")
Cervical Cancer:
Epidemiology and Prevention Research
Advances
Mahboobeh Safaeian, Ph.D.
safaeianm@mail.nih.gov
National Cancer Institute
HPV & Cervical Cancer Research
Discovery of
HPV
Natural history of
HPV and
pathogenesis of
cervical cancer
defined
Method for
assembly of
HPV VLP
defined
1983
Late 80’s-90’s
Cervarix first
licensed in the
EU for
adolescent
girls/young
women
Phase III
clinical trials
in humans
1992
HPV vaccine
trials in
animals and
early phase
trial in humans
1990’s-early 2000’s
FDA licenses
Gardasil for
girls/young
women
2000’s
2004
2006
2007
FDA extends
Gardasil
licensure to
males & for
prevention of
anal
infections/
lesions
2009+
Summary of Today’s Talk
• Epidemiology of cervical cancer
• Prevention
• Immunogenicity of HPV
Cervical Cancer
epidemiology
• Worldwide ~500,000 new cases per year
• Worldwide ~250,000 deaths per year
• 2nd/3rd most common cancer in women
• Incidence and survival rates vary by
geographical region
Age-standardized incidence and mortality rates of
cervical cancer, 2002
Mortality rate
per 100,000
women
4.0
11.2
Incidence rate
per 100,000
women
10.3
19.1
0
5
10
15
20
Developed Countries
Less Developed Countries
GLOBOCAN 2002
25
The Primary Risk Factor for Cervical Cancer:
Human Papillomavirus (HPV)
HPV
• Small DNA virus (~8000bp)
• More than 100 types
identified based on the
genetic sequence of the outer
capsid protein L1
• 40 types infect the mucosal
epithelium
• ~15 carcinogenic HPV types
HPV - epidemiology
• Most common viral sexually transmitted infection
• High infectiousness
• Peak prevalence 15-25 years
• The HPVs can infect men and women at multiple sites, including:
– MEN: oral cavity, penis, scrotum, urethra, anus
– WOMEN: oral cavity, cervix, vagina, vulva, anus
• Infections generally transient (1-2 years)
• Manifestation of infection depends on the site of infection
and the genotype of HPV.
– Carcinogenic neoplasia and cancer of cervix, oropharynx, and anus; less
likely to cause cancer at other sites, ex: HPV16 and 18
– Non-carcinogenic anogenital warts, ex: HPV6 and 11
Working model of cervical carcinogenesis
normal
cervix
HPV infection
persistence
high grade
neoplasia
invasion
Working model of cervical carcinogenesis
normal
cervix
HPV infection
Younger age
Increasing # sex partners
“Male factor”*
persistence
high grade
neoplasia
invasion
Working model of cervical carcinogenesis
normal
cervix
HPV infection
Younger age
Increasing # sex partners
“Male factor”*
persistence
HPV type (HPV-16)
Host immune response
Exogenous factors eg.
Smoking?
high grade
neoplasia
invasion
Working model of cervical carcinogenesis
normal
cervix
HPV infection
Younger age
Increasing # sex partners
“Male factor”*
persistence
HPV type (HPV-16)
Host immune response
Exogenous factors eg.
Smoking?
high grade
neoplasia
Increasing age
HPV type (HPV-16)
Smoking
Multiparity? OC use?
Host immune responses
invasion
Secondary Prevention: Interrupting
disease progression
Working model of cervical carcinogenesis
normal
cervix
HPV infection
persistence
high grade
neoplasia
invasion
Screening for HPV infection and precursor lesions
Frequent pap smear cytology
HPV DNA testing (age 30+)
Treatment of precursor lesions by excisional therapy is
> 95% effective
The Papanicolaou (Pap) test has significantly
reduced the incidence of cervical cancer in
populations where screening has been well
implemented.
Country
Coverage
Mortality
reduction
Iceland
National
80%
Finland
Wide
50%
Switzerland
Wide
34%
Denmark
40%
25%
Norway
5%
10%
Anderson et al.
