMDC Monthly 9.4 M 1985 -- 2010 Demographics DMDC Monthly 109.7 M 1985 -- 2010 MEPS MEPCOM Monthly 37.9 M 1985 -- 2010 Deploy (PGW) DMDC Single 682 K 1990 -- 1991 Deploy (CENTCOM) DMDC Monthly 3.5 M 1993 – 2010 Deploy Forms MEDPROS, PIMR, EDHA Daily/Weekly 8.1 M 1996 – 2010 Inpatient-MTF/TED DHSS Monthly 2.5 M 1990 – 2010 Outpatient-MTF/TED DHSS Weekdays 201.4 M 1996 – 2010 Reportable Events MTFs Daily 266.8 K 1994 – 2010 Immunizations DEERS Weekdays 87.0 M 1980 -- 2010 DoDSR DoDSR Weekly 57.5 M 1985 -- 2010 Casualty WHS / AFIP Quarter/Month 48.7 K 1985 -- 2010 TMDS FHP&R Daily 4.5M 2005 – 2010 TRAC2ES (CENTCOM) TRANSCOM/FHP&R Weekly 72.9K 2001 – 2010 UNCLASSIFIED Rows Time Period AFHSC Divisions Data Management & Tech Support Reportable Events Process Provider / Lab Report Installation / Ship / Unit PM Installation / Unit Prev Med DRSi Installation / Unit Prev Med AFRESS Navy Environmental PM Unit Regional Medical Command Navy Marine Corps Public Health Center Army Public Health Command (P) Monthly/Weekly AFMOA / MAJCOM Air Force Sch of Aerospace Med Weekly Armed Forces Health Surveillance Center/DMSS UNCLASSIFIED AFHSC Divisions Data Management & Tech Support Defense Medical Epidemiology Database UNCLASSIFIED AFHSC Divisions Data Management & Tech Support DMSS & Functional Relationships PERSONNEL DATA MEDICAL DATA Active Duty Since 1990 6.6 million persons 74.9 million records In-patient Since 1990 2.7 million records 8.9 million records Reserve Component Since 1990 2.4 million persons 27.6 million records Ambulatory Since 1996 161.8 million records 556.9 million records Active Duty Casualty Since 1980 40,600 records Reportable Events Since 1995 215,000 records 120,000 records Military Entrance Processing Stations Since 1985 11.1 million persons 23.1 million records Immunizations Since 1980 51.6 million records SEROLOGIC DATA Deployment Rosters Since 1990 2.6 million persons 4.0 million records Serologic Specimens Since 1985 9.0 million persons 46.1 million specimens Pre and Post Deployment Health Assessments Since 1994 6,366114 surveys Disease and Non-Battle Injury (aggregate) Since 1996 98,900 records DMSS Services of the Armed Forces Health Surveillance Center Medical Surveillance Monthly Reports (MSMR) DEPLOYMENT DATA Monthly Synchronization Hospitalization Queries Ambulatory Queries Adhoc Requests Studies and Analyses Routine Reports & Summaries DMED Version 3.6 Remote Access to DMSS data (non-privacy act only) DMSS: Defense Medical Surveillance System DMED: Defense Medical Epidemiology Database UNCLASSIFIED Reportable Events Queries Personnel data Queries AFHSC Divisions Data Management & Tech Support • World’s largest serum repository • Unrivaled potential for sero-epi studies • ~ 40 various size sample requests/year • 60M serial serum specimens from 10M individuals • Linked to demographic, military, and medical information via the DMSS DoD Serum Repository UNCLASSIFIED AFHSC Divisions Epidemiology & Analysis Director Science Advisor HQ Staff Deputy Director Communications, Standards, & Training Division Data Management & Tech Support Division Epidemiology & Analysis Division PERSONNEL Uniformed: 17 FederalCiv: 4 Contract: 63 UNCLASSIFIED GEIS Operations Division Epidemiology & Analysis Customers • Secretary of Defense • Assistant Secretary of Defense for Health Affairs [ASD(HA)] • USCG Director of Health and Safety • Joint Chiefs • Service Surgeons General • Service Public Health Hubs • AFHSC Staff UNCLASSIFIED Epidemiology & Analysis Data sources: DMSS, DoDSR, others