Aging Demographics and Psychiatric Diagnoses in the Elderly
advertisement

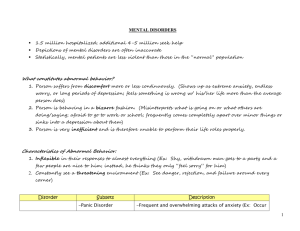
Aging Demographics and Psychiatric Diagnoses in the Elderly Marguerite R. Poreda, MD Assistant Professor USF COM Department of Psychiatry and Behavioral Medicine Training Director Geriatric Psychiatry Associate Director Memory Disorders Clinic Adult, Geriatric and Forensic Psychiatry The views expressed in this presentation are my own and do not necessarily represent those of USF, MacDill AFB, the VA or any other agency of the Federal Government or the State of Florida. The speaker does not receive honoraria, grants or research support from any pharmaceutical company nor is on any pharmaceutical’s Speaker’s Bureau Aging Demographics and Psychiatric Diagnoses in the Elderly: what I will review Aging demographics (baby boomers, the aging population, the ‘old,’ ‘very old,’ ‘oldest old’; what age defines geriatrics?) Understanding psychiatric nomenclature: Axis I - V Psychiatric Diagnoses: Axis I - depression, anxiety, BMD, psychotic disorders, delirium, dementias, alcohol/SA; Axis II – Personality Disorders and Mental Retardation Suicide risk factors Elder abuse, neglect and exploitation What is Geriatric Psychiatry? Fastest growing field of psychiatry; branch of medicine concerned with prevention, diagnosis, and treatment of physical and psychological disorders in the elderly and with the promotion of longevity An ‘official’ ABPN subspecialty in 1989 Managing elderly patients requires ‘special’ knowledge: possible differences in mental health presentations, frequent co-exiting and complicating chronic medical diseases, multiple medications (drug-drug interactions, pharmacodynamics and pharmacokinetics) and aging specific issues What’s in an age? What age makes you a geriatric patient? What makes you ‘elderly’? Age 65 and older: elderly, ‘old’ Age 85 and older: ‘very old’ or ‘old, old’ Age 100 and older: ‘oldest old’ “Baby Boomers” – those born between 1946 1964, 78 million US Americans alive today and will be turning 60 years of age in 2006 2024.……“Graying of America” Geriatric Statistics: U.S. Bureau of the Census: Life expectancy: 1950 = 68 years; 1991 = 79 years for women/72 years for men* In the year 2000 = 12.4% of the U.S. population - 35 million Americans - were 65 years or older* By 2030 = percentage increased to 20% -1 in 5 people will be older than 65; 2025 in Florida – 1 in 4 people People age 85 and older: are the fastest growing segment of our population – from 4 M today to 20 M by 2050;* constitute 10% of those 65 years and older; there are 39 men for every 100 women 85 years old or older *Administration on Aging. Statistics on the Aging Population, Rockville, MD; US Department of Health and Human Services; 2003; U.S. Bureau of the Census. Geriatric Statistics The old, old (age 85 and older) consume the largest amount of Medicare resources; 5% of the Medicare population consumes 50% of the Medicare dollars – many are the ‘frail elderly’ On average, by age 75, older adults have between two and three chronic medical conditions; some as many as ten to twelve medical conditions and as many medications Geriatric Statistics: Mental Health 20% of the US population over the age of 65 has a mental illness** As the population ages, the number of people with mental illness will double to 15 million by 2030 Number of people over age 65 years with mental illness will equal the number of people with mental illness in ALL other age groups* Older adults are less likely to seek mental health: only 4% of non-institutionalized US population seek mental health treatment*** Older adults are more likely to be identified, diagnosed and receive treatment from their primary care physician**** *Bartels SJ (in press). **Jeste, DV, Consensus statement on the upcoming crisis in geriatric mental health, Arch. Gen. Psychiatry 1999: 56(9): 848-53. ** * Olfson M, Outpatient mental health care in non-hospital settings. Am. J Psychiatry 1996; 153(10): 1353-6. * ** * Kaplan