Organization and results of the cervical cytology screening
program in British Columbia, 1955-85. Br Med J 1988;
296(6627): 975-8
Coverage: 85%
Incidence of cervical cancer: fell 78%
Mortality from cervical cancer: 72%
If Pap Smears successfully prevented cervical cancer, why not simply
use them to screen everyone else?
A. Three-visit cycle: 1. Cytology; 2. Colposcopy; 3. Treatment
B. Cytology is an insensitive test (negative test = poor reassurance);
repeat iterations (e.g., regular or annual Pap smears) are necessary.
C. Cytology is a poorly reproducible (subjective) test and difficult to
maintain performance
D. Colposcopy is not as good as you think it is.
E. Bottom Line: U.S. program costs billions of $ annually
F. Tests with better test characteristics, less visits per cycle, fewer
cycles per lifetime
HPV Testing for Screening
ALTS Trial
HPV vs Repeat Cytology for Triage of ASCUS (N=2,324)
Sensitivity % Referral
(CIN2+)
HC2
95.9%
56.1%
ThinPrep (ASCUS+) 85.0%
58.6%
Solomon et al, JNCI, 2001
Comparative efficacy of visual inspection with acetic acid, HPV testing and conventional cytology in
cervical cancer screening: a randomized intervention trial in Osmanabed District, Maharashtra State, India
Cervical cancer incidence rates among screen
negative women by study group (2000-2007)
New cancer
cases
# of Women
Incidence Rate
(per 100,000)
HPV
8
24,380
3.7
Cytology
22
23,762
15.5
VIA
25
23,032
16.0
Osmanabed District, Maharashtra State, India,
Sankaranarayanan et al., NEJM, 2009
Current US Recommendations: Women 30 Years and Older
Cytology
Negative
Oncogenic HPV Testing
Oncogenic
HPV -
Repeat test in 3 years
Oncogenic
HPV+
Repeat test in 6-12 months
Concerns about Screening Using HPV Tests
• Will screening be used incorrectly, e.g., among
young women?
• Will the tests include the right types and proper
thresholds for positivity?
Primary Prevention:
Prophylactic vaccination
Current Prophylactic Vaccines are Based on
L1 Papillomavirus-Like Particles
• Empty shells composed of
the L1 major virion protein
25
HPV VLP Vaccines
Manufacturer
Trade name
HPV types
Theoretic coverage
Merck
GlaxoSmithKline
Gardasil®
Cervarix™
L1 HPV6 20 ug
L1 HPV11 40 ug
L1 HPV16 40 ug
L1 HPV18 20 ug
70% of CxCa
90% GW
L1 HPV16 20 ug
L1 HPV18 20 ug
70% of CxCa
Expression system
Aluminum salt
(Alum): 225 ug
Yeast
ASO4: (Alum: 500 ug +
MPL: 50 ug)
Hi-5 Baculovirus
Dosing Schedule
0, 2, 6 months
0, 1, 6 months
Adjuvant
Who Can Receive the Vaccine and For What Purpose?
Licensure (FDA)
Gardasil licensure
Females ages 9-26 for the prevention of cervical, vulvar, vaginal, and anal
disease
Males ages 9-26 for the prevention of genital warts and anal disease
Cervarix licensure
Recommendations for Use
(ACIP-CDC)
Females ages 10-25 for the prevention of cervical disease
Advisory Committee on Immunization Practices-CDC
recommendations
Females: Recommended for ages 11-12; as early as 9 yrs & catch up
vaccination through age 26
Males: Gardasil recommended for boys 11-12; catch-up to 21 yrs
HPV Vaccine Efficacy*
Endpoint
HPV 16/18-related
CIN2/3 or AIS
Efficacy
100%
HPV 6/11/16/18
related CIN
95%
HPV 6/11/16/18
related genital warts
99%
*Among 16-26 year old females. CIN – cervical intraepithelial neoplasia; AIS – adenocarcinoma in situ
HPV Vaccine Doesn’t Treat
Established Infections
Control Arm (298/220)
HPV Arm (248/177)
49.8 48.8
% Clearance
50
40
31.3
33.4
30
VE = -2.0%
20
10
VE = 2.5%
0
6-Mo
12-Mo
Time
29
Hildesheim et al., JAMA 2007
HPV Vaccine
Adverse Reactions
• Local reactions
84%
(pain, swelling)
• Fever
10%*
• No serious adverse reactions
reported
*similar to reports in placebo recipients (9%)
Does the vaccine protect against other
HPV types?
