Consulting Info with logo template etc in header and footer
advertisement

Document for Submission to the University of Heriot -Watt Life Sciences’
Research Ethics Committee, v1.0
February 2012
Tungsten Carbide with Cobalt Binder: An
Historical Cohort and Nested Case-Control
Study of Lung Cancer – UK Component
In collaboration with:
University of Pittsburgh
University of Illinois at Chicago
OUR IMPACT ON THE ENVIRONMENT
At IOM we seek to minimise our environmental impact. We produce thousands of
reports every year and these consume a large quantity of paper. To minimise our
impact on the environment, we prefer to only provide an electronic copy of reports,
although we can provide a paper copy on request. If you have any additional
requirements please let us know.
CONTENTS
EXECUTIVE SUMMARY
4
1
BACKGROUND AIMS AND OBJECTIVES
6
1.1
1.2
1.3
1.4
Objective
Specific Aims
Background
Significance
6
6
6
7
2
RESEARCH DESIGN AND METHODS
8
2.1
2.2
2.3
2.4
2.5
2.6
Study Interventions
Task 1 – Site Cohort Enumeration
Task 2 – Data Processing, Validation and Management
Task 3 – Vital Status Tracing
Task 4 – Integration of Exposure Data
Statistical Analysis
8
8
9
9
9
10
3
HUMAN SUBJECTS
11
3.1
3.2
3.3
3.4
General Characteristics
Inclusion/Exclusion Criteria
Identifying Subjects
Ethical clearance and Informed Consent
11
11
11
11
4
POTENTIAL RISKS
12
4.1
4.2
4.3
Confidentiality
Potential Benefits
Data and Safety Monitoring Plan
12
12
12
5
COSTS AND PAYMENTS
13
5.1
5.2
5.3
Research Study Payments
Qualifications of Investigators
Sources of Support
13
13
13
6
REFERENCES
14
7
APPENDIX 1 – RESEARCH PROPOSAL FOR THE INTERNATIONAL
STUDY
16
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
EXECUTIVE SUMMARY
Information gathered in a feasibility study shows that a scientifically rigorous and
comprehensive epidemiology study of workers employed in the manufacture or production
of tungsten carbide with a cobalt binder (WCCo) is feasible and should include workers
from 10 manufacturing sites in the United States and nine manufacturing sites in Europe,
two of which are located in the West Midlands in England. This large epidemiology study,
referred to as the Phase 3 study, will represent multiple companies, countries and
manufacturing processes and will be larger, more robust and more definitive than any
WCCo epidemiology study done to date.
The proposed historical cohort study is designed as an essential step in appraising the
health implications of occupational exposure to WCCo. The primary research objectives of
the Phase 3 study are:
1. To investigate the total and cause-specific mortality experience of current and
former workers potentially exposed to WCCo at multiple US and EU industrial sites
that produce(d) WCCo and/or manufacture(d) WCCo products, as compared with
the experience of the corresponding national and local populations from which the
workforces were drawn, with adjustment for potential confounding factors and with
emphasis on malignant neoplasms of the lung. For the UK component, this will
involve using mortality rates for the West Midland and for England and Wales
combined. An analysis for all sites combined will be carried out by colleagues in
Pittsburgh; a separate analysis of the UK sites will be carried out by IOM
researchers.
2. To characterize as completely as possible the past and current working
environment of the study members from the sites relative to work area, job
title/function and potential for exposure to WCCo as well as potential co-exposures
to several known or suspected human carcinogens including tungsten (W),
tungsten carbide (WC), carbon (C) and cobalt (Co). Work to gather the data
required at the UK sites will be undertaken by IOM, with the analysis being carried
out by each unit using agreed upon methodology that will be proposed by
colleagues at the University of Illinois at Chicago and will be modified or accepted
by consensus at the forthcoming conference in Edinburgh in June.
3. To determine the relationship between level and duration of WCCo exposure and
mortality from malignant lung neoplasms with analytic adjustment to the extent
possible for potential co-exposures, including tobacco smoking habits. Whether a
separate analysis will be carried out for the two UK sites will very much depend on
a sufficient number of lung cancer cases being recruited to the study and therefore
sufficient statistical power for a separate meaningful analysis.
4. To provide a framework for ongoing mortality surveillance of workers potentially
exposed to WCCo with and without concomitant co-exposures.
Our statistical analysis of the study data will consist of two major parts, each of which is
designed to address specific objectives of the study:
Part 1 Analysis of total and cause-specific mortality patterns in relation to basic
demographic and work history factors (e.g., study site, race, gender, age, calendar time,
year of hire, duration of employment and the time since first employment), with focus on
cancer mortality and emphasis on the implicated site of interest (lung).
Page 4 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
Part 2 Analysis of total and cause-specific mortality in relation to occupational exposure to
WCCo with analytic adjustment for potential confounding and/or effect modification by
smoking and co-exposures to known or suspected carcinogens including W, WC, C and Co
also with focus on cancer mortality and emphasis on lung cancer.
The cohort will include approximately 15,000 U.S. workers employed since 1950 at one or
more of included locations.
The racial, gender and ethnic characteristics of the study population reflect the
demographics of the areas surrounding the plants. No exclusion criteria will be based on
race, ethnicity, gender or HIV status.
Page 5 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
1
BACKGROUND AIMS AND OBJECTIVES
1.1
OBJECTIVE
Information gathered in a feasibility study shows that a scientifically rigorous and
comprehensive epidemiology study of workers employed in the manufacture or production
tungsten carbide with a cobalt binder (WCCo) is feasible and should include workers from
at 10 manufacturing sites in the United States and nine in Europe, including two from the
United Kingdom. This large epidemiology study, referred to as the Phase 3 study, will
represent multiple companies, countries and manufacturing processes and will be larger,
more robust and more definitive than any WCCo epidemiology study done to date.
1.2
SPECIFIC AIMS
The proposed historical cohort study is designed as an essential step in appraising the
health implications of occupational exposure to WCCo. The primary research objectives of
the Phase 3 study are:
1. To investigate the total and cause-specific mortality experience of current and
former workers potentially exposed to WCCo at multiple US and EU industrial sites
that produce(d) WCCo and/or manufacture(d) WCCo products, as compared with
the experience of the corresponding national and local populations from which the
workforces were drawn, with adjustment for potential confounding factors and with
emphasis on malignant neoplasms of the lung.
2. To characterize as completely as possible the past and current working
environment of the study members from the sites relative to work area, job
title/function and potential for exposure to WCCo as well as potential co-exposures
to several known or suspected human carcinogens including W, WC, C and Co.
3. To determine the relationship between level and duration of WCCo exposure and
mortality from malignant lung neoplasms with analytic adjustment to the extent
possible for potential co-exposures, including tobacco smoking habits.
4. To provide a framework for ongoing mortality surveillance of workers potentially
exposed to WCCo with and without concomitant co-exposures.
1.3
BACKGROUND
Several international health research agencies have recently acted to label tungsten
carbide with a cobalt binder (WCCo), also referred to as “hardmetal,” as a probable human
carcinogen. A review of the scientific basis for this decision reveals significant weaknesses
in the primary occupational epidemiologic studies of French and Swedish workers on which
it was based (Hogstedt and Alexandersson, 1990; Lasfargues et al., 1994; Moulin et al.,
1998; Wild et al., 2000).
To address these limitations, a 3-phase occupational
epidemiology investigation of workers employed in the tungsten carbide (WC) industry was
initiated in the early 2000’s by the International Tungsten Industry Association (ITIA).
Phase 1 of this investigation was a feasibility study conducted by BBL, Inc. in 2006 to
determine the availability and accessibility of company records needed for the main
epidemiology study that comprises Phase 3 of the investigation. The Phase 1 feasibility
study was extended and enhanced in Phase 2 by the University of Pittsburgh (UPitt) and
the University of Illinois at Chicago (UIC) under a research contract from ITIA. Phase 2,
Page 6 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
conducted from October 2007 through October 2008, allowed researchers: (1) to
communicate with plants directly to help clarify specific study needs; (2) to establish
communication avenues with key plant personnel and enabled those personnel to prepare
their facilities for inclusion in the Phase 3 study; (3) to apply different or additional feasibility
criteria to the data obtained in Phase 1 and (4) to establish parameters that created the
framework within which the Phase 3 study will proceed.
1.4
SIGNIFICANCE
Based on the conclusions of the feasibility study, sufficient demographic and WH data are
available to conduct an historical cohort mortality study of former and current workers with
potential exposure to WCCo at each of the study sites. Multiple sites were chosen to afford
better opportunities for contrasting cohort attributes, processes, work practices and
exposures; multiple sites also increases the likelihood of producing definitive and
informative conclusions by increasing the statistical power and the precision of the risk
estimates for detecting true excess risks overall and in relation to occupational factors.
Page 7 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
2 RESEARCH DESIGN AND METHODS
Investigators will first completely ascertain the cohort of workers with potential exposure to
WCCo (Research Objective 1). The University of Illinois at Chicago (UIC) will perform a
comprehensive exposure reconstruction of manufacturing processes and will develop task
and time-specific estimates of exposure (Research Objective 2). The exposure matrix will
enable UPitt investigators to construct summary measures of exposure to contaminants
(Research Objective 3) and enable ongoing mortality surveillance of the cohort (Research
Objective 4).
The historical cohort study will provide the epidemiological platform for the proposed
investigation, including a nested case-control study of lung cancer. The cohort study will
focus on mortality from lung cancer and other cause of death categories (including total
mortality).
2.1
STUDY INTERVENTIONS
UPitt under the direction of the Principal Investigator, Gary M. Marsh, Ph.D., and CoInvestigator, Jeanine M. Buchanich, Ph.D., will oversee all aspects of the study. For the
UK sites, work will be overseen by Damien McElvenny, Principal Epidemiologist at the
IOM.
2.2
TASK 1 – SITE COHORT ENUMERATION
The cohort will be enumerated by UPitt using all available corporate and plant-based
employee records; IOM will enumerate the two UK cohorts and make data available to
UPitt in a suitably anonymised form. The cohort will include active, terminated, retired and
deceased employees. To the extent possible, relevant cohort data will be derived initially
from records maintained by the companies in machine-readable format. To ensure that the
cohort enumeration is complete and accurate, IOM staff will also review all hard copy
employee records at the plants. Hard copy records will include work applications, detailed
job service records and death certificates. Scanners will be used to capture any cohort
data from the hard copy records.
The cohort enumeration will include four basic categories of employee data:
a. Data on personal identifiers and demographic factors (e.g., name, national
insurance number, national health service number, birth date, gender, pay
type and employment status)
b. Data on employment history and exposure (e.g., for each job held,
beginning and end dates, department, work area and job title, types and
levels of exposure (if known))
c. Data on health outcome (certification of death and cause of death)
d. Data on potential confounding factors (e.g., tobacco smoking history and
previous and subsequent employment)
Due to the variations in available cohort data, each plant will follow a unique protocol
during the cohort enumeration phase.
Page 8 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
These sites were chosen because they have been in operation long enough for a
meaningful epidemiological study (20+ years), have detailed work history available for all
employees who ever worked at the site and have had more than 500 employees
historically. Two UK sites will be included in the cohort enumeration for Part 1 of the Phase
3 study. The sites are the Sandvik plants at Coventry (hard metal production, powder
production) and Featherstone (pressing, green shaping, sintering, hard grinding, coating).
At the end of Task 1, IOM staff will have visited both of the two UK sites included in Part 1
of the Phase 3 study and collected all relevant demographic and work history data.
2.3
TASK 2 – DATA PROCESSING, VALIDATION AND MANAGEMENT
2.3.1
Electronic records
Electronic records will be supplied directly from the sites. A process for electronically
collecting data from each facility will be implemented to combine all data into single
relational database system housed on IOM’s secure servers, a copy of which will be
transferred, after appropriate anonymisation to UPitt colleagues. The electronic data will
be exported into a common data format, for example, an ASCII text file, a Microsoft Excel
file or a Microsoft Access database.
2.3.2
Hard copy records
Hard copy records will be produced from all scanned records. Hard copy records will be
processed by IOM clerical staff or, if the volume is sufficiently large, the scanning will be
subcontracted to an approved subcontractor. Abstracted data will be independently
double-entered and discrepancies resolved against source documentation. Separate data
files will be maintained according to the source of the data (e.g. payroll, pension, human
resources). Data from different sources will be merged onto the database once deemed to
have been accurately entered. If the data entry is outsourced, regular checks will be made
with the subcontractor on progress and accuracy of their work. The subcontractor staff will
sign appropriate confidentiality undertakings and when their work is complete, will provide
all the data collected to IOM and not retain any data on their own systems. They will be
asked to formally declare that they have complied with this. The method of transfer from
the subcontractor to IOM will be agreed in advance and will be secure, making appropriate
use of adequate encryption.
2.4
TASK 3 – VITAL STATUS TRACING
For the international analysis, the cohort’s vital status will be determined as of December
31, 2008 or a later date if deemed feasible. For the UK sites, it is likely that mortality data
will be complete to the end of 2010 or possibly 2011, depending on the timing of death
ascertainment for analysis. All identified employees will be sent for tracing at the National
Health Service Central Register (NHSCR) in Southport. IOM will be notified of workers that
have died, embarked or are untraceable on the NHSCR.
2.5
TASK 4 – INTEGRATION OF EXPOSURE DATA
UPitt investigators will work closely with UIC investigators to coordinate the integration and
verification of data from the epidemiological and exposure assessment components of the
study. This will involve linking the job/exposure matrix (JEM) created by UIC investigators
with the individual WHs and epidemiological data compiled by the UPitt investigators and
Page 9 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
exposure analysis provided by each unit. The JEM will be standardised based on the
consensus between participating units so that the relevant parts can be shared with
participating units for their analysis. UPitt will also serve as a clearing house for all
exposure assessment-related study data, and will be responsible for maintaining an
inventory and ultimately an archive of all project data. UIC/UPitt will make the relevant part
of the job/exposure matrix for the UK sites available to IOM researchers so that a UK
analysis can be undertaken in a way that is consistent with the international analysis.
2.6
STATISTICAL ANALYSIS
The following section applies to the statistical analysis plan for the entire Phase 3 study.
Because the recommended study sites are highly diverse relative to geographic location,
cohort size and cohort entry period (facility start date in most cases), we propose to
approach the statistical analysis in a site-specific manner, pooling data across sites only if
warranted by evidence of sufficient homogeneity. The advantage of such diversity from an
epidemiological standpoint is the ability to assess the consistency of our findings across
the study populations. Efforts will be made to pool data when warranted, however, as this
will improve the precision of the mortality risk estimates and increase the statistical power
to detect epidemiologically important excess risks. A separate analysis will be undertaken
for each of the two UK plants, and if appropriate, for the two plants combined.
Our statistical analysis of the study data will consist of two major parts, each of which is
designed to address specific objectives of the study:
Part 1 Analysis of total and cause-specific mortality patterns in relation to basic
demographic and work history factors (e.g., study site, race, gender, age, calendar
time, year of hire, duration of employment and the time since first employment),
with focus on cancer mortality and emphasis on the implicated site of interest
(lung).
Part 2 Analysis of total and cause-specific mortality in relation to occupational exposure to
WCCo with analytic adjustment for potential confounding and/or effect modification
by smoking and co-exposures to known or suspected carcinogens including W,
WC, C and Co also with focus on cancer mortality and emphasis on lung cancer.
Part 1 will include a descriptive analysis of externally standardized mortality ratios (SMRs),
with SMRs based on both national and local standard population death rates (for the UK,
this will be for England and Wales and the West Midlands, respectively). The descriptive
phase of the analysis is useful for examining the basic structure and consistency of the
overall and study factor-specific mortality risks and for determining appropriate cutpoints for
categorizing continuous study variables.
Part 2 will include multi-variablee analyses of internal cohort rates to facilitate the
simultaneous adjustment for multiple potential confounding factors and the assessment of
effect modification among two or more study factors. In particular, Part 2 will include
relative risk regression modeling (based on Cox proportional hazards model) of internal
cohort rates.
The modeling of internal cohort rates provides mortality comparisons within the cohort that
are unbiased by the “healthy worker effect” associated with external general population
comparisons. The scope of the multi-variable analysis for lung cancer mortality will be
determined largely by the corresponding number of observed deaths and their factor-
Page 10 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
specific distributions. In addition, we may need to limit certain statistical analyses to
subgroups with sufficiently large numbers of observed deaths (e.g., white males).
3 HUMAN SUBJECTS
3.1
GENERAL CHARACTERISTICS
The UK cohort will include between 1000 and 2000 workers employed since 1950 at one of
the two UK factories.
The socioeconomic status of the study population is likely to reflect the demographics of
the area surrounding the plants (the West Midlands). No exclusion criteria will be based on
gender or length of employment. Contract staff may have to be excluded if details are not
held at the factories concerned.
3.2
INCLUSION/EXCLUSION CRITERIA
Only those employees who were working in 1950 or hired later will be included in the study.
Those employees who ended their employment prior to 1950 will be excluded. There is a
possibility that some contract workers may be excluded.
3.3
IDENTIFYING SUBJECTS
All workers employed by Sandvik or its predecessor at one of the two factories beginning in
1950 or 1966 (depending which plant) will be included in the study.
3.4
ETHICAL CLEARANCE AND INFORMED CONSENT
Ethical clearance for the UK component of this study will be sought from an appropriate
NHS research ethics committee in the West Midlands. In addition exemption from having
to gain informed consent for the cohort study from current and former members of the
workforces will be sought. There may be an expectation that presentations may have to be
made to the current workforce about the proposed study, allowing current workers to optout of the study if they so wish (from the National Information Governance Board and/or the
management or workforce representatives). Trades Unions or routes of publicising the
study may have to be utilised to bring the study to the attention of former employees.
For the case-control study, informed consent will need to be obtained for all participants (or
their proxies). These participants may have to be approached via their General
Practitioners (GPs). It is anticipated that a small payment may be made to GPs to facilitate
this, and that those who are interviewed are compensated for their expenses. The
existence of the study may be advertised in advance to potentially relevant GP practices;
advice on this will be sought from the Medical Research Information Service. Advice will
also be sought as to whether ethical clearance for the case-control study should be sought
separately from that for the case-control study, or it be sought at the same time.
Page 11 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
4 POTENTIAL RISKS
Although every effort will be made to ensure the confidentiality of subject data, study
members are subject to the risk of a breach of confidentiality.
4.1
CONFIDENTIALITY
All data relating to the study will be kept confidential and any statistical analyses carried out
will be done so using a pseudonymised data set. Any data transferred to UPitt and/or UIC
for the international analysis will also be via a pseudonymised data set. All electronic data
held by IOM will be on a secure server and in full accordance with IOM’s system level
security policy. This policy will be subject to the scrutiny of that National Information
Governance Board’s Security Review Team. All paper records will be held in lockable
cabinets only accessible by named researchers involved with the study. Any data that is
published will be done in such a way that individuals cannot be identified.
4.2
POTENTIAL BENEFITS
As will all studies of this type, individual subjects will not directly benefit from participation
but workers exposed to tungsten carbide and society as a whole will potentially benefit
from the knowledge garnered in this study.
4.3
DATA AND SAFETY MONITORING PLAN
Data collection procedures and policies, vital status tracing progress and confidentiality
assurances will be monitored. Study guidelines regarding patient confidentiality are strictly
enforced and will also be reviewed quarterly to determine potential improvements.
Page 12 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
5 COSTS AND PAYMENTS
5.1
RESEARCH STUDY PAYMENTS
No research subject will be charged nor paid to be a participant in this study, although GPs
may be paid a small fee to pass on details of the study to potential participants and
participants may be paid a small fee for expenses and inconvenience.
5.2
QUALIFICATIONS OF INVESTIGATORS
The Principal Investigator will be Gary M. Marsh, Ph.D. who has over 20 years of
experience in biostatistical and epidemiological research. Dr. Marsh is a Professor of
Biostatistics, Graduate School of Public Health and will supervise, coordinate and oversee
all aspects of the core support program, and will play a major role in the annual mortality
analyses and preparation of reports.
Jeanine M. Buchanich, Ph.D., Research Assistant Professor of Biostatistics and Deputy
Director of Epidemiology for the Center for Occupational Biostatistics and Epidemiology
(COBE) at the Graduate School of Public Health, University of Pittsburgh will serve as a
Co-Investigator. Dr. Buchanich has more than 10 years experience in occupational health
research and has served as project coordinator on numerous projects. She has authored
more than 25 occupational health articles appearing in the peer-reviewed literature.
A second co-investigator of the proposed project is Ada O. Youk, Ph.D., Research
Assistant Professor of Biostatistics. Dr. Youk will have primary responsibility for
coordinating the analytical aspects of the core support program including the construction
of standard rate files and the annual mortality analyses. She will also play a major role in
the preparation of progress reports and scientific publications.
The lead investigator for the UK component of this study is Professor Damien McElvenny
BSc(Hons), MSc, CStat, principal epidemiologist at IOM. Damien has over 25 years of
experience in occupational health research and has been first-named author on several
peer-reviewed scientific papers, and over 30 papers in total.
5.3
SOURCES OF SUPPORT
This study is being funded under subcontract from the International Tungsten Industry
Association via the University of Pittsburgh.
Page 13 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
6 REFERENCES
Breslow NE, Day NE. The design and analysis of cohort studies. In: Statistical Methods in
Cancer Research, Vol. II. International Agency for Research on Cancer. Lyon, France:
IARC Scientific Publications No. 82, 1987.
Buchanich JB, Dolan DG, Marsh GM, Madrigano J. Under ascertainment of deaths using
Social Security records: A recommended solution to a little-known problem. Am J
Epidemiol 162:193-194, 2005.
Cox DR. Regression models and life tables (with discussion). J R Stat Soc 34B:187-220,
1972.
Cox DR. Partial likelihood. Biometrika 62:269-276, 1975.
Doll R. Occupational cancer: A hazard for epidemiologists. Int J Epidemiol 14:22-31,
1985.
Esmen NA.
industry.
Exposure estimation in four major epidemiologic studies in acrylonitrile
Scand
J
Work
Env
Hea
24:Sup2:63-70,
1998.
Esmen NA, Kennedy KJ, Hall TA, Phillips ML, Marsh GM.
exposures. Chem-Biol Interact 166:245-253, 2007a.
Classification of worker
Esmen NA, Hall TA, Phillips ML, Marsh GM. Chemical process based reconstruction of
exposures for an epidemiological study: I. Theoretical and methodological issues. ChemBiol Interact 166:254-263, 2007b.
Esmen NA, Hall TA, Phillips ML, Jones EP, Basara H, Marsh GM, Buchanich JM.
Chemical process based reconstruction of exposures for an epidemiological study: II.
Estimated exposures to chloroprene and vinyl chloride. Chem-Biol Interact 166:264-276,
2007c.
Hogstedt C, Alexandersson R. Mortality among hard metal workers. Arbete Hälsa, 21, 126, 1990.
IARC. Monographs on the evaluation of carcinogenic risks to humans. Volume 86, Cobalt
in hard metals and cobalt sulfate, Lyon, France, 2006.
Lasfargues G, Wild P, Moulin JJ, Hammon B, Rosmorduc B, Rondeau du Noyer C,
Lavandier M and Moline JJ. Lung cancer mortality in a French cohort of hard-metal
workers. Am J Ind Med 26:585-595, 1995.
Marsh GM, Youk AO, Stone RA, Sefcik S, Alcorn CW. OCMAP-PLUS, A new program for
the comprehensive analysis of occupational cohort data. J Occup Environ Med 40:351362, 1998.
Marsh GM, Youk AO, Stone RA, Buchanich JM, Gula MJ, Smith TJ, Quinn MM. Historical
cohort study of US man-made vitreous fiber production workers: I. 1992 fiberglass cohort
follow-up: initial findings. J Occup Environ Med 43:741-756, 2001.
Page 14 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
Marsh GM, Ehland J, Sefcik S, Alcorn C. Mortality and population data system (MPDS).
Pittsburgh, PA: University of Pittsburgh (Department of Biostatistics Technical Report),
2005.
Marsh GM, Youk AO, Buchanich JM, Cunningham M, Esmen NA, Hall TA, Phillips ML.
Mortality patterns among industrial workers exposed to chloroprene and other substances.
I. General mortality patterns. Chem-Biol Interact 166: 285-300, 2007a.
Marsh GM, Youk AO, Buchanich JM, Cunningham M, Esmen NA, Hall TA, Phillips ML.
Mortality patterns among industrial workers exposed to chloroprene and other substances.
II. Mortality in relation to exposure. Chem-Biol Interact 166:301-316, 2007b.
Moulin JJ, Wild P, Mur JM, Fournier-Betz M, Mercier-Gallay M. A mortality study of cobalt
production workers: An extension of the follow-up. Am J of Ind Med 23:281-288, 1993.
Moulin JJ, Wild P, Romazini S, Lasfargues G, Peltier A, Bozec C, Deguerry P, Pellet F,
Perdrix A. Lung cancer risk in hard metal workers. Am J Epidemiol 148:241-248, 1998.
Mur JM, Moulin JJ, Charruyer-Seinerra MP, Lafitte J. A cohort mortality study among
cobalt and sodium workers in an electrochemical plant. Am J Ind Med 11:75-81, 1987.
Phillips ML, Esmen NA. Computational method for ranking task-specific exposures using
multi-task time-weighted average samples. Ann Occup Hyg 43:201-213, 1999.
Santhanam AT.
Cemented carbides.
In: Kirk-Othmer Encyclopedia of Chemical
Technology, Vol. 4, 4th Ed. Ed. Kroschwitz JI and Howe-Grant M. New York: John Wiley
& Sons, 1992.
STATA Statistical Software: Release 11.0. College Station, TX, STATA Corp., 2009.
Wild P, Perdix A, Romazini S, Moulin JJ, Pellet F. Lung cancer mortality in a site
producing hard metals. Occup Environ Med 57:568-573, 2000.
Youk AO, Marsh GM, Stone RA, Buchanich JM, Smith TJ. Historical cohort study of U.S.
man-made vitreous fiber production workers III: Analysis of exposure-weighted measures
of respirable fibers and formaldehyde in the nested case-control study of respiratory
system cancer. J Occup Environ Med 43:767-778, 2001.
Youk AO, Buchanich JM, Marsh GM, Cunningham MC, Esmen NE. Pharmaceutical
production workers and the risks of mortality from respiratory system cancer and lymphatic
and hematopoetic tissue cancers. J Occup Environ Med 51:903-915, 2009.
Page 15 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
7 APPENDIX 1 – RESEARCH
INTERNATIONAL STUDY
7.1
PROPOSAL
FOR
THE
BACKGROUND
Tungsten carbide (WC) is the most common of the hard metals, materials formed by
binding or cementing metallic carbides with a soft and ductile metal binder (IARC, 2006),
usually cobalt or nickel. Hard metals are manufactured by a powder metallurgy process
consisting of a sequence of carefully-controlled steps designed to obtain a final product
with specific properties, microstructure and performance (Santhanam, 1992). Several
international health research agencies, including the International Agency for Research on
Cancer (IARC, 2006), have recently acted to label WC with a cobalt binder (WCCo) as a
probable human carcinogen (category 2A). IARC ruled there was limited evidence in
humans and sufficient evidence in animals that WCCo acted as a lung carcinogen (IARC,
2006).
A review of the scientific basis for this decision revealed significant weaknesses in the
primary occupational epidemiologic studies of French and Swedish workers on which it
was based (Hogstedt and Alexandersson, 1990; Lasfargues et al., 1995; Moulin et al.,
1998; Wild et al., 2000). Three of the four epidemiological studies were not mutually
independent (Lasfargues et al., 1995; Moulin et al., 1998; Wild et al., 2000). The four
epidemiological investigations also shared limitations which negatively impacted their
interpretability, including: poorly defined exposure assessments; inconsistent and
ambiguous smoking histories and classification; a lack of regional mortality comparisons; a
lack of internal cohort rate comparisons; and incomplete job histories. To address these
limitations, a 3-phase, international occupational epidemiology investigation of workers
employed in the tungsten carbide (WC) industry was initiated in the early 2000’s by the
International Tungsten Industry Association (ITIA).
7.1.1
Phase 1
Phase 1 of this investigation was a feasibility study conducted by BBL, Inc. in 2006 to
determine the availability and accessibility of company records needed for the main
epidemiology study that comprises Phase 3 of the investigation. The Phase 1 feasibility
study was extended and enhanced in Phase 2 by the University of Pittsburgh (UPitt) and
the University of Illinois at Chicago (UIC) under a research contract from ITIA.
7.1.2
Phase 2
In Phase 2, conducted from October 2007 through October 2008, UPitt and UIC developed
and applied several criteria for a candidate site to be included in the Phase 3 study,
including a minimum size of 100 or more employees historically for United States (US)
sites and 500 or more employees historically for European (EU) sites. Sites also had to
have been producing WCCo or WC products since at least 1980 to allow an adequate
latency period for disease development.
Additionally, detailed work history (WH)
information had to be available for all employees who ever worked at the facility. The last
consideration, for non-US sites, was whether vital status tracing was possible within that
country. This information was gathered via the telephone survey and/or during a site visit.
The study questionnaire used in the telephone survey had separate epidemiology and
industrial hygiene components and was administered by a professional interviewer on the
Page 16 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
UPitt staff. Surveys were completed in April 2008. Following the surveys, UPitt and UIC
investigators conducted four US and two EU site visit trips that included a total of 18 sites
during the Phase 2 study. The sites visited were representative of the candidate sites with
respect to country, company and process.
A final report on the results of the Phase 2 enhanced feasibility study was submitted to ITIA
in November 2008 (Marsh et al., 2008). The Phase 2 report, which also included a draft
protocol for the Phase 3 study, showed that a scientifically rigorous and comprehensive
epidemiology study of hardmetal workers was feasible and should include workers from
nine manufacturing sites in the US and nine manufacturing sites in EU including sites in
Austria (AT), England (UK), Germany (DE) and Sweden (SE). Since the submission of the
Phase 2 report, one company (ATI) chose to withdraw from the study, requiring us to
replace two ATI plants with three plants owned by Kennametal. This brings the total
number of plants in the US portion of the study to 10.
To ensure that the data collected from all US and EU can be combined ultimately for
purposes of a pooled cohort data analysis, the Phase 3 protocol includes strict provisions
for maintaining a common data collection and statistical analysis protocol. UPitt and UIC
are responsible for coordinating these activities during the course of Phase 3.
7.1.3
Phase 3
7.1.3.1 US Component
In 2009, UPitt and UIC began limited work on the US portion of the Phase 3 epidemiology
study under a grant from the Pennsylvania State Department of Health (PADOH). This
work, termed Part 1 of the Phase 3 study, involves the collection and processing of
relevant study data (demographic, work history and industrial hygiene data) from several of
the US manufacturing sites and represents the first step to enumerating the US study
population. Prior to data collection, the two participating companies in the US study,
Sandvik and Kennametal, notified their employees of their possible inclusion in the
historical cohort study. Table 1 shows the progress of the 10 sites participating in the US
portion of the study.