Operational surveillance analysis (600/yr) Support for: –DoD policy development –GAO investigations –Congressional Inquiries Analysis for MSMR articles Special Studies / Research Support Includes specialized influenza surveillance/analysis Focused periodic reports (1450/yr) UNCLASSIFIED Epidemiology & Analysis Example of MSMR Support US Military Malaria Cases Jan 02-Dec 08 55 45 Other 40 Korea 35 Afghanistan 30 25 20 15 10 October 2008 July April January October 2007 July April January October 2006 July April January October 2005 July April January October 2004 July April January October 2003 July April January October 2002 July 0 April 5 January Number of cases Likely infection location Peacekeeping mission in Liberia 50 Source: MSMR Vol 16, No. 1 Jan 09, AFHSC UNCLASSIFIED Epidemiology & Analysis Example of Serum Study: Hantavirus in Military Personnel from Four Corners Area UNCLASSIFIED Epidemiology & Analysis May 2010: AFHSC Routine Reports* Type Total # Reports Reportable Medical Events/Communicable Diseases Deployment Health Assessments Influenza H1N1 Vaccine Safety and Compliance Medical Evacuations Deployment Health Report Malaria Smallpox Cardiac Adverse Events Report Training-related injuries Leishmaniasis Traumatic Brain Injury Post Traumatic Stress Disorder MHS Dashboard Measures FHP QA Measures Wounded Service Members Vaccine Adverse Events Special Surveillance: Amputations, DVT, Leish, ARDs Injury Installation Reports Lost duty Meningococcal Report 53 28 11 5 4 0 (quarterly) 1 1 1 1 3 1 1 1 1 2 1 1 2 1 # Unique Reports 7 18 3 2 1 0 (quarterly) 1 1 1 1 3 1 1 1 1 2 1 1 2 1 Over 50 routine reports distributed monthly, quarterly, weekly, or daily (1448 total reports annually) Over 600 requests performed annually UNCLASSIFIED Epidemiology and Analysis Quarterly Deployment Health Report October 2010, page 6 of 16 UNCLASSIFIED Request Process Request arrives at AFHSC Assign to Liaison Clarify question, draft analysis plan RESEARCH Status determination PUBLIC HEALTH PRACTICE Analysis plan presented at R3 IRB Coding & output Review, approval and delivery De-identified dataset Summary table UNCLASSIFIED Request Process Requestor Contacts AFHSC • Service liaisons – Army – Navy, • Marine Corps • Coast Guard – Air Force • Special Projects lead • Residency Program • Communications Center • Other staff interactions UNCLASSIFIED Request Process Clarify the Question Can We Do It? • Legal – DMSS is System of Records – Human Subjects Protection – Classified or Privacy Protected • Scientifically Sound (Methods Valid) • Data/Sera Available UNCLASSIFIED Request Process Clarify the Question Should We Do It? • Requestor’s Intent & Authority • Militarily Relevant • Military Sponsor • Level of Surveillance (Strategic vs Unit) • Intent – Related to Public Health – Purpose (Scope of Responsibility) – PH Practice v Research UNCLASSIFIED Request Process Request arrives at AFHSC Assign to Liaison Clarify question, draft analysis plan RESEARCH Status determination PUBLIC HEALTH PRACTICE Analysis plan presented at R3 IRB Coding & output Review, approval and delivery De-identified dataset Summary table UNCLASSIFIED Types of Requests • “Operational” – Strategic – DoD-wide – Public Health Practice • Research – Support – Internal research UNCLASSIFIED Public Health Practice • Specific authorization • Accountability to the public • May legitimately involve persons who did not volunteer to • • participate Draws on the principles of public health ethics by focusing on populations while respecting the dignity