(cross-protection)
Summary of the vaccine efficacy reported for selected
HPV types not in the vaccine formulation:
FUTURE1
Gardasil
6-month
persistence
PATRICIA2
Cervarix
12-month
persistence
CVT3
Cervarix
12-month
persistence
Related type
HPV31
HPV52
HPV58
HPV33
33.6%*
2.3%
12.8%
22.5%
80.5%*
-7.8%
-17.7%
41.0%*
45.7%*
-20.0%
-6.3%
37.3%
HPV45
20.1%
60.0%*
52.0%
Outcome Evaluated
Vaccine HPV type
HPV16
HPV18
*Statistically significant VE
32
1: NEJM 2007
2: Lancet 2009
3: Cancer Discovery 2011
Does the vaccine protect against HPV
infections at other anatomic sites?
HPV causes cancer at several anatomic
sites
Figure compliments of Dr. Doug Lowy
Protection against other cancers
• Vaginal/vulvar- 100% VE
• Anal cancer- from CVT ~85% in naïve
population
• Penile- high protection against penile
precancer
• Oral- no data yet
Summary of Vaccine Findings in Young
Women
• High level prevention of precancerous cervical
lesions when administered to females without
infection by vaccine-type HPVs
– Not therapeutic
• Generally safe and well-tolerated
– None of the deaths considered vaccine related
– Cannot cause infection or cancer (b/c only contains 1
protein from each targeted type)
• Additional results
– High efficacy for prevention of HPV-related extra-genital
lesions
Summary of questions that still need
addressed
• How long is the duration of protection (past
10 yrs)?
• Will the vaccine work in special populations
(i.e.: HIV-positive)?
• How should the vaccine be integrated into
existing screening programs?
• How should the vaccine be introduced in
countries without screening programs?
Cervical VE among women who received
<3 doses of the HPV vaccine
Background
• 3-dose HPV vaccine regimen provides robust
protection against cervical HPV infection and
disease
– costly and difficult to complete, especially in lowresource settings
• ~20% of women received <3 doses
– due to pregnancy and colposcopy referral
• Objective: compare efficacy of <3 doses to the
standard regimen
Dose- stratified VE after 4-yrs follow-up
# of
Doses
Arm
Control
# with
% with
#
persistent* persistent
Women HPV16/18 HPV16/18
infection
infection
3010
133
HPV16/18 VE (95%CI)
4.4%
3
80.9% (71.1% to 87.7%)
HPV
Kreimer AR et al JNCI
2957
25
0.9%
*12 month+ persistence
Dose- stratified VE after 4-yrs follow-up
# of
Doses
Arm
#
Women
# with
persistent
HPV16/18
infection
Control
3010
133
% with
persistent
HPV16/18
infection
4.4%
3
HPV16/18 VE (95%CI)
80.9% (71.1% to 87.7%)
HPV
2957
25
0.9%
Control
380
17
4.5%
2
84.1% (50.2% to 96.3%)
HPV
422
3
Kreimer AR et al Provisionally accepted JNCI
0.7%
Dose- stratified VE after 4-yrs follow-up
# of
Doses
Arm
#
Women
# with
persistent
HPV16/18
infection
Control
3010
133
% with
persistent
HPV16/18
infection
4.4%
3
HPV16/18 VE (95%CI)
80.9% (71.1% to 87.7%)
HPV
2957
25
0.9%
Control
380
17
4.5%
2
84.1% (50.2% to 96.3%)
HPV
422
3
0.7%
Control
188
10
5.3%
1
100% (66.5% to 100%)
HPV
196
0
0.0%
p trend= 0.2
Kreimer AR et al Provisionally accepted JNCI
Lack of evidence for bias in immune levels by # of
doses received
HPV16 antibody titers one-month post-vaccination
Doses
received
N
Median
Range
1
30
355
59 - 43388
2
140
425
4 – 56575
3
120
456
51 - 72760
Kruskal-Wallis
0.45
Summary
• Sufficient evidence to modify existing 3-dose
schedules?