Page 17 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
Table A.1: Progress of US Sites Included in Tungsten Carbide Workers Study
Site (Company)
Company
Employee
Notification
Site Tour
Work History
(WH) Data
Collection
WH Data
Processing
IH Data
Collection
IH Data
Processing
Asheboro, NC
(Kennametal)
Completed
Not Done
Not Done
Not Done
Not Done
Not Done
Bedford, PA
(Kennametal)
Completed
Completed
Completed
Ongoing
Completed
Not Done
Irwin, PA
(Kennametal)
Completed
Completed
Not Done
Not Done
Not Done
Not Done
Fallon, NV
(Kennametal)
Completed
Completed
Mostly
completed
Ongoing
Completed
Not Done
Henderson, NC
(Kennametal)
Completed
Completed
Completed
Completed
Completed
Not Done
Johnson City, TN
(Kennametal)
Completed
Completed
Completed
Not Done
Completed
Not Done
Completed
Completed
Completed
Completed
Completed
Not Done
Completed
Completed
Completed
Ongoing
Completed
Not Done
Traverse City, MI
(Kennametal)
Completed
Not Done
Not Done
Not Done
Not Done
Not Done
West Branch, MI
(Sandvik)
Completed
Completed
Completed
Completed
Completed
Not Done
Orwell, OH
(Kennametal)
Roanoke
Rapids,
NC
(Kennametal)
Page 18 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
7.1.3.2 EU Component
In 2010, data collection activities began at the Reutte, AT site owned by the Ceratizit
Company; the AT study is being directed by Dr. Manfred Neuberger. Due to lack of
funding, none of the other country-specific investigations has begun. The current proposal
includes funding for these investigations. Table 2 shows the status of the nine plants
participating in the EU component of the study.
Table A.2: Progress of EU Sites Included in Tungsten Carbide Workers Study
Site (Company)
Company
Employee
Notification
Site Tour
Work History
(WH) Data
Collection
WH Data
Processing
IH Data
Collection
IH Data
Processing
Fagersta, Sweden
(Sandvik)
Not Done
Completed
Not Done
Not Done
Not Done
Not Done
Gimo, Sweden
(Sandvik )
Not Done
Completed
Not Done
Not Done
Not Done
Not Done
Stockholm, Sweden
(Sandvik)
Not Done
Completed
Not Done
Not Done
Not Done
Not Done
Coventry, England
(Sandvik)
Not Done
Completed
Not Done
Not Done
Not Done
Not Done
Featherstone,
England (Sandvik)
Not Done
Completed
Not Done
Not Done
Not Done
Not Done
Mistelgau, Germany
(Kennametal)
Not Done
Completed
Not Done
Not Done
Not Done
Not Done
Not Done
Completed
Not Done
Not Done
Not Done
Not Done
Not Done
Completed
Not Done
Not Done
Not Done
Not Done
Unknown
Completed
Underway
Underway
Underway
Underway
Ebermannstadt,
Germany
(Kennametal)
Essen,
Germany
(Kennametal)
Reutte, Austria
(Ceratizit)
7.2
SIGNIFICANCE OF PHASE 3 STUDY
The Phase 3 historical cohort study was designed to overcome the methodological
limitations of earlier studies by including a rigorous exposure assessment component, a
nested case-control study of lung cancer cases and matched controls to obtain smoking
information and the use of external and internal cohort rate comparisons. The Phase 3
study, which will represent multiple sites and manufacturing processes, will be larger, more
robust and more definitive than any WCCo epidemiology study done to date.
Our preliminary data collection revealed that five main exposure agents should be
evaluated and compared for potential adverse health effects: tungsten (W), WC, WCCo,
carbon black (C) and cobalt (Co). Our large cohort size will involve more person-years
than any previous study of tungsten carbide workers, giving us greater power when
examining exposure contrasts and industry subsections. The large number of lung cancer
Page 19 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
deaths we expect to observe in the cohort study includes a surplus number of deaths
sufficient for maintaining good to excellent statistical power while accounting for the
additional sample size requirements needed to assess confounding and effect modification.
This study will test the hypotheses that: 1) Co in the presence of WC is a carcinogen; 2)
smoking explains the excess; 3) C, a suspected lung carcinogen, is associated with the
excess; 4) Co alone is associated with the excess. If only hypothesis (2) is rejected and
the lung cancer excess is corrected for smoking, then the project presents an opportunity
to develop a carcinogenic index for the combination of three carcinogenic co-exposures.
Potential candidates for such an index range from weighted linear combination of
exposures to exposure matrices that consider different lag times for each toxicant. The
validation and use of the exposure index requires outcome data, which in turn requires the
completion of the initial analyses. Even though it may not move from the theoretical
development phase, we plan to consider the necessary theoretical and mathematical
aspects of this problem and propose solutions as part of the study.
7.3
PHASE 3 STUDY - PRIMARY RESEARCH OBJECTIVES
The proposed historical cohort study is designed as an essential step in appraising the
health implications of occupational exposure to WCCo. The primary research objectives of
the Phase 3 study are:
1. To investigate the total and cause-specific mortality experience of current and
former workers potentially exposed to WCCo at multiple US and EU industrial
sites that produce(d) WCCo and/or manufacture(d) WCCo products, as
compared with the experience of the corresponding national and local
populations from which the workforces were drawn, with adjustment for potential
confounding factors and with emphasis on malignant neoplasms of the lung.
2. To characterize as completely as possible the past and current working
environment of the study members from the sites relative to work area, job
title/function and potential for exposure to WCCo as well as potential coexposures to several known or suspected human carcinogens including W, WC,
C and Co.
3. To determine the relationship between level and duration of WCCo exposure and
mortality from malignant lung neoplasms with analytic adjustment to the extent
possible for potential co-exposures, including tobacco smoking habits, via
internal adjustment with a nested case-control study or external adjustment with
a Monte Carlo sensitivity analysis.
4. To provide a framework for ongoing mortality surveillance of workers potentially
exposed to WCCo with and without concomitant co-exposures.
The epidemiology component of the Phase 3 study will be complemented by a
comprehensive and rigorous exposure assessment component conducted by UIC
(Research Objective 2 above). The primary research objectives of the exposure
reconstruction component are:
1. To generate scientifically sound estimates of exposure to WCCo and other potential
carcinogens for all job and/or task categories on a site-specific and time-dependent
basis. Average and cumulative exposure metrics will be developed and adjusted
for country, company and site variability linearly. The interaction between company
and country will also be tested.
Page 20 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
2. To create exposure classes for subsequent statistical analysis in the epidemiology
component of the study.
3. To assess the robustness of the exposure reconstruction models employed with
respect to uncertainties arising from data gaps and inherent variability.
7.4
PHASE 3 STUDY - PROPOSED EPIDEMIOLOGIC STUDY DESIGN
This section includes a summary of the key aspects of the proposed study design. We
provide more details about our study design, including the proposed exposure
reconstruction, in our detailed Phase 2 report and Phase 3 study protocol included as
Appendix A to this document (Marsh et al., 2008).
7.4.1
Historical Cohort Study
Based on the conclusions of the Phase 1 and 2 studies, sufficient demographic and WH
data are available to conduct an historical cohort mortality study of former and current
workers with potential exposure to WCCo at each of the study sites. Multiple sites were
chosen to afford better opportunities for contrasting cohort attributes, processes, work
practices and exposures; multiple sites also increases the likelihood of producing definitive
and informative conclusions by increasing the statistical power and the precision of the risk
estimates for detecting true excess risks overall and in relation to occupational factors.
As underway for the US sites in Part 1 of the Phase 3 study, UIC and UPitt investigators
will first completely ascertain the cohort of workers with potential exposure to WCCo
(Research Objective 1). UIC will perform a comprehensive exposure reconstruction of
manufacturing processes and will develop task and time-specific estimates of exposure
(Research Objective 2). The exposure matrix will enable UPitt investigators to construct
summary measures of exposure to contaminants (Research Objective 3) and enable
ongoing mortality surveillance of the cohort (Research Objective 4).
The historical cohort study will provide the epidemiological platform for the proposed
investigation, including a nested case-control study of lung cancer. The cohort study will
focus on mortality from lung cancer and other cause of death categories (including total
mortality).
7.4.2
Nested Case-Control Study
Adjustment for potential confounding by smoking will occur primarily through nested casecontrol studies conducted in most countries (AT, SE, US or UK) or, in DE, via external
adjustment. The nested case-control study of lung cancer can be considered as a special
case of the corresponding relative risk regression analysis. That is, for each case (death)
due to lung cancer identified in the cohort, we will randomly select a group of matched
controls from the corresponding risk set formed for the relative risk regression analysis.
The non-case members of each risk set are matched on the exact event (death) age of the
case, gender and year of birth (caliper-matched as tightly as possible). We will select two
controls for each case.
To obtain more detailed or otherwise unavailable information on potential risk factors for
the cases and controls, an attempt will be made to locate and interview a knowledgeable
informant, ideally the worker himself or a surviving member of the worker’s immediate
family (proxy respondent). Potential informants will be instructed to return the consent form
within two weeks of the date of the letter indicating their willingness to participate. Willing
Page 21 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
informants will be contacted by a professional interviewer for a brief (20-30 minute)
telephone interview concerning such items as the subject’s smoking, non-occupational and
occupational history. The case-control study questionnaire proposed for this study will be
based upon the one already used in a nested case-control study of lung cancer among
workers with potential exposure to man-made vitreous fibers. We will modify the existing
instrument as necessary to capture specific risk factors of interest for WCCo workers.
7.4.3
Exposure Reconstruction
The basic exposure model is job class (a), task (b) and year (y) normalized exposure levels
adjusted for country (X1), company (X2) and location (X3). In specific terms the
fundamental linear adjustments to exposure levels with country by company interaction
may be expressed as:
E (a, b, y ) o (a, b, y ) country X 1 company X 2 site X 3 countryCompany X 1 X 2
where
, E , 0 f (a, b, y0 ) or g (a, b, )
for country, company and site calculations.
At this point, we do not know whether exposure values near the start-up (y0) can be found
or whether an asymptotic value (y=∞) for exposure can be determined. Between start-up
based or asymptotic functions which define the exposure and coefficients, we shall choose
the function that is convenient and/or tractable. That formulation will be used consistently
to adjust for the time decline of exposures first with the simplifying assumption that the
exposure matrix is multiplied by a scalar function of time. If this approach does not provide
reasonable results, then more complicated solutions will be sought. Once this function is
determined, all deterministic or empirical models will be adjusted using this relationship.
The general exposure reconstruction process and the steps that may be involved in this
process have been summarized in Table 3 below. Clearly, while some of the steps are
sequential, many of the process steps are concurrent. It should be noted that while much
of the methodology is written in general terms, the evaluation of each facility is
independent. Some of the information shown in the table will be collected on an as-needed
basis and some of the operations will be carried out on an as-required basis. The general
approach is the least complicated path without sacrificing rigor. In order to aggregate the
cohort across plants, the determinants of exposure will be adjusted to account for the
differences in operations from one facility to another using the empirically modeled
correction shown above.
Table A.3: Summary of Exposure Reconstruction Method
1. Selected process information collection
a. Process operation documents
b. Facility layouts and plans
c. Technical memos and other sources
d. General annual production records
2. Exposure information collection
a. All (occupational) IH monitoring data, including area and personal exposure
sampling data
b. Documentation pertaining to
Page 22 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
i.
ii.
iii.
iv.
v.
Sampling
Administrative orders
Environmental exposure monitoring
Occupational hygiene inspection reports
Occupational health reports filed to or by regulatory agencies (as
applicable)
3. Selected job and task identification
a. Job descriptions as written in company records
b. As described by experienced persons (as needed)
4. Projection of results backwards through time from contemporary data (as needed)
5. Operations analysis of the production processes
6. Mathematical modeling of the information gathered above
7. Verification of models from extant data
8. Generation of task-based exposures
9. Construction of a site-specific job/exposure matrix detailing exposures for each job
title (or group of job titles) as a function of specific agents and appropriate time
intervals
7.5
PHASE 3 STUDY- STATISTICAL ANALYSIS PLAN
This section includes a summary of the key aspects of the proposed statistical analysis.
We provide more details about our study design, including the proposed exposure
reconstruction, in our detailed Phase 2 report and Phase 3 study protocol included as
Annex A to this document (Marsh et al., 2008).
Because the recommended US/EU study sites are highly diverse relative to geographic
location, cohort size and cohort entry period (facility start date in most cases), we propose
to approach the statistical analysis in a site-specific manner, pooling data across sites only
if warranted by evidence of sufficient homogeneity. The advantage of such diversity from
an epidemiological standpoint is the ability to assess the consistency of our findings across
the study populations. Efforts will be made to pool data when warranted, however, as this
will improve the precision of the mortality risk estimates and increase the statistical power
to detect epidemiologically important excess risks.
Our statistical analysis of the study data will consist of two major parts, each of which we
designed to address specific objectives of the study:
Part 1 Analysis of total and cause-specific mortality patterns in relation to basic
demographic and work history factors (e.g., study site, race (US sites), gender, age,
calendar time, year of hire, duration of employment and the time since first
employment), with focus on cancer mortality and emphasis on the implicated site of
interest (lung).
Part 2 Analysis of total and cause-specific mortality in relation to occupational exposure to
WCCo with analytic adjustment for potential confounding and/or effect modification
Page 23 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
by smoking and co-exposures to known or suspected carcinogens including W,
WC, C and Co also with focus on cancer mortality and emphasis on lung cancer.
Part 1 will include a descriptive analysis of externally standardized mortality ratios (SMRs),
with SMRs based on both national and local standard population death rates. The
descriptive phase of the analysis is useful for examining the basic structure and
consistency of the overall and study factor-specific mortality risks and for determining
appropriate cutpoints for categorizing continuous study variables.
Part 2 will include multi-variable analyses of internal cohort rates to facilitate the
simultaneous adjustment for multiple potential confounding factors and the assessment of
effect modification among two or more study factors. In particular, Part 2 will include
relative risk regression modeling (based on Cox proportional hazards model) of internal
cohort rates.
The modeling of internal cohort rates provides mortality comparisons within the cohort that
are unbiased by the “healthy worker effect” associated with external general population
comparisons. The scope of the multi-variable analysis for lung cancer mortality will be
determined largely by the corresponding number of observed deaths and their factorspecific distributions. In addition, we may need to limit certain statistical analyses to
subgroups with sufficiently large numbers of observed deaths (e.g., white males).
To provide the most unbiased assessment of lung cancer risk possible from the available
study data, we have included in Part 2 a nested case-control study of lung cancer in the
AT, SE, UK and US sites. As described above, we will make an intensive effort to obtain
the most complete and accurate individual worker-level data on tobacco smoking habits for
all cases (deaths) of lung cancer and corresponding groups of non-cases (controls)
selected at random from the remaining cohort members. In the DE sites, we will control for
potential confounding by smoking via external adjustment.
While we plan to collect smoking information to the extent possible on all study members,
these data may be incomplete. By performing this adjustment in the case-control setting
we will be more likely to have complete data on smoking as most of the cases and
corresponding controls will fall into the later time periods when these data are more
complete. The statistical analysis of the case-control data will involve relative risk
regression modeling of the matched sets with adjustment for potential confounding by
smoking and co-exposures to several known or suspected carcinogens.
7.6
PHASE 3 STUDY - STRENGTHS AND LIMITATIONS
The strengths of the proposed study can be summarized as follows:
1. The study represents the joint efforts of a nationally and internationally recognized
occupational health research team with more than 30 years of experience designing
and conducting historical cohort and case-control studies of the types proposed
herein, including the largest occupational cohort, incidence and case-control study
of brain cancer ever conducted.
2. The UIC and UPitt investigators share a long history of highly successful and
productive collaborative research, as evidenced by the many jointly authored peerreviewed publications cited in their respective curricula vitae.
3. The proposed historical cohort study design and nested case-control study of lung
cancer, which will enable analytic adjustments for smoking and co-exposures to
Page 24 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
known or suspected carcinogens, will provide the best available estimates of total
and cause-specific mortality risks among workers, overall, and in relation to
occupational WCCo exposure.
4. A particular strength of this study is the ability to characterize the working history of
study members relative to WCCo exposure and co-exposures to other known or
suspected carcinogens. The UIC exposure assessment team plans to use a variety
of statistical and other estimation methods to assign meaningful and scientifically
defensible exposure estimates to workers over time.
5. Based on our estimates, the statistical power of the proposed cohort study to detect
epidemiologically important (1.5-fold or greater) overall excesses in all cancers
combined and in lung cancer is essentially 1.0. The study affords a sufficiently long
time period for potential WCCo exposure and a sufficiently long observation period
to observe cancer outcomes in relation to WCCo exposure. Therefore, our
proposed study is able to detect a true increased risk or to conclude that there is no
increased risk if one is not detected. Additionally, because the number of expected
cancers is so large, the power necessary to detect 1.5 fold or greater risks in larger
subgroups of the cohort will also be in the good to excellent range.
6. Also based on our independent estimates, the power of the nested case-control
study of lung cancer to detect epidemiologically important (1.5-fold or greater)
excesses in relation to key study factors is in the excellent range (95% or greater).
This focused sub-study will also allow adjustment for potential confounding by
smoking in addition to co-exposures to known or suspected carcinogens.
7. The addition of Co production companies to the study would be a large advantage
of the Phase 3 study over previous studies of WCCo workers. However, the
inability to include subjects with Co-only exposure does not represent a fatal flaw to
the main study design. The Phase 3 WCCo worker epidemiology study will be
comprehensive, scientifically sound and far superior overall to the existing
epidemiology studies. The limited orthogonal contrasts for Co and WC simply
suggests that we may be unable to sort out completely the contribution of each
exposure alone if increased lung cancer mortality risks are observed among
subjects with combined exposures.
8. The historical cohort study can form the basis for ongoing mortality surveillance of
the workers with potential occupational exposure to WCCo.
The limitations of the proposed study can be summarized as follows:
1. Although it appears from the Phase 1 and Phase 2 studies that much of the data
necessary to adequately address the question regarding WCCo exposure and lung
cancer exists, we may find that some records are unavailable. We believe,
however, that we have taken every reasonable approach to resolve or work around
these limitations in designing the proposed study.
2. Although the cohort study has good to excellent statistical power to detect important
excesses in mortality from all cancers combined and lung cancer in the total cohort
and its larger subgroups, the power will be less to detect excesses in smaller
subgroups of the total study population, such as factor-specific groups within study
site. The same feature will also apply to the case-control study.
Page 25 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
3. Because a large and diverse number of agents are used or produced at the plants,
it may not be possible to identify the specific etiologic agent or combination of
agents if an overall excess in cancer mortality is found. This is a limitation of all
epidemiology studies of this type that attempt to relate mortality outcomes to
specific chemical exposures. We have, to the extent possible, designed all aspects
of our study to offset or mitigate this limitation.
4. The use of external adjustment for confounding by smoking in the DE sites has
some limitations. Although we will attempt to estimate the patterns of smoking
among WCCo exposed workers from information available in the peer-reviewed
literature, there remains the chance that these estimates are not truly
representative of the smoking prevalence in the worker cohorts. The smoking rates
will most likely be based only on one time period which would not reflect temporal
changes in smoking habits which can occur, particularly over the long duration of an
historical cohort study. We may also be limited by the extent to which detailed
smoking information is available in the literature.
5. On balance, we believe that the strengths of the proposed study outweigh its
weaknesses. We are also confident that our investigation will produce scientifically
sound, meaningful and defensible results, and will provide a significant contribution
to the body of knowledge concerning the health implications of exposure to WCCo.
7.7
QUALIFICATIONS OF THE RESEARCH TEAMS
7.7.1
University of Pittsburgh
For more than 45 years, the UPitt, Department of Biostatistics (BIOS) has been one of the
leading academic centers of occupational and environmental health research in the United
States. BIOS faculty have been active in the development and application of biostatistical
methods to study potential health effects of workplace exposures in a variety of industrial
settings.
The Center for Occupational Biostatistics and Epidemiology (COBE) was established in
February 2008 as a specialty research center within the Department of Biostatistics (BIOS)
in UPitt’s Graduate School of Public Health (GSPH). The mission of the COBE is to build
further upon existing departmental strengths in occupational biostatistics and epidemiology,
to enhance collaborative research across departments and schools at UPitt, to promote
both national and international recognition of these fields of strength and to increase
opportunities for external collaboration and programmatic funding.
Gary M. Marsh, Ph.D., F.A.C.E., Professor of Biostatistics, Epidemiology, and Clinical and
Translational Science is the Director of the COBE; Jeanine M. Buchanich, M.Ed., Ph.D.,
Research Assistant Professor of Biostatistics is Deputy Director of Epidemiology and Ada
O. Youk, Ph.D., Assistant Professor of Biostatistics is Deputy Director of Biostatistics.
COBE research and administrative staff include master’s level biostatisticians, master’s
level information science specialist/computer programmer, research specialists and
technical/clerical support staff, including a graduate student researcher and a professional
telephone interviewer.
The UPitt group has conducted occupational studies to investigate the long-term health
effects of exposure to such agents as man-made mineral fibers, formaldehyde, acrylamide,
acrylonitrile, arsenic, petrochemicals, aromatic amines and pharmaceuticals. They have
also applied their expertise in occupational epidemiological research to environmental
Page 26 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
epidemiologic studies of communities exposed to industrial pollutants or to hazardous
waste site materials.
Currently, the UPitt group is conducting an historical cohort study of nearly a quarter million
jet engine manufacturing workers for the Pratt & Whitney Company, a mortality surveillance
system for the Owens Corning Company and an historical cohort study of pharmaceutical
workers for the Eli Lilly Company. The Pratt &Whitney study is a collaborative effort with
the Department of Neuro-Oncology within UPMC and UIC.
7.7.2
University of Illinois at Chicago
UIC’s Environmental and Occupational Health Sciences (EOHS) Division is housed within
the School of Public Health and its goal is to protect the environment and improve the
health of workers and the general public. The Illinois Occupational and Environmental
Health and Safety Education and Research Center (Illinois ERC) was established in 1977
as one of the first National Institute of Occupational Safety and Health (NIOSH)
Educational Resource Centers in the US.
The Division has a nationally recognized program in IH that is accredited by the
Accreditation Board for Engineering and Technology. Within the division, the research
carried out by the occupational epidemiology team includes mathematical modeling,
engineering, industrial and environmental field studies and general occupational hygiene.
In addition to the mathematical, engineering, aerosol physics and industrial hygiene
expertise, the team can draw upon the medical expertise within the division. Currently, the
UIC team is engaged in several projects, three of which are in collaboration with the
University of Pittsburgh team. Before the formation of the UIC team, the collaboration in
large scale industrial epidemiology studies between the UPitt and UIC principal
investigators started in 1975 and has continued more or less unbroken ever since.
Nurtan A. Esmen, Ph.D., FAIHA, FRSH, is Emeritus Professor of EOHS; Kathleen
Kennedy, M.S. is project coordinator. The UIC team also includes a senior research
scientist.
7.8
PROPOSED TERMS AND CONDITIONS
7.8.1
Research Agreement
We propose to conduct this study as a sponsored research project within the University of
Pittsburgh (UPitt). The Sponsor (ITIA) will work with staff at the UPitt, Office of Research
to develop a mutually acceptable research agreement.
7.8.2
Organization of Subcontractors and Collaborators
The UPitt component will be directed by Gary M. Marsh, Ph.D., F.A.C.E. Dr. Marsh is
Professor of Biostatistics, Epidemiology, and Clinical and Translational Science, and
Director of the Center of Occupational Biostatistics and Epidemiology at the University of
Pittsburgh, Graduate School of Public Health. Jeanine Buchanich, Ph.D., Research
Assistant Professor of Biostatistics and Ada Youk, Ph.D., Assistant Professor of
Biostatistics will serve as co-investigators on the project.
The UIC component, which will provide the exposure reconstruction for the Phase 3 study,
will be directed by Nurtan A. Esmen, Ph.D., Emeritus Professor of Environmental and
Page 27 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
Occupational Health Sciences. Kathleen Kennedy, M.S. will serve as project coordinator.
UIC will serve as a subcontractor to UPitt.
DataBanque (DB), a Pittsburgh-based company under the direction of Susan Allen, will
serve as the data processing subcontractor to UPitt.
As noted above, the UPitt and UIC investigators will also be responsible for coordinating
the efforts of the EU investigators to ensure that common US/EU data collection and
analysis protocols are followed for purposes of a pooled data analysis.
The EU country-specific investigators will be responsible for enumerating their cohorts,
collecting and processing the data and conducting the vital status tracing. They will also be
responsible for the conduct of the country-specific case-control studies. The EU
investigators are:
Manfred Neuberger, Ph.D., Professor of Environmental Health, Center of Public
Health, and head of the Department of Preventive Medicine, Institute of
Environmental Health at the Medical University of Vienna will direct the study of the
Reutte Austria site;
Peter Morfeld, Ph.D., Head of the Institute for Occupational Epidemiology and Risk
Assessment (IERA), Evonik Services GmbH will direct the study of the three
German sites;
Magnus Svartengren, Ph.D., Professor of Environmental and Occupational
Medicine, Karolinska Institute in Stockholm and Unit Head, Environmental
Medicine, Department of Occupational and Environmental Health at Stockholm
Center for Public Health will direct the study of the three Swedish sites;
Damien McElvenny, M.Sc., Emeritus Professor of Epidemiology, University of
Central Lancashire, will direct the study of the two UK sites.
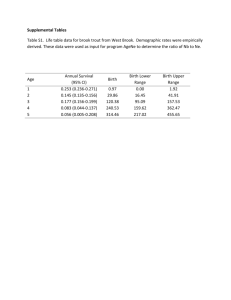
The organization and coordination between UPitt and the various subcontractors is
displayed in Figure A.1.
Page 28 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
Figure A.1: Organizational Structure of Phase 3 Study
UPitt
(Marsh/
Buchanich/
Youk)
UIC
(Esmen/
Kennedy)
DB
(Allen)
AT
(Neuberger)
7.9
DE
(Morfeld)
SE
(Svartengren)
UK
(McElvenny)
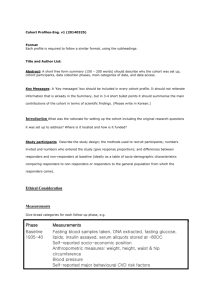
PERIOD OF PERFORMANCE
The work proposed herein for the Phase 3 study is estimated to take three years to
complete. Figure A.2 shows the proposed timeline and key activities of the Phase 3 study.
7.9.1
Reports and Manuscripts
Progress reports will be issued to the sponsor annually during the course of the Phase 3
study. Investigators will also prepare draft manuscripts for publication in peer-reviewed
journals. The sponsor will be granted a customary 30-60 day sponsor review period on all
draft manuscripts before they are submitted for publication in the peer-reviewed scientific
literature.
7.9.2
Data Confidentiality
The US and EU investigators will maintain the confidentiality of all hard copy and electronic
records, assuring that information is kept in locked files (and password protected electronic
media files) and that persons working with these records are made aware of their
confidentiality. A Confidentiality Statement Form will be executed and kept on file for each
individual working with these records. All UPitt staff will also sign the required NDI-Plus
Supplemental Assurance Form to ensure the confidentiality of NDI-Plus vital status and
cause of death data.
7.9.3 Quality Assurance and Quality Control Features of Proposed Study
7.9.3.1 Good Epidemiology Practices Guidelines
Page 29 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
During the preparation of this proposal and the performance of the contract, UPitt and UIC
have/will adhered/adhere strictly to the Good Epidemiology Practices Guidelines (GEP)
described by Cook (1991). The GEP provides guidance regarding protocol development,
reporting, quality assurance of data maintenance, and documentation of analytic
procedures.
7.9.3.2 Metrics Used to Ensure Data Quality and to Determine Progress
Standard UPitt data checks will be used throughout the proposed study to ensure the
integrity of all study data. This will include a formal check of the completeness and
accuracy of the cohort enumeration and vital status tracing, as well as comprehensive
audits of all primary study data coding and keying. For example, the coding and keyentering of all primary study data will be 100% verified by a second data coding clerk.
UPitt staff will strive to achieve cohort completeness, follow-up and cause of death
ascertainment rates of at least 95%. The UPitt guidelines will also be made part of the
common data collection and analysis protocol followed by the EU investigators.
Page 30 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested case-control study of lung cancer - UK component
Figure A.2: Proposed Timeline for Phase 3 Study
Activities
Data collection and processing
Remaining site data collection
Remaining data processing
Vital status tracing
SSA approval, file preparation & results
Death certificate requests
NDI approval, file preparation & results
Lung cancer case identification
Case-control study
Control selection
Case-control enrollment & interviews
Exposure reconstruction
Data abstraction
Operations analyses
Standardization of job titles
Modeling
Job dictionary creation
Exposure matrix creation
EU sites
Data collection and abstraction
Vital status tracing
Case-control study (where applicable)
Exposure reconstruction
Analyses
Data integration
Cohort analyses
Case-control analyses
Final report/manuscript
Year 1
Year 2
Year 3
Q3 '11 Q4 '11 Q1 '12 Q2 '12 Q3 '12 Q4 '12 Q1 '13 Q2 '13 Q3 '13 Q3 '13 Q1 '14 Q1 '14
Page 31 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
ANNEX A
Cohort Mortality Study of Workers Exposed to
Tungsten Carbide with a Cobalt Binder
Phase 2 Study Final Report &
Phase 3 Study Proposal
submitted by
The University of Pittsburgh
Department of Biostatistics
Center for Occupational Biostatistics & Epidemiology
and
The University of Illinois at Chicago
Environmental and Occupational Health Sciences
Division
November 7, 2008
Page 32 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
Table of Contents
Page
List of Tables .........................................................................................................................xxxvii
List of Figures .......................................................................................................................xxxvii
Acknowledgments ............................................................................................................... xxxviii
Executive Summary ............................................................................................................... xxxix
1. Phase 2 Study - Background .................................................................................................. 45
2. Phase 2 Study – Results .......................................................................................................... 46
2.1. Survey Development & Administration ............................................................................ 46
2.2. Site Visit Summaries ......................................................................................................... 46
2.3. Site Eligibility .................................................................................................................... 49
2.4. Site Selection for Phase 3 Study ........................................................................................ 57
2.5. Country-Specific Issues Identified in Phase 2 ................................................................... 57
2.6. Phase 2 Study Conclusions ................................................................................................ 58
3. Phase 3 Study - Primary Research Objectives ..................................................................... 59
4. Phase 3 Study - Proposed Epidemiologic Study Design ...................................................... 60
4.1. Overview ........................................................................................................................... 60
4.2. Organization of Subcontractors and Collaborators ........................................................... 60
4.3. Historical Cohort Study ..................................................................................................... 61
4.4. Basic Structure and Characteristics of the Cohort ............................................................. 61
4.5. Available Study Data ......................................................................................................... 62
5. Phase 3 Study - Proposed Exposure Reconstruction Study Design ................................... 64
5.1. Understanding of the Problem ........................................................................................... 64
5.2. Primary Research Objectives of the Exposure Assessment Component ........................... 64
5.3. Methodologic Approach .................................................................................................... 65
5.3.1. Basic Approach .......................................................................................................... 65
5.3.2. Collection of Information ........................................................................................... 67
5.3.2.1. Preliminary information ...................................................................................... 67
5.3.2.2. Standardization of job and department titles ...................................................... 67
5.3.2.3. Collection of historical exposure data ................................................................ 67
5.3.2.4. Abstraction and analysis of historical exposure data ......................................... 68
5.3.2.5. Collection of historical job and task information ................................................ 68
5.3.3. Preliminary Exposure Analysis .................................................................................. 70
5.3.4. Identification of Confounding Exposures .................................................................. 70
5.3.5. Identification of Missing Exposures and Information Gaps ....................................... 71
Page 33 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
5.4. Modeling............................................................................................................................ 72
5.4.1. Exposure Metrics ........................................................................................................ 72
5.4.2. Mathematical and Physical Models ............................................................................ 73
5.4.3. Statistical Models ....................................................................................................... 74
5.4.3.1. Monte Carlo modeling of interpolated, extrapolated and missing data.............. 74
5.4.3.2. Inversion with proportional extrapolation .......................................................... 74
5.5. Exposure Data Analysis .................................................................................................... 75
5.5.1. Existing Usable Exposure Data .................................................................................. 75
5.5.2. Determination of Classification Limits ...................................................................... 75
5.5.3. Calculation of Job Specific Exposures ....................................................................... 76
5.5.4. Assigning Job Specific Exposures and Merging Exposures ...................................... 76
6. Phase 3 Epidemiology Study - Proposed Work Plan and Timetable ................................. 77
6.1. Task 1A - Cohort Enumeration ......................................................................................... 77
6.2. Task 1B – Plant Data Collection ....................................................................................... 77
6.3. Task 2A - Data Processing, Validation and Management ................................................. 78
6.3.1. United States ............................................................................................................... 78
6.3.1.1. Electronic records ............................................................................................... 78
6.3.1.2. Hard copy records ............................................................................................... 78
6.3.2. Austria ........................................................................................................................ 78
6.3.3. Germany ..................................................................................................................... 78
6.3.4. Sweden ....................................................................................................................... 79
6.3.5. United Kingdom ......................................................................................................... 79
6.3.6. All Study Sites ............................................................................................................ 79
6.3.6.1. Data Integration .................................................................................................. 79
6.3.6.2. Data Storage ........................................................................................................ 80
6.3.6.3. Data Backup ........................................................................................................ 80
6.3.6.4. Documentation .................................................................................................... 81
6.4. Task 2B – Exposure Modeling and Job Dictionary........................................................... 81
6.5. Task 3 - Cohort Follow-Up ............................................................................................... 82
6.5.1. United States ............................................................................................................... 82
6.5.2. Austria ........................................................................................................................ 82
6.5.3. Germany ..................................................................................................................... 82
6.5.4. Sweden ....................................................................................................................... 83
6.5.5. United Kingdom ......................................................................................................... 83
6.6. Task 4 - Integration of Exposure Assessment Data ........................................................... 83
Page 34 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
6.7. Task 5 - Statistical Analyses .............................................................................................. 83
6.7.1. Overview of General Approach .................................................................................. 83
6.7.2. Descriptive Analysis of General Mortality Patterns ................................................... 85
6.7.2.1. Construction of Basic Person-Year Arrays ......................................................... 85
6.7.2.2. Analysis by Worker Type ..................................................................................... 85
6.7.3. Procedures to Account for Unknown Race ................................................................ 86
6.7.4. Calculation of Internal Cohort Rates, Expected Numbers of Deaths and SMRs ....... 87
6.7.5. Analysis of Mortality in Relation to Exposure to WCCo and Other Substances ....... 88
6.7.6. Descriptive Analysis ................................................................................................... 89
6.7.7. Relative Risk Regression Modeling ........................................................................... 90
6.8. Controlling for Confounding by Smoking ........................................................................ 91
6.8.1. External Adjustment for Confounding by Smoking ................................................... 91
6.8.2. Internal Adjustment for Confounding by Smoking .................................................... 91
6.8.2.1. Matching cases to controls .................................................................................. 92
6.8.2.2. Obtaining data on cases and controls ................................................................. 92
6.8.2.3. Statistical analysis of nested case-control study ................................................. 93
6.9. Statistical Power Characteristics ................................................................................... 93
6.9.1. Cohort study ........................................................................................................... 93
6.9.2. Case-control study .................................................................................................. 94
6.10. Strengths and Weaknesses of the Proposed Study .......................................................... 94
6.11. Qualifications of the Research Teams ............................................................................. 96
6.11.1. University of Pittsburgh ........................................................................................... 96
6.11.2. University of Illinois at Chicago .............................................................................. 96
7. Phase 3 Study - Administrative Details ................................................................................ 98
7.1. Project Structure ................................................................................................................ 98
7.2. Period of Performance ....................................................................................................... 98
7.3. Investigators ...................................................................................................................... 98
7.4. Progress Reports ................................................................................................................ 98
7.5. Data Confidentiality .......................................................................................................... 98
7.6. Quality Assurance and Quality Control Features of Proposed Study ............................... 99
7.6.1. Good Epidemiology Practices Guidelines .................................................................. 99
7.6.2. Metrics Used to Ensure Data Quality and to Determine Progress ............................. 99
8. Project Budget Justification ................................................................................................ 100
References Cited ........................................................................................................................... 4
Appendix A Phase 2 Survey Instrument ................................................................................ 103
Page 35 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
Appendix B ICDA Defined Cause of Death Categories ........................................................ 106
Appendix C Biosketches of Investigators ............................................................................... 110
Page 36 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
4.