MS, et al, Managing depressed and suicidal geriatric patients. Gerontologist 1999; 39(4): 417-25. A Guide Through DSM-IV TR for the non-psychiatrist (for diagnosis, treatment and medication management) DSM-IV TR: Multiaxial System Axis I: Clinical D/O Axis II: Personality D/O Mental Retardation Axis III: General Medical Conditions Axis IV: Stressors (primary and/or secondary GMC, support group, education, housing, access to health care, occupational, financial, legal, social, recent loss and other psychosocial and environmental problems) Axis V: GAF (Global Assessment of Functioning scale 0-100) Multiaxial System - Example Axis I: Major Depressive Disorder, recurrent, moderate without psychotic features; R/O alcohol abuse Axis II: Cluster B traits Axis III: hypothyroidism, DMII, HBP Axis IV: poor social support – few friends and husband has left/whereabouts unknown, education – quit high school to get married and have a baby, homeless after hurricane Katrina, access to health care – lack of health coverage, occupational and financial - unemployed, legal recent DUI Axis V: GAF: 58 Axis I Disorders Axis I Disorders: Mood D/O (Depressive D/O and Bipolar D/O)* Adjustment D/O* Anxiety D/O* Somatoform/Factitious/Dissociative D/O Impulse Control D/O Paraphilias/Sexual and Gender Identity D/O Eating D/O Sleep D/O* Delirium, Dementia, Amnestic and other Cognitive D/O* Alcohol and Substance Related D/O* Schizophrenia and other Psychotic D/O (such as Delusional D/O) Axis II Disorders Axis II: Personality D/O Mental Retardation (onset before age 18, IQ at/below 70) General Diagnostic Criteria for a Personality Disorder Simply put: an extreme variant of normal personality traits ENDURING pattern of inner experience and behavior that deviates markedly from the expectations of the individual’s culture, is INFLEXIBLE and PERVASIVE across a broad range of personal and social situations, leads to clinically significant distress or impairment in social, occupational, or other important areas of functioning, is stable and of long duration (traced back to early adolescence or early adulthood) and not better accounted for by another mental, substance abuse d/o or medical condition (e.g. head trauma) General Diagnostic Criteria for a Personality Disorder Manifested in 2 or more areas: -cognition (ways of perceiving and interpreting self, others, and events) -affectivity (in range, intensity, lability and appropriateness of emotional response) -interpersonal functioning -impulse control Personality Disorders Cluster A: Paranoid PD, Schizoid PD, Schizotypal PD Cluster B: Antisocial PD, Borderline PD, Histrionic PD, Narcissistic PD Cluster C: Avoidant PD, Dependent PD, Obsessive-Compulsive PD PD NOS (mixed personality) General Population Statistics AS-PD = 2% B-PD = 2% (but 10% of all psych outpatients/75%-90% are women) H-PD = 2-3% N-PD=<1% BUT among chronic pain patients – a disproportionate percentage: AS-PD = 5% B-PD = 7-25% H-PD = 8-26% N-PD = 5-22% NIH Survey (2001-2002 National Epidemiologic Survey) estimated that 14.8% of American adults = 30.8 million Americans met criteria for at least one PD Late Life Stressors that place older adults at risk of mental health disorders Chronic physical health condition(s) Death of a loved one Caregiving Social isolation/lack or loss of social support Significant loss of independence History of mental health problems Late Life Stressors that place older adults at risk of mental health disorders Old age – even though older adults are more likely to experience life stressors – old age is NOT a risk factor for an increasing risk for a mental health disorder; in fact, ‘most’ older adults are able to cope with late life stressors without developing significant mental health disorders Successful aging: Vaillant; Success throughout the life cycle: Neugarten Most common mental disorders of old age are………… …..depressive disorders, cognitive disorders, anxiety disorders and alcohol use disorders Psychiatric disorders other than depression