– Not randomized
– Small number of events
– Durability of protection for <3 doses
• Proof of principle: <3 doses may provide a high
degree of protection against cervical HPV-16/18
– Public health: could prevent similar amounts of
disease with fewer doses of vaccine
Immunogenicity of bivalent HPV vaccine
among partially vaccinated young
adolescent girls in Uganda
Rationale
• HPV vaccine produces high levels of antibodies
– Shown to be protective of HPV16/18 infections and
associated lesions
– Neutralizing antibodies thought to be responsible
for the protection
• From CVT, vaccine efficacy among adult women
who received either one or two doses of HPV
vaccine was similar to women who received all
three vaccines doses.
• None of the HPV vaccine efficacy randomized
clinical trials were conducted in Africa, where
majority of cervical cancer cases occur.
Rationale
• Difficult to know whether partial vaccination will
provide the same benefit of protection from HPV
infection as full vaccination
– Use immunogenicity data to address
• Prior infection with HPV provides protection
– Modest levels of antibodies produced following
natural infection are sufficient for protection from
subsequent infection with the same HPV type.
Hypothesis
• Given what we know from the vaccine and
natural history studies, we hypothesize that the
anti-HPV antibodies of girls who received 1 or 2
does of the vaccine even though decreased will
be non-inferior compared to those who received
3 doses
– Significantly higher than levels reported after natural
infection required for protection
Primary Objectives
•
To investigate whether the HPV16/18 immune
responses elicited by the bivalent vaccine for
girls who received one dose and those who
received two doses are similar to girls who
received all three doses of the bivalent HPV
vaccine.
Collaborators
• PATH
– D. Scott LaMontagne, PhD
• Uganda
– Emmanuel Mugisha, MPH, PhD
– Edward Kumakech, BSN, MSc, MPH
• NCI
– Mahboobeh Safaeian, PhD
– Ligia Pinto, PhD
Immunogenicity of HPV VLP Prophylactic
Vaccines: Where We Are and Where We
Are Going
52
Studies at the HPV Immunology Lab at NCI
HPV VLP Vaccine
Cellular Immune Responses
Humoral Immune
Responses
Neutralizing Abs
Affinity
Systemic
Local
B cell memory
T cell proliferative
responses
Th1; Th2;
inflammatory
cytokines
Cross-reactivity
?
Correlates/Mechanisms ?
Long-Term Protection
Cross Protection
Host Gene
Expression
Profiles
Assays used to measure HPV
Immunogenicity
Polyclonal (P) vs.
Monoclonal (M)
P
Neutralizing
No
Remark
GSK
Competitive
Luminex
immunoassay
(cLIA)
M
Yes
Merck
Secreted alkaline
phosphatase
neutralization
assay (SEAP-NA)
P
Yes
Name
ELISA
Throughput,
volume
requirement
High throughput,
low sample
volume
High throughput,
multiplexing, high
sample volume
Gold standard; Low throughput,
Laborious
high sample
volume
HPV16/18 Immunogenicity
55
Vaccine Immunogenicity - CVT
HPV16 & HPV18 ELISA GMT: by vaccination arm
Antibody Levels (GMT) EU/mL
10000
1000
HPV Vaccinated
100
Naturally Infected
Not infected
10
1
0
1
6
7
12
24
36
48
Safaeian et al. in preparation
I. Natural History
Background
• HPV vaccine evokes high levels of antibodies
that are protective for HPV16/18 infections and
associated lesions
• Neutralizing antibodies are demonstrated to be
sufficient for protection in animals
Do antibodies produced following HPV infection
protect against subsequent HPV infections?