List of Tables
Table 1. Phase 2 Site Visit Examination of Work History and Industrial Hygiene Records ....... 47
Table 2. WCCo Sites Eligible for Inclusion in Phase 3 Study ..................................................... 53
Table 3. WCCo Sites Ineligible for Inclusion in Phase 3 Study .................................................. 54
Table 4. Summary of Exposure Reconstruction Method ............................................................. 22
5.
List of Figures
Figure 1. Determination of WCCo Phase 3 Facilities: Hierarchical, Criteria-Based Selection ... 51
Figure 2. Organizational Structure of Phase 3 Study ................................................................... 28
Page 37 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
Acknowledgments
The International Tungsten Industry Association sponsored this research. The researchers
would like to acknowledge the cooperation and assistance of the representatives and
consultants of ITIA and the Alldyne ATI, ATI Stellram, Ceratizit, HB Carbide, Kennametal,
Plansee and Sandvik personnel at the sites we visited. The research proposal and the conduct
of Phase 2 were approved by the Institutional Review Boards (IRB) of the University of
Pittsburgh and the University of Illinois at Chicago.
Page 38 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
Executive Summary
Background
Several international health research agencies have recently acted to label tungsten carbide
with a cobalt binder (WCCo), also referred to as “hardmetal,” as a probable human
carcinogen. A review of the scientific basis for this decision reveals significant weaknesses
in the primary occupational epidemiologic studies of French and Swedish workers on which
it was based (Hogstedt and Alexandersson, 1990; Lasfargues et al., 1994; Moulin et al.,
1998; Wild et al., 2000). To address these limitations, a 3-phase occupational epidemiology
investigation of workers employed in the tungsten carbide (WC) industry was initiated in the
early 2000’s by the International Tungsten Industry Association (ITIA).
Phase 1 of this investigation was a feasibility study conducted by BBL, Inc. in 2006 to
determine the availability and accessibility of company records needed for the main
epidemiology study that comprises Phase 3 of the investigation. The Phase 1 feasibility
study was extended and enhanced in Phase 2 by the University of Pittsburgh (UPitt) and the
University of Illinois at Chicago (UIC) under a research contract from ITIA. Phase 2,
conducted from October 2007 through October 2008, allowed researchers: (1) to
communicate with plants directly to help clarify specific study needs; (2) to establish
communication avenues with key plant personnel and enabled those personnel to prepare
their facilities for inclusion in the Phase 3 study; (3) to apply different or additional
feasibility criteria to the data obtained in Phase 1 and (4) to establish parameters that created
the framework within which the Phase 3 study will proceed.
Three sites of the 60 from the Phase 1 study have been closed or operations have been
consolidated (Sandvik Seco Carboloy Warren MI – closed; Kennametal Lorch Germany –
closed; Sandvik Hard Materials Epinouze France – combined with Grenoble France site).
We added one site not included in the EpiFS survey (Ceratizit Luxembourg) for a total of 58
sites evaluated.
Phase 2- Methods and Results
UPitt and UIC developed and applied several criteria for a candidate site to be included in
the Phase 3 study, including a minimum size of 100 or more employees historically for
United States (US) sites and 500 or more employees historically for European (EU) sites.
Sites also had to have been producing WCCo or WC products since at least 1980 to allow an
adequate latency period for disease development. Additionally, detailed work history (WH)
information had to be available for all employees who ever worked at the facility. The last
consideration, for non-US sites, was whether vital status tracing was possible within that
country. This information was gathered via the telephone survey and/or during a site visit.
The study questionnaire used in the telephone survey had separate epidemiology and
industrial hygiene components and was administered by a professional interviewer on the
UPitt staff. Surveys were completed in April 2008. Following the surveys, UPitt and UIC
investigators conducted four US and two EU site visit trips that included a total of 18 sites
during the Phase 2 study. The sites visited were representative of the candidate sites with
respect to country, company and process.
Overall, we determined in the Phase 2 study that 18 sites met the criteria for inclusion in the
Page 39 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
Phase 3 study and 40 sites did not meet the criteria. The eligible sites are: Kennametal,
Orwell, OH; Kennametal, Johnson City, TN; Kennametal, Bedford, PA; Sandvik, West
Branch, MI; Kennametal Roanoke Rapids, Weldon, NC; Kennametal, Fallon, NV;
Kennametal, Henderson, NC; ATI Alldyne Powder Technologies, Huntsville, AL; ATI
Metalworking, LaVergne, TN; Sandvik Coromant, Gimo, Sweden; Sandvik Vastberga,
Stockholm, Sweden; Sandvik Seco Tools AB, Fagersta, Sweden; Sandvik Coromant,
Feathestone, UK; Sandvik Powder Production, Coventry, UK; CERATIZIT Austria GmbH,
Reutte, Austria; Kennametal, Mistelgau, Germany; Kennametal, Ebermannstadt, Germany;
Kennametal, Essen, Germany.
Three additional US sites may be included after more information can be found about the
whereabouts of archived records. The Kennametal facilities in Chestnut Ridge, PA, Irwin,
PA and Rogers, AR sent some files off-site for storage and the exact location of these
records has not yet been determined. We are also still working to finalize the eligibility of
three French sites and have identified two French physicians who are interested in
collaborating with us. We are still determining whether the requisite records are available at
the sites and if these physicians will be able to gain access to the necessary vital status
tracing services. For purposes of this report, these US and French sites will be considered
ineligible.
Phase 2- Conclusions
The information gathered in Phase 2 showed that a scientifically rigorous and comprehensive
epidemiology study of WCCo workers is feasible and should include workers from at least
18 manufacturing sites in the US and EU. The Phase 3 study, which will represent multiple
companies, countries and manufacturing processes, will be larger, more robust and more
definitive than any WCCo epidemiology study done to date. Additionally, Phase 2 revealed
that five main exposure agents should be evaluated and compared for potential adverse
health effects in the main epidemiology study: tungsten (W), WC, WCCo, carbon black (C)
and cobalt (Co).
The efficiency and meaningfulness of these comparisons will be improved in the main study
if the levels of exposures to the agents (termed “contrasts”) being compared are not highly
collinear, that is, at least a portion of one exposure is uncorrelated with the other exposure.
These uncorrelated components are termed “orthogonal contrasts.” While adequate
orthogonal contrasts are possible between the first four agents, the uncorrelated portion of
the WC and Co contrast is limited by small sample sizes. A straightforward and very
efficient solution to this issue is to include subjects in the study from facilities at which there
is Co exposure but no W or WC exposure. We believe that the supplier(s) of Co powder to
the facilities we visited would be good candidates for inclusion in the main study. The
limited orthogonal contrasts for Co and WC do not represent a fatal study flaw, but suggest
that we may be unable to sort out completely the contribution of each exposure alone if
increased lung cancer mortality risks are observed among subjects with combined exposures.
The inclusion of subjects with Co only exposure will increase the sample size of the
available orthogonal contrasts for Co and WC, which will increase the statistical efficiency
or power of the main study.
Page 40 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
Phase 3 Study - Primary Research Objectives
The proposed historical cohort study is designed as an essential step in appraising the health
implications of occupational exposure to WCCo. The primary research objectives of the
Phase 3 study are:
1.
To investigate the total and cause-specific mortality experience of current and former
workers potentially exposed to WCCo at multiple US and EU industrial sites that
produce(d) WCCo and/or manufacture(d) WCCo products, as compared with the
experience of the corresponding national and local populations from which the
workforces were drawn, with adjustment for potential confounding factors and with
emphasis on malignant neoplasms of the lung.
2.
To characterize as completely as possible the past and current working environment
of the study members from the sites relative to work area, job title/function and
potential for exposure to WCCo as well as potential co-exposures to several known
or suspected human carcinogens including W, WC, C and Co.
3.
To determine the relationship between level and duration of WCCo exposure and
mortality from malignant lung neoplasms with analytic adjustment to the extent
possible for potential co-exposures, including tobacco smoking habits, via internal
adjustment with a nested case-control study or external adjustment with a Monte
Carlo sensitivity analysis.
4.
To provide a framework for ongoing mortality surveillance of workers potentially
exposed to WCCo with and without concomitant co-exposures.
The epidemiology component of the Phase 3 study will be complemented by a
comprehensive and rigorous exposure assessment component conducted by UIC (Research
Objective 2 above). The primary research objectives of the exposure reconstruction
component are:
1. To generate scientifically sound estimates of exposure to WCCo and other potential
carcinogens for all job and/or task categories on a site-specific and time-dependent basis.
Average and cumulative exposure metrics will be developed and adjusted for country,
company and site variability linearly. The interaction between company and country will
also be tested.
2. To create exposure classes for subsequent statistical analysis in the epidemiology component
of the study.
3. To assess the robustness of the exposure reconstruction models employed with respect to
uncertainties arising from data gaps and inherent variability.
Page 41 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
Phase 3 Study - Proposed Epidemiologic Study Design
Based on the conclusions of the Phase 1 and 2 studies, sufficient demographic and WH data
are available to conduct an historical cohort mortality study of former and current workers
with potential exposure to WCCo at each of the study sites. Multiple sites were chosen to
afford better opportunities for contrasting cohort attributes, processes, work practices and
exposures; multiple sites also increases the likelihood of producing definitive and
informative conclusions by increasing the statistical power and the precision of the risk
estimates for detecting true excess risks overall and in relation to occupational factors.
UIC and UPitt investigators will first completely ascertain the cohort of workers with
potential exposure to WCCo (Research Objective 1). UIC will perform a comprehensive
exposure reconstruction of manufacturing processes and will develop task and time-specific
estimates of exposure (Research Objective 2). The exposure matrix will enable UPitt
investigators to construct summary measures of exposure to contaminants (Research
Objective 3) and enable ongoing mortality surveillance of the cohort (Research Objective 4).
The historical cohort study will provide the epidemiological platform for the proposed
investigation, including a nested case-control study of lung cancer. The cohort study will
focus on mortality from lung cancer and other cause of death categories (including total
mortality). Adjustment for potential confounding by smoking will occur primarily through
nested case-control studies conducted in most countries (Austria (AT), Sweden (SE), US or
the United Kingdom (UK)) or, in Germany (DE), via external adjustment.
Phase 3 Study- Statistical Analysis Plan
Because the recommended study sites are highly diverse relative to geographic location,
cohort size and cohort entry period (facility start date in most cases), we propose to approach
the statistical analysis in a site-specific manner, pooling data across sites only if warranted
by evidence of sufficient homogeneity. The advantage of such diversity from an
epidemiological standpoint is the ability to assess the consistency of our findings across the
study populations. Efforts will be made to pool data when warranted, however, as this will
improve the precision of the mortality risk estimates and increase the statistical power to
detect epidemiologically important excess risks.
Our statistical analysis of the study data will consist of two major parts, each of which is
designed to address specific objectives of the study:
Part 1
Analysis of total and cause-specific mortality patterns in relation to basic
demographic and work history factors (e.g., study site, race (US sites), gender, age,
calendar time, year of hire, duration of employment and the time since first
employment), with focus on cancer mortality and emphasis on the implicated site of
interest (lung).
Part 2
Analysis of total and cause-specific mortality in relation to occupational exposure
to WCCo with analytic adjustment for potential confounding and/or effect
modification by smoking and co-exposures to known or suspected carcinogens
including W, WC, C and Co also with focus on cancer mortality and emphasis on
lung cancer.
Page 42 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
Part 1 will include a descriptive analysis of externally standardized mortality ratios (SMRs),
with SMRs based on both national and local standard population death rates. The descriptive
phase of the analysis is useful for examining the basic structure and consistency of the
overall and study factor-specific mortality risks and for determining appropriate cutpoints for
categorizing continuous study variables.
Part 2 will include multi-variate analyses of internal cohort rates to facilitate the
simultaneous adjustment for multiple potential confounding factors and the assessment of
effect modification among two or more study factors. In particular, Part 2 will include
relative risk regression modeling (based on Cox proportional hazards model) of internal
cohort rates.
The modeling of internal cohort rates provides mortality comparisons within the cohort that
are unbiased by the “healthy worker effect” associated with external general population
comparisons. The scope of the multi-variable analysis for lung cancer mortality will be
determined largely by the corresponding number of observed deaths and their factor-specific
distributions. In addition, we may need to limit certain statistical analyses to subgroups with
sufficiently large numbers of observed deaths (e.g., white males).
To provide the most unbiased assessment of lung cancer risk possible from the available
study data, we have included in Part 2 a nested case-control study of lung cancer in the AT,
SE, UK and US sites. In this study, we will make an intensive effort to obtain the most
complete and accurate individual worker-level data on tobacco smoking habits for all cases
(deaths) of lung cancer and corresponding groups of non-cases (controls) selected from the
remaining cohort members. In the DE sites, we will control for potential confounding by
smoking via external adjustment.
While we plan to collect smoking information to the extent possible on all study members,
these data may be incomplete. By performing this adjustment in the case-control setting we
will be more likely to have complete data on smoking as most of the cases and corresponding
controls will fall into the later time periods when these data are more complete. The
statistical analysis of the case-control data will involve relative risk regression modeling of
the matched sets with adjustment for potential confounding by smoking and co-exposures to
several known or suspected carcinogens.
Phase 3 Study- Organization of Subcontractors and Collaborators
The UPitt component will be directed by Gary Marsh, Ph.D. and Jeanine Buchanich, Ph.D.
UIC, under the direction of Nurtan Esmen, Ph.D. and Steven Lacey, Ph.D., will serve as a
subcontractor to UPitt for the exposure reconstruction; DataBanque (DB), a Pittsburgh-based
company under the direction of Susan Allen, will serve as the data processing subcontractor.
The EU site investigators will be responsible for enumerating the country-specific cohorts,
collecting and processing the data and conducting the vital status tracing. Manfred
Neuberger, Ph.D., Professor of Environmental Health, Center of Public Health, and head of
the Department of Preventive Medicine, Institute of Environmental Health at the Medical
University of Vienna will oversee the Reutte Austria site; Peter Morfeld, Ph.D., Head of the
Institute for Occupational Epidemiology and Risk Assessment (IERA), Evonik Services
GmbH will oversee the three German sites; Magnus Svartengren, Ph.D., Professor of
Page 43 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
Environmental and Occupational Medicine, Karolinska Institute in Stockholm and Unit
Head, Environmental Medicine, Department of Occupational and Environmental Health at
Stockholm Center for Public Health will oversee the three Swedish sites and Thomas
Sorahan, Ph.D., Professor of Occupational Epidemiology, The University of Birmingham,
Institute of Occupational Health will coordinate the two UK sites. The investigators from
the EU countries will report directly to the UPitt and UIC investigators. The identification of
an Austrian collaborator occurred relatively recently and, as such, some details regarding the
AT cohort enumeration and processing are still under development.
Phase 3- Projected Timeline and Budget
The proposed Phase 3 Study is anticipated to take approximately four to five years to
complete. Part 1 of the Phase 3 study is anticipated to begin in November 2008 or following
receipt of pending funds from the State of Pennsylvania Department of Health (PADOH).
Subsequent parts of Phase 3 will be started as additional funding becomes available.
The PADOH has stated their intention to provide UPitt with $670,000 in direct costs for Part
1 of Phase 3 of the full epidemiology study and they have received a detailed application
from UPitt for these funds. The initiation of Phase 3 Part 1 is dependent upon the receipt of
the funds. Subsequent parts of Phase 3 are contingent upon procuring additional funding
sources and, at that time, the specific tasks and detailed budgets will be provided to the
sponsor.
We estimate that the total costs of the Phase 3 study will be in the $4-5 million range (direct
costs), depending on the total number of manufacturing sites included.
Page 44 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
1.
Phase 2 Study - Background
Several international health research agencies have recently acted to label tungsten carbide
with a cobalt binder (WCCo), also referred to as “hardmetal,” as a probable human
carcinogen. A review of the scientific basis for this decision reveals significant weaknesses
in the primary occupational epidemiologic studies of French and Swedish workers on which
it was based (Hogstedt and Alexandersson, 1990; Lasfargues et al., 1994; Moulin et al.,
1998; Wild et al., 2000). To address these limitations, a 3-phase occupational epidemiology
investigation of workers employed in the tungsten carbide (WC) industry was initiated in
the early 2000’s by the International Tungsten Industry Association (ITIA).
Phase 1 of this investigation was a feasibility study conducted by BBL, Inc. in 2006 to
determine the availability and accessibility of company records needed for the main
epidemiology study that comprises Phase 3 of the investigation. The Phase 1 feasibility
study was extended and enhanced in Phase 2 by the University of Pittsburgh (UPitt) and the
University of Illinois at Chicago (UIC) under a research contract from ITIA.
Phase 2, conducted from October 2007 through October 2008, allowed researchers to
communicate with plants directly to help clarify specific study needs; it also allowed the
investigators to establish communication avenues with key plant personnel and enabled
those personnel to prepare their facilities for inclusion in the Phase 3 study. Phase 2 also
allowed researchers to apply different or additional feasibility criteria, based upon critical
study components in an hierarchical structure, to the Epidemiological Investigation
Feasibility Study (EpiFS) data (Schell et al., 2006) obtained in Phase 1 and to establish
parameters that created the framework within which the Phase 3 study will proceed.
Page 45 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
2.
Phase 2 Study – Results
2.1.
Survey Development & Administration
Due to some concerns that the earlier EpiFS may not have completely captured information
on the extent to which powder production or use occurred in the potential study sites, UPitt
independently contacted and surveyed the sites included in the original EpiFS survey to
obtain information on powder production and related factors (dates of operation, type of
powder, workforce size, co-exposures, etc.). We needed to be certain that we were not
excluding any potentially informative sites when we developed the selection algorithm to
identify the subset of plants for further evaluation in Phase 2.
The study questionnaire, shown in Appendix A, had separate epidemiology and industrial
hygiene (IH) components and was administered by a professional interviewer on the UPitt
staff. In April 2008, we concluded the survey phase after completing a survey for each of
the sites. Three sites of the 60 from the Phase 1 study have been closed or operations have
been consolidated (Sandvik Seco Carboloy, Warren, MI – closed; Kennametal, Lorch,
Germany – closed; Sandvik Hard Materials, Epinouze, France – combined with Grenoble,
France site). We added one site not included in the EpiFS survey (Ceratizit, Luxembourg)
for a total of 58 sites evaluated.
2.2.
Site Visit Summaries
The UPitt and UIC investigators conducted four United States (US) and two European (EU)
site visit trips which included a total of 18 sites during the Phase 2 study. Table 1 below
summarizes the information gathered during the visits regarding the availability and
completeness of work history (WH) and IH data.
Page 46 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
Table 4. Phase 2 Site Visit Examination of Work History and Industrial Hygiene
Records
Trip Date
Plant
Location
WH Records
On site; older hard
copy, 2003+ electronic;
WH details in active
files, not in retiree
files.
Hard copy; active on
site with 9-10 yr WH
gaps; inactive file
availability unknown
(at HQ?).
IH Records
Bedford, PA
Last 2 yrs of files on
site; inactive to Iron
Mountain; active are
electronic; WH detail
included.
2005+ electronic;
some earlier hard
copies on site; older
may be at HQs or Iron
Mountain.
Orwell, OH
1999+ electronic;
active and last 2 yr of
terminations (terms) on
site; WH detail
included; files to HQ
until ~ 1998 then to
Iron Mountain.
Electronic ~ 2004+;
current back to 1980s
hard copy; fewer data
for earlier years.
1985+ electronic;
1986-2006 active, term
hard copies on site;
terms not available
1978-1986; WHs no
job titles (JTs) only
departments.
2004+ electronic; prior
to 1991 no
measurements.
US1
Feb. 2729 2008
Kennametal
USA Irwin
(Carbidie)
Irwin, PA
US1
Feb. 2729 2008
Kennametal
USA Chestnut
Ridge
Latrobe, PA
US1
US1
US2
US2
US3
Feb. 2729 2008
Feb. 2729 2008
April 1-3
2008
April 1-3
2008
April 2830 2008
Kennametal
USA Bedford
Kennametal
USA Orwell
Kennametal
Placentia, CA
USA Placentia
Kennametal
Fallon NV
Alldyne ATI
Powder
Technologies
Fallon, NV
On site active and term
hard copies; 1998+
electronic; WH details
available.
Huntsville, AL
All active and inactive
hard copy files in
Nashville; 1995+
records electronic.
On site; older hard
copy, 2000+
electronic.
2000+ on site; earlier
record availability
unknown (at HQ?).
Last 10 yrs electronic;
1980's/1990s records
hard copy in
Pittsburgh currently, to
be returned in near
future.
2004+ electronic;
2001-04 records in
Knoxville; prior to
2001 at TMC
Huntsville.
Page 47 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
Trip Date
US3
US4
EU1
EU1
EU1
EU1
April 2830 2008
May 2122 2008
June 6-18
2008
June 6-18
2008
June 6-18
2008
June 6-18
2008
Plant
Location
WH Records
IH Records
Henderson, NC
Active and term hard
copy records on site;
some electronic, WH
details available.
Sampling from 1980's;
last 2-3 yrs electronic,
older hard copy; on
site.
West Branch,
MI
Inactive files on site,
contain WH details;
active stored off site by 1998+ electronic; midAccenture, being
1980's to 1998 hard
moved to Fairlawn NJ, copy on site.
could not view WH
details.
Fagersta, SE
Records in Swedish;
1972+ active and term
hard copies on site,
WH details available;
prior to 1972 may be at
original company
Fagersta AB; no
electronic files.
2002+ electronic; older
files from mid-1970's
hard copy.
Gimo, SE
Records in Swedish;
active and term hard
copies on site; 2006+
electronic; WH details
available.
Electronic and hard
copy format; did not
view on site, will
folllow up in Phase 3
to verify format, extent
and availability of
records.
Kennametal
Ebermannstadt,
Germany
DE
Ebermannstadt
Records in German;
1991+ electronic;
active and term hard
copy on site; WH
detail available.
Electronic database
through workers' comp
service; additional
hard copy info on site;
documentation back to
1981, earlier in
archive.
Kennametal
Germany
Mistelgau
Records in German;
1987+ electronic;
active and term hard
copy on site; WH
detail available.
Electronic database
through workers' comp
service; on site hard
copy records with
additional details from
1983 to present.
Kennametal
USA
Henderson
Sandvik West
Branch
Sandvik Seco
Tools
Sandvik
Coromant
Mistelgau, DE
Page 48 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
Trip Date
EU1
EU1
EU2
EU2
June 6-18
2008
June 6-18
2008
July 1318 2008
July 1318 2008
Plant
Sandvik
Coromant UK
Sandvik
Powder
Production
UK
CERATIZIT
Austria
GsmbH
Sandvik Hard
Materials SAS
EU2
July 1318 2008
CERATIZIT
Luxembourg
2.3.
Site Eligibility
Location
WH Records
IH Records
Featherstone,
UK
Records may be on site
or stored at Halesowen
HQ; files not viewed;
will need to verify
format and availability
in Phase 3.
2002+ electronic;
earlier not thought to
be available.
Coventry, UK
1970+ active and term
on site, earlier terms
may have been
destroyed; some may
be at Halesowen;
~1998+ electronic.
1999+ records,
electronic and hard
copy on site; some
data early 1990's;
Reutte, AT
Records in German;
active and term on site;
1998+ electronic; prior
to 1998 (back to 1950's
or 1920's) scanned and
entered into electronic
system; WH detail
available.
Hard copy 1992 to
present on site; OSBS
(federal service) can
order measurements, at
agency and also on
site.
Grenoble, FR
Records in French;
active hard copy on
site, detail WH
available; term hard
copy may be at
Epinouze or destroyed;
no electronic records.
Hard copy late 1960's
to present on site;
measurements in
personal medical
documents, some may
exist outside of these.
Mamer, LU
Records in French;
active hard copy on
site, do not include
WH details; records
older than 12 yrs
destroyed; 2000+
electronic.
Records on site from
1990's to present; hard
copy and electronic.
UPitt and UIC developed specific criteria to evaluate the eligibility of the sites for inclusion
in the Phase 3 study. We implemented a minimum size of 100 or more employees
historically for US sites and 500 or more employees historically for EU sites. Including
sites with fewer employees would dramatically reduce the efficiency of the teams to collect
and process the site-specific information. Sites also had to have been producing WCCo or
Page 49 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
WC products since at least 1980 to allow an adequate latency period for disease
development. Additionally, detailed WH information had to be available for all employees
who ever worked at the facility. The last consideration, for non-US sites, was whether vital
status tracing was possible within that country. Figure 1 depicts the way in which using
those three selection parameters reduced the number of eligible facilities to nine in the US
and nine in the EU.
Page 50 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
Figure 3. Determination of WCCo Phase 3 Facilities: Hierarchical, Criteria-Based
Selection
Total number of
facilities
n=58
US
n=20
101+ employees
n=19
Non-US
n=38
< 100
employees
n=1
< 500
employees
n=16
501+ employees
n=22
Start year?
<1980
n=15
Start year?
<1980
n=20
1980+
n=2
1980+
n=4
Detailed work
history
available since
plant start up?
Yes
n=9
Detailed work
history
available since
plant start up?
No
n=6
Yes
n=11
No
n=9
Vital status
tracing
possible?
Yes
n=9
Vital status
tracing
possible?
No
n=0
Yes
n=9
No
n=2
Country
US
n=9
Austria
n=1
Germany
n=3
Sweden
n=3
UK
n=2
Tables 2 and 3 provide specific information on each site regarding the selection criteria for
inclusion in the Phase 3 study, including the total number of employees, the years of
operation and the availability of detailed WHs. This information was gathered via the
Page 51 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
telephone survey and/or during a site visit. Table 2 shows the 18 sites that met the criteria
and Table 3 shows the 40 sites that did not meet the criteria; also shown in Tables 2 and 3
are whether the sites were deemed eligible in the Phase 1 EpiFS study (Selected (Sel) by
BBL).
Page 52 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested case-control study of lung cancer - UK component
Table 5. WCCo Sites Eligible for Inclusion in Phase 3 Study
Eligible Facilities
(Start - 1980 or earlier)
Kennametal United States Orwell
Kennametal United States Johnson City a.
Kennametal USA Bedford
Sandvik West Branch MI
Kennametal Roanoke Rapids a.
Kennametal USA Fallon
Kennametal USA Henderson
ATI Alldyne Powder Technologies
ATI Metalworking a.
Sandvik Coromant Sweden
Sandvik Sweden Vastberga a.
Country
United States
United States
United States
United States
United States
United States
United States
United States
United States
Sweden
Sweden
Location
Orwell, OH
Johnson City, TN
Bedford, PA
West Branch, MI
Weldon, NC
Fallon, NV
Henderson, NC
Huntsville, AL
LaVergne, TN
Gimo
Stockholm
Sel BBL
Yes
Yes
Yes
Yes
Yes
No
No
Yes
No
Yes
Yes
Total
Employees
More than 1,000
501 to 1,000
251 to 500
251 to 500
501 to 1,000
101 to 250
101 to 250
501 to 1,000
501 to 1,000
More than 1,000
More than 1,000
Year Plant
Opened
1960
1966
1952
1975
1980
1960
1980
1960
1976
1951
1953
Sandvik Seco Tools AB
Sandvik Coromant UK
Sandvik Powder Production UK
CERATIZIT Austria GmbH
Kennametal Germany Mistelgau
Kennametal Germany Ebermannstadt
Sweden
UK
UK
Austria
Germany
Germany
Fagersta
Featherstone
Coventry
Reutte
Mistelgau (Bavaria)
Ebermannstadt (Bavaria)
Yes
Yes
Yes
Yes
Yes
Yes
More than 1,000
501 to 1,000
501 to 1,000
More than 1,000
501 to 1,000
501 to 1,000
1931
1966
1950
1929
1971
1971
Kennametal Essen a.