are found in lower prevalence among the elderly than at any other stages of the life cycle Suicide risk in the elderly *National Institute of Mental Health’s Epidemiologic Catchment Area (ECA) Study Suicide Risk Factors for Adults: Demographic Men at greater risk than women; Caucasians account for more than 90% of all suicides Age clusters: age 15-19, 20-24 and over age 60 Marital status: widowed, divorced and single individuals at greater risk than married individuals (more pronounced in men) Living alone; no children under age 18 living in household Alcohol/Substance Abuse history History of mental illness; previous suicide attempt Firearm(s) in the home 30% have seen a physician within 30 days; 60% have seen a physician within 6 months Suicide Assessment: SAD PERSONS…….a mnemonic Sex (male) - (age 65 – 15.5:100,000; white male older than 85 - suicide rate of more than 50:100,000 compared to the US population in 2002) Age (older) – (beginning at age 60) Depression Previous suicide attempts ETOH/SA Rational thinking loss (psychosis) Social supports lacking Organized plan to commit suicide No spouse (divorced > widowed > single) Sickness (physical illness) Risk of Suicide in People with Selected Psychiatric Disorders Condition………. Estimated Lifetime Suicide Risk Major Depression………………….14.6 Bipolar Mood Disorder…………….15.5 Dysthymia…………………………... 8.6 Schizophrenia………………………. 6.0 Panic Disorder……………………….7.2 Source: Pies(2004). Data from APA (2003); and Harris and Barraclough (1997) Suicide Risk Suicide risk can not be predicted from any one factor Predicting suicide is VERY difficult BUT failure to assess for suicidality is the key to liability; asking about suicide does NOT increase the risk Depressive Disorders MDE: single, recurrent; with atypical features; with catatonia; with postpartum onset; with psychotic features; with seasonal pattern (SAD) Dysthymic Disorder Depressive Disorder NOS ................................................................ Adjustment Disorder Bereavement/Abnormal Bereavement Depression Prevalence rate: 4.4% - by DSM IV criteria Up to 20% of community-dwelling older adults endorse significant depressive symptoms that do not meet full criteria for a mood disorder – subsyndromal depression is the modal form in older adults* Late-onset depressive disorder is associated with being widowed, having a chronic medical illness and with a high rate of recurrence Up to 80% of patients in LTC (NH/ALF) may experience a mood disorder Adjustment Disorders; (Abnormal) Bereavement *APA Working Group on the Older Adult (Brochure) 1998; WDC. Depression in the Elderly: Signs and Symptoms Reduced energy and concentration Decreased appetite, weight loss Sleep complaints – early morning awakenings and frequent awakenings SOMATIC COMPLAINTS ‘pseudodementia’ Episode with ‘melancholic features’, hypochondriasis, hopelessness, feelings of worthlessness, paranoia and suicidal ideation Anxiety Disorders Usually begins in early or early or middle adulthood but may appear after age 60 Prevalence rate: 5.5% -11.4* but with the elderly - up to 20% with 37% comorbidity with depression, dementia and medical illnesses such as CHF, CAD, diabetes *U.S. Department of Health and Human Services. Mental Health: Report of Surgeon General; 1999 Anxiety Disorders: Prevalence (among older community-dwelling individuals) GAD = 7.3% Phobias = 3.1% Panic D/O = 1.0% Obsessive-compulsive disorders = 0.6% Interrelationships Among Depression and Anxiety Disorders Generalized anxiety disorder Obsessive compulsive disorder Social anxiety disorder Depression Specific (simple) phobia Panic disorder Posttraumatic stress disorder There is considerable overlap among symptoms of depression and anxiety disorders DSM-IV-TR. Washington, DC: American Psychiatric Association; 2000. Major Symptoms of Depression and GAD Overlap Generalized anxiety disorder Major depressive disorder Worry Anxiety Muscle tension Palpitations Sweating Dry mouth Sleep disturbance Depressed mood Psychomotor agitation Concentration difficulty Irritability Fatigue Anhedonia Appetite disturbance Worthlessness Suicidal ideation Nausea DSM-IV-TR. Washington, DC: American Psychiatric Association; 2000. Continuum of Anxiety and Depression Anxiety disorders Comorbid depression and anxiety Stahl SM. J Clin Psychiatry. 