Impact of antibodies on future infection
- Methods
Costa Rica HPV16/18 Vaccine Trial (CVT): Control Arm
Control Arm: N=3736
Exclusions: N=923
HPV16 DNA- N=2813
HPV16 Sero+ (N=699; 25%)
HPV16 Sero- (N=2114; 75%)
Impact of antibodies on future infection
- Methods
• Exposure: anti-HPV16 (or 18) serostatus at
entry among HPV16 (or 18) DNA-negatives at
enrollment
– Tertiles
• Outcome: Rates of newly detected HPV16 (or
18) infections during follow-up
• Direct (polyclonal) ELISA used to measure
seropositivity
Multivariate Rate Ratio
Elevated antibody levels associated with decreased risk of
infection compared with seronegatives for both
HPV16 (50%) and HPV18 (60%)
10
Seronegative: Reference
Seropositive: Low tertile
Seropositive: Medium Tertile
Seropositive: High Tertile
Sero-
1
0.5
0
HPV16
HPV18
Safaeian et al., JNCI, 2010
Implications
• High levels of vaccine evoked antibody
Median HPV 16 AB in the high tertile group
133 (85-255)
Median HPV16 AB among vaccinated women
At 7 months
At 12 months
3631 (1823-5520)
At 48 months
2304 (1381-4308)
1212 (623-2449)
• Duration of current vaccine protection may be
long.
II. Vaccination
Cross-protection
Summary of the ATP vaccine efficacy reported for
selected HPV types not in the vaccine formulation
FUTURE1
Gardasil
6-month
persistence
PATRICIA2
Cervarix
12-month
persistence
CVT3
Cervarix
12-month
persistence
Related type
HPV31
HPV58
HPV33
33.6%*
12.8%
22.5%
80.5%*
-17.7%
41.0%*
45.7%*
-6.3%
37.3%
HPV45
20.1%
60.0%*
52.0%
Outcome Evaluated
Vaccine HPV type
HPV16
HPV18
*Statistically significant VE
64
1: NEJM 2007
2: Lancet 2009
3: Cancer Discovery 2011
Which marker to follow-up?
• 48 women
– Randomly selected, 3 doses of the vaccine received
• Sera from enrollment, 1m and 12m visits
• SEAP (an assay to measure neutralizing
potential) with:
– HPV16, HPV18 (positive control)
– HPV31, HPV45 (vaccine efficacy observed)
– HPV52, HPV58 (no vaccine efficacy)
– BPV (negative control)
Cross-Protection Pilot Study
*
*
*
*
*p<0.001
Kemp…Safaeian et al., Vaccine, 2011
Cross-Protection Pilot Study
*
*
*
*p<0.001
Kemp…Safaeian et al., Vaccine, 2011
Cross-Protection Pilot Study
*
*
*
*
*p<0.001
Kemp…Safaeian et al., Vaccine, 2011
Cross-Protection Pilot Study
*
*
*
*
*p<0.001
Kemp…Safaeian et al., Vaccine, 2011
Cross protection findings
• Characterized and optimized the SEAP for
several phylogenetically related HPV types
• Neutralizing antibodies may be responsible
Cross-protection
Nested Case-control Study
• HPV vaccinated arm only
• Compare immune responses of:
– Cases: HPV vaccinated women with an incident
infection with HPV types 31 (n=97), 45 (n=55), and 58
(n=100)
– Controls: HPV vaccinated women without infection
with these types (n=120)
• Serum from multiple time-points tested and levels
compared between cases and controls.