Germany
Essen (North Rhine)
Yes
More than 1,000
1926
WH Records
Available
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Some (31-71
missing)
Not sure
Yes
Yes
Yes
Yes
Some (26-77
missing)
a. Record availability was not ascertained with a site visit
Page 53 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested case-control study of lung cancer - UK component
Table 6. WCCo Sites Ineligible for Inclusion in Phase 3 Study
Reason
Country
Location
Sel BBL
Total
Employees
Year Plant
Opened
WH Records
Available
Size
Australia
Newcastle
No
51 to 100
1960 s
No
Sandvik Brazil
Records
Brazil
Sao Paulo
Yes
501 to 1,000
1963
No
Kennametal Canada Victoria
Records
Canada
Victoria
No
251 to 500
1941
No
Sandvik China
Size/Age
Lang Fang
No
251 to 500
1995
Yes
Seco - Pramet Tools, s.r.o.
Records
China
Czech
Republic
Sumperk
Yes
More than 1,000
1951
No
Size/Records
France
Bordeaux
No
101 to 250
1953
Don't know
Records
France
Andrezieux
Yes
More than 1,000
1975
No
Sandvik SAS (France)
Tracing
France
Fondettes
Yes
501 to 1,000
1957
Yes
Sandvik Grenoble/Epinouze
Records
France
Grenoble
Yes
501 to 1,000
1950s
Yes
Age/Records
Germany
Horb (Baden)
Yes
More than 1,000
1991
No
Size/Records
Germany
No
251 to 500
1973
No
No
501 to 1,000
1985
Yes
Ineligible Facilities
Sandvik Australia
Kennametal France Bordeaux
Kennametal France
Andrezieux
CERATIZIT Horb GmbH
Kennametal Germany
Nabburg
Kennametal Vohenstrauss
Sandvik Gunther & Co.
GmbH Frankfurt
Age
Germany
Nabburg
Vohenstrauss
(Bavaria)
Size/Age
Germany
Frankfurt
No
51 to 100
1985
Yes
Sandvik WALTER AG
Records
Germany
Tübingen (Baden)
Yes
More than 1,000
1924
No
Size
India
Bangalore
No
101 to 250
1967
Yes
Records
India
Pune
Yes
501 to 1,000
1960
No
Kennametal India Bangalore
Sandvik Asia Ltd
Page 54 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested case-control study of lung cancer - UK component
Reason
Country
Location
Sel BBL
Total
Employees
Year Plant
Opened
WH Records
Available
Kennametal Israel Shlomi
Size
Israel
Shlomi
No
251 to 500
1950s/1988
No
Kennametal Italy Milano
Size/Records
Italy
Milano
No
101 to 250
1956
No
Size
Japan
Miyagi
No
101 to 250
1976
Yes
Records
Luxembourg
Mamer
NA
More than 1,000
1971
Some
Size
Mexico
Tlalneplantla
No
101 to 250
1962
Yes
Ineligible Facilities
Sandvik K.K., Semine plant
CERATIZIT Luxembourg
Sandvik Mexico
Kennametal Netherlands
Arnheim
Kennametal Netherlands
Hardenberg
Records
Netherlands
Arnheim
Yes
501 to 1,000
1947
No
Size/Records
Netherlands
Hardenberg
No
251 to 500
1956
No
Sandvik Baildonit Poland
Size/Age
Poland
Baildonit
No
101 to 250
1994
Yes
Sandvik Russia Moscow
Tracing
Russia
Moscow
No
More than 1,000
1936
Yes
Kennametal Spain Vitoria
Size/Records
Spain
Vitoria-Alava
No
251 to 500
1970
No
Sandvik Espanola
Size
Spain
Caldes de Montbui
No
101 to 250
1953
Yes
ATI Stellram SA
Size
Switzerland
Gland
No
101 to 250
1974
Yes
Sandvik Taiwan
ATI Alldyne Powder
Technologies
Size
Taiwan
Chung Li
No
101 to 250
1970
Yes
Age
United States
Gurley, AL
Yes
251 to 500
1981
Yes
HB Carbide
Kennametal United States
Asheboro
Kennametal United States
Chestnut Ridge
Age
United States
Lewiston, MI
No
101 to 250
1982
No
Age
United States
Asheboro, NC
No
101 to 250
1982
Yes
Records
United States
Latrobe, PA
Yes
501 to 1,000
1958
No
Page 55 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested case-control study of lung cancer - UK component
Ineligible Facilities
Kennametal United States
Irwin
Kennametal United States
Placentia
Kennametal United States
Rancho Cucamonga
Kennametal United States
Rogers AR
Kennametal United States
Traverse City
Sandvik Coromant Stafford
Sandvik Hard Materials
Valenite
Reason
Country
Location
Sel BBL
Total
Employees
Year Plant
Opened
WH Records
Available
Records
United States
Irwin, PA
Yes
251 to 500
1976
No
Records
United States
Placentia, CA
Yes
251 to 500
1944
No
Records
United States
Monrovia, CA
No
101 to 250
1947/1996
No
Records
United States
Rogers, AR
Yes
More than 1,000
1954
No
Size
United States
Traverse City, MI
No
51 to 100
1972
Yes
Age
United States
Houston, TX
No
101 to 250
2000
Yes
Records
United States
Westminster, SC
Yes
501 to 1,000
1978
No
Page 56 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
2.4.
Site Selection for Phase 3 Study
As shown in Table 2, 9 US and 9 EU (Austria (AT)=1, Germany (DE)=3, Sweden (SE)=3
and UK=2) sites met all necessary criteria for inclusion in the Phase 3 study. With the
inclusion of these 18 sites, the Phase 3 study will represent multiple companies, countries
and manufacturing processes, and will be larger, more robust and more definitive than any
WCCo epidemiology study done to date.
As noted in Table 3, many sites were deemed ineligible due to small facility sizes (n<100
for US sites or n<500 for non-US sites); record availability was also a limiting factor for
many of the sites. The one site in Russia was deemed ineligible due to an inability to get
detailed vital status and cause of death information.
Three additional US sites may be included after more information can be found about the
whereabouts of archived records. The Kennametal facilities in Chestnut Ridge, PA, Irwin,
PA and Rogers, AR sent some files off-site for storage and the exact location of these
records has not yet been determined. For purposes of this report, these three sites will be
considered ineligible.
We are still working to finalize the eligibility of three French sites currently listed as
ineligible in Table 3 (Grenoble/Epinouze and Fondettes). We have identified two French
physicians who are interested in collaborating with us on the study but we are still
determining whether the requisite records are available at the sites and if these physicians
will be able to gain access to the necessary vital status tracing services. We will be unable
to include the French sites unless both aspects can be finalized in accordance with our study
protocol although we remain hopeful about the possibility of including French sites. For
purposes of this report, though, the French sites will be considered ineligible.
2.5
Country-Specific Issues Identified in Phase 2
One of the primary purposes of the Phase 2 study for sites located in non-US countries was
to determine the availability and accessibility not only of the necessary WH and IH data but
also the strengths and limitations of conducting vital status tracing in these countries.
As shown in Figure 1 and Table 3, 16 sites from 14 countries were eliminated because they
did not meet the minimum size requirement. The UPitt and UIC investigators felt that it
was necessary to have at least 500 employees ever employed in non-US sites because of the
added difficulty of enlisting a country-specific co-investigator, developing a countryspecific protocol for cohort enumeration and data collection and performing vital status.
Two German sites did not start production until the mid-1980’s (Kennametal Vohenstrauss)
and early 1990’s (CERATIZIT Horb) and were thus not eligible for inclusion. Nine other
non-US sites destroyed WH and/or personnel records so did not have the necessary records
available for study. The one site located in Russia (Sandvik Moscow) was excluded due to
the difficulties in obtaining complete and accurate vital status information for the workers.
Facilities in four EU countries (AT, DE, SE and UK) met the entrance criteria for the Phase
3 study. UPitt and UIC have determined that the most time and cost-effective way in which
Page 57 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
to collect the required data from these sites is to enlist the cooperation of country-specific
co-investigators who will oversee the work for the sites in their respective countries. The
information regarding these investigators and any remaining country-specific issues
identified in the Phase 2 study are described in our discussion of the Phase 3 study.
2.6.
Phase 2 Study Conclusions
The information gathered in Phase 2 showed that a scientifically rigorous and
comprehensive epidemiology study of WCCo workers is feasible and should include
workers from at least 18 manufacturing sites in the US and EU. The Phase 3 study, which
will represent multiple companies, countries and manufacturing processes, will be larger,
more robust and more definitive than any WCCo epidemiology study done to date.
The interviews, site visits and discussions with company officials to date indicate there are
five main exposure agents that should be evaluated and compared for potential adverse
health effects in the main epidemiology study: tungsten (W), WC, WCCo, carbon black (C)
and cobalt (Co). The efficiency and meaningfulness of these comparisons will be improved
in the main study if the levels of exposures to the agents (termed “contrasts”) being
compared are not highly collinear, that is, at least a portion of one exposure is uncorrelated
with the other exposure. These uncorrelated components are termed “orthogonal contrasts.”
If exposures to agents are perfectly correlated then it is not possible to distinguish
statistically the independent effects of each exposure.
Our investigations to date indicate that adequate orthogonal contrasts exist among the first
three agents and adequate epidemiological studies exist on C to help overcome any
remaining collinearity issues. However, we have found that exposures to WC and Co are
generally highly correlated (collinear), and the uncorrelated portion of the relationship
between these two exposures, or available orthogonal contrast, is limited by small sample
sizes. Moreover, there is only very limited epidemiological data available on the
independent health effects of Co powder exposure that would permit indirect analytical
control for the independent effect of this agent (Moulin et al., 1993; Mur et al., 1987).
These studies do not provide quantitative and/or interpretable exposure levels for the
subjects. This lack of exposure information precludes their use as a source of exposure
information for Phase 3 study purposes.
A straightforward and very efficient solution to this issue is to include subjects in the study
from facilities at which there is Co exposure but no W or WC exposure. We believe that the
supplier(s) of Co powder to the facilities we visited would be good candidates for inclusion
in the main study.
It is important to note that the inability to include subjects with Co only exposure does not
represent a fatal flaw to the main study design. As described in detail in subsequent
sections, the Phase 3 WCCo worker epidemiology study will be comprehensive,
scientifically sound and far superior overall to the existing epidemiology studies. The
limited orthogonal contrasts for Co and WC simply suggests that we may be unable to sort
out completely the contribution of each exposure alone if increased lung cancer mortality
risks are observed among subjects with combined exposures. The inclusion of subjects with
Co only exposure will increase the sample size of the available orthogonal contrasts for Co
Page 58 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
and WC, which will increase the statistical efficiency or power of the main study.
Obviously, if the results of the study show no association between WCCo exposure and
lung cancer mortality, then the inclusion of the Co only group would be irrelevant.
However, if the study shows an association between exposure to WCCo and lung cancer,
then it would be important to determine the contributions of both WC and Co alone and in
combination. Unfortunately, if an association is found and if we are unable to sort out
completely the independent Co effect, then retrofitting the study design to improve this
contrast may not be a viable option.
The following sections of this proposal describe the objectives, design, work plan, timetable
and budget associated with the epidemiology and biostatistical component of the Phase 3
study. When the exact information needed to estimate certain study design or cost
parameters was unavailable from the Phase 1 or Phase 2 studies, we made reasonable
assumptions as required to arrive at our best estimate.
3.
Phase 3 Study - Primary Research Objectives
The proposed historical cohort study is designed as an essential step in appraising the health
implications of occupational exposure to WCCo. The primary research objectives of the
Phase 3 study are:
1. To investigate the total and cause-specific mortality experience of current and former
workers potentially exposed to WCCo at multiple US and EU industrial sites that
produce(d) WCCo and/or manufacture(d) WCCo products, as compared with the
experience of the corresponding national and local populations from which the
workforces were drawn, with adjustment for potential confounding factors and with
emphasis on malignant neoplasms of the lung.
2. To characterize as completely as possible the past and current working environment of
the study members from the sites relative to work area, job title/function and potential
for exposure to WCCo as well as potential co-exposures to several known or suspected
human carcinogens including W, WC, C and Co.
3. To determine the relationship between level and duration of WCCo exposure and
mortality from malignant lung neoplasms with analytic adjustment to the extent possible
for potential co-exposures, including tobacco smoking habits, via internal adjustment
with a nested case-control study or external adjustment with a Monte Carlo sensitivity
analysis.
4. To provide a framework for ongoing mortality surveillance of workers potentially
exposed to WCCo with and without concomitant co-exposures.
Page 59 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
4.
Phase 3 Study - Proposed Epidemiologic Study Design
4.1.
Overview
This section discusses the study design proposed for this investigation and the associated
work plan. The key study components were arranged to ensure that the stated study
objectives will be achieved with the greatest precision and efficiency attainable from the
available study data.
Based on the conclusions of the Phase 1 and 2 studies, sufficient demographic and WH data
are available to conduct an historical cohort mortality study of former and current workers
with potential exposure to WCCo at each of the study sites. Multiple sites were chosen to
afford better opportunities for contrasting cohort attributes, processes, work practices and
exposures; multiple sites also increases the likelihood of producing definitive and
informative conclusions by increasing the statistical power and the precision of the risk
estimates for detecting true excess risks overall and in relation to occupational factors.
UIC and UPitt investigators will first completely ascertain the cohort of workers with
potential exposure to WCCo (Research Objective 1). UIC will perform a comprehensive
exposure reconstruction of manufacturing processes and will develop task and time-specific
estimates of exposure (Research Objective 2). The exposure matrix will enable UPitt
investigators to construct summary measures of exposure to contaminants (Research
Objective 3) and enable ongoing mortality surveillance of the cohort (Research Objective
4).
4.2.
Organization of Subcontractors and Collaborators
The organization and coordination between UPitt and the various subcontractors is
displayed in Figure 2. The UPitt component will be directed by Gary Marsh, Ph.D. and
Jeanine Buchanich, Ph.D. UIC, under the direction of Nurtan Esmen, Ph.D. and Steven
Lacey, Ph.D., will serve as a subcontractor to UPitt for the exposure reconstruction;
DataBanque (DB), a Pittsburgh-based company under the direction of Susan Allen, will
serve as the data processing subcontractor.
The EU site investigators will be responsible for enumerating the country-specific cohorts,
collecting and processing the data and conducting the vital status tracing. Manfred
Neuberger, Ph.D., Professor of Environmental Health, Center of Public Health, and head of
the Department of Preventive Medicine at the Institute of Environmental Health at the
Medical University of Vienna will oversee the Reutte Austria site; Peter Morfeld, Ph.D.,
Head of the Institute for Occupational Epidemiology and Risk Assessment (IERA), Evonik
Services GmbH will oversee the three German sites; Magnus Svartengren, Ph.D., Professor
of Environmental and Occupational Medicine, Karolinska Institute in Stockholm and Unit
Head, Environmental Medicine, Department of Occupational and Environmental Health at
Stockholm Center for Public Health will oversee the three Swedish sites and Thomas
Sorahan, Ph.D., Professor of Occupational Epidemiology, The University of Birmingham,
Institute of Occupational Health will coordinate the two UK sites. The investigators from
the EU countries will report jointly to the UPitt and UIC investigators. The identification of
Page 60 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
an Austrian collaborator occurred relatively recently and, as such, some details regarding
the AT cohort enumeration and processing are still under development.
Figure 4. Organizational Structure of Phase 3 Study
UPitt
(Marsh/
Buchanich)
UIC
(Esmen/
Lacey)
DB
(Allen)
AT
(Neuberger)
4.3.
DE
(Morfeld)
SE
(Svartengren)
UK
(Sorahan)
Historical Cohort Study
As noted earlier, the historical cohort study will provide the epidemiological platform for
the proposed investigation and will include a nested case-control study of lung cancer. The
cohort study will focus on mortality from lung cancer and other cause of death categories
(including total mortality). Adjustment for potential confounding by smoking will occur
primarily through nested case-control studies conducted in most countries (US, AT, SE and
UK) or, in Germany, via external adjustment.
4.4.
Basic Structure and Characteristics of the Cohort
Historical cohorts are generally defined as individuals who worked for a period of time (or
any time) between two dates, the cohort entry and cohort end dates. The entry and end
dates are determined by a number of factors including the relevant operating dates of the
study plant, the availability of records, the availability of standard death rates and of
Page 61 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
information needed to trace individuals and the minimum observation time (latency period)
associated with the disease(s) under study.
Table 2 summarizes the relevant epidemiological characteristics of each of the study sites,
as gleaned from the Phase 2 study. Table 2 shows that the study sites are highly diverse
relative to geographic location, cohort size and cohort entry period (typically plant start up).
Because of this heterogeneity, we will approach all aspects of our investigation in a sitespecific manner, combining activities or data across two or more sites only if warranted by
evidence of sufficient homogeneity.
The cohort entry period for each study site, except Reutte, is defined as the earliest date
(year) of hire until December 31, 2007. For the Reutte site, we will use a cohort entrance
date of January 1, 1950 to obviate the difficulties associated with data collection, exposure
reconstruction and vital status tracing in the 1929-1949 period. Workers hired at Reutte
before 1950 who worked beyond January 1, 1950 will be included in the cohort, however.
We propose to include in our study population all workers from each study site regardless of
gender, race or duration of employment unless it presents an undue hardship for the
investigator to enumerate the cohort in this way. Because the SE sites were enumerated for
an earlier study using a six-month minimum duration of employment, we have agreed to
uphold that entrance criteria for the SE sites in the Phase 3 study. Based upon the data
gathered in the Phase 1 and 2 studies, we are estimating that the total Phase 3 cohort will
include between 7,000 and 10,000 employees from the US facilities and between 10,000
and 15,000 employees from the EU facilities.
Many historical cohort studies of this type impose arbitrary minimum duration of
employment restrictions (e.g., six months or one year) to screen out temporary, summer or
short-term workers who are assumed to be unrepresentative of the longer-term workforce.
We believe that a more scientifically defensible approach is to include all workers initially,
and then handle any demonstrable differences among short-term workers analytically via
stratification or modeling.
In fact, short-term workers can provide unique and
epidemiologically valuable information as they may have higher or otherwise different
exposures to the agents of interest due to working in less desirable entry-level positions, for
example. Collecting records on all employees also eliminates on-site work history
screening by untrained data clerks who may miscalculate the duration of employment and
exclude eligible employees or who may exclude a worker with multiple periods of
employment and, therefore multiple records, whose total duration of employment cannot be
accurately ascertained by examining any one WH record.
We propose to determine the mortality experience of the cohort from date of cohort entry
until December 31, 2008. Our proposed study design affords ample WCCo exposure time
and follow-up time to examine meaningful mortality trends and exposure-response
relationships. The maximum follow-up time ranges from 29 years (Henderson, NC) to 59
years (Reutte, AT and Coventry, UK). The overall study also allows for the analysis of
mortality patterns relative to WCCo and other exposures in earlier and later calendar time
periods.
4.5.
Available Study Data
Page 62 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
Table 2 also indicates, with the variable entitled “WH Records Available,” the completeness
and availability of the demographic and WH records necessary to conduct an epidemiologic
study. The Phase 2 survey and site visits revealed that all information necessary for tracing
the cohort (i.e., name, birth date, Social Security number or government ID) is available for
each plant meeting the selection criteria. Dates of hire and termination are available for
every member of the cohort; therefore, mortality and exposure analyses can include timedependent variables such as duration of employment and time since first employment
(latency). Detailed WH records are also available at the job level for these sites, which will
enable linking these data with the exposure reconstruction being conducted by UIC; this
will also allow investigators to identify and calculate exposure levels properly for individual
employees. However, analyses may be limited by incomplete or limited information
available on subgroups of the cohort, such as females.
Complete adjustment for potential confounders of lung cancer (e.g., smoking history) may
not be possible with the information available in the company-held records; however, to the
extent possible, all relevant data will be microfilmed during our site visits. These data will
then be processed accordingly and merged with available demographic information to form
the master cohort file. Nested case-control studies will be conducted in most countries (AT,
SE, UK and US) to examine more fully the extent to which our lung cancer risk estimates
are confounded by smoking; for the German sites, the risk estimates will be externally
adjusted for potential confounding by smoking via Monte Carlo simulation.
The availability of exposure data among all of the study sites is satisfactory. The available
direct exposure measurements can be used for adjustment for time period, country,
company and site variability considerations as well as for the final validation of the
exposure model as structured in the job-exposure matrix. However, there are two perceived
difficulties. The most important is the collinearity, or correlation, between Co and WC
exposures which, if associated with an adverse outcome, might be difficult to differentiate
from one another. As discussed earlier, our primary proposed solution would be to include
in the Phase 3 study facility(ies) which use(s) Co but does not have WC exposure; we could
also attempt to model the effects of Co using the very limited data found in the peerreviewed literature (Moulin et al., 1993; Mur et al., 1987). The second perceived problem,
of lesser importance, is that the co-exposure information is not complete so the exposure
assessment portion of the study will more thoroughly attempt to adjust for potential coexposures to known and suspected carcinogens, including C.
Page 63 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
5.
Phase 3 Study - Proposed Exposure Reconstruction Study Design
5.1.
Understanding of the Problem
The proposed research is a hypothesis-testing study of the relationship between WCCo
exposure and mortality experience. However, the ability of the study to identify the
probable etiologic agent(s) for any observed excesses will depend upon a thorough and
scientifically defensible reconstruction of exposure to WCCo, WC, W, Co and other agents
such as C, coupled with a statistical analysis of the epidemiologic data that includes
adjustment for potential confounders such as smoking and co-exposures to occupational
carcinogens, as well as exposure-response analysis.
This study is a multi-site, multi-process study in which the mortality outcomes may be
pooled to achieve the maximum statistical power. It is essential, therefore, that the exposure
estimates for the members of the merged facilities have a sound empirical basis so that the
delineation of exposure classes is meaningful and consistent across facilities. Moreover, the
exposure reconstruction for the cohort must be sufficiently refined to provide an adequate
number of exposure classes for the epidemiologic exposure-response analysis while keeping
misclassification rates within acceptable limits. Uncritical use of limited or poorly
documented exposure sampling data or quantification of exposures based on expert
judgment may result in serious job exposure misclassification problems. Exposure
reconstruction should draw upon on all available empirical data, including site-specific
(occupational) IH measurements, site-specific historic process data, physico-chemical
principles and accepted engineering models. Experimental empirical modeling may also be
necessary to fill gaps in knowledge.
The proposed research therefore requires two components involving comparable levels of
effort and sophistication: an exposure reconstruction component that synthesizes all
available empirical data relating to historic and current exposures and a statistical
component that analyzes the epidemiologic data in relation to this exposure reconstruction
with adjustment for potential confounding factors.
5.2.
Primary Research Objectives of the Exposure Assessment Component
To determine the relationship between occupational exposure to WCCo and mortality
experience, the primary research objectives of the exposure reconstruction component are:
1)
2)
3)
To generate scientifically sound estimates of exposure to WCCo and other potential
carcinogens for all job and/or task categories on a site-specific and time-dependent
basis. Average and cumulative exposure metrics will be developed and adjusted for
country, company and site variability linearly. The interaction between company and
country will also be tested.
To create exposure classes for subsequent statistical analysis in the epidemiology
component of the study.
To assess the robustness of the exposure reconstruction models employed with
respect to uncertainties arising from data gaps and inherent variability.
Page 64 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
5.3.
Methodologic Approach
5.3.1. Basic Approach
The basic exposure model is job class (a), task (b) and year (y) normalized exposure levels
adjusted for country (X1), company (X2) and location (X3). In specific terms the
fundamental linear adjustments to exposure levels with country X company interaction may
be expressed as:
E ( a, b, y ) o ( a, b, y ) country X 1 company X 2 site X 3 countryCompany X 1 X 2
where
, E , 0 f (a, b, y0 ) or g (a, b, )
for country, company and site calculations.
At this point, we do not know whether exposure values near the start-up (y0) can be found
or whether an asymptotic value (y=∞) for exposure can be determined. Between start-up
based or asymptotic functions which define the exposure and coefficients we shall choose
the function that is convenient and/or tractable. That formulation will be used consistently
to adjust for the time decline of exposures first with the simplifying assumption that the
exposure matrix is multiplied by a scalar function of time. If this approach does not provide
reasonable results, then more complicated solutions will be sought. Once this function is
determined, all deterministic or empirical models will be adjusted using this relationship.
The general exposure reconstruction process and the steps that may be involved in this
process have been summarized in Table 4. Clearly, while some of the steps are sequential,
many of the process steps are concurrent. It should be noted that while much of the
methodology is written in general terms, the evaluation of each facility is independent.
Some of the information shown in the table will be collected on an as-needed basis and
some of the operations will be carried out on an as-required basis. The general approach is
the least complicated path without sacrificing rigor. In order to aggregate the cohort across
plants, the determinants of exposure will be adjusted to account for the differences in
operations from one facility to another using the empirically modeled correction shown
above.
Page 65 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
Table 7. Summary of Exposure Reconstruction Method
1. Selected process information collection
a. Process operation documents
b. Facility layouts and plans
c. Technical memos and other sources
d. General annual production records
2. Exposure information collection
a. All (occupational) IH monitoring data, including area and personal exposure
sampling data
b. Documentation pertaining to
i) Sampling
ii) Administrative orders
iii) Environmental exposure monitoring
iv) Occupational hygiene inspection reports
v) Occupational health reports filed to or by regulatory agencies (as applicable)
3. Selected job and task identification
a. Job descriptions as written in company records
b. As described by experienced persons (as needed)
4. Projection of results backwards through time from contemporary data (as needed)
5. Operations analysis of the production processes
6. Mathematical modeling of the information gathered above
7. Verification of models from extant data
8. Generation of task-based exposures
9. Construction of a site-specific job/exposure matrix detailing exposures for each job title
(or group of job titles) as a function of specific agents and appropriate time intervals
Page 66 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
5.3.2. Collection of Information
5.3.2.1. Preliminary information
Any exposure reconstruction study must start with extensive familiarization of the
investigators with the work tasks and operations history. Some of this work was performed
and compiled during Phase 2 and will be informative. In addition, one of the team members
is a mechanical engineer with extensive metals industry experience. Both of these
considerations are time-saving.
For further specific information collection, additional visits will be scheduled during the
Phase 3 study at the convenience of the personnel of the facility to be visited. In these visits
an extensive documentation of the processes, operations and tasks will be made; again, this
is likely simplified to some degree by the prior efforts. In addition, all extant information
on sampling will be requested.
It is important to emphasize that we will need this information from all plants included in
Phase 2 irrespective of whether the plant is included in Phase 3 or not. Although not all of
the information gathered would be necessarily used in the initial exposure estimation, it is
necessary for the empirical correction factor and for the basic exposure based stratification
of the cohort. In addition, much of the information will be necessary for more extensive
exposure reconstruction should that become necessary to understand an excess in mortality
(if an excess is observed).
Obviously, the exposure reconstruction process may be more efficiently designed with the a
priori knowledge of the quantity and quality of the data available. As it is planned, the
exposure reconstruction is sequential and adjusted as the data evolves. In that respect it is
efficient and allows considerable latitude for the development of improved mathematical
methods. As the work tasks and operations information is collected and coded, exposure
measurement information will be analyzed to determine the extent and quality of these
measurements with respect to exposure reconstruction.
5.3.2.2. Standardization of job and department titles
To elucidate the exposure-specific information, a set of standardized job title codes will be
developed. The highest order in the hierarchy of the standardization process is the spelling
and word order of jobs. The second in this hierarchy is the query of the meaning of an
uncertain job title to a person familiar with the specific process and job title information.
The last resort is the professional judgment by the industrial hygienist to either decide the
equivalency of one title to another or to deem the job title as undecipherable. In our
experience in well over three-dozen facilities, only a fraction of a percent of jobs was
ultimately deemed undecipherable. In these cases, together with untitled or unknown jobs,
the contribution of the lost record to the aggregate person years in each facility was
negligibly small.
5.3.2.3. Collection of historical exposure data
Page 67 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
Historical monitoring data may be available only for more recent years, and the “quality” of
the data with respect to the coverage of the jobs or tasks can only be determined through
extensive examination of the available information. In general, the monitoring in the
industry has been limited to several broad classes as defined by the purpose of the sampling
campaigns carried out for some specific requirement. Typically IH monitoring has
considered only the “known culprits,” such as Co, and rarely samples for compounds with
undefined health effects. Environmental samples do not define exposure but may show the
mixture of chemical challenges potentially present in each facility. Similar concerns exist
with permits, inspections, etc. The historical exposure data in conjunction with the
documentation of environmental concerns constitutes the basis of the investigation.
5.3.2.4. Abstraction and analysis of historical exposure data
Historical monitoring data from the facilities will be acquired where possible. We would
like to obtain exposure data from all facilities included in Phase 2 (Tables 1 and 2) that are
in the countries selected for the Phase 3 study. A substantial amount of monitoring data has
been collected by the facilities and the results are available. After the determination of the
data quality, we propose to analyze these data, in conjunction with the information collected
as described in sections 5.3.2.1 to 5.3.2.3 with respect to the construction of mathematical
interpolative and extrapolative models. The information available, extant and missing data,
will determine the sophistication of the mathematical models that can be generated. In other
words, in cases where the information is lacking, the mathematical model would of
necessity be a crude one.
In addition, we propose to analyze these data with respect to the best classification scheme
suggested by the distribution of the data itself. In this approach, arbitrary a priori
definitions of exposure classes are avoided and the utilization of the information content of
the data is maximized.
IH data are often happenstance measurements taken to satisfy other purposes. Therefore,
even though the existing data set may have coverage over a long period of time, it might not
be directly applicable to the exposure reconstruction. However, data spanning long periods
of time have important uses in determining historical trends (Sections 5.4.3.1 and 5.4.3.2).
These trends may be compared to calculated exposures as a secondary validation of the
calculations. In addition, prediction from the mathematical models may also be compared
to the existing data. In this respect, the data can serve as a direct validation. There are a
few difficulties in this process, especially when the existing data cover only a small
operational span of the process variables (Esmen, 1998). Unfortunately, the last problem is
virtually impossible to predict without working with the actual data. Therefore, the
resolution of any difficulties will be a part of this research project.
5.3.2.5. Collection of historical job and task information
According to the Phase 2 study, there are job, task and operations data available. Job or
occupation descriptions are a key component to understanding the determinants of exposure
for any worker. The main sources of information that describe jobs and their associated
tasks can be found in company personnel files or in labor-management contracts. Typically,
such job descriptions are general in nature, describing the overall tasks associated with the
Page 68 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
occupation. Information relating to job/occupational categories can usually be found in the
personnel and payroll files of the organization. Although the main source of general
job/occupation information is at the corporate or facility level, specifics such as discrete
tasks and how the tasks are performed, what equipment they are performed on, how often
they are performed, etc. are not contained in the job/occupational descriptions. This
information can often be collected during the site visits.
Company records at the facility and corporate level will be reviewed to determine the
availability and completeness of the job/occupation data. Job titles and descriptions also
undergo relatively routine rewriting and redefinition. This often occurs as a result of new
labor-management contracts and with the changing or addition of new products. While in
many organizations job/occupational descriptions are retained for some period after
redefinition, there is no legal requirement for their long-term retention. Most companies
undergo routine purging of unneeded records. Often records purges result in the loss of
job/occupational information for those jobs/occupations that are no longer used. In order to
fill these gaps, we will rely upon the job dictionary (as determined from WH or other
records) to identify job or occupational titles that are not described in existing personnel
records. For those jobs where no job descriptions are available, we will collect appropriate
information from knowledgeable company personnel so that these jobs/occupations can be
adequately described.
Job/occupational descriptions that are used for personnel or payroll purposes are generally
reliable; however, they do not usually reflect routine operational variability, the personal
preferences of workers in doing a task, daily changes in tasks performed, etc. Information
about particular aspects of a job/occupation such as the equipment worked with, materials
or processes where the job/occupation tasks were performed and the frequency of task
performance may be available at the facility level; however, it is doubtful that information
of this type is designated for long-term retention. Anecdotal evidence regarding how a task
performance varied with respect to written job descriptions must be obtained through site
visits, information from knowledgeable personnel and operations analyses.