1993;54(1 suppl):33-38. Major depressive disorder Co-morbidity: Depression and Anxiety -- 1/3 –> 1/2 of people with depression will meet criteria for an anxiety disorder --More then 1/2 of people with an anxiety disorder will eventually experience a depressive disorder --Even among patients diagnosed with a depressive disorder who do NOT meet criteria for a formal anxiety disorder, the majority experience anxiety symptoms The Affective Spectrum Dysthymia….. Single MDE…. Chronic MDE…. Atypical MDD…. Recurrent MDD…. BIPOLAR SPECTRUM……… The Affective Spectrum: Bipolar Mood Disorders Bipolar l Bipolar ll Mania and Major Depression Hypomania and Major Depression Cyclothymia (non-major depression as well as hypomania) Hyperthymic temperament (‘ascending order’ up the bipolar spectrum) Secondary Mania (due to other illnesses or medications) Bipolar lll The Affective Spectrum: Bipolar Mood Disorders...range of rates Bipolar l 0.0 - 1.7% Bipolar ll 0.2 – 3.0% Bipolar Spectrum Disorders 2.6 – 6.5% overall = 3.4% Equal males/ females Sex (sex difference only significant in BMD II and Cyclothymic D/O) Bipolar Mood Disorders 1.7% population = 3.3 million (US) 6th leading cause of disability worldwide – esp. from undertreated or resistant depression Suicide: 25% attempt, 11-19% complete Complex non-Mendelian inheritance – several genes involved >90% will have future episodes 10-15% will have >10 episodes Bipolar Mood Disorders Onset (average in years): --1st impairment = 15-19 --1st treatment = 22 --1st hospitalization = 25 Younger Age of Onset: AD medications, stimulants, SA, ‘genetic’ anticipation Late Life Onset: 30-60 years Secondary Mania of Late Life Bipolar Mood Disorders 69% of patients are misdiagnosed at least once 35% were symptomatic for more than 10 years before correct diagnosis Increased mortality (unnatural and natural causes of death) Co-morbid anxiety rates in patients with Bipolar Mood Disorder are between 30% 40%* *McElroy et al., Am J Psychiatry 158: 420-426, 2001 Symptom Domains of Bipolar Disorder Dysphoric or Negative Mood Manic Mood and Behavior and Behavior • Euphoria • Grandiosity • Depression • Pressured speech • Anxiety • Irritability • Impulsivity • Hostility • Excessive libido • Violence BIPOLAR • Recklessness • Suicide • Social intrusiveness DISORDER • Diminished need for sleep Psychotic Symptoms • • Delusions Hallucinations Slide courtesy of Keck PE Jr.; adapted from Goodwin FK, Jamison KR. Manic-Depressive Illness. Oxford University Press: New York, NY; 1990. Cognitive Symptoms • • • • Racing thoughts Distractibility Disorganization Inattentiveness Screening Tools: The Mood Disorder Questionnaire Important symptoms: Hyper or more energetic than usual Predominately or thematically irritable Distinctly self-confident, positive or self-assured Less sleep than usual More talkative or speaking faster than usual Racing thoughts Easily distracted Problems at work and socially More interest in sex Taking unusual risks Excessive spending Screening Tools: The Mood Disorder Questionnaire (cont.) The Mood Disorder Questionnaire (MDQ) Derived from DSM-IV criteria and clinical experience Initial validation study of MDQ in psychiatric outpatients (N = 198) Sensitivity = 73% and Specificity = 90% for Bipolar I and II Validation study of MDQ in general population (N = 711) Sensitivity = 28% and Specificity = 97% for Bipolar I and II MDQ as screening tool (13 questions) Positive MDQ 7 “yes” responses; Negative MDQ 7 “yes” responses Rapid screening tool – 10 minutes or less Patients can self-administer MDQ while in the waiting area Does not require trained evaluators Easily used in primary care settings Hirschfeld RMA, et al. J Clin Psychiatry. 