Acknowledgements
• Proyecto Guanacaste, Costa Rica
– Rolando Herrero
– Ana Cecilia Rodriguez
– Paula Gonzalez
– Carolina Porras
– Silvia Jimenez
– Jorge Morales
• DDL
– Wim Quint
– Leen-Jan van Doorn
•
•
•
•
•
HPV Immunology Lab
Ligia Pinto
Troy Kemp
David Pang
Marcus Willliams
• US NCI
– Allan Hildesheim
– Sholom Wacholder
– Mark Schiffman
– Diane Solomon
– Mark Sherman
– John Schiller
– Doug Lowy
– Sarah Coseo
– Wenny Lin
– Arpita Ghosh
• GSK
Sylviane Poncelete
Francis Dessy
• PPD
• Mark Esser
Special thanks to the women of Guanacaste who participated in this study.
E
EXTRA SLIDES
Results from Randomized Clinical Trials of
HPV L1 VLP Vaccines
Both quadrivalent (HPV-16,-18, -6, -11) and bivalent (HPV-16, 18) vaccine trials showed:
- High levels of immunogenicity
>99% seroconversion rates in 9-26 years old
Antibody titers considerably higher than observed in natural infection
Antibodies increase with each dose and decline over time after the 3rd dose
Heterogeneity observed between individuals; this heterogeneity not well
understood
74
Antibody Responses to the Vaccine Sustained
Through 6.4 years
B, Romanowski for the GlaxoSmithKline
Vaccine HPV-007 Study Group;
75Lancet
2009
Serum Neutralizing Antibody Levels After Cervarix &
Gardasil Vaccination
Direct Comparison
Reverse Cumulative Distribution Curves After 3 Doses
(HPV DNA/Sero-Negative at Entry)
18-26 years
76
(Einstein M. et al. Hum Vaccine 2009)
Assays used to measure HPV
Immunogenicity
Polyclonal (P) vs.
Monoclonal (M)
P
Neutralizing
No
Remark
GSK
Competitive
Luminex
immunoassay
(cLIA)
M
Yes
Merck
Secreted alkaline
phosphatase
neutralization
assay (SEAP-NA)
P
Yes
Name
ELISA
Throughput,
volume
requirement
High throughput,
low sample
volume
High throughput,
multiplexing, high
sample volume
Gold standard; Low throughput,
Laborious
high sample
volume
HPV Vaccine Studies at the HPV Lab
Defining Markers of Immune Responses to Vaccination
(Ultimate goal is to correlate against long-term vaccine success/failure)
Humoral Immunity:
HPV Neutralizing antibodies induced by vaccination in blood and at the
cervix
Validation and optimization of assays to identify ideal assay and
sample type
Cross-Neutralizing antibodies associated with protection against crossrelated HPV types
Antibody Avidity and B cell memory responses
78
HPV Vaccine Humoral Immunity: Systemic
and Mucosal Anti-HPV16 and Anti-HPV18
Antibody Responses from Vaccinated Women
1. Which is the ideal method for monitoring antibody responses
in clinical trials?
2. Are systemic levels of antibodies reflective of cervical levels ?
(Kemp et al. 2008. Vaccine) 79
Main Methods Used in Clinical Trials for
Measurement of Antibodies
- HPV IgG Levels
- ELISA (direct and V5/J4 inhibition assay)
- Luminex Bead Assay (cLIA)
- Neutralization Potential
- SEAP (neutralization assay)
80
ELISA correlated very well with the SEAP-NA
Serum
Cervical Secretion
A.
C.
105
N= 100
Spearman= 0.91
p< .0001
105
Anti-HPV16 Titer (1/Dilution)
Anti-HPV16 Titer (1/Dilution)
106
104
103
102
101
100
N= 42
Spearman= 0.84
p< .0001
104
103
HPV-16
102
101
100
100
101
102
103
104
105
106
100
101
Anti-HPV16 VLP IgG (EU/ml)
104
D.