and rights of individuals May be distinguished from research on the basis of general legal authority, specific intent, responsibility, participant benefits, experimentation, and subject selection UNCLASSIFIED Public Health Practice Primary intent • Prevent or control disease or injury and improve health • Benefit is to the population from which information is gathered • Military PH Practice – Commanders, supervisors, individual Service members, and MHS shall promote, improve, conserve, and restore physical/mental wellbeing…across the full range of military activities and operations – Conduct activities common to other public health agencies, including disease/injury surveillance, “reportable medical event” case reporting, outbreak investigation, program evaluation etc. UNCLASSIFIED Public Health Research Primary intent • If to generate or contribute to generalizable knowledge, then • • research If to prevent or control disease or injury or improve a public health program, then non-research (= PH practice = “operational”) If changes from prevention or control to generating generalizable knowledge, then it becomes research UNCLASSIFIED Request Process Request arrives at AFHSC Assign to Liaison Clarify question, draft analysis plan RESEARCH Status determination PUBLIC HEALTH PRACTICE Analysis plan presented at R3 IRB Coding & output Review, approval and delivery De-identified dataset Summary table UNCLASSIFIED Request Process • Draft Analysis Plan UNCLASSIFIED Request Process Present to Request/Report Review (R-3) Team • Epidemiology & Analysis Chief • E & A Asst Chief • Service liaisons • Science advisor • Senior Epidemiologists • Senior Biostatisticians • MSMR staffer • Others ad hoc UNCLASSIFIED Request Process R-3 Presentation (“Morning Rounds”) • S: Requestor, Question • O: Background material, supporting • • literature, military relevance, etc. A: Public Health Practice or Research P: Analysis Template UNCLASSIFIED Request Process R-3 Team Review • R-3 Team questions the presenter • Presenter may need to further clarify the question (to R-3 or with customer) – Can we do it – Should we do it • New R3 approval process, if needed UNCLASSIFIED Request Process Request arrives at AFHSC Assign to Liaison Clarify question, draft analysis plan RESEARCH Status determination PUBLIC HEALTH PRACTICE Analysis plan presented at R3 IRB Coding & output Review, approval and delivery De-identified dataset Summary table UNCLASSIFIED Request Process Analysis • Once approved by R-3, assignment to analyst • Coding – – – – – – Complicated person-time calculations Complex case definitions Multiple/complex outputs Modifications to original request Prioritization with other requests Technical difficulties • May need to return to R-3 UNCLASSIFIED Request Process Request arrives at AFHSC Assign to Liaison Clarify question, draft analysis plan RESEARCH Status determination PUBLIC HEALTH PRACTICE Analysis plan presented at R3 IRB Coding & output Review, approval and delivery De-identified dataset Summary table UNCLASSIFIED Request Process Analysis • Output – De-identified data set – Summary table • Deliver to customer UNCLASSIFIED AFHSC Example H1N1 Influenza Response UNCLASSIFIED Detection of Pandemic Flu (pH1N1) ESSENCE Cases First ESSENCE Alert (26 Apr 09) 2009 Navy FM (1st case) presents in San Diego 37 Sailors present in San Diego 2 Army FM present in San Antonio March April May UNCLASSIFIED June July Pandemic Influneza • First four cases of pandemic H1N1 detected in two AFHSC/GEIS funded laboratories – Specimens and information provided to CDC • Three DoD pH1N1 strains used by WHO as potential seed strains; one was selected • Supported the diagnostic confirmation of the first H1N1 cases in 14 different countries (US, Bhutan, Cambodia, Djibouti, Kuwait, Kenya, Lao People’s Democratic Republic, Lebanon, Egypt, Nepal, Colombia, Ecuador, Peru, Republic of the Seychelles) • Numerous pH1N1 laboratory capacity building for diagnosis – NAMRU-3: 30 countries and 70 participants in 3 weeks!!! UNCLASSIFIED Communication: DoD Global Influenza Activity Samples Received: Total= Cumulative Samples since 1 September 2009, New=Previous Two Week Period USAFSAM TOTAL 6,293 Flu A: LRMC/CHPPM (NEW) TOTAL TOTAL 1,289 (164) Flu A: H1N1: 1 TOTAL 3,495 (80) 13 pH1N1: (1) H3N2: pH1N1 1,122 (165) TOTAL CONUS MEDCENs TOTAL NAMRU-3 TOTAL 2,576 (508) 1,729 (NEW) Flu A: 793 (122) Flu B: 15 8 H3N2: 24 Flu B: 30 (11) Flu B: 4 (1) TOTAL H3N2: pH1N1: Flu A: H1N1: H1N1: H3N2: H3N2: pH1N1 : 342 (21) pH1N1 : Flu B : Flu B: 2 (NEW) 2 AFRIMS TOTAL 2 (1) Guam (NEW) 5 733 TOTAL 11 Flu A: (NEW) 1666 Flu A: 101 284 (53) TOTAL 288 11 260 (96) Flu A: H1N1: 3 (2) H3N2: 21 (12) pH1N1: Flu B: pH1N1: 68 Flu B: 4 (3) 16 pH1N1: 147 (29) (4) 70 (7) NAMRU-2 TOTAL (NEW) 1503 H1N1: H3N2: Flu A: pH1N1 H1N1: Flu B: H3N2: 58 pH1N1: 107 225 H5N1: Flu B: DoD Research Labs (NEW) Note: H5N1 (positives/tested or pending) results are cases that have been confirmed and reported through WHO in compliance with the International Health Regulations 2005. 3 H1N1: H3N2: 5 H3N2: Flu B: Medical Centers/Clinics 17 5 363 (30) Flu A: DoD Service Labs 3 22 (1) 48 USAMRU-K H1N1: NMRC-Lima pH1N1 46 91 37 H5N1: Flu A: H3N2: (NEW) H1N1: Flu B: H1N1: pH1N1: 369 H1N1: (NEW) 562 H3N2: pH1N1: TOTAL Flu A: (NEW) 8,279 1,740 Flu A: (NEW) 615 H1N1: TOTAL CENTCOM-Mil Flu B: 507 H1N1: TAMC 162 (92) (NEW) Flu A: Flu B: Flu B: Flu A: H3N2: pH1N1 1,885 USF Japan (NEW) 1,098 164 167 H1N1: H3N2: NHRC USF Korea (NEW) 472 60 2 Communication: Surveillance Partner Reporting Sentinel Surveillance Population-Based/Recruit Electronic Military Health Surveillance DOS Embassy Lab-Specific Regional UNCLASSIFIED Communication: Network Summary Available at: http://www.afhsc.mil ü60 UNCLASSIFIED 2009 pH1N1: AFHSC Coordination Attributes Combined Under One Roof • Laboratory network: Global visibility • Reportable Medical Events: Uniformed personnel visibility • Conference call coordination • Daily/weekly reporting for chain of command UNCLASSIFIED Intelligent Medicine • “…‘intelligent medicine’ that will give physicians the tools they need to regain control over medical decisions made for their patients.” “A Path to Intelligent Medicine” Walter Eisner, from Rick Guyer, MD; outgoing President of the North American Spine Society, farewell speech at annual meeting, October, 2007 UNCLASSIFIED Intelligent Medicine • “…bringing real thought to bear on our prevention and treatment strategies, not just falling back on the conventional treatment, whether high-tech or alternative, in a knee-jerk reaction;” – …in charge or your own health and fitness” – A guide for patients to “help their doctors” and wisely use the medical and preventive options available in the current environment. Ronald Hoffman, MD Intelligent Medicine: A Guide to Optimizing Health and Preventing Illness for the Baby-Boomer Generation, 1997, Simon and Schuster UNCLASSIFIED Intelligent Military Medicine • Evidence based policy and prevention strategies for the United States Armed Forces UNCLASSIFIED Questions UNCLASSIFIED