2003;64:53-59. Bipolar Disorders: in Older Adults * True prevalence is unknown (elderly underutilize mental health services, underreport mental health problems, receive care in other settings) Co-morbidity is the rule rather than the exception (neurological illness, diabetes….7 or more co-morbid diagnoses in 20% of elderly BMD)* Lifetime rate of substance abuse: 20-30% Difference between ‘early onset’ bipolar d/o vs. ‘late onset’ bipolar d/o Mania associated with medical conditions Depp & Jeste 2004; Regenold, et al. Bipolar Disorders: in Older Adults Primary vs. Secondary Mania Primary: -onset early in life -no obvious medical cause Secondary: -onset later in life -related medical cause (CNS lesions, metabolic disease) -higher familial rate of bipolar illness -better general response to lithium -lower familial rate of bipolar illness -generally poor response to lithium Bipolar Disorders: in Older Adults Depression usually precedes mania by 20 years In general, manic symptoms are milder compared to younger patients May present with mixed, manic, dysphoric or agitated states More likely to have irritability, treatment resistance, higher mortality rate Develop dementia at a higher rate than elderly without bipolar illness BMD – late onset Persons age 60 years and older may constitute as much as 25% of the population with BMD* New-onset BMD frequency declines with advanced age with as few as 6%-8% of all new cases of BMD developing in persons age 60 years and older* Co-morbid Axis I disorders include: alcohol abuse disorders = 38.1%, dysthymia = 15.5%, GAD = 20.5%, panic disorder = 19.0% (men – greater prevalence of alcoholism; women greater prevalence of panic disorder)** * * ** Sajatovic M, et al: New-onset bipolar disorder in later life. Am J Geriatr Psychiatry 2005; 13: 282-289. Almeida, OP, Fenner, S: Bipolar disorder. Int Psychogeriatr 2002; 14:311-322. Goldstein, BI, et al: Am J Psychiatry 2006; 163:319-321. Sleep Disturbances in the Elderly Prevalence of Insomnia by age group*: Age Age Age Age 18-34 35-49 50-64 65-79 – – – – 14% 15% 20% 25% *Mellinger GD et al. Arch Gen Psychiatry 1985;42:225-232. Medications Primary Sleep Disorders Medical Conditions Complaint of Insomnia Psychiatric Conditions Psychosocial Factors Poor Sleep Hygiene Examples of ‘Legal’ Drugs That Cause Insomnia Alcohol Decongestants CNS stimulants Stimulating antidepressants Beta-blockers Diuretics Thyroid hormones Bronchodilators Nicotine Calcium channel blockers Caffeine Corticosteriods CNS Depressants Quinidine Anticonvulsants Antiparkinsonian agents Overlap in Sleep Disorders Associated with Poor Sleep &/or Excessive Daytime Sleepiness Narcolepsy Circadian Rhythm Sleep Disorder/ Shift Work Sleep Disorder Central Sleep Apnea Obstructive Sleep Apnea Excessive Sleepiness Inadequate Sleep and/or Poor Sleep Hygiene Medication Side Effects PLM D/O RLS Primary RLS Overall prevalence: 3-15% Mean age of onset: 34 +/- 20 years Highly variable course Primary (idiopathic) RLS make up majority of cases; majority are hereditary Not all patients with PLMD have RLS BUT most patients with RLS have PLMD Secondary RLS Iron deficiency (5% of patients with RLS have iron Renal failure Pregnancy Parkinson’s Disease Neuropathy Medications may aggravate: antihistamines, TCAs, SSRIs, DA receptor blockers deficiency; 25-30% of patients with iron deficiency anemia have RLS) Medical Condition CV disease Pulmonary Disease e.g. COPD GERD Renal failure Parkinsonism Chronic Pain Nocturia Psychiatric Condition Depression Anxiety Dementia – with DAT: circadian rhythm disruption with pronounced fragmentation of sleep-wake pattern Substance Abuse Vulnerability to Sleep D/O Older age (besides that which relates to medical problems and medications): as relates to sleep efficiency and brain’s sleep-generating processes and age related advanced sleep phase Personality and ability to handle external stressors Biological clock sensitivity to changes in time, to go to bed and/or wake up Even modest amounts of alcohol can interfere