Imaging Anatomy of the Heart and Great Vessels
advertisement

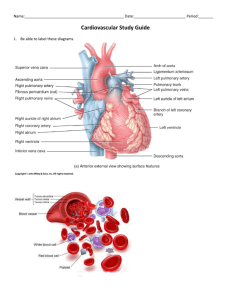
Imaging Anatomy of the Heart and Great Vessels Reghard du Toit Imaging modalities • Chest radiograph: the plain CXR is widely used for the initial assessment of the heart and great vessels. • Angiography: Involves injection of contrast directly into the heart chambers via a pigtail catheter usually introduced the femoral artery for the left sided chambers and through the femoral vein for the right sided chambers • Coronary angiography: Involves selective catheterization of the coronary arteries • CT and MRI • Nuclear medicine; Mainly for functional assessment of the heart ( not discussed) • Echocardiography; Ultrasound allow both structural and functional assessment but requires considerable expertise and is not discussed in this presentation. Gross anatomy and orientation of the heart • Lies obliquely in the chest. • Left atrium forms the base or posterior part and the superior and inferior pulmonary veins drain into its four corners. • Right atrium forms the right border and the SVC and IVC drain into its upper and lower parts. • The apex and left border are formed by the left ventricle • The right ventricle forms the anterior part. • The inferior (diaphragmatic) part of the heart is formed by both the ventricles anteriorly and a small part of the right atrium posteriorly where the IVC enters this chamber. The Heart: Gross anatomy and orientation • • • • • Lies obliquely in the chest Pyramidal in shape Left atrium forms the base or posterior part Right atrium forms the right heart border Left ventricle forms the apex and left heart border • Right ventricle forms the anterior part • Inferior or diaphragmatic part formed by both ventricles anteriorly and a small part of the right atrium posteriorly. • The oblique orientation of the heart causes the ventricles to lie anterior and inferior to the atria. • Heart also clockwise rotated about its axis which cause the right atrium and ventricle to be at a slightly higher level than the left. • The interatrial and interventricular septa lie in a left anterior oblique plane. • The tricuspid and mitral valves are roughly vertically oriented. Anatomy of the heart Cardiac valves on CXR • On PA views the valves lie close to a line from the left atrium to the lowest point of the right heart border. • On a lateral view the pulmonary and aortic valves lie just above and the mitral and tricus valves just below a line drawn from T5 to the apex of the heart. Position of the cardiac valves on plain radiography Pericardium • Closed sac consisting of parietal and visceral layers that is draped over the heart and great vessels and enclose a potential space which contains 20-25ml of serous fluid. ( 1-2 mm in diameter) • Visceral layer adhered to myocardium and is known as the epicardium. • Parietal layer only bound inferiorly to central tendon of diaphragm and superiorly where it fuses with the covering of the great vessels. • Pericardial reflections (basically the boundaries of the closed sac) : • 1. Oblique sinus; space between the IVC and pulmonary veins. • 2. Transvers sinus; space between the aorta and pulmonary artery. • The serous pericardial layers extend anterosuperiorly over the SVC and separately over the aorta and pulmonary artery. • The pericardium extends superiorly for 2-3cm over the ascending aorta and over the pulmonary artery almost to its bifurcation. • Some fat is present between the epicardium and myocardium and this normally increases with age. • Fat is also present between the pericardium and the mediastinal pleura and it may be extensive in the anterior and lateral cardiophrenic angles where it is know as the pericardial fat pad. Pericardial fat pad Axial CT scan shows a large cardiophrenic fat pad. Normal variant. Cardiac chambers and valves • Right atrium: • Has a smooth posterior wall into which the great veins drain. The coronary sinus drains into the posterior wall between the orifice of the IVC and the tricuspid valve. The interatrial septum bears an oval depression, known as the fossa ovalis which represents the closed foramen ovale. The right atrial appendage projects anterosuperiorly and to the left and is the only part of the right atrium to contribute to the cardiac outline on the lateral view. The inner wall of the atrial appendage is ridged by musculi pectinati with a vertical ridge, the crista terminalis. • • • • Right ventricle • • • • • • Normally in contact with the lower half of the sternum on the lateral view. The inner wall is coarsely trabeculated by thick muscular bundles except for the smooth muscular conus ( infundibulum) of the ouflow tract. The crista supraventricularis demarcates the smooth conus from the trabeculated wall on the septal aspect of the conus. A muscular band, moderator band , tranverses the cavity carrying the right bundle branch fibres. It crosses from the lower ventricular septum to the anterior wall joining the anterior papillary muscle. The entrance to the right ventricle is the tricuspid valve. This has three leaflets or cusps each attached to papillary muscles by the chordae tendineae. The pulmonary valve has three semilunar cusps, right and left anterior and posterior. This is the most anterior and