5.3.2.5.1. Process information
Many of the tasks performed by workers at the process level are not described in the job
descriptions. Additionally, this type of information is not contained formally within the
documents available at the plant level. This type of information can be obtained by
discussion with workers and supervisors who were actually involved in the processes or
tasks. As an example, in one studied facility that produced a synthetic polymer, the job
description related that a task of one category of workers was to clean the process strainers.
Further definition of this task was obtained by process supervisors. Still further definition
was obtained from workers who actually conducted the task. From the workers, it was
noted that this specific task could be accomplished in a variety of ways, each having a
different potential for exposure. This type of variability is observed in exposure studies of
workers. Typically, variability of exposure measurements for a single worker is larger than
that component of variability associated with sampling and analysis of samples. How
workers conduct their assigned tasks explains why worker exposures for the same task in
the same or a similar location can vary dramatically.
The tasks that a worker may be asked to perform can change periodically. These changes
Page 69 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
may be related to new products, process changes or equipment changes – fundamental
issues in an industrial facility. Typically, the determinants of process-related task changes
can be identified by a review of process records that describe what products are being made.
5.3.2.5.2. Operations analyses
The work task analysis of production procedures, frequency of operations and changes in
production figures provide a reasonably coherent picture of potential changes in the
exposure levels over time. In addition, operations analyses are required to define the
equivalence of operations with respect to a chosen contaminant (Esmen, 1979). The
modeling methods used in this type of analysis are straightforward. Based on documented
process changes, adjustments are made to exposure concentration levels. Usually, these
adjustments are based on dimensionless scaling using either empirically determined
coefficients (or powers) or production level scaling that suggests that all things being equal,
the exposures increase linearly for tasks related to batch operations and as the 1/3 power for
tasks related to continuous operations.
The ultimate goal is to develop an exposure profile for each job class. We will consider
approaching the problem using generalized operation families and creating a task-based
family tree of operations. The model developed on this basis will be tested against the
existing exposure measurements; Monte Carlo analysis of potential outcomes is usually an
efficient method to test the validity of a model as well as its sensitivity and specificity.
5.3.3. Preliminary Exposure Analysis
Exposure reconstruction studies usually have many levels of complexity. We propose to
create and code an exposure measurement-based job/exposure dictionary in matrix form.
Available measured exposures will be assigned to the corresponding dictionary entries
strictly as placeholders. Analysis of the process and product information, confounder
identifications and other potentially useful information will also be entered. Inspection of
the job dictionary will provide the plant-specific jobs and time periods for which the
exposures were not measured. In other words, the gaps in the data will be immediately
apparent. The cohort mortality study team and the exposure reconstruction team will
coordinate their efforts to create a job/exposure matrix that can be directly used in
epidemiological software (OCMAP-PLUS (Marsh et al., 1998)).
5.3.4. Identification of Confounding Exposures
The potential exposures will differ from site to site depending on the processes present and
material used. Since the Phase 2 study lacks details on the particular contaminants included
in the exposure data, it is likely that some of the potential carcinogens may have to be
modeled as a unit step (exposed/not exposed) as a function of time. The inclusion of a
binary exposure characteristic in the worker exposure matrix does not create problems. The
determination of the characteristics of the exposure metric function is a priori. The method
of analysis used in gauging the number of exposure classes that can be generated is
sufficiently general to include the possibility of dichotomous characterization of exposures.
However, it might be possible that the rational analysis of exposure classification may
suggest a different number of classes for the same compound in different facilities. The
Page 70 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
epidemiologic analysis generated by such an outcome and the resolution of specific
problems will be addressed as a part of the proposed research. At this point we speculate
that the problem of different numbers of exposure classes for a given compound in different
facilities will be confined to the exposures to confounding compounds.
5.3.5. Identification of Missing Exposures and Information Gaps
The Phase 2 study suggested that the availability of the historical monitoring data is limited
to certain years and there is no indication of the quality of the data with respect to the
coverage of the jobs or tasks. The exposure data that can be used directly will be the basis
for all estimation processes. These data define the availability of direct exposure
information and must be used as a basis for exposure reconstruction by other means.
However, available monitoring data must be reviewed critically with respect to the sampling
strategy employed (e.g., random, worst case, happenstance) and the completeness of
documentation.
The Phase 2 study also suggested that the availability of the historical process and
environmental control information may be limited to certain years and there is no indication
of the quality of the process data with respect to the coverage of both the production and
control of the processes. Exposure reconstruction through modeling and by Bayesian
methods require process, exposure control and environmental information that range from
straightforward design and operational characteristics of the manufacturing processes to
operations that may be unique to the plant. Therefore, the following date and facility
specific exposure and process related information will be obtained to the extent possible.
i. The process equipment in use:
Whenever necessary, plant design layouts and equipment drawings that may pertain to
modeling will be collected and analyzed. Information on changes in process equipment,
plant expansion and/or contraction, replacement of processes and dates corresponding to
these events will also be sought. General and working area ventilation and installation dates
will also be requested as a part of the information on process variables.
ii. The production variables:
Change in production, plant repair and outages, production figures during constant
operations without process malfunction. Start-up and shut-down procedures and dates will
also be sought. Historical information on raw material input rates or product shipping rates
will also be requested.
iii. Personal protective equipment usage and work practices:
Information on the known personal protective equipment usage, work practice rules, and
unusual practices will be requested.
The collected information will be analyzed for each facility. The information availability
has three possible outcomes.
i. If the information is available for all plants that information is complete and no further
action is necessary.
Page 71 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
ii. If the information is available in some facilities and not others, then this is a true
information gap. As a part of the research, ways and means to close this information gap
will be sought.
iii. If the information is not available for any of the facilities, the importance of the specific
piece of information will be evaluated. The lack of an essential or very important piece of
information will be judged as a true and important information gap, and as a part of the
research, ways and means to close this information gap will be sought. If the piece of
information is judged to be not critical, it will be deemed an inconsequential information
gap. Although there are risks associated with this classification, as the researchers may not
be fully cognizant of the critical nature of missing information, this expediency may be
heuristically justified in terms of efficiency and fiscal limits.
The information collected and analyzed as specified in this section will be used to derive
process modeling based factors for extrapolation from known levels to unknown levels, for
validation of process models between known levels and for general model building and
adjustments, as well as serving as the basis for the design of experiments to obtain missing
information.
In most cases, missing process information can be augmented from metallurgical and/or
manufacturing sources. This approach, while not a primary information source, can provide
invaluable information resources especially for operations that are no longer in use. In our
experience, we have found that the literature-based augmentation of information is superior
to expert opinion, which is the last resort for information augmentation.
5.4.
Modeling
There are several distinct phases of modeling. During the first phase, the information
collected to date (however complete or incomplete) is used in a binary exposed/not exposed
scheme for job titles, years and pre-selected agent or agent/process combinations. The
results of this phase are used to select the combinations of interest for further refinement.
The hierarchically preferred methods of modeling may be listed as follows:
1. Extrapolation or interpolation of extant exposure measurements (for all combinations
that span the entire time or entire life of the process)
2. Modeling of exposures
3. Verification of models
a. Comparison with existing measurements
b. Comparison of predictions with existing data from other operation specific
sources
5.4.1. Exposure Metrics
The primary exposure metric to be used is the time integrated cumulative exposure. The
estimator for this exposure is the class average exposure multiplied by time. This estimate
may be determined readily by the product of the exposure level (the average airborne
Page 72 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
concentration) and the time spent at that job classification. However, the exposure level is a
function of time; therefore the summation must be carried out at reasonable small intervals
of time. The selection of the time interval for cumulating exposures depend on the
availability of a number of parameters, some of which (such as ability to discern job titles as
a function of time) are not related to the exposure reconstruction process. In that sense, it is
impossible to assign an a priori target to the refinement of exposure levels as a function of
time. The exposure reconstruction will compute average exposures for each job title in as
fine of intervals as possible. Particle size dependent exposure levels (respirable, thoracic
and inhalable) will be determined if possible.
5.4.2. Mathematical and Physical Models
Mathematical and physical models of exposure start from the premise that the exposure to a
contaminant has two characteristic parts: one that is controlled by the properties of the
source and the other controlled by the work practices of each worker. Super-imposed upon
these two characteristic exposures, uncontrolled and/or uncharacterized variations generate
the differences in exposure values. While the exposure of each worker is a continuous,
highly auto-correlated function in time, the samples taken from this universe can be well
represented by a right skewed distribution of measured exposure levels. The lognormal
central tendency of exposure measurements has been both empirically and theoretically
shown to be applicable to environmental sample analysis. Based on these observations, a
known characteristic exposure may be scaled upwards or downwards to account for the
process changes. It is not realistic to expect to model the characteristic exposure that is
defined by the work practices. This however, does not present a problem.
It may be shown that the characteristic exposures based on individual work practice
contribute to the between worker variance and the characteristic exposure that is due to the
source parameter shifts the distribution. It may be stated that the changes due to process
variables by and large change the median. The term “by and large” is a weak condition that
is heuristically necessary. There are counter examples to the statement that suggest that
process shifts the median. For example, controls that introduce high but intermittent
releases will tend to reduce within worker variance. In the proposed research, the
mathematical models to be developed and used will be wary of these types of important
exceptions, and verify each step to the extent that it is verifiable.
Noting that mathematical modeling is a process of creating a symbolic representation of
some phenomenon, its procedures include building a conceptual model. Therefore, the
investigator would have to decide what factors are relevant to the problem and what
parameters can be de-emphasized. Once a model has been developed, it must be challenged
to the fullest extent to ensure that it is an accurate reflection of reality. It would not be
wrong to claim that mathematical models evolve from simplifying assumptions to more
refined representations of reality through the accumulation of insight gained at each step.
With the individual exposure reconstruction team members bringing different areas of
expertise to the project, we will follow the procedural steps outlined below.
1.
Construct a very simple model with a complete list of assumptions that go
with the model.
2.
Select several prominent parameters by sensitivity analysis.
Page 73 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
3.
Construct the relationship between the reconstructed exposure and these
parameters.
4.
Does this make physical or chemical sense? If not change the assumptions.
5.
Develop the controlling equations and make predictions.
6.
Is the result produced reasonable? Perform perturbation analysis (if
necessary) and improve the model as need.
7.
When the model is satisfactory, validate the model using existing
measurements. If the validation is satisfactory then the model is ready to be used. If it
is not satisfactory, a more complicated model can be sought.
It is important to note that the determining factor in the success of exposure estimation is
not the precision of the estimates but the ability of the estimates to achieve the ordering of
exposures and exposure bands assigned to exposure classes. The bounds of the exposure
levels that can be assigned to a job class are very strongly influenced by the precision of the
job dictionary rather than the precision of the assigned exposures (Esmen et al., 2007a).
A complete understanding of the underlying scientific and engineering principles of the
exposure kinetics and the industrial processes being modeled is necessary. In some cases,
the coupling between the two highly complicated systems may not be apparent or may be
too complicated to be tractable. If a problem is not amenable to modeling, then other
extrapolation techniques must be found. There are many predictive techniques and they are
used often in making a wide range of predictions from simple industrial control predictions
to complicated econometric forecasts. Some of these methods are directly adaptable to the
extrapolative needs of exposure reconstruction. The order of preference in the method
selection is based on the dependence of the method on conjecture. The remaining exposure
reconstruction methods to be used in this study are listed in the order of preference.
5.4.3. Statistical Models
The statistical methods of interpolation or extrapolation usually require large amounts of
data. If such data are available, or can be obtained through field measurements and/or
experiments, then the two statistical methods we propose to use are listed in the order of
preference.
5.4.3.1. Monte Carlo modeling of interpolated, extrapolated and missing data
Available IH sampling data records will be used to generate a distribution of historic plant
exposure conditions. This distribution will be combined with a distribution of employee
work patterns to generate a combined distribution of employee exposures over the years of
operation of the plant.
5.4.3.2. Inversion with proportional extrapolation
The Principal Investigator of the exposure reconstruction (NE) previously developed a
mathematical model to invert time averaged samples to rank the contributing tasks (Phillips
& Esmen, 1999; Phillips et al., 2001). The method is designed to rank the tasks performed
during sampling in the order of their influence. Extensive simulation results suggest that the
Page 74 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
method is acceptably reliable in selecting one or two of the most influential tasks based on a
rather modest number of time-weighted average samples (6 to 12 or so). While the method
is not designed to estimate the absolute contribution level of each task to the composite,
using the assumption that these influential tasks are the driving mechanism of exposure
change, the exposure values may be extrapolated using equally weighted proportional
change in these tasks.
The applications involving this method will assume that the change in the characteristic
exposure potential of the contributing tasks are either known or can be calculated. It would
be very unlikely to assume that data exists with respect to the exposure potential of each
task. However, distinct tasks are usually easier to model than an integrated value for
exposure. Therefore, a mathematical formula may be elucidated to represent the change in
exposure level as a function of changes in the exposure potential of the dominant tasks of a
job classification. Although arguable or partly defensible, both the concept and application
of this procedure contains a number of assumptions that are either intuitive or can not be
readily substantiated. Therefore, this is a less preferred extrapolation than the data based
methods above.
5.5.
Exposure Data Analysis
The necessary empirical data for the creation or validation of modeled exposures will be
extracted from existing exposure measurements.
5.5.1. Existing Usable Exposure Data
Exposure data will be scrutinized to determine its usability. For example, area samples are
not directly usable exposure measures. While they might be useful in modeling exercises,
extreme caution is required in their inclusion in an exposure reconstruction study. Another
common mistake is averaging the occasional short-term sample with a group of long-term
samples. Combining samples with significantly different sampling times will introduce
significant errors. For such combinations, the variances of short- and long-term sample
must be known. Therefore, care will be taken in the calculation of long-term averages using
different duration samples. While the procedure is not a difficult one, it must be observed
since the errors propagate over time and across classes depending upon the type of
extrapolation or interpolation methods used.
5.5.2. Determination of Classification Limits
The classification of jobs or workers by exposure is an important undertaking in any
occupational epidemiology study. Hitherto, exposure classification designs have been
strongly motivated by a desire to generate a sufficient number of exposure classes for the
determination of a potential exposure-response relationship. Thus, the partitioning of
exposures has been more or less arbitrary. The interpretative problems created by the
selection of an arbitrary number of exposure assignment classes have been addressed only
recently. This theory and its application to real data sets suggest that the choice of the
number of exposure classes based on epidemiological convenience might not be
Page 75 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
appropriate. However, by considering an acceptable level of exposure misclassification and
by assuming the probable exposure distributions, it is possible to calculate the allowable
number of exposure classes and the proper partitioning ratios between these classes. Thus,
the trade-off between misclassification and number of exposure classes was shown to be a
satisfactory solution. In this study, the number of exposure classes and the boundaries for
each class will be determined by the methods published by the investigators of this grant
(Esmen et al. 2007a, 2007b, 2007c).
5.5.3. Calculation of Job Specific Exposures
Upon final enumeration of the cohort, UIC researchers will prepare a job dictionary which
they will utilize in the exposure assessment. The finalized job/exposure matrix containing
job-specific exposures determined by UIC will be linked with the epidemiological data
collected by UPitt. It has been our experience that many iterations between the
epidemiologic and exposure assessment phases are necessary to finalize the job/exposure
matrix, so UPitt and UIC investigators will work closely throughout its preparation.
Exposure profiles will be developed for each job title, or group of job titles, in order to
estimate exposure levels for each worker. These exposure levels will be expressed as an
exposure matrix and the exposure vector of the individual will be calculated based on the
exposures indicated in the matrix for each job held by the individual.
5.5.4. Assigning Job Specific Exposures and Merging Exposures
As suggested above, job-specific time-weighted average exposure is the primary exposure
metric. If it is at all possible, particle-size specific cumulative exposure levels based on
three overlapping size groups (inhalable, thoracic and respirable) will be estimated for the
three main component aerosols. C exposures are expected to be in the respirable size range,
whereas Co and WCCo particulate exposures are expected to cover the entire spectrum.
After final validation, the exposure reconstruction results will be prepared in a job/exposure
matrix usable in the cohort mortality study. Although this would theoretically be the
official end of the exposure estimation procedure, the exposure estimation team and the
epidemiology/statistical teams are expected to cooperate closely in the final analyses and
interpretation of results. The two teams have cooperated in numerous studies and they are
well aware of the fact that minor questions that require a coordinated effort tend to arise
until the last version of the final report is prepared and ready to be submitted. Our
experience has also shown that the cooperation and coordination between the two teams
continues well past the final report through the publication of scientific papers.
Page 76 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
6.
Phase 3 Epidemiology Study - Proposed Work Plan and Timetable
Following is a description of the major project tasks associated with the proposed
epidemiology study. The epidemiology and biostatistics component will run concurrently
with the exposure reconstruction phase. Draft manuscripts for peer-reviewed publication
and a final report for the sponsor will be produced in the last quarter of the project.
6.1.
Task 1A - Cohort Enumeration
The WCCo cohort will be enumerated by the study investigators using all available
corporate and plant-based employee records, including those currently stored in archives.
The cohort will include active, terminated, retired and deceased employees who worked one
or more days from cohort entry date through December 31, 2007.
To the extent possible, relevant cohort data will be derived initially from records in
machine-readable format. To ensure that the cohort enumeration is complete and accurate,
study staff will also review all hard copy employee records at the plants. Hard copy records
will include work applications, detailed job service, insurance and death certificates.
The cohort enumeration will include four basic categories of employee data:
1) Data on personal identifiers and demographic factors (e.g., name, social security
number, birth date, race, gender, pay type and employment status)
2) Data on employment history and exposure (e.g., beginning and end dates, department,
work area, job title/function, types and levels of exposure (if known) for each job held)
3) Data on health outcome (certification of death and cause of death)
4) Data on potential confounding factors (e.g., tobacco smoking history and previous and
subsequent employment)
Due to the variations in available cohort data, each plant will follow a unique protocol
during the cohort enumeration phase.
6.2.
Task 1B – Plant Data Collection
The exposure reconstruction component of the study will collect, as necessary and to the
extent possible, data related to processes, exposures and jobs/tasks as detailed in Table 4.
These data will be collected with the coordination and assistance of plant contacts
established in Phase 2 of the study and the country specific collaborators identified for
Phase 3. The UIC investigators will work with the plant contacts and collaborators to
collect the relevant information in the most expeditious and cost-effective manner.
Page 77 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
6.3.
Task 2A - Data Processing, Validation and Management
6.3.1. United States
6.3.1.1. Electronic records
Electronic records will be supplied directly from each of the nine US sites. A process for
electronically collecting data from each facility will be implemented to combine all data
into single relational database system housed on UPitt’s servers. The electronic data will be
exported into a common data format, for example, an ASCII text file, a Microsoft Excel file
or a Microsoft Access database.
6.3.1.2. Hard copy records
UPitt scanners will be used to capture any cohort data from the hard copy records and hard
copy records will be produced from all records scanned at the nine US sites. Hard copy
records will be sent to DataBanque (DB), the UPitt data processing subcontractor, and
prepared for abstraction. There, each file will be assigned to a box and will be given a file
barcode. Abstractors will prepare the file for abstraction by segmenting the documents as
critical or non-critical and in date order; they will then sort out relevant data from the
employee files and transcribe it onto a standardized abstraction form. Abstraction will be
double-blind verified to the minimum standard set by the UPitt (typically less than 5% error
rate in any field). Abstracted information will be keyed exactly as it appears on the form
and 100% double-blind verified. UPitt staff will visit the DB site weekly to confirm
accordance with the agreed upon standards and to independently audit the abstraction and
data entry. Master demographic and WH files will be created that will serve as the basis of
files formatted for various statistical analyses. These files can be transferred to and from
UPitt via CD, DVD and via secure web interfaces.
6.3.2. Austria
The Austrian investigator will work with plant personnel to obtain electronic copies of the
data, to the extent possible, and to coordinate the hard copy data abstraction. We are
continuing to work closely with the newly identified Austrian investigator to finalize the
details regarding the Austrian cohort enumeration and data processing.
6.3.3. Germany
The study data from the three German sites will be collected using an electronic, web-based
data collection system, the Health Study Application (HSA). It enables users at plant study
sites to gather protected personal data, e.g. personnel or medical data, and contains user
interfaces to input exposure, covariable and response data in German. Site users view and
edit data (e.g. first and last name, date of birth, etc.) and then a unique identification
pseudonym (PID) is created for every cohort member; this number can only be translated by
a data protection commissioner. The German investigators will only have access to the PID
and not the de-identified data. To ensure complete cohort enumeration and data linkage,
site plants will send a list of eligible active and retired workers to the data protection
Page 78 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
commissioner who imports eligible study members into the HSA-application, where the
PID is automatically generated for each worker.
6.3.4. Sweden
The three Swedish sites in this study have already been evaluated in an historical cohort
mortality study. Therefore, the Swedish investigator will begin the cohort enumeration with
those study files. To prevent undue hardship and eliminate the possibility of missing or
destroyed records, the same six-month minimum duration of employment criteria used in
the original Swedish studies will be used in the Phase 3 study. The Swedish investigator
will travel to the facilities and abstract the relevant study data for all employees who were
hired after the end of the original study and will update work histories for those employees
working as of the end of the original study.
6.3.5. United Kingdom
The UK investigator will visit the two sites (Sandvik Coromant and Sandvik Powder
Production) with a team of survey assistants from the University of Birmingham. All
available useful information from company personnel files will be transcribed onto a study
form for all past and present employees who satisfy the study inclusion criteria (e.g., all
workforce employees with one or more days worked from cohort entry date through
December 31, 2007). Useful information includes identifying particulars (full names, dates
of birth and last known address), work history details (dates of hire, first job/department,
changes of job within company and dates of leaving employment) and smoking history.
Information abstracted by University of Birmingham personnel onto forms will be
computerized at the university using a common database structure for all centers. All
computerized information will be double-checked with the source forms. Duplicate entries
will be identified and combined into a single entry.
6.3.6. All Study Sites
6.3.6.1. Data Integration
Initially, all sites will be provided with a standardized data layout. The layout will outline
the data variables and data type fields (e.g. date fields, text fields or numeric fields) required
by UPitt. Each site will abstract and enter the data, according to the layout, into a file or
database with one of the following file formats:
Microsoft Excel spreadsheet
Microsoft Access database
Comma-delimited ASCII text file
Tab-delimited ASCII text file
Fixed-width ASCII text file
These files can then be transferred to UPitt's servers via CD, DVD or a secure web
interface. A process for electronically collecting data from all sources and combining this
Page 79 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
data into a single relational database system to be housed on UPitt’s servers will be
implemented. When the transfer is complete, all data will be imported directly into MySQL
tables. These various data sets are normalized through recoding and then they are combined
to create the main research MySQL database(s). All data tables that are edited via human
interaction (i.e. not programmatically) are done so via software that maintains an audit trail.
This audit trail contains the original state of the record being updated, the user who is
updating the record and the reason the record is being updated. The audit trail can be used
to revert to an earlier version of a record should an input error occur. Potential problems of
data management and analysis include: missing data, coding errors and inaccurately
recorded data. UPitt has created software procedures that programmatically check for and
correct these problems in the MySQL research datasets.
6.3.6.2. Data Storage
Data storage will include the coding, creating and updating of MySQL databases and
applying quality control procedures while accurately documenting the entire process. The
MySQL relational database system is robust and scalable and has been successfully used by
UPitt to store and manipulate complex data sets consisting of millions of records. All data
will be imported directly into MySQL tables. The data received from the sites will be
transferred directly to MySQL database tables on the UPitt server using a MySQL ODBC
driver for Windows. The ODBC method is consistently used by UPitt to populate research
databases and it has been thoroughly tested for completeness and accuracy. Extensive edit
checks on the newly created tables will be executed to ensure consistency with the source
data files. Once data is entered into a MySQL table it is never modified without first storing
a copy of the original data in the MySQL table.
The following software will be used to create and maintain the datasets:
Microsoft Excel: Used to import and export data.
Microsoft Access: Used to import and export data.
Java: Used to develop web-based data access tools.
MySQL: The RDBMS.
SQL: Query language used to interface to the RDBMS. Used to create, query,
update and maintain data sets and generate reports.
Perl: Used to develop web-based reporting tools and to create, query, update and
maintain datasets.
Standard Linux tools: Used for access control, backups, data checks, logging, webbased tool development, report generation and file manipulation.
6.3.6.3. Data Backup
UPitt’s servers use RAID - 5 disk arrays which guards against data loss. Automated daily
backups are performed and these backup sets are burned onto DVDs. These backup sets
can be used to restore data and software should any data loss occur. In addition, a backup
server is used to store the current software and databases. This backup server can be put
into place should the main server fail. Any manual modifications to the data involve an
audit trail which can be used to revert to an earlier version of a record should an input error
occur.
Page 80 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
6.3.6.4. Documentation
The process(es) applied to the data that transform it from source data to the final research
database data are documented. In addition any software and/or scripts that are used to
create and modify the database data will be internally documented. This internal
documentation will include things such as code comments and examples.
6.4.
Task 2B – Exposure Modeling and Job Dictionary
Estimation of occupational exposures informs and bolsters the health outcomes data of the
occupational epidemiology study. The estimation of exposures relies on two principle sets
of information: historic IH data to validate exposure models and information on the
manufacturing environment. In this study, exposure reconstruction should draw upon on all
available empirical data, including site-specific IH sampling measurements, site-specific
historic chemical process data, physiochemical principles and accepted chemical
engineering models.
The content and extent of IH data from the 18 visited facilities was identified in Phase 2 of
the study. In Phase 3, these data will be collected and abstracted. IH data will also be
requested from the facilities considered in Phase 2 that did not meet the selection criteria to
be included in Phase 3. These additional data are important for the study to determine
between-site and between-country variability of exposure for similar operations. A large
portion of the data is available in electronic format, with a manageable remainder in hard
copy format that will be copied or scanned. A master exposure database will be constructed
for critical elements including contaminant name, concentration measured, date recorded,
process area or department where sample was taken and tasks performed. Descriptive
statistics will be generated. These data will serve to validate physico-chemical exposure
models developed by the research team.
The evaluation of each facility is independent. In order to aggregate the cohort across
plants, the determinants of exposure will be adjusted to account for the differences in
operations from one facility to another. Facility specific exposure and process related
information will be obtained to the extent possible.
General production process information was collected in Phase 2 of the study. In Phase 3,
available essential engineering records will be collected and reviewed. These data will be
representative of facility changes in operations and layout over space and time. These data
may include facility schematics, production records and other types of records and can
indicate major engineering/production changes throughout the life of a given facility.
Information of ventilation, work processes and personal protective equipment will also be
requested.
The integration of facility and production data, complemented by historic IH data,
comprises the overall exposure experience of the workforce that will inform the
epidemiology study.
Page 81 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
6.5.
Task 3 - Cohort Follow-Up
The cohort’s vital status will be determined as of December 31, 2008. The UPitt
investigators will utilize customized country-specific vital status tracing protocols, as
detailed below.
6.5.1. United States
Study members for US plants with unconfirmed vital status (not known from company-held
records to be alive or dead as of the vital status end date (12/31/2008)) will be entered into
the standard UPitt two-stage vital status tracing protocol to identify deaths among cohort
members (Buchanich et al., 2005).
Phase 1 consists of sending all the names of cohort members not known to be alive to the
Social Security Administration (SSA). The SSA identifies living, unknown and deceased
vital status. Phase 2 consists of sending subjects identified as having died prior to 1979 to
the health department of the state of death to obtain a death certificate. All death certificates
will be coded to the underlying cause of death by a U.S. National Center for Health
Statistics nosologist using the International Classification of Diseases (ICD) rules in effect
at the time of death. This method of coding, combined with the use of standard death rates
that are also specific to the corresponding time period, ensure the comparability of cause of
death categorization over time.
Subjects identified as unknown or deceased after 1978 will be sent to the National Death
Index - Plus (NDI+) to obtain the coded cause of death. NDI-Plus became available to
researchers in 1997 and provides the underlying and multiple causes of death for deceased
study subjects. These searches will be supplemented, as necessary, by commercial tracing
agencies (e.g., Lexis-Nexis).
6.5.2. Austria
Vital status tracing systems in Austria are in electronic form at the pension insurance bureau
and Statistik Austria from 1970 to the present. Employees will be matched to the national
systems using their unique identification system and date and cause of death will be
abstracted for matches. Employees not known to be alive or dead from January 1, 1950
through January 1, 1970 will be manually searched through local registries to determine
date and cause of death.
6.5.3. Germany
A data protection contract between the University of Cologne and site plants will be
negotiated and signed. Based on this contract, the data protection commissioner will send a
list of retired workers with names, date of birth and last address to the University of
Cologne for determination of vital status and date and cause of death for deceased persons.
These data are then sent back to the data commissioner who imports the data into the HSA,
Page 82 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
where the relevant PID will be matched to the open identifier. The German investigators
then merge together the datasets using the PID.
6.5.4. Sweden
Cohort members will be traced using current data lists and previous staff registries, which
contain information on time of birth and period of employment. The social security
numbers can be determined from plant records or with the help of the Swedish regional
social insurance office via the Swedish Central Statistics Agency (SCB) and church records
in the respective parishes. Employee social security numbers will be matched to the
national death registry for the entire period. Death certificates will then be obtained from
the SCB. Employees with foreign citizenship during their employment or those who
emigrated will be excluded from evaluation.
6.5.5. United Kingdom
In the UK, the Information Centre for Health and Social Care (IC) can arrange for bona fide
researchers to be given copies of death certificates for deaths. The IC is a recently created
body that has taken over many of the roles in medical research previously carried out by the
Office for National Statistics (ONS). Death certificates will be supplied with underlying
causes and multiple causes coded according to the ICD revision in effect at time of death. It
will not be necessary to get written permission from each living study subject as regular
updates of death are not required for this study. It will be necessary, however, to obtain the
approval of a local Research Ethics Committee to obtain the details of earlier deaths.
6.6.
Task 4 - Integration of Exposure Assessment Data
This task involves the integration of the exposure assessment data to be developed by UIC.
Details of the independent exposure assessment component of the proposed study are
provided in Section 5. UPitt investigators will work closely with UIC investigators to
coordinate the integration and verification of data from the epidemiological and exposure
assessment components of the study.
This will involve linking the job/exposure matrix created by UIC investigators with the
individual WHs and epidemiological data compiled by the UPitt investigators (detailed in
Sections 5.5.4. and 5.5.5.). UPitt will also serve as a clearing house for all exposure
assessment-related study data, and will be responsible for maintaining an inventory and
ultimately an archive of all project data.
6.7.
Task 5 - Statistical Analyses
6.7.1. Overview of General Approach
As noted, the study sites are highly diverse relative to geographic location, cohort size and
cohort entry period (facility start date in most cases). Because of this heterogeneity, we
propose to approach the statistical analysis in a site-specific manner, pooling data across
Page 83 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
sites only if warranted by evidence of sufficient homogeneity. The advantage of such
diversity from an epidemiological standpoint is the ability to assess the consistency of our
findings across the study populations. Efforts will be made to pool data when warranted,
however, as this will improve the precision of the mortality risk estimates and increase the
statistical power to detect epidemiologically important excess risks.
Our statistical analysis of the study data will consist of two major parts, each of which is
designed to address specific objectives of the study:
Part 1
Analysis of total and cause-specific mortality patterns in relation to basic
demographic and work history factors (e.g., study site, race (US sites), gender,
age, calendar time, year of hire, duration of employment and the time since first
employment), with focus on cancer mortality and emphasis on the implicated site
of interest (lung).
Part 2
Analysis of total and cause-specific mortality in relation to occupational exposure
to WCCo with analytic adjustment for potential confounding and/or effect
modification by smoking and co-exposures to known or suspected carcinogens
including W, WC, C and Co also with focus on cancer mortality and emphasis on
lung cancer.