with sleep quality causing sleep fragmentation and early morning awakenings; aggravates OSA Evaluating Causes of Insomnia Situational factors that are major stressors such as a life trauma or an upcoming important event Environmental factors such as too much noise, temperature that are too hot or too cold, or working a night shift Factors related to medications, both prescription and nonprescription (i.e. CNS stimulants/activating antidepressants) Medical problems such as pain d/o, endocrine d/o, menopause, BPH, incontinence, CHF, PUD/GERD, COPD, allergic rhinitis, seizure d/o Consequences of Poor Sleep in older adults Ancoli-Israel s, Cook JR. J Am Geriatr Soc 2005;53 (suppl):S264-S271 Difficulty sustaining attention and slowed response time Decreased ability to accomplish daily tasks Impairments in memory and concentration Increased consumption of healthcare resources higher incidence of symptoms related to depression and anxiety Increased risk of falls (even after controlling for medication use, age, difficulty walking, difficulty seeing and depression) Shorter survival/increased institutionalization rate Inability to enjoy social relationships/decreased QOL Increased incidence of cognitive decline Increased incidence of pain Improving Sleep Complaints Treat underlying depression (up to 80% experience insomnia) Treat underlying anxiety disorder Treat underlying schizophrenia Treat underlying Sleep D/O (i.e. obstructive sleep apnea with CPAP/weight loss) Treat underlying Medical D/O and Neurological D/O ‘Manage’ medication(s) Limit alcohol Behavioral interventions tend to be more effective over time = GOOD SLEEP HYGIENE Prevalence: Alcohol Abuse/Dependence More than half of people over age 65 do not drink at all ‘At risk drinking’ (more than 2 drinks/day for a man and more than 1 drink/day for a woman): 6-9% (minimum) Up to 17% of older adults (over age 60) misuse alcohol or prescription drugs (5% - 10% of patients seen in an outpatient setting and 7% - 22% of medical inpatients)* (approximately) 2/3 of alcohol problems are “long standing” while 1/3 are a late-onset problem appearing for the 1st time later in life POSSIBLY associated with retirement, bereavement or depression *J. Geriatr. Psychiatry Neuro. 2000:13;106-14. Prevalence: Alcohol Abuse/Dependence “heavy alcohol use” = 3 – 25% “alcohol abuse” = 15% men/12% women ……..drinking in excess of recommended limits/guidelines – with women, rapid progression to alcohol-related illnesses such as cirrhosis, sleep problems and cognitive problems Prevalence: Alcohol Abuse/Dependence Alcohol dependence: prevalence is 8 – 14%; most common psychiatric disorder Often accompanied by other substance abuse d/o (particularly nicotine), anxiety/panic, mood disorders and antisocial personality disorder Guidelines National Institute on Alcohol Abuse: no more than 1 drink per day and/or no more than 2 drinks on any occasion or 7 standard drinks/week; never more than 4 standard drinks on any drinking day AAFP: no more than 2 drinks per day for men/1 drink per day for women If you give a 30 year old vs. 80 year old, each 2 drinks, the 80 year old will have a BAL of 3 drinks = age related changes in lean body mass/total body water/increased body fat/increased sensitivity and decreased tolerance to alcohol coupled with drug-drug interaction/metabolic changes (pharmacokineticspharmacodynamics) Statistics: National Institute on Alcohol Abuse and Alcoholism (NIAAA) Alcoholism is a lifelong disease with a relapsing, remitting course, has a genetic component along with environmental and interpersonal factors…………. Other ‘Illegal’ Substances of Abuse Marijuana Cocaine Amphetamines Hallucinogens/NMDA Phencyclidine …………………………. Few statistics available for the elderly; many addicts die before they reach an older age because of overdoses, deterioration in health/health consequences/premature death and death due to violence OTC and Prescription Use/Misuse Laxatives Antihistamines OTC stimulants and herbals Antibiotics BZDs/meprobomate - for sedation or anxiety Analgesics/opioids 63-79% of ER MDs fail to recognize elderly alcoholic it is estimated that as many as 20% of elderly inpatients are ‘alcoholic’ and up to 30% are problem users of sedative/hypnotics, antianxiety agents and/or analgesics; interactions of alcohol and (legal/prescribed) drugs Clinical Presentation in the Elderly with an Alcohol/SA Problem Do NOT present as: substance seeking behavior such as characterized by crime, manipulativeness, and antisocial behavior Presentations vary but may include: marital discord, falls, confusion, poor personal hygiene, depression, anxiety, sleep complaints, malnutrition, delirium, dementia Pain*: International Association for the Study of Pain (IASP) 50 million Americans suffer from chronic pain Chronic pain disables more people and adds more to health care costs than does heart disease and cancer combined 25-50% of community-dwelling older adults suffer pain problems; 45-80% of NH patients suffer pain problems 50% of adults older than 60 suffer from some form of LBP Incidence of OA - increases with age: affects 21M of USA population; 80% of patients older than 65 (knee/hip/hand) *MMWR 53 [18]: 388-89, 2004. Classifying Pain Acute Duration vs Chronic Nociceptive Pathophysiology vs Neuropathic Acute vs Chronic Pain States Acute vs Chronic • Associated with tissue • Extends beyond expected damage • Increased autonomic nervous activity • Resolves with healing of injury • Serves protective function period of healing • No protective function • Degrades health and functioning • Contributes to depressed mood Turk, Okifuji. Okifuji. In: Bonica’ Bonica’s Management of Pain. 2001; Chapman, Stillman. In: Pain and Touch. Handbook of Perception and Cognition. Cognition. 2nd ed. 1996; Fields. Neuropsychiatr Neuropsychol Behav Neurol. 1991;4:831991;4:83-92. Examples of Nociceptive and Neuropathic Pain Nociceptive Mixed Neuropathic Caused by tissue damage Caused by combination of primary injury and secondary effects Caused by lesion or dysfunction in the nervous system • Arthritis • Mechanical low back pain • Sports/exercise injuries • Postoperative pain • • • • Low back pain Fibromyalgia Neck pain Cancer pain • • • • • • • Painful DPN PHN Neuropathic low back pain Trigeminal neuralgia Central poststroke pain Complex regional pain syndrome Distal HIV polyneuropathy Effects of Chronic Pain on the Patient Physical Functioning/Quality of Life: -ability to perform ADLs -sleep disturbances Social Consequences: -Relationship with family & friends -intimacy/sexual activity -social isolation Psychosocial Morbidity: -depression -anxiety -anger -loss of self esteem Societal Consequences -healthcare costs -disability -lost workdays In the elderly, with use of BZDs, Sleep Medications, Muscle Relaxants, and Opioids… -- watch for cognitive, behavioral, and psychomotor effects such as memory impairment, residual daytime sedation, rebound insomnia and unsteady gait falls Dementia 2nd most common cause of disability among people age 65 and older (second only to arthritis) DAT Dementia: Statistics (Dementia of Alzheimer’s Type) Incidence: 5-8% ……….over age 65 15-20%……..over age 75 25-50+%……..over age 85 Women > Men (1.2-1.5 to 1.0) If trends continue, population with DAT will quadruple within the next 50 years…….. New Cases/Year=360,000=40 new cases/hour Projected Prevalence of Alzheimer’s Disease (AD) 16 4 Million AD Cases Today— Over 14 Million Projected Within a Generation 14.3 14 11.3 12 10 8.7 8 6 4 5.8 6.8 4 2 0 2000 2010 2020 2030 Year Evans DA. Milbank Q 1990;68:267-289. Wacanta J. European Psychiatry 2003; 18: (2003) 306–313 2040 2050 Dementia: DAT Alzheimer’s Dementia accounts for 50-75% of all dementias 5 million Americans have DAT (2000); by 2050 – 14 million 1/3 of risk for DAT is genetics; 2/3 involves non-genetic factors – particularly lifestyle choices we make like physical activity, good diet, optimizing mental health, continued cognitive challenges/learning, high BMI, fat intake, HBP, high