superior of all the cardiac valves. Left atrium • Forms the upper and posterior part of the heart on lateral views. • Receives four pulmonary veins in its upper part. • Has a long narrow, trabeculated appendage that projects anteriorly on the left side of the pulmonary trunk- only seen on the frontal view when enlarged. Left ventricle • • • • • • Thick walled and elongated cone shaped. Forms the lower half of the posterior part of the heart on the lateral view. The mitral valves has two cusps and separates the left ventricle from the left atrium. The free margins of the two cusps, anterior and posterior, is attached to the ventricular wall by chordae tendineae. Instead of a muscular conus as on the right, the larger anterior cusp separates inflow and outflow tracts and blood flows over both its surfaces. The mitral and aortic valves are in fibrous continuity. • The aortic valve has three semilunar cusps, anterior and left and right posterior. • There is a localized dilatation or sinus above each cusp known as the sinuses of Valsalva. • Ventricular septum diameter 5-10mm. • Myocardial thickness 10-12mm. Papillary muscles and chordae tendineae Three chamber MPR shows left ventricular papillary muscles and chordae tendineae Coronal MPR shows LV papillary muscles The coronary arteries and veins • Right coronary artery arises from the anterior sinus and is also known as the right coronary sinus. • Left coronary artery arises from the left posterior sinus and is also known as the left coronary sinus. • No artery arises from the right posterior sinus, also know as the non-coronary sinus. Overview Anterior Right ant oblique Lateral Right coronary artery • The RCA supplies the right ventricle and inferior wall of the left ventricle. • Arises from the anterior coronary sinus of Valsalva and passes between the pulmonary trunk and right atrium to decend in the right atrioventricular groove as the marginal artery. • Anastomose with the left coronary artery in the region of the posterior interventricular groove. Branches • 1. Conus artery to the pulmonary outflow tract. • 2. Atrial and ventricular branches. • 3. Branch to SA node which curves anticlockwise around the SVC . • 4. Acute marginal branches supply the right ventricle. • 5. Branch to AV node • 6. Posterior interventricular artery forms the terminal part of the RCA and supplies the inferior surface of the left ventricle and posterior two-thirds of the interventricular septum. Left coronary artery • Arises from the left posterior sinus of Valsalva and supplies the remainder of the left ventricle. • Bifurcates early into the left circumflex artery and anterior decending artery • Left circumflex continues laterally in the atrioventricular groove to anastomose with the RCA. • LAD decends in the anterior interventricular groove. Branches of LAD • 1. Septal branches • 2. Diagonal branches that run over the anterolateral wall of the left ventricle supplying it. • 3. Occasionally a branch to the right ventricle. Branches of the Left circumflex artery • 1. Obtuse marginal branches which supply the lateral wall of the left ventricle. • 2. Atrial branches. • In general the RCA supplies the right ventricle and the inferior part of the left ventricle. The LCA supplies the remainder of the left ventricle. • The intervetricular septum is supplied by the LCA anteriorly and the RCA posteriorly. • The SA node is supplied by the RCA in > 50 % and the AV node >90% by the RCA. Coronary dominance • Is determined by the artery that supplies the PDA and the posterolateral artery, in effect the artery supplying the posterior and lateral wall of the left ventricle. • Right-dominant: RCA supplies both these arteries ( 60%) • Left-dominant: Circumflex artery supplies both these arteries. ( 15%) • Co-dominant: RCA supplies the PDA and circumflex artery supplying the posterolateral artery. ( 25%) Veins of the heart • Venous drainage of the heart mainly ( 60% ) via veins that accompany the coronary arteries and which drains via the coronary sinus. • The coronary sinus lies in the posterior atrioventricular groove and drains into the posterior wall of the right atrium to the left of the orifice of the IVC. Tributaries • • • • Great cardiac vein: ascends in the anterior interventricular groove and then runs to the left in the atrioventricular groove to become the coronary sinus. Middle cardiac vein: ascends in the posterior interventricular groove. Small cardiac vein: accompanies the marginal branches of the RCA, then posteriorly in the right atrioventricular groove to enter the right side of the coronary sinus. Left posterior ventricular vein: accompanies the obtuse marginals of the LCA and drain into the coronary sinus. Great vessels Aorta • Aortic root ( diameter of 3,7 cm with variation of 0,3 cm in diameter) • First few centimetres from aorta valve to just above the coronary sinuses. • It lies at the level of the right third costal cartilage anteriorly and T5 posteriorly • The wall has three focal dilatations corresponding to the three semilunar cusps of the aortic valve. MPR Saggital view of thoracic aorta Ascending aorta • Continues superiorly, anteriorly and to the right for approximately 5cm. • Becomes aortic arch at the level of the manubrial angle. • Right ventricle is