Part 1 will include a descriptive analysis of externally standardized mortality ratios (SMRs),
with SMRs based on both national and local standard population death rates. The
descriptive phase of the analysis is useful for examining the basic structure and consistency
of the overall and study factor-specific mortality risks and for determining appropriate
cutpoints for categorizing continuous study variables.
Part 2 will include multi-variate analyses of internal cohort rates to facilitate the
simultaneous adjustment for multiple potential confounding factors and the assessment of
effect modification among two or more study factors. In particular, Part 2 will include
relative risk regression modeling (based on Cox proportional hazards model) of internal
cohort rates.
The modeling of internal cohort rates provides mortality comparisons within the cohort that
are unbiased by the “healthy worker effect” associated with external general population
comparisons. The scope of the multi-variable analysis for lung cancer mortality will be
determined largely by the corresponding number of observed deaths and their factorspecific distributions. In addition, we may need to limit certain statistical analyses to
subgroups with sufficiently large numbers of observed deaths (e.g., white males).
To provide the most unbiased assessment of lung cancer risk possible from the available
study data, we have included in Part 2 a nested case-control study of lung cancer in the AT,
SE, UK and US sites. In this study, we will make an intensive effort to obtain the most
complete and accurate individual worker-level data on tobacco smoking habits for all cases
(deaths) of lung cancer and corresponding groups of non-cases (controls) selected from the
remaining cohort members. In the DE sites, we will control for potential confounding by
smoking via external adjustment.
While we plan to collect smoking information to the extent possible on all study members,
these data may be incomplete. By performing this adjustment in the case-control setting we
Page 84 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
will be more likely to have complete data on smoking as most of the cases and
corresponding controls will fall into the later time periods when these data are more
complete. The statistical analysis of the case-control data will involve relative risk
regression modeling of the matched sets with adjustment for potential confounding by
smoking and co-exposures to several known or suspected carcinogens.
The following sections describe details of our statistical analysis plan.
6.7.2. Descriptive Analysis of General Mortality Patterns
6.7.2.1. Construction of Basic Person-Year Arrays
We will examine the total and cause-specific mortality experiences of the site-specific
cohorts from the cohort entry date (Table 2) to December 31, 2008. Using an OCMAPPLUS (Marsh et al., 1998) modified life table procedure, we will jointly classify the personyears at risk contributed by each study member by the primary study factors: study site,
race, gender, follow-up period, age group, year of hire, duration (years) of employment
(DOE), the time (years) since first employment (TSFE) and worker type (short-term, longterm).
The final categorization of these factor-specific person-year arrays will be determined upon
examination of the actual data. For certain sites, we may need to group person-years into
broader categories due to the smaller cohort sizes. For workers whose vital status cannot be
traced, person-year counts will be accumulated until the last point of verifiable alive status,
which is usually the date of termination from employment. Person-years relative to DOE
and TSFE will begin on the starting date of the first job in the WH (date of hire) or January
1, 1950 for Reutte, AT employees hired before that date.
6.7.2.2. Analysis by Worker Type
The purpose of our proposed analysis by worker type is to analytically separate the
mortality experience of workers with short overall employment histories from those having
long-term employment histories. Short-term workers are often more transient and may have
behavior and lifestyle characteristics associated with less favorable overall mortality
patterns. They may also have unique or higher occupational exposures to the agents of
interest due to working in less desirable entry-level positions. By design, this separation by
worker type provides the opportunity to examine mortality patterns among long-term
workers unconfounded by behavior, lifestyle or exposure patterns unique to short-term
workers.
We propose to examine the mortality patterns of short-term workers using two different
approaches. While the actual cutpoint used to dichotomize workers into short and longterm categories is essentially arbitrary, a point between one to five years is often used in
studies of this type with the ultimate point depending in part on the distribution of the
cohort by overall DOE.
Page 85 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
In the first, more conventional prospective approach, we will analyze short-term workers by
stratifying the person-years of the total cohort by DOE as noted above, using the short vs.
long-term worker cutpoint as the upper bound of the first DOE interval. Here, the personyears of the workers whose total DOE is less than the cutpoint are combined with the shortterm portion of person-years contributed by the long-term workers. Because this cohort is
primarily an incidence cohort (dates of hire and cohort entry equivalent), the long-term
workers will contribute person-years to the short-term category. In effect, this analysis
focuses on the mortality experience of all workers during the short-term portion of their
employment history. Also, here the short-term workers can serve as the baseline category
for the remaining long-term categories.
In the second, retrospective approach to our worker type analysis, we will exclude the shortterm portion of the person-years for long-term workers from the short-term workers personyear counts. For long-term workers, person-year counts will begin at the short vs. long-term
worker cutpoint. In effect, this analysis of long-term workers resets the starting date for
person-year counts from the cohort entry date to the date when the cutpoint is reached. In
contrast to the first approach, this analysis focuses on the mortality experience of short-term
workers only as a distinct subcohort of the total study population. As such, this group
cannot be used as a baseline category for the long-term workers, and we will need to
interpret our results considering the fact that they are not entirely prospective in nature.
6.7.3. Procedures to Account for Unknown Race
The EU sites do not routinely collect race nor are national death rates available by race so
we will not analyze these sites by race.
We will collect information on race from the US sites but anticipate from our experience
with past occupational cohort studies that this variable will be unavailable for some
employees. Rather than making arbitrary assumptions about the race of the unknowns or
eliminating workers with unknown race from the analysis, we propose to handle this
common data deficiency analytically using a procedure unique to the OCMAP-PLUS
software (Marsh et al., 1998).
In our analytic approach, called the Proportional Allocation Method (PAM), the personyears and observed deaths accumulated by study members of unknown race are assigned to
the white or nonwhite categories in proportion to the distribution of study members with
known race. For example, if a cohort with 1,300 person-years included 800 white personyears, 200 nonwhite person-years and 300 person-years with unknown race, 800/1000 or
80% of the 300 unknown race person-years (240) would be assigned to the white category,
and 200/1000 or 20% (60) would be assigned to the nonwhite category resulting in an
estimated total race-specific person-year distribution of 1040 white and 260 nonwhite.
Also to help reduce bias, the PAM will be performed within strata defined by study site,
gender, age group and time period. The resulting total number of assigned white and
nonwhite person-years and observed deaths will then represent weighted averages of the
stratum-specific assignments. The stratification will not be extended to other study
variables such as DOE or TSFE to avoid sparse data problems.
Page 86 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
While the PAM estimation procedure does not enable the imputation of race data for
individual study members, it does permit the person-years and observed deaths of study
members with unknown race to be included in the grouped external mortality comparisons.
This is done under the reasonable assumption that the distribution of whites and nonwhites
in a given stratum of workers with unknown race is equivalent to the corresponding
distribution based on known race.
6.7.4. Calculation of Internal Cohort Rates, Expected Numbers of Deaths and SMRs
We will compute expected numbers of deaths by multiplying the person-years at risk in the
factor-specific categories by the corresponding mortality rates in the appropriate general
populations. For the US sites, we will compute expected numbers of deaths using as
standard populations the total US and the local study site areas (defined as counties or
aggregates of counties) from which the associated workforces were largely drawn.
Our US mortality rate files are available from the earliest observation time (1952 – the start
of the Bedford facility) through 2005. Population-weighted county rates will be obtained
from the Mortality and Population Data System (MPDS) developed and maintained by the
investigators at UPitt (Marsh et al., 2005). MPDS county rates are currently available for
cancer categories from 1950 through 2005 and for noncancer categories from 1962 through
2005. For the sites which started operations before 1962 (Bedford - 1952, Fallon - 1960 and
Orwell - 1960), we will apply 1962-1964 rates to the1960-1964 period. We anticipate that
our US and local rate files will be current through 2007 by the time of this analysis.
For the EU sites, we will compute expected numbers of deaths based on the associated
national and regional rates. These requisite rates are available and will be obtained by the
country-specific investigators from the appropriate national or regional government vital
statistics offices. Modifying our cause of death categories somewhat to account for US-EU
differences in cause of death categorizations may be necessary. Our MPDS system is
entirely flexible in this regard and will enable us to form compatible US-EU rates.
Because local area death rates usually provide the most valid available mortality
comparisons [as they tend to adjust for the social, cultural and economic factors related to
disease, including smoking to some extent (Doll, 1985)], the analysis of general mortality
patterns will focus primarily on the local county or regional comparisons.
For the sites in Germany, we will use external smoking-specific reference populations, such
as those developed in the US by the American Cancer Institute, to control for potential
confounding by smoking. For the AT, SE, UK and US sites, we believe that adjusting the
lung cancer risks associated with WCCo exposure for potential confounding by smoking
can be done more effectively and with greater statistical efficiency in the context of a nested
case-control study (described below).
We will express mortality excesses and deficits as Standardized Mortality Ratios (SMRs),
that is, the ratio of observed numbers of deaths to expected numbers of deaths. SMRs for
total and cause-specific mortality will be computed for the subgroups of the total cohort
defined by study site, race (US), gender, age group, follow-up period, year of hire, DOE,
TSFE and worker type. Where deemed appropriate via homogeneity analysis, SMRs will
also be computed for two or more study sites combined. Appendix B provides the cause of
Page 87 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
death categories and corresponding revision-specific International Classification of Diseases
(ICD) Codes that we will use in the mortality analysis.
For our descriptive analyses of SMRs, deviations of the SMR below and above 1.00,
indicating deficit and excess mortality risks, respectively, will be identified using exact
Poisson probabilities described by Breslow and Day (1987). For all of our analyses, twotailed p-values less than 0.05 will be deemed statistically significant and those greater than
or equal to 0.05 and less than 0.10 will be deemed marginally statistically significant. No
formal probability adjustments will be made for the multiple statistical comparisons to be
performed in the analysis (although this will be considered in the interpretation of the
findings) or for the PAM estimation procedure used to reallocate unknown race personyears and observed deaths.
6.7.5. Analysis of Mortality in Relation to Exposure to WCCo and Other Substances
Using the historical exposure data estimated for WCCo and other agents in the UIC
exposure assessment phase of the proposed study, we will use OCMAP-PLUS to compute
various time-dependent summary measures of exposure for individual workers. These
summary measures, which will serve as the exposure variables in our exposure-response
analysis, are described in detail below.
For exposure agents characterized quantitatively or qualitatively, we will compute the basic
measure “duration of exposure.” The duration of exposure measure for a given agent
(termed Agent_Dur) computed over Nj jobs during exposure period j can be expressed as
Nj
1 if exposed
Agent _ Durj Timei Expi , where Expi
i 1
0 if unexposed
where Time i and Exp i represent DOE and exposure level, respectively, of the ith job in the
WH during exposure period j. The DOE measure considered in the general mortality
analysis can be viewed as a special case of this duration of exposure measure where Exp i =
1 for all jobs in the WH.
For exposure agents measured quantitatively, the time-weighted cumulative exposure
(termed Agent_Cum) is defined analogously as
Nj
Agent _ Cum j Timei Expi
i 1
where Exp i is the quantitative exposure value for the ith job.
For quantitatively measured exposure agents, we will also consider a third summary
exposure measure, average intensity of exposure. This measure can be computed separately
or in conjunction with duration of exposure and/or cumulative exposure. The average
intensity of exposure (termed Agent_AIE), computed over Nj jobs during exposure period
j, is calculated by dividing Agent_Cum by Agent_Dur or
Page 88 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
Agent _ AIE j
Agent _ Cum j
Agent _ Durj
Agent_AIE represents the average intensity of exposure during periods when the worker is
exposed to that agent. The default exposure period j described in the above expressions is
the total employment history (i.e., the time interval from date of hire to date of termination,
accounting for gaps such as sick leaves, layoffs, strikes, etc.).
The interpretation of internal rates or SMRs relative to the exposure measures described
above relies on the implicit assumption that mortality during a given observation period is
related to the duration, cumulative or average intensity of exposure received from hire date
up to the point of observation for mortality. For some agents, including WCCo, the actual
effectiveness to cause disease may change over time, and may be negligible during parts of
the employment history (e.g., for cancers, the time between initiation of tumor growth and
death) (Caplan et al., 1984). To enable some adjustment for this changing effectiveness, we
may also examine a weighted or lagged form of the above summary measures. The choice
of the lagging period depends on known or hypothesized exposure-response and latency
(time from first exposure to development of disease) characteristics of the agent and disease
under study.
For example, a reasonable lagging period for examining the WCCo exposure-lung cancer
relationship is five years, because WCCo exposures received five years before the date of
death probably did not impact on the mortality risk (i.e., assuming that on the average, a
period of five years elapses between formation of tumor, diagnosis and ultimately death).
Lagging can also be used in conjunction with exposure time “windows”, where the
“effective” exposure is calculated during a pre-determined window of time that lags the risk
period a pre-determined number of years. Lagging with and without exposure time windows
was used by UPitt investigators in a recent historical cohort study of man-made vitreous
fiber workers (Youk et al., 2001).
In addition to and with the summary measures described above, we will relate mortality
risks to the time-dependent variable, time since first exposure the agent(s) of interest
(termed Agent_TSFExp). Agent_TSFExp will be computed from the date of first exposure
until the first occurrence of the date of death or the end of the study period. Unlike the
variable TSFE used in the general mortality analysis, Agent_TSFExp discounts the
irrelevant elapsed time from date of hire until the date of the first exposure. For a given
agent, the non-time-dependent variables age and calendar time of first exposure will also be
considered alone and in combination with the summary exposure measures described above.
6.7.6. Descriptive Analysis
One objective of this analysis is to examine descriptively, using externally standardized
(local comparison) SMRs, the relationship between exposure to WCCo and other agents and
total and cause-specific mortality, with focus on cancer and emphasis on lung cancer.
Although the relative risk regression analysis described below is more appropriate for the
analysis of multiple exposures and/or potential confounders, the SMR-based, exposurerelated analysis provides descriptive information on observed deaths relative to the same
exposure measure categorizations used below in the relative risk regression analysis.
Page 89 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
Using a modified life table algorithm in OCMAP-PLUS, we will jointly classify personyears at risk contributed by each study member by study site, race (US), gender, calendar
time period, age group and categories of one or more of the summary exposure measures
computed for WCCo and other agents as described above. For a given summary measure
and cause of death category, we will categorize deaths using approximate percentiles (e.g.,
quartiles or quantiles) of the distribution of deaths according to the summary measure. The
baseline category will include the person-years of strictly unexposed workers as well as the
person-years of exposed workers up to the time of their first exposure. We will compute
SMRs for the various categories of the summary exposure measures as described in the
general mortality analysis section.
6.7.7. Relative Risk Regression Modeling
Relative risk (RR) regression modeling will be used to investigate the dependence of the
internal cohort rates (modeled as time to death) for lung cancer on combinations of the
WCCo exposure measures, with adjustment for potential confounding factors and potential
co-exposures. Risk sets will be explicitly constructed from the cohort data file with age as
the primary time dimension, using the RISKSET program module in OCMAP-PLUS
(Marsh et al., 1998). Risk sets will be matched further on gender and year of birth to
control for cohort effects. For the exposure-response analyses, the time-dependent exposure
measures of interest will be evaluated for each individual at each event time they were at
risk (the date of death of the case).
Multiplicative relative risk models of the form λ(t) = λ0(t) exp{x(t)β} will be fit to the
internal cohort rates (Cox, 1972; Cox, 1975), and the conditional logistic regression
program in STATA (STATA Corp., 2007) will be used to estimate β from the explicitly
constructed risk sets. To parallel the descriptive SMR analysis of mortality in relation to
exposure, categorized forms of the covariates will be considered. The statistical
significance of each main effect (expressed as a global p-value) will be assessed with a
likelihood ratio statistic. For the quantitative exposure variables (both WCCo measures and
co-exposures) that exhibit a monotonically increasing or decreasing pattern in the parameter
estimates, a test for linear trend will be conducted (expressed as a trend p-value). Joint
effects of the WCCo exposure measures and the co-exposures as well as effect
modifications will be assessed to the extent possible.
To elucidate complexities in possible exposure response relationships, we will attempt to
perform analyses relaxing the assumed linearity in dose-response by modeling the effects of
exposure using piecewise linear functions (linear splines). Knots will be defined at tertiles
(or quartiles) of the lung cancer case distribution for each of the exposures. Splines defined
in this manner will be used to assess possible interactions of the exposures with other
potential confounders which allow for separate non-linear exposure-response relationships
for levels of the confounders.
Additional analyses may also include the assessment of adequate functional forms for
exposures using fractional polynomials. All possible exposure response models will be fit
including powers of the “primary” exposure, adjusting for the other exposures; the “best”
model at each level of complexity will be identified from a direct search based on the
residual deviance, and compared to a model assuming a linear functional form.
Page 90 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
To account for potential collinearities among the WCCo exposure and co-exposures (W,
WC, Co and C), orthogonal polynomials can be defined based on a modified Gram-Schmidt
procedure (Phillips & Esmen, 1999). Orthogonal polynomials can be used to assess the
significance of variables with the effect of the collinear variable “removed”. In this way,
the contribution of each exposure that is uncorrelated with the other can be determined.
Parallel to the descriptive SMR analyses, we will also explore a possible exposure-response
relationship between lung cancer and exposure to each exposure of interest utilizing
exposure-weighting as an alternative characterization of exposure. Due to the uncertainties
in selecting an appropriate exposure-weighting scheme, a range of plausible time lags and
unlagged/lagged time windows will be considered.
6.8.
Controlling for Confounding by Smoking
The importance of potential confounding by smoking in studies of lung cancer is
indisputable. We propose to address the likelihood and extent that confounding by smoking
may contribute to the results of the lung cancer analyses in this study in two ways, via
external and internal adjustment.
6.8.1. External Adjustment for Confounding by Smoking
For the facilities in Germany, we propose to adjust our lung cancer risk via external
adjustment. Without smoking information directly on the workers or from the sites, an
estimate of the possible confounding due to smoking can be found using estimates of the
smoking prevalence in the WCCo exposed and unexposed workers, the original unadjusted
lung cancer risk due to WCCo and an estimate of the lung cancer risk due to smoking in the
general population.
We will attempt to identify peer-reviewed studies and occupational exposure surveys
providing information on smoking patterns among WCCo-exposed workers that are
independent of our epidemiological study. We will also identify comparison smoking
prevalence information for the respective general populations of the study using peerreviewed studies, government reports and other sources.
We will accomplish the external adjustment for smoking using the methods described by
Steenland and Greenland (2004). Their Monte Carlo based strategy is an extension of
indirect confounding methods proposed by Axelson and Steenland (1988). An unadjusted
risk estimate can be adjusted by a bias factor to obtain an externally adjusted risk. This bias
factor reflects the possible confounding of the unadjusted risk by a related factor like
smoking.
6.8.2. Internal Adjustment for Confounding by Smoking
For the AT, SE, UK and US sites, we will conduct a nested case-control study to obtain
smoking information on the cases and controls using an interview with the case or the nextPage 91 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
of-kin of the case (when the case is deceased). Details regarding the country-specific
methods of locating, contacting and interviewing knowledgeable informants are under
development and will be finalized as this portion of the Phase 3 study progresses.
6.8.2.1. Matching cases to controls
The nested case-control study of lung cancer can be considered as a special case of the
corresponding relative risk regression analysis described above. That is, for each case
(death) due to lung cancer identified in the cohort, we will randomly select a group of
matched controls from the corresponding risk set formed for the relative risk regression
analysis. As noted in that section, the non-case members of each risk set are matched on the
event (death) age of the case, gender and year of birth. We will select two controls for each
case.
6.8.2.2. Obtaining data on cases and controls
To obtain more detailed or otherwise unavailable information on potential risk factors for
the cases and controls, an attempt will be made to locate and interview a knowledgeable
informant, ideally the worker himself or a surviving member of the worker’s immediate
family (proxy respondent). The potential informant will be found from plant record
information or by the same tracing sources used to determine the vital status of the study
cohort. To obtain a minimum of two controls for each case, it is estimated that
approximately four cohort members per case (or their next of kin, if deceased) will need to
be contacted.
Before the contacting and interviewing processes for the case-control study can begin, it
will be necessary to obtain approval from the National Death Index to allow access to the
NDI-Plus system and the use of personal information on the death certificate (e.g., address
of next of kin) for follow-back purposes. As part of securing this approval, it will also be
necessary to clear this research proposal through the UPitt Institutional Review Board
(IRB), a group that ensures the protection of research subjects. IRB approval will also be
required by some state health departments before they will release copies of death
certificates, especially for studies involving followback.
Another study protocol issue relates to obtaining the informed consent of study members (or
proxy respondents) before they are interviewed for the case-control study (note: consent of
individual workers can be waived by the IRB at the cohort level). It is proposed that a
country-specific introductory letter be sent to potential informants to announce the purpose
and importance of the study and introduce the investigators. To enhance participant
response, the letter should indicate that the proposed study is supported by the companies as
well as the local union(s). A consent form will be included with the approach letter,
requiring informants to indicate their willingness to participate by signing the appropriate
line on the form.
Potential informants will be instructed to return the consent form within two weeks of the
date of the letter indicating their willingness to participate. At the end of this waiting
period, willing informants will be contacted by a professional interviewer for a brief (20-30
minute) telephone interview concerning such items as the subject’s smoking, nonPage 92 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
occupational and occupational history. To eliminate potential biases, the interviewer will
not be aware of case-control status when making the telephone calls. A questionnaire will
be mailed, with a pre-addressed postage-paid return envelope, to potential informants with a
known address but no available phone number.
The case-control study questionnaire proposed for this study will be based upon the one
already used in a nested case-control study of lung cancer among workers with potential
exposure to man-made vitreous fibers. We will modify the existing instrument as necessary
to capture specific risk factors of interest for WCCo workers.
6.8.2.3. Statistical analysis of nested case-control study
The statistical analysis of the case-control data will be conducted along the lines of the
relative risk regression modeling described in above, but will also include the additional
data on risk factors that will be obtained from the interviews of cases or their proxy
respondent and the matched controls.
6.9.
Statistical Power Characteristics
A primary objective of our proposed cohort study is to evaluate mortality risks with
emphasis on malignant neoplasms, in particular, lung cancer. Thus, an assessment of the
study’s statistical power to detect important cancer excesses is an important consideration.
Because cancer in general and specifically lung cancer are both highly prevalent diseases
(especially in older males), we are confident that we will obtain an adequate number of
cases for sufficient statistical power to detect a true 1.5 or greater mortality risk for all
cancers combined and lung cancer. We estimated power using:
1)
estimated cohort size of 21,000 individuals (≈8,500 US and ≈12,500 EU)
2)
estimated range of average follow-up time of 25-30 years
3)
US age-adjusted rates for 1980 white males aged 25+ years (all cancer –
407/100,000; lung cancer – 130/100,000)
Based on these calculations, we estimate between 2,140 and 2,450 all cancer deaths, of
which 680-800 will be due to lung cancer.
6.9.1. Cohort study
Based on the above numbers, the power of detecting a true 1.5-fold or larger excess in total
cancer and lung cancer deaths is essentially 1.0. We recognize that the statistical power will
be less to detect excesses within separate plants or other relevant study subgroups, however,
our estimated number of deaths includes a surplus number of deaths that will enable us to
achieve good to excellent power in most of the larger subgroups examined.
Page 93 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
6.9.2. Case-control study
For our nested case-control study of lung cancer, the power of detecting a true 1.5-fold or
larger excess risk is greater than 95% based on 1:1 case:control matching and assuming the
proportion of controls exposed is 30%. The large number of lung cancer deaths we expect
to observe in the cohort study includes a surplus number of deaths sufficient for maintaining
good to excellent statistical power while accounting for the additional sample size
requirements needed to assess confounding and effect modification.
6.10. Strengths and Weaknesses of the Proposed Study
The strengths of the proposed study can be summarized as follows:
1.
The study represents the joint efforts of a nationally and internationally recognized
occupational health research team with more than 30 years of experience
designing and conducting historical cohort and case-control studies of the types
proposed herein, including the largest occupational cohort, incidence and casecontrol study of brain cancer ever conducted.
2.
The UIC and UPitt investigators share a long history of highly successful and
productive collaborative research, as evidenced by the many jointly authored peerreviewed publications cited in their respective curricula vitae.
3.
The proposed historical cohort study design and nested case-control study of lung
cancer, which will enable analytic adjustments for smoking and co-exposures to
known or suspected carcinogens, will provide the best available estimates of total
and cause-specific mortality risks among workers, overall, and in relation to
occupational WCCo exposure.
4.
A particular strength of this study is the ability to characterize the working history
of study members relative to WCCo exposure and co-exposures to other known or
suspected carcinogens. The UIC exposure assessment team plans to use a variety
of statistical and other estimation methods to assign meaningful and scientifically
defensible exposure estimates to workers over time.
5.
Based on our estimates, the statistical power of the proposed cohort study to detect
epidemiologically important (1.5-fold or greater) overall excesses in all cancers
combined and in lung cancer is essentially 1.0. The study affords a sufficiently
long time period for potential WCCo exposure and a sufficiently long observation
period to observe cancer outcomes in relation to WCCo exposure. Therefore, our
proposed study is able to detect a true increased risk or to conclude that there is no
increased risk if one is not detected. Additionally, because the number of expected
cancers is so large, the power necessary to detect 1.5 fold or greater risks in larger
subgroups of the cohort will also be in the good to excellent range.
6.
Also based on our independent estimates, the power of the nested case-control
study of lung cancer to detect epidemiologically important (1.5-fold or greater)
excesses in relation to key study factors is in the excellent range (95% or greater).
Page 94 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
This focused sub-study will also allow adjustment for potential confounding by
smoking in addition to co-exposures to known or suspected carcinogens.
7.
The addition of Co production companies to the study would be a large advantage
of the Phase 3 study over previous studies of WCCo workers. However, the
inability to include subjects with Co-only exposure does not represent a fatal flaw
to the main study design. The Phase 3 WCCo worker epidemiology study will be
comprehensive, scientifically sound and far superior overall to the existing
epidemiology studies. The limited orthogonal contrasts for Co and WC simply
suggests that we may be unable to sort out completely the contribution of each
exposure alone if increased lung cancer mortality risks are observed among
subjects with combined exposures.
8.
The historical cohort study can form the basis for ongoing mortality surveillance
of the workers with potential occupational exposure to WCCo.
The weaknesses of the proposed study can be summarized as follows:
1.
2.
Although it appears from the Phase 1 and Phase 2 studies that much of the data
necessary to adequately address the question regarding WCCo exposure and lung
cancer exists, we may find that some records are unavailable. We believe,
however, that we have taken every reasonable approach to resolve or work around
these limitations in designing the proposed study.
Although the cohort study has good to excellent statistical power to detect
important excesses in mortality from all cancers combined and lung cancer in the
total cohort and its larger subgroups, the power will be less to detect excesses in
smaller subgroups of the total study population, such as factor-specific groups
within study site. The same feature will also apply to the case-control study.
3.
Because a large and diverse number of agents are used or produced at the plants, it
may not be possible to identify the specific etiologic agent or combination of
agents if an overall excess in cancer mortality is found. This is a limitation of all
epidemiology studies of this type that attempt to relate mortality outcomes to
specific chemical exposures. We have, to the extent possible, designed all aspects
of our study to offset or mitigate this limitation.
4.
The use of external adjustment for confounding by smoking in the German sites
has some limitations. Although we will attempt to estimate the patterns of
smoking among WCCo exposed workers from information available in the peerreviewed literature, there remains the chance that these estimates are not truly
representative of the smoking prevalence in the worker cohorts. The smoking
rates will most likely be based only on one time period which would not reflect
temporal changes in smoking habits which can occur, particularly over the long
duration of an historical cohort study. We may also be limited by the extent to
which detailed smoking information is available in the literature.
On balance, we believe that the strengths of the proposed study outweigh its weaknesses.
We are also confident that our investigation will produce scientifically sound, meaningful
Page 95 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
and defensible results, and will provide a significant contribution to the body of knowledge
concerning the health implications of exposure to WCCo.
6.11. Qualifications of the Research Teams
6.11.1. University of Pittsburgh
For more than 45 years, the UPitt, Department of Biostatistics (BIOS) has been one of the
leading academic centers of occupational and environmental health research in the United
States. BIOS faculty have been active in the development and application of biostatistical
methods to study potential health effects of workplace exposures in a variety of industrial
settings.
The Center for Occupational Biostatistics and Epidemiology (COBE) was established in
February 2008 as a specialty research center within the Department of Biostatistics (BIOS)
in UPitt’s Graduate School of Public Health (GSPH). The mission of the COBE is to build
further upon existing departmental strengths in occupational biostatistics and epidemiology,
to enhance collaborative research across departments and schools at UPitt, to promote both
national and international recognition of these fields of strength and to increase
opportunities for external collaboration and programmatic funding.
Gary M. Marsh, Ph.D., F.A.C.E., Professor of Biostatistics is the Director of the COBE;
Jeanine M. Buchanich, M.Ed., Ph.D., Research Assistant Professor of Biostatistics is
Deputy Director of Epidemiology and Ada O. Youk, Ph.D., Research Assistant Professor of
Biostatistics is Deputy Director of Biostatistics. COBE research and administrative staff
include two master’s level biostatisticians, two master’s level information science
specialists, one computer programmer, two research specialists and four technical/clerical
support staff including graduate student researchers and a professional telephone
interviewer.
The UPitt group has conducted occupational studies to investigate the long-term health
effects of exposure to such agents as man-made mineral fibers, formaldehyde, acrylamide,
acrylonitrile, arsenic, petrochemicals, aromatic amines and pharmaceuticals. They have
also applied their expertise in occupational epidemiological research to environmental
epidemiologic studies of communities exposed to industrial pollutants or to hazardous waste
site materials.
Currently, the UPitt group is conducting an historical cohort study of nearly a quarter
million jet engine manufacturing workers for the Pratt & Whitney Company, a mortality
surveillance system for the Owens Corning Company and an historical cohort study of
pharmaceutical workers for the Eli Lilly Company. The Pratt &Whitney study is a
collaborative effort with the Department of Neuro-Oncology within UPMC and UIC.
6.11.2. University of Illinois at Chicago
Page 96 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
UIC’s Environmental and Occupational Health Sciences (EOHS) Division is housed within
the School of Public Health and its goal is to protect the environment and improve the
health of workers and the general public. The Illinois Occupational and Environmental
Health and Safety Education and Research Center (Illinois ERC) was established in 1977 as
one of the first National Institute of Occupational Safety and Health (NIOSH) Educational
Resource Centers in the US.
The Division has a nationally recognized program in IH that is accredited by the
Accreditation Board for Engineering and Technology. Within the division, the research
carried out by the occupational epidemiology team includes mathematical modeling,
engineering, industrial and environmental field studies and general occupational hygiene.
In addition to the mathematical, engineering, aerosol physics and industrial hygiene
expertise, the team can draw upon the medical expertise within the division. Currently, the
UIC team is engaged in several projects, three of which are in collaboration with the
University of Pittsburgh team. Before the formation of the UIC team, the collaboration in
large scale industrial epidemiology studies between the UPitt and UIC principal
investigators started in 1975 and has continued more or less unbroken ever since.
Nurtan A. Esmen, Ph.D., FAIHA, FRSH, is a Professor of EOHS; Steven E. Lacey, Ph.D.,
CIH, CSP, is an Assistant Professor of EOHS and is Director of the Illinois ERC Industrial
Hygiene Program. The UIC team also includes a project manager and a senior research
scientist.
Page 97 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
7.
Phase 3 Study - Administrative Details
7.1.
Project Structure
UPitt will serve as the main contractor and will provide the epidemiology and biostatistics
component of the proposed cohort mortality study of workers potentially exposed to WCCo.
UIC will serve as a subcontractor to UPitt and will direct the exposure reconstruction
component. The work of the country-specific investigators and the data processing
subcontractor will also be overseen by UPitt.
