primary care physician
advertisement

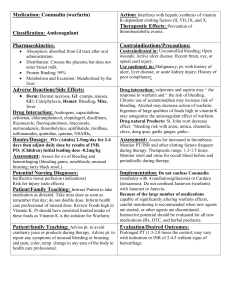
PRIMARY CARE PHYSICIAN: CC:Follow-up anticoagulation. HISTORY: PMHx: DM, HTN, hyperlipidemia Primary Warfarin Indication: Secondary Indication: Indication Description: Atrial Fibrillation Not Applicable No additional comments. Signs/Symptoms Bleeding (See "Heme History" below for details): Nose Bleeds: No Gum Bleeds: No Change in Urine Color: No Change in Stool Color: No Bright Red Blood per Rectum: Yes Abnormal Bruising: No Signs/Symptoms of Potential Embolic Events: No Heme_History: patient reports occasional rectal bleeding with constipation which he contributes to hemorrhoids, unchanged. Current EtOH Use: Current Smoker: No No Changes In (See "Additional History" below for details): Diet: Yes Medications: No Activities / Lifestyle: No Health Status: No Additional History: patient increased intake of vit K foods from once weekly to five times weekly. He continues to consume 2 glasses of wine per week. He notes fasting glucose readings at home ranging from 152 to 180 over the past 2 weeks. He denies hypoglycemic episodes. Denies polyuria, polydipsia, polyphagia. He denies missed doses of any meds. Additional Assessment: INR subtherapeutic likely due to increase in vit K foods; therapeutic at last visit on same dose. DM: uncontrolled; meter download: 14 day avg: 172 Medications were reviewed and updated: Yes Informed Patient or Caretaker: Yes Patient or Caretaker Verbalize Understanding: Yes Warfarin Handout(s) Provided: No ASSESSMENT/PLAN: Well appearing in no acute distress. Date INR: 9/4/2008 Site Test Performed: UNC Goal INR: 2 - 3 INR Results: 1.7 Current Dose: 5mg MWF, 2.5mg TRSS Plan for Warfarin Dose: Increase current dose to 2.5mg MWF, 5mg TRSS. Repeat INR Date: 9/18/2008 2. DM: increase metformin 500mg po bid to 1000mg po bid. Continue to monitor glucose readings, bring meter to follow up visit for further assessment and medication adjustment. Total time spent face-to-face with this patient at this visit was 35 minutes.