anterior and to the left, pulmonary trunk to the left and the right atrium and SVC to the right. • Diameter 3,2cm with variation of 0,5 cm at level of pulmonary trunk bifurcation. Aortic arch • • • • • • Runs superiorly and posteriorly from right to left. ( 1,5 cm with variation of 1,2 cm in diameter) At first anterior to the trachea and oesophagus and then over the pulmonary trunk and left main bronchus to a position left of body of T4. Pulmonary trunk bifurcates beneath the arch and the right pulmonary passes to the right of the arch. The left pulmonary artery is attached to the junction of the arch and descending aorta ( i.e. isthmus) by the ligamentum arteriosum. In the majority of people (65%) the major vessels arise from the arch in the following order: 1) Brachiocephalic artery 2) Left common carotid artery 3) Left subclavian artery • • • • • The following arteries may also arise from the arch: -one or both bronchial arteries -thyroidea ima artery -inferior thyroid artery -internal thoracic artery • • Descending aorta • Passes down the posterior mediastinum to the aortic hiatus of the diaphragm at the vertebral body of T12. • Diameter 2,5cm with variation of 0,4 cm . • Lies behind the left main stem bronchus, pulmonary artery and left atrium. • Right lung and pleura lie laterally. • Vertebral column lies posteriorly and medially. • Oesophagus lies antero-medially except in its upper portion where it lies to the right. Branches • 1) Nine pairs of intercostal arteries • 2) Bronchial arteries, the number and location of which are variable. • 3) Oesophageal branches; up to five arteries which form an anastomotic plexus with branches of the inferior thyroid, inferior phrenic and left gastric arteries. • 4) Spinal arteries, up to three branches • 5) Mediastinal branches • 6) A pair of superior phrenic arteries • 7) A pair of subcostal arteries • The aorta is fixed within the thorax at certain anatomical points, the aortic isthmus, aortic valve, the main aortic branches, the intercostal vessels and the diaphragm. Great Veins • • • • • The SVC is formed by the right and left brachiocephalic veins behind the junction of the manubrium and the first costal cartilage. The SVC enters the right atrium at the level of the right third costal cartilage. It lies to the right of the aortic arch and anterior to the right main stem bronchus. The azygos vein arches over the right main stem bronchus to drain into the posterior aspect of the SVC. SVC diameter 1,4 cm with variation of 0,4cm at level of aortic arch and 2cm with variation of 0,4cm at pulmonary trunk bifurcation. • The brachiocephalic veins are formed by the union of the internal jugular and subclavian veins behind the medial end of either clavicle. • Both receive the internal thoracic and inferior thyroid veins, while the left sided superior intercostal vein and thymic vein also drains into the left brachiocephalic vein. • The IVC runs a short course of only a few centimetres in the thorax and often makes up the lowest portion of the cardiac silhouette on the right Pulmonary arteries • • • • • • The pulmonary trunk bifurcates beneath the aortic arch into right and left main pulmonary arteries. Pulmonary trunk diameter 2,4cm with variation of 0,2cm. The right pulmonary artery passes under the arch in front of the right main bronchus and behind the ascending aorta and SVC. Proximal right pulmonary artery diameter 1,9cm with variation of 0,3cm. It is crossed anteriorly by the right superior pulmonary vein ( right hilar point on frontal radiograph) It divides into an upper and lower branch before entering the lung hilum. • The left main pulmonary artery passes to the left, initially in front of the left main bronchus but then curves superior to the bronchus. • Left pulmonary artery diameter 2,1cm with variation of 0,4 cm. • The ligamentum arteriosum runs posteriorly from the left pulmonary artery to its attachment at the aortic isthmus. • The left main pulmonary artery is shorter than the right and lies at a higher position. • The left pulmonary vein crosses anteriorly, thus marking the left hilar point which is 1cm higher than the right. Pulmonary Veins • The pulmonary veins enter the left atrium from the posterolateral margin, two from each lung. • They usually converge on the left atrium beneath the level of the pulmonary arteries. • They may however become confluent before entering the left atrium. References • 1. Butler P, Mitchell AVM, Ellis H (1999) Applied Radiological Anatomy. Cambridge University Press. • 2. Netter FH Atlas of Human Anatomy, Saunders Elsevier. • 3. Ryan S, McNicholas M, Eustace S (2011) Anatomy for Diagnostic Radiology 3rd ed, Saunders Elsevier. • 4. James Obrien, Manvedi B, Serichai E, Hecht D, Jacobs K: Anatomy of the Heart at Multidetector CT; What the radiologist needs to know. Radiographics November-December 2007 27: 1569-1582. • 5. Hym Woo Goo, In-Sock Park, Jae-Kun Ko, Yong Hwue Kim, Dong-Mon Seo : CT of Congenital Heart disease; Normal Anatomy and Typical Pathologic Conditions. Radiographics October 2003 23: 147-165. • 6. www.radiologyassistant.nl : Cardiac Anatomy from left to right by Tineke Willems and Maricke Hazenwinkel. • 7. www.radiologyassistant.nl : Coronary Anatomy and anomalies by Robin Smithuis andTineke Willems.