7.2.
Period of Performance
The work proposed herein for the Phase 3 study is anticipated to take approximately four to
five years to complete. Part 1 of the Phase 3 study is anticipated to begin in November
2008 or following receipt of pending funds from the State of Pennsylvania Department of
Health (PADOH). Subsequent parts will be started as funding becomes available.
7.3.
Investigators
The UPitt contract will be directed by Gary M. Marsh, Ph.D., Professor of Biostatistics,
who will be Principal Investigator. Jeanine M. Buchanich, Ph.D., Research Assistant
Professor of Biostatistics and Ada O. Youk, Ph.D., Research Assistant Professor of
Biostatistics will be Co-Investigators with Dr. Marsh. The UIC subcontract will be directed
by Nurtan Esmen, Ph.D., Professor of Environmental and Occupational Health Sciences,
and Steven Lacey, Ph.D., Assistant Professor of Environmental and Occupational Health
Sciences, will be Co-Investigator with Dr. Esmen. The investigators’ biosketches
investigators are available in Appendix C.
7.4.
Progress Reports
Reports will be issued to the sponsor annually and at the end of the project. Investigators
will also prepare manuscripts for publication in peer-reviewed journals throughout the
project period.
7.5.
Data Confidentiality
The Principal Investigators will maintain the confidentiality of all hard copy and electronic
records, assuring that information is kept in locked files (and password protected electronic
media files) and that persons working with these records are made aware of their
Page 98 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
confidentiality. A Confidentiality Statement Form will be executed and kept on file for
each individual working with these records. All UPitt staff will also sign the required NDIPlus Supplemental Assurance Form to ensure the confidentiality of NDI-Plus vital status
and cause of death data.
According to university guidelines, upon funding of the proposed research project this
protocol will be submitted to the respective IRB’s of UPitt and UIC.
7.6.
Quality Assurance and Quality Control Features of Proposed Study
7.6.1. Good Epidemiology Practices Guidelines
During the preparation of this proposal and the performance of the contract, UPitt and UIC
have/will adhered/adhere strictly to the Good Epidemiology Practices Guidelines (GEP)
described by Cook (1991). The GEP provides guidance regarding protocol development,
reporting, quality assurance of data maintenance and documentation of analytic procedures.
7.6.2. Metrics Used to Ensure Data Quality and to Determine Progress
Standard UPitt data checks will be used throughout the proposed study to ensure the
integrity of all study data. This will include a formal check of the completeness and
accuracy of the cohort enumeration and vital status tracing, as well as comprehensive audits
of all primary study data coding and keying. For example, the coding and key-entering of
all primary study data will be 100% by a second data coding clerk. UPitt staff will strive to
achieve cohort completeness, follow-up and cause of death ascertainment rates of at least
95%.
Page 99 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
8.
Project Budget Justification
The proposed Phase 3 Study is anticipated to take approximately four to five years to
complete. Part 1 of the Phase 3 study is anticipated to begin in November 2008 or
following receipt of pending funds from the PADOH. Subsequent parts of Phase 3 will be
started as additional funding becomes available.
The PADOH has stated their intention to provide UPitt with $670,000 in direct costs for
Part 1 of Phase 3 of the full epidemiology study and they have received a detailed
application from UPitt for these funds. The initiation of Phase 3 Part 1 is dependent upon
the receipt of the funds. Subsequent parts of Phase 3 are contingent upon procuring
additional funding sources and, at that time, the specific tasks and detailed budgets will be
provided to the sponsor.
We estimate that the total costs of the Phase 3 study will be in the $4-5 million range (direct
costs), depending on the total number of manufacturing sites included.
Page 100 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
References Cited
Axelson O, Steenland, K. Indirect Methods of Assessing the Effects of Tobacco Use in
Occupational Studies. American Journal of Industrial Medicine 1988:105-118, 1988.
Breslow NE, Day NE. The Design and Analysis of Cohort Studies. In: Statistical Methods
in Cancer Research, Vol. II, International Agency for Research on Cancer, IARC Scientific
Publications No. 82, Lyon, France, 1987.
Buchanich J, Dolan D, Marsh G, et al. Under ascertainment of deaths using Social Security
records: A recommended solution to a little-known problem. American Journal of
Epidemiology..162:193-194, 2005.
Caplan RJ, Marsh GM, Enterline PE. A generalized effective exposure modeling program
for assessing dose-response in epidemiologic investigations. Comput Biomed Res. 16:587596, 1984.
Cook RR: Overview of good epidemiologic practices. J Occup Med. 33(12):1216-20,
1991.
Cox DR. Regression models and life tables (with discussion). J R Stat Soc. 34B:187-220,
1972.
Cox DR. Partial likelihood. Biometrika 62:269-276, 1975.
Doll R: Occupational Cancer: A Hazard for Epidemiologists. Inter J Epidemiol. 14: 22-31,
1985.
Esmen NA: Retrospective industrial hygiene surveys. Amer. Ind. Hyg. Assoc. J. 40:58-65,
1979.
Esmen NA: Exposure estimation in four major epidemiologic studies in acrylonitrile
industry Scand. J. Work Environ Health. 24:Sup2:63-70, 1998.
Esmen NA, Kennedy KJ, Hall TA, Phillips ML, Marsh GM. Classification of Worker
Exposures. Chemico-Biological Interactions. 166:245-253, 2007a.
Esmen NA, Hall TA, Phillips ML, Marsh GM. Chemical process based reconstruction of
exposures for an epidemiological study: I. Theoretical and Methodological issues.
Chemico-Biological Interactions, 166:254-263, 2007b.
Esmen NA, Hall TA, Phillips ML, Jones EP, Basara H, Marsh GM, Buchanich JM.
Chemical process based reconstruction of exposures for an epidemiological study: II.
Estimated exposures to Chloroprene and Vinyl Chloride. Chemico-Biological Interactions,
166:264-276, 2007c.
Hogstedt, C. and Alexandersson, R.. Mortality among hard metal workers. Arbete Hälsa,
21, 1-26, 1990.
Lasfargues, G., Wild, P., Moulin, J.J., Hammon, B., Rosmorduc, B., Rondeau du Noyer, C.,
Page 101 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
Lavandier, M. and Moline, J.J. Lung cancer mortality in a French cohort of hard-metal
workers. Am. J. Ind. Med., 26, 585-595. 1995.
Marsh GM, Youk AO, Stone RA, Sefcik S, Alcorn CW: OCMAP-PLUS, A New Program
for the Comprehensive Analysis of Occupational Cohort Data. J Occup Environ Med.
40:351-362, 1998.
Marsh GM, Ehland J, Sefcik S, Alcorn C. Mortality and Population Data System (MPDS).
Pittsburgh, PA: University of Pittsburgh (Department of Biostatistics Technical Report),
2005.
Moulin JJ, Wild P, Mur JM, Fournier-Betz M, Mercier-Gallay M. A Mortality Study of
Cobalt Production Workers: An Extension of the Follow-Up. American Journal of
Industrial Medicine. 23:281-288, 1993.
Moulin, J.J., Wild, P., Romazini, S., Lasfargues, G., Peltier, A., Bozec, C., Deguerry, P.,
Pellet, F. and Perdrix, A. Lung cancer risk in hard metal workers. Am. J. Epidemiol., 148,
241-248. 1998.
Mur JM, Moulin JJ, Charruyer-Seinerra MP, Lafitte J. A Cohort Mortality Study Among
Cobalt and Sodium Workers in an Electrochemical Plant. American Journal of Industrial
Medicine. 11:75-81, 1987.
Phillips ML, Esmen NA. Computational Method for ranking task-specific exposures using
multi-task time-weighted average samples. Ann Occup. Hyg. 43:201-213, 1999.
Phillips ML, Esmen NA, Costantino J. The Reliability of Multiple Regression and an
Alternative Method for Extracting Task-Specific Exposure Estimates from Time-Weighted
Average Data. App. Env. and Occup. Hyg. 16:1-10, 2001.
Schell J.D., MacNair D.J. and Tollerud, D.J.. Epidemiological investigation feasibility
study prepared for the International Tungsten Industry Association. 2006.
STATA Statistical Software: Release 6.0. College Station, TX, STATA Corp., 2007.
Steenland K, Greenland, S. Monte Carlo Sensitivity Analysis and Bayesian Analysis of
Smoking as an Unmeasured Confounder in a Study of Silica and Lung Cancer. American
Journal of Epidemiology 160:384-392, 2004.
Wild, P., Perdix, A., Romazini, S., Moulin, J.J. and Pellet, F. Lung cancer mortality in a
site producing hard metals. Occup. Environ. Med., 57, 568-573. 2000.
Youk AO, Marsh GM, Stone RA, Buchanich JM, Smith TJ. Historical Cohort Study of
U.S. Man-Made Vitreous Fiber Production Workers III: Analysis of Exposure-Weighted
Measures of Respirable Fibers and Formaldehyde in the Nested Case-Control Study of
Respiratory System Cancer. J Occ Env Med 43(9): 767-778, 2001.
Page 102 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
Appendix A
Phase 2 Survey Instrument
Page 103 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
TUNGSTEN INDUSTRY PHASE TWO STUDY
University of Pittsburgh Epidemiology Component
1. In what year did plant operations begin?
2. How many employees:
a. Currently?
b. At plant start up?
c. Peak employment period(s)?
d. When was (were) the peak employment period(s)?
e. How much turnover is there (i.e., on average, what percentage of the workforce
terminates employment each year)?
3. Are detailed work history records available for all employees since the year that plant
operations began?
a. If no, what type of employee records may be missing (terminated, retired)?
b. If no, for what years might records be missing?
4. In what format are the records?
a. Does the format vary by time period?
b. What format(s) is/are used for the time periods identified?
5. Do records have the following information?
a. Complete name?
b. Social security number (US)/Other unique ID (non-US)?
i. If non-US is answered “no”, is a corresponding identifying number used in
this country for vital status tracing?
ii. What is this number called and how is it used?
c. Date of birth?
d. Gender?
e. Race or ethnicity?
Page 104 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
University of Illinois at Chicago Exposure Reconstruction Component
1. What products or materials has the plant produced?
2. Has the plant ever produced or used the following materials?
a. Tungsten
b. Tungsten carbide
c. Other carbides (e.g., titanium, tantalum, niobium)
d. Cobalt
e. Nickel
f. Chromium
g. Powdered metals
h. Any other materials not mentioned
3. Were any of the following processes ever performed at the plant?
a. Metal powder production
b. Mixing, granulating, palletizing, green shaping, or pressing of metal powder
c. Hardmetal finishing, grinding, or sharpening
d. Welding, brazing, or sintering
e. Foundry operations
f. Surface treatment (e.g., plasma spray, chemical vapor deposition)
g. Any other processes not mentioned
4. Was industrial hygiene monitoring (e.g., air sampling) ever performed at the plant?
a. If yes, are these records accessible?
4. Does the plant maintain any engineering process records?
a. If yes, what types of information do the records contain?
Page 105 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
5.
Appendix B
ICDA Defined Cause of Death Categories
Page 106 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
Appendix A
Causes of Death Categories and Revision-Specific International Classification
of Disease (ICD) Codes Used in Mortality Analysis
Cause of Death Category
6th & 7th
Revision
(1950-67)
8th Revision
(1968-78)
9th Revision
(1979-1998)
10th Revision
(1999+)
01
All Causes of Death
001-999
000-999
001-999
A00-Y89
02
Tuberculosis
001-019
010-019
010-018
A15-A19
03
All Malignant Neoplasms
140-205
140-209
140-208
C00-C97
04
Buccal Cavity and Pharynx
140-148
140-149
140-149
C00-C14
05
Digestive Organs and Peritoneum
150-159
150-159
150-159
C15-C26, C48
06
Esophagus
150
150
150
C15
07
Stomach
151
151
151
C16
08
Large Intestine
153
153
153
C18
09
Rectum
154
154
154
C20-C21
10
Biliary Passages and Liver Primary
155
155,156
155,156
C22,C24
11
Pancreas
157
157
157
C25
12
All Other Digestive
152,156,158,159
152,158,159
152,158,159
C17,C19, C23,
C26,C48
13
Respiratory System
160-164
160-163
160-165
C30-C39
14
Larynx
161
161
161
C32
15
Bronchus, Trachea, Lung
162,163
162
162
C33-C34
16
All Other Respiratory
160,164
160,163
160,163,164,165
C30-C31,
C37-C39
17
Breast
170
174
174,175
C50
18
All Uterine (female only)
171,172-174
180,181,182.0 ,
182.9
179,180,181,182
C53-C55
19
Cervix (female only)
171
180
180
C53
20
Other Female Genital Organs
(female only)
175,176
183-184
183-184
C51-C52,
C56-C58
21
Prostate (male only)
177
185
185
C61
22
Testis and Other Male Genital
Organs (male only)
178,179
172.5,173.5,186
187
186,187
C60,C62-C63
23
Kidney
180
189.0,189.1,189.2
189.0,189.1,189.2
C64-C65
24
Bladder and Other Urinary Organs
181
188,189.9
188,189.3,189.4,
189.8, 189.9
C66-C68
25
Malignant Melanoma of Skin
190
172.0-172.4
172.6-172.9
172
C43
26
Eye
192
190
190
C69
27
Central Nervous System
193
191,192
191,192
C70-C72
Label
Page 107 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
Label
Cause of Death Category
6th & 7th
Revision
(1950-67)
8th Revision
(1968-78)
9th Revision
(1979-1998)
10th Revision
(1999+)
28
Thyroid Gland and Other
Endocrine Glands and Related
Structures
194,195
193,194
193,194
C73-C75
29
Bone
196
170
170
C40-C41
30
All Lymphatic and Hematopoietic
Tissue
200-205
200-209
200-208
C81-C96
31
Hodgkins Disease
201
201
201
C81
32
Non-Hodgkins Lymphoma
200, 202, 205
200, 202
200, 202.0, 202.1,
202.8, 202.9
C82, C83.0C83.8, C84,
C85.1-C85.9
33
Leukemia and Aleukemia
204
204-207
204-208
C91-C95
34
All Other Lymphatic and
Hematopoietic Tissue
203
203, 208, 209
202.2, 202.3,
202.4, 202.5,
202.6, ,203
C88, C90, C96
35
All Other Malignant Neoplasms
165,191,197-199
171,173.0-173.4
173.6-173.9
195-199
171,173 , 195199
C44-C47,
C49,C76-C79,
C80, C97
36
Benign Neoplasm
210-239
210-239
210-239
D10-D36
37
Diabetes Mellitus
260
250
250
E10-E14
38
Cerebrovascular Disease
330-334
430-438
430-438
I60-I69
39
All Heart Disease
400-402,410-443
390-398,400.1
400.9,402,404
410-414,420-429
390-398,402,404
410-429
I00-I02,I05-I09,
I11, I13-I14,
I20-I28,I30-I52
40
Rheumatic
400-402,410-416
390-398
390-398
I00-I02,I05-I09
41
Ischemic
420,422.1
410-414
410-414
I20-I25
42
Chronic Disease of Endocardium
and Other Myocardial Insufficiency
421,422.0,422.2
424,428
424,428
I33-I41
43
Hypertension with Heart Disease
440-443
400.1,400.9,402
404
402,404
I11,I13
44
All Other Heart Disease
430-434
420-423
425-427,429
415-417,420-423
425-427,429
I26.0, I27-I28,
I30-I32, I42-I43,
I44-I52
45
Hypertension w/o Heart Disease
444-447
400.0,400.2
400.3,401,403
401,403,405
I10, I12, I15
46
Nonmalignant Respiratory Disease
241,470-527
460-519
460-519
J00-J99
47
Influenza and Pneumonia
480-483,490-493
470-474,480-486
480-487
J10-J18
48
Bronchitis, Emphysema, Asthma
501,502,527.1,241
490-493
490-493
J40-J46
49
Bronchitis
501,502
490,491
490,491
J40-J42,J44
50
Emphysema
527.1
492
492
J43
51
Asthma
241
493
493
J45-J46
Page 108 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
Label
Cause of Death Category
6th & 7th
Revision
(1950-67)
8th Revision
(1968-78)
9th Revision
(1979-1998)
10th Revision
(1999+)
460-466
500-519
460-466 ,470478,
494-496,500-519
J00-J06,J20-J22,
J30-J39, J47,
J60-J70,J80-J86,
J90-J99
52
Other Nonmalignant Respiratory
470-475,500,510527.0,527.2
53
Ulcer of Stomach and Duodenum
540,541
531-533
531-533
K25-K27
54
Cirrhosis of Liver
581
571
571
K70,K74
55
Nephritis and Nephrosis
590-594
580-584
580-589
N00-N29
56
All External Causes of Death
800-999
800-999
E800-999
V01-Y89
57
Accidents
800-962
800-949
E800-949
V01-X59
58
Motor Vehicle Accidents
810-835
810-823
E810-825
V01-V99
59
All Other Accidents
800-802,840-962
800-809,824-949
E800-807,E826949
W00-X59
60
Suicides
963,970-979
950-959
E950-959
X60-X84
61
Homicides and Other External
964,965,980-999
960-978
980-999
E960-978
E980-999
X85-Y36,
Y40-Y89
000-009
020-136
240-246
251-389
440-458
520-530
534-570
572-577
590-796
001-009
020-139
240-246
251-389
440-459
520-530
534-570
572-579
590-799
A00-A09,
A20-B19,
B25-B99,
D00-D09,
D37-D89,
E00-E07,
E15-G99,
H00-H99,
I70-I99,
K00-K23,
K28-K67,
K71-K73,
K75-K93,
L00-L99,
M00-M99,
N30-R99
not applicable
042-044, 795.8
B20-B24
62
All Other Causes
020-138,206-207,
240,242-254,270326,340-398,450468,530-539,542580,582-587,600795
63
Acquired Immunodeficiency
Syndrome (AIDS) (from 1987)
not applicable
Page 109 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
Appendix C
Biosketches of Investigators
Page 110 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
BIOGRAPHICAL SKETCH
Provide the following information for the key personnel in the order listed for Form Page 2.
Follow the sample format for each person. DO NOT EXCEED FOUR PAGES.
NAME
POSITION TITLE
Gary M. Marsh, Ph.D., F.A.C.E.
Professor of Biostatistics
Director, Center for Occupational Biostatistics and
Epidemiology
EDUCATION/TRAINING (Begin with baccalaureate or other initial professional education, such as nursing, and include postdoctoral training.)
INSTITUTION AND LOCATION
University of Pittsburgh, Pittsburgh, PA
University of Pittsburgh, GSPH
University of Pittsburgh, GSPH
DEGREE
(if applicable)
YEAR(s)
FIELD OF STUDY
B.S.
M.S. (Hyg.)
Ph.D.
1973
1974
1977
Mathematics
Biostatistics
Biostatistics
A. Positions and Honors
Positions and Employment
1978 – 84 Assistant Professor of Biostatistics, Univ. of Pittsburgh, Graduate School of Public Health
(GSPH)
1983 – 92 Assistant Director, Center for Environmental Epidemiology Univ. of Pittsburgh, GSPH
1984
1984 – 91
1991-date
2007
2008-date
Faculty, Graduate Summer Session in Epidemiology, Univ. of Minnesota, School of Public
Health
Associate Professor of Biostatistics, Univ. of Pittsburgh, GSPH
Professor of Biostatistics, Univ. of Pittsburgh, GSPH
Interim Chair, Dept. of Biostatistics, Univ. of Pittsburgh, GSPH
Director, Center for Occupational Biostatistics and Epidemiology, Univ. of Pittsburgh, GSPH
Other Experience and Professional Memberships
1974-date American Statistical Association
-Secretary, Vice President, President-Pittsburgh Chapter, 1979-82
-National Council Representative, 1981-1982
1974-date Biometric Society
1978-date Society for Occupational and Environmental Health
-National Governing Council, 1986-1989
1979-date Society for Epidemiological Research
1986-date Pennsylvania Public Health Association
-Member, Board of Directors, 1989-92
1988-date International Society for Environmental Epidemiology
1996-date International Commission on Occupational Health
1997-date Fellow, American College of Epidemiology (F.A.C.E.)
Honors
1973
1981
1994
1997
1999
2006, 08
B.S. Mathematics, cum laude
Adolf G. Kammer Merit in Authorship Award for Best Publication in Field of Occupational
Health, Principal Author
Outstanding Teacher Award, University of Pittsburgh GSPH
Fellow, American College of Epidemiology
50 at 50 Award, selected as one of the 50 outstanding contributors in the field of public health
in the 50 year history of the Graduate School of Public Health
University of Pittsburgh Innovator Award 2006, 2008
Page 111 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
6.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
B. Selected Peer-Reviewed Publications (Publications selected from 127 peer-reviewed publications)
MARSH GM, Ehland J, Paik M, Preininger M, Caplan R: OCMAP/PC: A User Oriented Cohort
Mortality Analysis Program for the IBM PC. The American Statistician 40:308-309, 1986.
MARSH GM: A Strategy for Merging and Analyzing Work History Data in Industry-wide Occupational
Epidemiology Studies. American Industrial Hygiene Association Journal, 48:414-419, 1987.
MARSH GM, Costantino JP, Lyons EE, Logue JN, and Fox JM: Health Effects of Exposure to the
Drake Chemical Company Superfund Site: Morbidity Patterns Among Former Employees. Journal of
Environmental Health 50:389-394, 1988.
MARSH GM, Co-Chien H, Rao BR, and Ehland J: OCMAP: Module 6-A New Computing Algorithm
for Proportional Mortality Analysis. American Statistician 43:127-128, 1989.
MARSH GM, Callahan C, Pavlock D, Leviton LC, Talbott E, Hemstreet G: A Protocol for Bladder
Cancer Screening and Medical Surveillance Among High Risk Groups: The Drake Health Registry
Experience. Journal of Occupational Medicine 32:881-886, 1990.
MARSH GM, Leviton LC, Talbott E, Callahan C, Pavlock D, Hemstreet G, Logue JN, Fox J, Schulte
P: The Drake Chemical Workers Health Registry Study: I. Notification and Medical Surveillance of a
Group of Workers at High Risk of Developing Bladder Cancer. American Journal of Industrial
Medicine 19:291-302, 1991.
MARSH GM, Enterline PE and McCraw D: Mortality Patterns Among a Cohort of Petroleum Refinery
and Petrochemical Plant Workers. American Journal of Industrial Medicine 19:29-42, 1991.
MARSH GM, Day R: A Model Standardized Risk Assessment Protocol for Use with Hazardous
Waste Sites. Environmental Health Perspectives 90:199-208, 1991.
MARSH GM, Stone RA, Henderson V: A Reanalysis of the National Cancer Institute Study on
Mortality Among Industrial Workers Exposed to Formaldehyde. Journal of Occupational Medicine
34:42-44, 1992.
MARSH GM, Stone RA, Esmen NA, Henderson VL: Mortality Among Chemical Plant Workers
Exposed to Formaldehyde and Other Substances. Journal of the National Cancer Institute 86:384385, 1994.
MARSH GM, Stone RA, Youk AO, Smith TS, Quinn MM, Henderson VL, Schall LC, Wayne LA, Lee
KY: Mortality Among United States Rock Wool and Slag Wool Workers: 1989 Update. Journal of
Occupational Health and Safety - Australia and New Zealand, 12(3):297-312, 1996.
MARSH GM, Stone RA, Esmen NA, Gula MJ, Gause CK, Petersen NJ, Meaney FJ, Rodney, S,
Prybylski D: A Case-Control Study of Lung Cancer Mortality in Six Gila Basin, Arizona Smelter
Towns. Environmental Research 75:56-72, 1997.
MARSH GM, Sefcik S, Alcorn C, Youk AO: OCMAP-PLUS, A New Program for the Comprehensive
Analysis of Occupational Cohort Data. Journal of Occupational and Environmental Health 40:351-362,
1998.
MARSH GM, Stone RA, Esmen NA, Gula MJ, Gause CK, Petersen NJ, Meaney FJ, Rodney S,
Prybylski D: A Case-Control Study of Lung Cancer Mortality in Four Rural Arizona Smelter Towns.
Archives of Environmental Health 53:15-28, 1998.
MARSH GM, Lucas L, Youk AO, Schall LC: Mortality Patterns among Workers Exposed to
Acrylamide: 1994 Follow-Up. Occupational and Environmental Medicine, 56:181-190, 1999.
MARSH GM, Youk AO, Collins J: A Reevaluation of Lung Cancer Risk in the NCI/NIOSH Acrylonitrile
Cohort Study. Scandinavian Journal of Work, Environment and Health 27:5-13, 2001.
MARSH GM, Youk AO, Stone, RA, Buchanich JM, Gula MJ, Smith TJ, Quinn MM: Historical Cohort
Study of U.S. Man- Made Vitreous Fiber Production Workers. I. 1992 Fiber Glass Cohort Follow-UpInitial Findings. Journal of Occupational and Environmental Medicine 43:741-756, 2001.
MARSH GM, Buchanich JM, Youk AO: Historical Cohort Study of U.S. Man-Made Vitreous Fiber
Production Workers. VI.Respiratory System Cancer SMRs Adjusted for the Confounding Effect of
Cigarette Smoking Journal of Occupational and Environmental Medicine 43:803-808, 2001.
MARSH GM, Youk AO, Stone RA, Buchanich JM, Gula MJ, Smith TJ, Churg A, Colby T: Does Fiber
Glass Pose a Respiratory Cancer Risk in Man? Findings from the Latest Update of the U.S. Cohort
Study of Man-Made Vitreous Fiber Workers. Annals of Occupational Hygiene 46(Supp.1): 110-114,
2002.
MARSH GM, Gula MJ, Youk AO, Cassidy LD: Bladder Cancer among Chemical Workers Exposed to
Page 112 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
Nitrogen Products and Other Substances. American Journal of Industrial Medicine 42:286-295, 2002.
MARSH GM, Gula MJ, Roggli V, Churg A: The Role of Smoking and Asbestos Exposure in a
Questionable Case of Mesothelioma. Industrial Health, 41:332-334, 2003.
MARSH GM, Youk AO. Reevaluation of Mortality Risks from Leukemia in the Formaldehyde Cohort
Study of the National Cancer Institute. Regulatory Toxicology and Pharmacology, 40:113-124, 2004.
MARSH Marsh GM, Youk AO, Buchanich JM, Esmen NA. Mortality Patterns among Workers in a U.S.
Pharmaceutical Production Plant. Annals of Epidemiology, 15:112-122, 2005.
MARSH GM, Youk AO. Reevaluation of Mortality Risks from Nasopharyngeal Cancer in the
Formaldehyde Cohort Study of the National Cancer Institute. Regulatory Toxicology and
Pharmacology, 42:275-283, 2005.
MARSH GM, Gula MJ. Employment as a Welder and Parkinson’s Disease among Heavy Equipment
Manufacturing Workers. Journal of Occupational and Environmental Medicine, 48:1031-1045, 2006.
MARSH GM, Youk AO, Buchanich JM, Cunningham M, Esmen NA, Hall TA, Phillips ML. Mortality
Patterns among Industrial Workers Exposed to Chloroprene and Other Substances: I. General
Mortality Patterns. Chemico-Biological Interactions 166:285-300, 2007.
MARSH GM, Youk AO, Buchanich JM, Cunningham M, Esmen NA, Hall TA, Phillips ML. Mortality
Patterns among Industrial Workers Exposed to Chloroprene and Other Substances: II. Mortality in
Relation to Exposure. Chemico-Biological Interactions 166:301-316, 2007.
MARSH GM, Youk AO, Morfeld P. Mis-Specified and Non-Robust Mortality Risk Models for
Naspharyngeal Cancer in the National Cancer Institute Formaldehyde Worker Cohort Study.
Regulatory Toxicology and Pharmacology 47:59-67, 2007.
MARSH GM, Youk AO, Buchanich JM, Kant IJ, Swaen G. Mortality among Workers Exposed to
Acrylamide: Updated Follow-up. Occupational and Environmental Medicine, 49:82-95, 2007.
MARSH GM, Youk AO, Buchanich JM, Erdal S, Esmen NA. Work in the Metal Industry and
Nasopharyngeal Cancer Mortality among Formaldehyde-Exposed Workers. Regulatory Toxicology
and Pharmacology, 48:308-319, 2007.
MARSH GM, Buchanich J, Youk A, Cunningham M, Kennedy K, Lacey S, Hancock R, Esmen N.
Long-Term Health Experience of Jet Engine Manufacturing Workers: I. Mortality from Central Nervous
System Neoplasms. Journal of Occupational and Environmental Medicine 50:1099-1116, 2008.
MARSH GM, Buchanich J, Youk A, Cunningham M, Kennedy K, Lacey S, Hancock R, Esmen N.
Long-Term Health Experience of Jet Engine Manufacturing Workers: II. Total and Cause-Specific
Mortality excluding Central Nervous System Neoplasms. Journal of Occupational and Environmental
Medicine 50:1117-1129, 2008.
Page 113 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
BIOGRAPHICAL SKETCH
Provide the following information for the key personnel in the order listed for Form Page 2.
Follow the sample format for each person. DO NOT EXCEED FOUR PAGES.
NAME
POSITION TITLE
Jeanine M. Buchanich
Research Assistant Professor
EDUCATION/TRAINING (Begin with baccalaureate or other initial professional education, such as nursing, and include postdoctoral training.)
INSTITUTION AND LOCATION
DEGREE
(if applicable)
YEAR(s)
FIELD OF STUDY
BS
MEd
1993
1996
Psychology
School Counseling
MPH
1998
Epidemiology
PhD
2007
Epidemiology
University of Pittsburgh College of Arts & Sciences
University of Pittsburgh School of Education
University of Pittsburgh Graduate School of Public
Health
University of Pittsburgh Graduate School of Public
Health
B. Positions and Honors
Positions and Employment
2008-date
University of Pittsburgh
Research Assistant
Professor
Graduate School of Public Health
2000-2008
University of Pittsburgh
Graduate School of Public Health
Research Specialist V
1998-2000
University of Pittsburgh
Graduate School of Public Health
Research Specialist IV
1996-1998
University of Pittsburgh
Graduate School of Public Health
Research Specialist III
Other Experience and Professional Memberships
1999-date
2006-date
2008-date
Society for Epidemiological Research
Society for Neuro-Oncology
Deputy Director, Epidemiology, Center for Occupational Biostatistics
and Epidemiology, Graduate School of Public Health, University of Pittsburgh
Honors
1989-1993
1990-1993
1993
1995-1996
2008-
Chancellor’s Scholar, Full Scholarship, University of Pittsburgh
Golden Key National Honor Society
B.S., Cum Laude
Chi Sigma Iota National Honor Society in Counseling
Who’s Who Among Executives and Professionals
7.
B. Selected Peer-Reviewed Publications
1.
Schall LC, Buchanich JM, Marsh GM, Bittner G: Utilizing Multiple Vital Status Tracing
Services is Necessary for Attaining Optimal Mortality Follow-up in Cohort Studies. Annals of
Page 114 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
Epidemiology, 11:292-296, 2001.
2.
Buchanich JM, Marsh GM, Youk AO: Historical Cohort Study of U.S. Man-Made Vitreous
Fiber Production Workers. V. Tobacco Smoking Habits. Journal of Occupational and
Environmental Medicine 43:793-802, 2001.
3.
Marsh GM, Youk AO, Buchanich JM, Cassidy LD, Lucas LJ, Esmen NA, Gathuru I.
Pharyngeal Cancer Mortality among Chemical Plant Workers Exposed to Formaldehyde.
Toxicology and Industrial Health, 18:257-268, 2002 (actual publication date January 2004).
4.
Stone RA, Youk AO, Marsh GM, Buchanich JM, Smith TJ, Quinn MM: Historical Cohort
Study of U.S. Man-Made Vitreous Fiber Production Workers IX: Summary of 1992 Mortality
Study Follow-Up and Analysis of Respiratory System Cancer among Female Workers.