cholesterol, vascular changes and neural changes Course lasts from 2 – 22 years Average life span following diagnosis is 7 – 10 years; life expectancy is significantly shortened (Other) Dementias………… -Vascular Dementias are estimated to account for 15% of all dementias -Dementia with Lewy Bodies* estimated to account for 7-26% -Parkinson’s Disease: dementia occurs in 2060% of PD patients (20% DAT) -Parkinson Plus Syndromes (Other) Dementias………… -Pick’s Disease/FTD/PPA -Huntington’s Disease -Creutzfeldt-Jakob disease -Associated with long term use of alcohol Overlapping classifications Alzheimer’s Disease Dementia of the Alzheimer’s Type Marlatt M.W. et al. Curr Med Chem. 2005;12:1137-47 Relative prevalence of different forms of dementia 50-60% Neuropsychiatric Clusters in Dementia Apathy: withdrawn, lack of interest, amotivation Depression: sad, tearful, hopeless, low self-esteem, anxiety, guilt Aggression: aggressive resistance, physical aggression, verbal aggression Agitation: walking aimlessly, pacing, trailing, restlessness, repetitive actions, dressing/undressing, sleep disturbance Psychosis: hallucinations, delusions, misidentifications LTC Setting – Patient Demographics --2/3 LTC patients carry a diagnosis of Dementia (80% due to DAT) --ONLY 25% of adults diagnosed with dementia are in LTC!!!!!!! --Caregiver: Burden/Stress/Depression/ Premature Death Caregivers 30-50% of caregivers of patients with dementia met the criteria for major depression and a larger proportion of caregivers suffer from psychiatric symptoms but are below the thresholds for psychiatric diagnoses* *Cohen and Eisdorfer 1989; Tennstedt et al 1992 Mild Cognitive Impairment (MCI) MCI (mild cognitive impairment): Cognitive impairment in elderly persons not of sufficient severity to qualify for a diagnosis of dementia……patients have complaints of impairment in memory or other areas of cognitive functioning usually noticeable to them or to those around them; performance on ‘memory or cognitive’ tests are usually below that expected for their age and education A ‘precursor’ to DAT in 50% of patients over 34 years MCI Prevalence Rate in the Community Normal aging MCI early DAT Prevalence rate for >60 years of age: 3% Prevalence rate for >75 years of age: 15% Annual conversion rate to DAT: 625%/year Elder Abuse, Neglect and Exploitation Elder Abuse, Neglect and Exploitation Types of elder abuse: physical abuse, sexual abuse, emotional/psychologic abuse, financial exploitation/victimization/undue influence, neglect, abandonment and self-neglect Most common type of elder abuse: neglect depriving an elder of something needed for daily living Second most common type of elder abuse: physical abuse Third most common type of elder abuse: financial exploitation Elder Abuse Statistics Prevalence: 1% - 12% Women more than men 75% of victims are physically frail; 50% are unable to care for themselves; many are confused or disoriented – some or most of the time Majority occurs in home setting Majority of perpetrators are family members usually a spouse or adult child STATISTICS: Elderly Physical or psychological abuse or neglect, financial exploitation/undue influence and violation of rights Can occur in family homes, nursing homes, board and care facilities, and hospitals Mistreated by their spouses, partners, children and other relatives and friends Elder partner abuse: long standing pattern of marital violence or as abuse originating in old age – as relates to issues in aging/disability, stress and changing family relationships Risk Factors for Abuse Older age (>75) Female Unmarried/widowed/divorced Lack of access to resources Low income Social isolation Minority status Low level of education Functional debility/taking multiple medications Substance abuse by caregiver or elder person Psychologic disorders (depression, anxiety) and character pathology Previous history of family violence Caregiver burnout and frustration Cognitive impairment Fear of change of living situation (home ALF/NH) The End QUESTIONS?