Journal of Occupational and Environmental Medicine 46(1):55-67, 2004.
5.
Dolan D, Youk AO, Marsh GM, Buchanich JM: A 50-year Historical Cohort Mortality Study
of Workers in a Pharmaceutical Plant. Journal of Occupational and Environmental Medicine
46(2):161-166, 2004.
6.
Marsh GM, Youk AO, Esmen NE, Buchanich JM. Mortality patterns among workers in a
U.S. pharmaceutical production plant. Annals of Epidemiology 15:112-122, 2005.
7.
Cassidy LD, Buchanich JM, Guice K. Comparison of Injury Severity Scoring Systems to
Identify Most Relevant Variables for Inclusion in a National Trauma Registry for Children.
Journal of Registry Management 32(1):4-10, 2005.
8.
Buchanich JM, Dolan DG, Marsh GM, Madrigano J. Under-Ascertainment of Deaths Using
Social Security Records: A Recommended Solution to a Little-Known Problem. American
Journal of Epidemiology, 162(2):193-4, 2005.
9.
Marsh GM, Youk AO, Buchanich JM, Swaen G, Kant IJ. Mortality Patterns Among Workers
Exposed to Acrylamide: Updated Follow-up. Journal of Occupational and Environmental
Medicine, 49(1):82-95, 2007.
10.
Esmen NA, Hall TA, Phillips ML, Jones EP, Basara H, Marsh GM, Buchanich JM. Chemical
process based reconstruction of exposures for an epidemiological study: II. Estimated
exposures to Chloroprene and Vinyl Chloride. Chemico-Biological Interactions, 166: 264-276,
2007.
11.
Hall TA, Esmen NA, Jones PE, Basara H, Phillips ML, Marsh GM, Youk AO, Buchanich JM,
Leonard R. Chemical Process Based Reconstruction of Exposures for an Epidemiological
Study: III. Analysis of Industrial Hygiene Samples. Chemico-Biological Interactions, 166: 277284, 2007.
12.
Marsh GM, Youk AO, Buchanich JM, Cunningham M, Esmen NA, Hall TA, Phillips ML. Mortality
Patterns among Industrial Workers Exposed to Chloroprene and Other Substances I. General
Mortality Patterns Chemico-Biological Interactions, 166: 285300, 2007.
13.
Marsh GM, Youk AO, Buchanich JM, Cunningham M, Esmen NA, Hall TA, Phillips ML. Mortality
Patterns among Industrial Workers Exposed to Chloroprene and Other Substances II. Mortality in
Relation to Exposure Chemico-Biological Interactions, 166: 301-316, 2007.
14.
Leonard RC, Lineker GA, Kreckmann KH, Marsh GM, Buchanich JM, Youk AO. Comparison of
standardized mortality ratios (SMRs) obtained from use of a reference population based on a
company-wide registry cohort to SMRs calculated against local and national rates. ChemicoBiological Interactions, 166: 317-322, 2007.
15.
Marsh GM, Youk AO, Buchanich JM, Erdal SE, Esmen NE. Work in the Metal Industry May Help
Explain Nasopharyngeal Cancer Mortality Excess among Workers Exposed to Formaldehyde.
Page 115 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested casecontrol study of lung cancer - UK component
Regulatory Toxicology and Pharmacology, 48: 308-319, 2007.
16.
Lippert JF, Lacey SE, Kennedy KJ, Esmen NA, Buchanich JM, Marsh GM. Magnetic field exposure
in a non-destructive testing operation. Archives of Environmental and Occupational Health, 62: 187193, 2007.
17.
Buchanich JM, Cassidy L, Guice K. National Trauma Registry for Children Project: A National
Hospital Survey. Journal of Registry Management, 35:12-17, 2008.
18.
Marsh GM, Buchanich JM, Youk AO, Cunningham M, Lieberman F, Kennedy KJ, Lacey SE,
Hancock RP, Esmen NA. Long-Term Health Experience of Jet Engine Manufacturing Workers: I.
Mortality from Central Nervous System Neoplasms. Journal of Occupational and Environmental
Medicine, 50:1009-1016, 2008.
19.
Marsh GM, Buchanich JM, Youk AO, Cunningham M, Lieberman F, Kennedy KJ, Lacey SE,
Hancock RP, Esmen NA. Long-Term Health Experience of Jet Engine Manufacturing Workers: II.
Total and Cause-Specific Mortality excluding Central Nervous System Neoplasms. Journal of
Occupational and Environmental Medicine, 50:1017-1029, 2008.
20.
Cassidy LD, Cunningham MA, Buchanich JM, Marsh GM, Guice K. Proposed Sampling Plan for a
National Trauma Registry for Children. Journal of Registry Management, 35:113-119, 2008.
21.
Buchanich JM, Songer TJ, Cassidy LD, Marsh GM, Ford HR. A Clinical Decision Making Rule for
Mild Head Injury in Infants & Toddlers. Saarrbrucken: VDM Verlag Dr. Muller, 2008.
Page 116 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested case-control study of lung cancer UK component
BIOGRAPHICAL SKETCH
Provide the following information for the key personnel in the order listed for Form Page 2.
Follow the sample format for each person. DO NOT EXCEED FOUR PAGES.
NAME
POSITION TITLE
Ada O. Youk, Ph.D.
Research Assistant Professor of Biostatistics
EDUCATION/TRAINING (Begin with baccalaureate or other initial professional education, such as nursing, and include postdoctoral training.)
INSTITUTION AND LOCATION
Duquesne University, Pittsburgh, PA
University of Pittsburgh
University of Pittsburgh, GSPH
DEGREE
(if applicable)
YEAR(s)
FIELD OF STUDY
B.S.
M.A.
Ph.D.
1988
1990
1996
Mathematics
Biostatistics
Biostatistics
C. Positions and Honors
Positions and Employment
1988-90 Teaching Assistant, University of Pittsburgh, Department of Mathematics
1990-96 Graduate Student Researcher, University of Pittsburgh, Department of Biostatistics
1996-02 Research Associate, University of Pittsburgh, Department of Biostatistics
2002Research Assistant Professor, University of Pittsburgh, Department of Biostatistics
Other Experience and Professional Memberships
1995-date
Member, Biometric Society (ENAR)
2004
Local Arrangements Chair, Biometric Society (ENAR)
1996-date
Member, American Statistical Association (ASA)
Honors
1984-88
1986
1988
1988
1988
1988-90
1990-96
1997
1997
2004-2005
2006
2007
Partial Competitive Scholarship, Duquesne University
Phi Eta Sigma National Honor Society
B.A., Cum Laude
National Collegiate Mathematics Award
Who’s Who Among American Colleges and Universities
Full Tuition Scholarship & Assistantship, University of Pittsburgh, Mathematics
Full Tuition Scholarship & Assistantship, University of Pittsburgh, Biostatistics
Delta Omega National Honor Society in Public Health
Student of the Year, American Statistical Association, Pittsburgh Chapter
Delta Omega National Honor Society in Public Health, President
University of Pittsburgh Innovator Award
Who’s Who Among American Educators
8. B. Selected Peer-Reviewed Publications (Publications selected from 49 peer-reviewed publications)
Talbott EO, YOUK AO, McHugh K, Shire J, Murphy B. Mortality among the residents of the Three Mile
Island area. Environmental Health Perspectives 2000;108(6):1-8.
Jain A, DiMartini A, Kashyap R, YOUK A, Gray W, Rohal S, Fung J. Long-term Follow-up after Liver
Transplantation for Alcoholic Liver Disease under Tacrolimus. Transplantation 2000; 70(9):1335-1342.
Marsh GM, YOUK AO. Absence of Cancer Risks among Workers Exposed to Acrylonitrile: A
Reanalysis of the NCI/NIOSH Cohort Study Data. Scan J Work, Environ and Health. 2001; 27(1):5-13.
Marsh GM, YOUK AO, Stone RA, Buchanich JM, Gula MJ, Smith TJ, Quinn MM. Historical Cohort
Page 117 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested case-control study of lung cancer UK component
Study of U.S. Man-Made Vitreous Fiber Production Workers: I. 1992 Fiber Glass Cohort Follow-Up Initial Findings. J Occ Env Med 2001; 43(9): 741-756.
YOUK AO, Marsh GM, Stone RA, Buchanich JM, Smith TJ. Historical Cohort Study of U.S. Man-Made
Vitreous Fiber Production Workers III: Analysis of Exposure-Weighted Measures of Respirable Fibers
and Formaldehyde in the Nested Case-Control Study of Respiratory System Cancer. J Occ Env Med
2001;43(9): 767-778.
Stone RA, YOUK AO, Marsh GM, Smith TJ, Quinn MM, Buchanich JM. Historical Cohort Study of U.S.
Man-Made Vitreous Fiber Production Workers IV: Quantitative Exposure-Response Analysis of the
Nested Case-Control Study of Respiratory System Cancer. J Occ Env Med 2001;43(9): 779-792.
Marsh GM, YOUK AO, Stone RA, Buchanich JM, Gula MJ, Smith TJ, Churg A, Colby T. Does Fiber
Glass Pose a Respiratory System Cancer Risk in Humans? Latest Findings from the US Cohort and
Nested Case-control Studies. Ann Occup Hyg 2002;46(1):1-5.
Marsh GM, Gula MJ, YOUK AO, Schall LC: Bladder Cancer among Chemical Workers Exposed to
Nitrogen Products and Other Substances. American Journal of Industrial Hygiene, 2002;42:286-295.
Cassidy LD, YOUK AO, Marsh GM. The Drake Health Registry Study: Cause-Specific Morality
Experience of Workers Potentially Exposed to Beta-naphthylamine. American Journal of Industrial
Medicine, 2003; 44:282-290.
Bloemen LJ, YOUK AO, Bradley TD, Bodner KM, Marsh GM. Lymphohematopoietic Cancer Risk
among Chemical Workers Exposed to Benzene. Occupational and Environmental Medicine, 2004;
61(3):270-274.
YOUK AO, Stone RA, Marsh GM. A Method for Imputing Data in Longitudinal Studies. Annals of
Epidemiology, In press.
Starr TB, Gause CG, YOUK AO, Stone RA, Marsh GM, Collins JJ. A risk assessment for occupational
acrylonitrile exposure using epidemiology data. Risk Analysis, In press.
Stone RA, YOUK AO, Marsh GM, Buchanich JM, Smith TJ. Historical Cohort Study of US Man-Made
Vitreous Fiber Workers IX: Analysis of Respiratory System Cancer Among Female Workers. JOEM,
2004; 46(1):55-67.
Dolan DG, YOUK AO, Marsh GM, Buchanich JM. A 50-Year Historical Cohort Mortality Study of
Workers in a Pharmaceutical Plant. JOEM, 2004;46(2):161-166.
Marsh GM, YOUK AO. Reevaluation of Mortality Risks from Leukemia in the Formaldehyde Cohort
Study of the National Cancer Institute. Regulatory Toxicology and Pharmacology, 2004; 40:113-124.
Wright CE, Zborowski JV, Talbott EO, McHugh-Pemu K, YOUK AO. Dietary Intake, Physical Activity,
and Obesity in Women with Polycystic Ovary Syndrome. International Journal of Obesity & Related
Metabolic Disorders, 2004; 28(8):1026-1032.
Marsh GM, YOUK AO, Buchanich JM, Esmen N. Mortality Patterns among Workers in a US
Pharmaceutical Production Plant. Annals of Epidemiology, 2005; 15(2):112-122.
Marsh GM, YOUK AO. Reevaluation of Mortality Risks from Nasopharyngeal Cancer in the
Formaldehyde Cohort Study of the National Cancer Institute. Regulatory Toxicology and
Pharmacology, 2005; 42:275-283.
Bromberger JT, Kravitz H, Wei HL, Brown C, YOUK AO, Matthews K. History of Depression and
Page 118 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested case-control study of lung cancer UK component
Women’s Current Health and Functioning During Midlife. General Hospital Psychiatry, in press.
Ramos RG, Talbott EO, YOUK AO, Karol MH. Community Urbanization and Hospitalization of Adults
for Asthma, Journal of Environmental Health, 2006; 68(8):26-32.
Marsh GM, YOUK AO, Buchanich JM, Cunningham M, Esmen NA, Hall TA, Phillips ML, Mortality
patterns among industrial workers exposed to chloroprene and other substances: I. General mortality
patterns, Chem.-Biol. Interact., 2007; 166:285-300.
Marsh GM, YOUK AO, Buchanich JM, Cunningham M, Esmen NA, Hall TA, Phillips ML. Mortality
patterns among industrial workers exposed to chloroprene and other substances: II. Mortality in relation
to exposure, Chem.-Biol. Interact., 2007;166: 301–316.
Marsh GM, YOUK AO, Morfeld P. Mis-specified Mortality Risk Models for Naspharyngeal Cancer in the
National Cancer Institute Formaldehyde Worker Cohort Study. Regulatory Toxicology and
Pharmacology, 2007; 47:59-67.
Leonard RC, Lineker GA, Kreckmann KH, Marsh GM, Buchanich J, YOUK AO. Comparison of
Standardized Mortality Ratios (SMRs) Obtained from Use of a Reference Population Based on
Company-Wide Registry Cohort to SMRs Calculated against Local and National Rates. Chem-Biol
Interact, 2007; 166:317-322.
Marsh GM, YOUK AO, Buchanich JM, Kant IJ, Swaen G. Mortality Patterns Among Workers Exposed
to Acrylamide: Updated Followup. Occupational and Environmental Medicine, 2007; 49:82-95.
Hall TA, Esmen NA, Jones PE, Basara H, Phillips ML, Marsh GM, YOUK AO, Buchanich JM, Leonard
R. Chemical Process Based Reconstruction of Exposures for an Epidemiological Study: III. Analysis of
Industrial Hygiene Samples. Chemico-Biological Interactions, 2007;166: 277-284.
Marsh GM, YOUK AO, Buchanich JM, Erdal S, Esmen NA. Work in the Metal Industry May Help to
Explain Nasopharyngeal Cancer Mortality Excess among Workers Exposed to Formaldehyde.
Regulatory Toxicology and Pharmacology, 2007; 48: 308-319.
Bromberger JT, Kravitz HM, Matthews K, YOUK AO, Brown C, Feng W. Predictors of First Lifetime
Episodes of Major Depression in Midlife Women. Psychological Medicine, in press.
Marsh GM, Buchanich JM, YOUK AO, Cunningham M, Lieberman F, Kennedy KJ, Lacey SE,
Hancock RP, Esmen NA. Long-Term Health Experience of Jet Engine Manufacturing
Workers: I. Mortality from Central Nervous System Neoplasms. JOEM, in press.
Marsh GM, Buchanich JM, YOUK AO, Cunningham M, Lieberman F, Kennedy KJ, Lacey SE,
Hancock RP, Esmen NA. Long-Term Health Experience of Jet Engine Manufacturing
Workers: II. Total and Cause-Specific Mortality excluding Central Nervous System
Neoplasms. JOEM, in press.
Page 119 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested case-control study of lung cancer UK component
BIOGRAPHICAL SKETCH
Provide the following information for the key personnel in the order listed on Form Page 2.
Photocopy this page or follow this format for each person.
NAME
POSITION TITLE
Nurtan Alan Esmen
Professor
EDUCATION/TRAINING (Begin with baccalaureate or other initial professional education, such as
nursing, and include postdoctoral training.)
INSTITUTION AND LOCATION
Northeastern University, Boston, MA
University of Pittsburgh, Pittsburgh, PA
University of Pittsburgh, Pittsburgh, PA
DEGREE
(if applicable)
YEAR(s)
B.Sc.
M.Sc.
Ph.D.
1965
1966
1970
FIELD OF STUDY
Engineering
Chem & Air Eng.
Chem / Air Eng & Math
Professional Experience:
Fellow: American Industrial Hygiene Association & Royal Society for the Promotion of Health
University of Illinois (Chicago) – Professor (2003 – to date); University of Oklahoma – Professor (1995 – 2003) and
Chair (1997 - 2002) of Occup. & Environ. Health; Esmen Research - Senior Partner & Principal Scientist (1990 1995); University of Pittsburgh – Professor (1980 – 1993), Program Director of Industrial Hygiene (1980 – 1990)
Associate Professor of Industrial Hygiene Engineering (1975 – 1980); Owens-Corning Fiberglas - Principal Scientist
(1974 – 1975); University of Delaware - Assistant Professor of Environmental Engineering (1970 – 1974); University
of Pittsburgh - Senior Research Staff (1965 – 1970) Harvard School of Public Health - Research Staff (1960 – 1965)
PUBLICATIONS:
(More than 150 articles and abstracts in Occupational. Hygiene, Aerosol Physics, Epidemiology and related subjects.
Only selected recent publications after 2000 are listed.)
JF Lippert, S.E. Lacey, K.J. Kennedy. N.A. Esmen, JM Buchanich and G,M, Marsh : Magnetic Field Exposure in a
Nondestructive Testing Operation, Archives of Environmental and Occupational Health 62:187-193 (2008)
TM Sorahan, , Pang, D., Esmen, N. A. and Sadhra, S: Urinary Concentrations of Toxic Substances: An Assessment of
alternative approaches to adjusting for specific gravity, J Occup. Env, Hyg, 5:721-723 (2008).
GM Marsh Buchanich JM, Youk, AO, Cunnigham MA, Lieberman FS, Kennedy, KJ, Lacey, SE, Hancock, RP,
Esmen, NA : Long-Term Health Experience of Jet Engine Manufacturing Workers: I. Mortality From Central Nervous
System Neoplasms J Occup Environ Med. 50:1099–1116 (2008)
GM Marsh, Buchanich JM, Youk, AO, Cunnigham MA, Lieberman FS, Kennedy, KJ, Lacey, SE, Hancock, RP,
Esmen, NA : Long-term Health Experience of Jet Engine Manufacturing Workers: II. Total and Cause-Specific
Mortality Excluding Central Nervous System Neoplasms J Occup Environ Med. 50:1117–1129 (2008)
GM Marsh, AO. Youk, JM. Buchanich, S. Erdal, NA. Esmen: Work in the Metal Industry May Help Explain
Nasopharyngeal Cancer Mortality Excess among Workers Exposed to Formaldehyde Reg Tox and Pharm. 48:308-319
(2007).
NA Esmen, KJ Kennedy, TA Hall, ML. Phillips, GM Marsh: Classification of Worker Exposures, ChemicoBiological Interactions, 166:245-253(2007)
NA Esmen, TA Hall, ML Phillips, GM Marsh: Chemical process based reconstruction of exposures for an
epidemiological study: I. Theoretical and Methodological issues, Chemico-Biological Interactions, 166:254263(2007)
NA Esmen, TA Hall, ML Phillips, EP Jones, H Basara, GM Marsh, JM Buchanich, Chemical process based
reconstruction of exposures for an epidemiological study: II. Estimated exposures to Chloroprene and Vinyl Chloride,
Chemico-Biological Interactions, 166:264-276(2007)
TA Hall, NA Esmen, EP Jones, H Basara, ML Phillips, GM Marsh, AO Youk, JM Buchanich, RC Leonard,, Chemical
process based reconstruction of exposures for an epidemiological study: III. Analysis of Industrial Hygiene Samples
Chemico-Biological Interactions, 166:277-284(2007)
GM Marsh, AO Youk, JM Buchanich, M Cunningham, NA Esmen, TA Hall, ML Phillips: Mortality patterns among
Page 120 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested case-control study of lung cancer UK component
industrial workers exposed to chloroprene and other substances: I. General mortality patterns, Chemico-Biological
Interactions, 166:285-300(2007)
GM Marsh, AO Youk, JM Buchanich, M Cunningham, NA Esmen, TA Hall, M.L. Phillips, Mortality patterns among
industrial workers exposed to chloroprene and other substances: II. Mortality in relation to exposure, ChemicoBiological Interactions, 166:301-316 (2007)
GM Marsh, AO Youk, JM Buchanich, S Erdal, NA Esmen: Work in the Metal Industry May Help Explain
Nasopharyngeal Cancer Mortality Excess among Workers Exposed to Formaldehyde Reg Tox and Pharm. 48:308-319
(2007).
GA Day, G. A., AB Stefaniak, A.B.,Hoover,M. D., Dickerson,R.M., Peterson,E. J., Esmen, N. A., Scripsick, R. C.:
"Bioavailability of Beryllium Oxide Particles: An In Vitro Study in the Murine J774A.1 Macrophage Cell Line
Model" Experimental Lung Research. 31: 341-360 (2005)
Johnston, KL, Phillips, ML, Esmen, NA, and Hall, TA: Evaluation of an Artificial Intelligence Program for Estimating
Occupational Exposures: Annals of Occ. Hyg. 49:147-153 (2005)
Marsh, GM, Youk, AO, Esmen, NA and Buchanich, JM: Mortality Patterns among Workers in an U.S.
Pharmaceutical Production Plant Annals of Epidemiology 15:112–122(2005).
Phillips, ML, Esmen, NA, Hall, TA, and Lynch, RL: Determinants of Exposure to Volatile Organic Compounds in
Four Oklahoma Cities J. Exp. Anal. and Environ. Epid. 15: 35-46 (2005)
Sorahan, T., and Esmen, N. A.: "Lung Cancer Mortality in UK nickel-cadmium battery workers, 1947-2000" Occup.
Env. Medicine 61:1008-1016 (2004)
Johnson, D. L. and Esmen, N. A.: Method induced exposure misclassification for a respirable dust sampled using
ISO/ACGIH/CEN criteria. Ann Occup Hyg. 48:13-20, (2004)
Esmen, N.A. " Benzene exposure assessments: past practices and future prospects" Proceedings of Workshop on
Leukemia Risks in Relation to Benzene Exposure. TM Sorahan (Edit) Institute of Petroleum, London p15-27(2003).
Marsh, G. M., Youk, A. O., Buchanich, J.M., Cassidy, L.D., Lucas, L.J., Esmen, N. A., Gathuru, I.: Pharyngeal cancer
mortality among chemical plant workers exposed to formaldehyde Toxicology and Industrial Health. !8:257-268
(2002)
Phillips, M. L., Esmen, N. A., Wang, D. and Hall, T. A.: Temporal and Spatial Variation in Monitoring of Urban Air
Pollutants In: Fate and Transport of Chemicals in the Environment: Impacts, Monitoring, and Remediation (R. L.
Lipnick, R. P. Mason, M. L. Phillips, & C. U. Pittman Eds.) American Chemical Society Monograph (2002)
Clinkenbeard, R. E., England, E.C., Johnson, D.L., Esmen, N. A., Hall, T.A., and Carlton, G. “Comparison of the
IOM inhalable aerosol sampler and a modified 37-mm cassette during aircraft corrosion control maintenance” App.
Env. and Occup. Hyg. 17:622-627(2002).
Esmen, N.A., Johnson, D. L., and Agron, G. M.: ”The Variability of Delivered Dose of Aerosols with the Same
Respirable Concentration but Different Size Distributions” Ann Occup. Hyg. 46:401-408(2002)
Collins, J. J., Ness, R., Tyl, R. Krivanek, N., Esmen, N. A., Hall, T. A., : A review of adverse pregnancy outcomes
and formaldehyde exposure in human and animal studies Regulatory Toxicology and Pharmacology 34:17-34 (2001)
Esmen, N. A. and Johnson, D. L.: Simulation Analysis of Inhalable Dust Sampling Errors Using a Multi-Component
Error Model Aerosol Science and Technol. 35:824-828 (2001)
Phillips, M. L., Hall, T. A. Esmen, N. A., Lynch, R. A. and Johnson, D. L. “Use of global positioning system
technology to track subjects’ location during environmental exposure sampling. J. Exposure Analysis and Environ.
Epid. 11: 207-215 (2001).
Phillips . M. L., Esmen, N. A., Costantino, J.: The Reliability of Multiple Regression and an Alternative Method for
Extracting Task-Specific Exposure Estimates from Time-Weighted Average Data App. Env. and Occup. Hyg. 16:110(2001)
Collins, J. J., Esmen, N. A. and Hall, T. A. : A Review and Meta-analysis of Formaldehyde Exposure and Pancreatic
Cancer Amer. J. Indus. Med. 39:336-345.(2001)
Johnson, D. L., Esmen, N. A., Carlson, K.D., Pearce, T. A and Thomas, B. N.: Aerodynamic behavior of lipid
microtubule aerosols. Journal of Aerosol Science 31:181-188 (2000)
Esmen, N. A. and Hall, T. A.: Theoretical investigation of the interrelationship between stationary and personal
sampling in exposure estimation App. Env. and Occup. Hyg. 15:114-119 (2000).
Esmen, N. A.: Multicomponent error model for mass measurement based size fractionating aerosol samplers App.
Env. and Occup. Hyg. 15:72-79 (2000).
Page 121 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested case-control study of lung cancer UK component
9.
BIOGRAPHICAL SKETCH
Provide the following information for the key personnel in the order listed on Form Page 2.
Follow this format for each person. DO NOT EXCEED FOUR PAGES.
NAME
POSITION TITLE
Lacey, Steven Edward
Assistant Professor
EDUCATION/TRAINING (Begin with baccalaureate or other initial professional education, such as nursing, and include postdoctoral training.)
INSTITUTION AND LOCATION
Texas Tech University, Lubbock, TX
Texas A&M University, College Station, TX
University of Illinois at Chicago, Chicago, IL
Johns Hopkins University, Baltimore, MD
DEGREE
(if applicable)
YEAR(s)
BS
MS
PhD
Postdoctoral Fellow
1991-1995
1997-2000
1999-2002
2002-2003
FIELD OF STUDY
Zoology
Industrial Hygiene
Env & Occ Health Science
Env Health Engineering
A. Positions and Honors
Positions and Employment
1997-1998
Emergency Medical Technician, Texas A&M University, College Station, TX
1998
Industrial Hygienist, Amoco Corporation, Houston, TX
1998-1999
Teaching Assistant, Texas A&M University, College Station, TX
1999
Industrial Hygienist, Albemarle Corporation, Houston, TX
1999-2002
Research Assistant, Great Lakes Center for Env & Occ Safety and Health, Chicago, IL
2000-2002
Teaching Assistant, University of Illinois at Chicago, Chicago, IL
2002-2003
Postdoctoral Fellow, Johns Hopkins University, Baltimore, MD
2004-2008
Assistant Research Professor, University of Illinois at Chicago, Chicago, IL
2008-present Assistant Professor, University of Illinois at Chicago, Chicago, IL
Director, Industrial Hygiene Program & Occupational Safety Program
Certified Industrial Hygienist #16269
Certified Safety Professional #19753
Professional Memberships
2003-present American Industrial Hygiene Association, Full Member
2004-2005, AIHA Engineering Committee Chair
2005-2006, AIHA Student & Early Career Professionals Committee Chair
2008-present, AIHA Board of Directors
2006-present International Society of Exposure Analysis, Member
2006-present American Conference of Governmental Industrial Hygienists, Member
2006-present International Occupational Hygiene Association, Affiliate Member
2006-present British Occupational Hygiene Society, Member
2008-present American Society of Safety Engineers, Member
Honors
1995
1998
Texas Tech University Biological Science Honor Student
AIHA, Deep South Section, Fred S. Venable Scholarship
Page 122 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested case-control study of lung cancer UK component
1999-2002
2001
2002
2004
2006
Committee
2006
NIOSH Industrial Hygiene Traineeship, University of Illinois at Chicago
Stockhausen Corporation Scholarship for Industrial Hygiene
Best Poster on Exposure Modeling, American Industrial Hygiene
Conference & Exposition, Graduate Student Section, San Diego, CA
AIHA Outstanding Committee Award, Engineering Committee
AIHA Outstanding Committee Award, Student & Early Career Professionals
President’s Award, AIHA Student & Early Career Professionals Committee
B. Publications and Recent Abstracts
Publications
1. Marsh G, Buchanich J, Youk A, Cunningham M, Lieberman F, Kennedy K, Lacey S, Hancock R, Esmen
N.
Long-term health experience of jet engine manufacturing workers: I. Mortality from central nervous
system neoplasms. J Occ Env Med 50:1099-1116 (2008).
2. Marsh G, Buchanich J, Youk A, Cunningham M, Lieberman F, Kennedy K, Lacey S, Hancock R, Esmen
N.
Long-term health experience of jet engine manufacturing workers: II. Total and cause-specific mortality
excluding central nervous system neoplasms. J Occ Env Med 50:1117-1129 (2008).
3. Kovalsky A, Lacey S, Kaphle U, Vaughn J. Risk perception and water purification practices for waterborne parasitic infections in remote Nepal. Trop Doct 38:229-231 (2008).
4. Lippert, J., Lacey, S., et al. Magnetic field exposure in a nondestructive testing operation. Arch Env
Occ Health 62:187-193 (2007).
5. Lacey, S., Forst, L., et al. Eye injury in migrant farm workers and suggested hazard controls. J Ag
Safety
Health 13:259-274 (2007).
6. Lacey, S., Conroy, L., et al. Dust emission rates from food processing. Ann Agric Environ Med 13:251257
(2006).
7. Lacey, S., Conroy, L., et al. Personal dust exposures at a food processing facility. J Agromed 11:49-58
(2006).
8. Forst, L., Noth, I., Lacey, S., et al. Barriers and benefits of protective eyewear use by Latino farm
workers.
J Agromed 11:11-17 (2006).
9. Forst, L., Lacey, S., et al. Effectiveness of community health workers for promoting use of safety
eyewear
by Latino farm workers. Am J Ind Med 46:607-613 (2004).
Recent Abstracts
1. Lacey, S., Horvatin, S., Kennedy, K., et al. Examination of worker ability to recall personal occupational
history. Abstract and presentation at British Occupational Hygiene Society Conference, Bristol, UK, May
2008.
2. Lacey, S., Esmen, N., Palmer, J., Kennedy, K. Reconstruction of exposures to metalworking fluids using
Page 123 of 124
Tungsten Carbide with a Cobalt Binder: an historical cohort and nested case-control study of lung cancer UK component
industrial time studies. Abstract and presentation at American Industrial Hygiene Conference and
Exposition, Philadelphia, PA, June 2007.
3. Lacey, S., Lippert, J., Esmen, N., Marsh, G. Electromagnetic field exposure in a non-destructive testing
operation. Abstract and presentation at American Industrial Hygiene Conference and Exposition,
Philadelphia, PA, June 2007.
4. Hancock, R., Esmen, N., Lacey, S., et al. Reconstruction of exposures in high temperature alloy surface
grinding. Abstract and presentation at American Industrial Hygiene Conference and Exposition,
Philadelphia, PA, June 2007.
6. Esmen, N., Hancock, R., Lacey, S., Kennedy, K. Exposure to aerosol generated in high temperature
alloy
surface grinding. Abstract and presentation at British Occupational Hygiene Society Conference,
Glasgow,
UK, April 2007.
7. Esmen, N., Lacey, S., Kennedy, K., Hancock, R. Exposure reconstruction strategy to examine
glioblastoma multiforme risk among a cohort of jet engine manufacturing workers. Abstract and
presentation at Society for Neuro-Oncology Annual Scientific Meeting, Orlando, FL, November 2006.
8. Lacey, S., Espinosa, R., et al. Development of a geospatial time dependent information system for
industrial hygiene. Abstract and presentation at American Industrial Hygiene Conference and
Exposition,
Chicago, IL, May 2006.
9. Esmen, N., Lacey, S., et al. Validation of near-field vapour exposure prediction equations for
unventilated
chemical industrial processes. Abstract and presentation at British Occupational Hygiene Society
Conference, Newcastle, UK, April 2006.
10. Lacey, S., Esmen, N., et al. Empirical observations on exposure rates with its implications in exposure
reconstruction. Abstract and presentation at International Society for Exposure Analysis Conference,
Tucson, AZ, November 2005.
Page 124 of 124