106
105
N= 42
Spearman= 0.89
p< .0001
105
N= 100
Spearman= 0.85
p< .0001
Anti-HPV18 Titer (1/Dilution)
Anti-HPV18 Titer (1/Dilution)
103
Anti-HPV16 VLP IgG (EU/ml)
B.
SEAP-NA
102
104
103
102
101
100
104
103
HPV-18
102
101
100
100
101
102
103
104
Anti-HPV18 VLP IgG (EU/ml)
ELISA
105
106
10-1
100
101
102
103
Anti-HPV18 VLP IgG (EU/ml)
81
(Kemp et al. 2008. Vaccine)
104
Serum antibody titers are generally
levels
ELISA reflective of cervical
SEAP-NA
(10-20 fold lower)
A.
106
N= 42
Spearman= 0.73
p< .0001
105
Anti-HPV16 Titer (1/Dilution)
Anti-HPV16 VLP IgG (EU/ml)
106
C.
104
103
102
101
100
N= 42
ELISA
Spearman= 0.74
p< .0001
105
104
103
HPV-16
102
101
100
100
101
102
103
104
105
101
102
Anti-HPV16 VLP IgG (EU/ml)
D.
106
105
N= 42
Spearman= 0.64
p< .0001
106
N= 42
Spearman= 0.75
p< .0001
Anti-HPV18 Titer (1/Dilution)
Anti-HPV18 VLP IgG (EU/ml)
104
Anti-HPV16 Titer (1/Dilution)
B.
Serum
103
104
103
102
101
100
105
104
103
HPV-18
102
101
100
10-1
100
101
102
103
Anti-HPV18 VLP IgG (EU/ml)
104
105
101
102
103
Anti-HPV18 Titer (1/Dilution)
82
(Kemp et al. 2008. Vaccine)
Cervix
104
Cross-protection
• 48 women
– Randomly selected, 3 doses of the vaccine received
• Sera from enrollment, 1m and 12m visits
• SEAP with:
– HPV16, HPV18 (positive control)
– HPV31, HPV45 (vaccine efficacy observed)
– HPV52, HPV58 (no vaccine efficacy)
– BPV (negative control)
HPV Neutralizing Titers (SEAP)
Cross-Protection Pilot Study
10000
Pre-Vax
*
1 dose
All doses
*
1000
100
*
*
10
1
HPV16 HPV18 HPV31 HPV45 HPV52 HPV58
*p<0.001
BPV
HPV Type
Kemp…Safaeian et al., Vaccine, 2011
HPV Neutralizing Titers (SEAP)
Cross-Protection Pilot Study
Pre-Vax
10000
*
1 dose
All doses
*
1000
*
*
100
*
10
1
HPV16 HPV18 HPV31 HPV45 HPV52 HPV58
*p<0.001
BPV
HPV Type
Kemp…Safaeian et al., Vaccine, 2011
HPV Neutralizing Titers (SEAP)
Cross-Protection Pilot Study
Pre-Vax
10000
*
1 dose
All doses
*
1000
*
100
*
*
*
10
1
HPV16 HPV18 HPV31 HPV45 HPV52 HPV58
*p<0.001
BPV
HPV Type
Kemp…Safaeian et al., Vaccine, 2011
HPV Neutralizing Titers (SEAP)
Cross-Protection Pilot Study
Pre-Vax
10000
*
1 dose
All doses
*
1000
*
100
*
*
*
10
1
HPV16 HPV18 HPV31 HPV45 HPV52 HPV58
*p<0.001
BPV
HPV Type
Kemp…Safaeian et al., Vaccine, 2011
Cross protection findings
• Characterized and optimized the SEAP for
several phylogenetically related HPV types
• Neutralizing antibodies may be responsible
HPV Vaccine Humoral Immunity: Analysis
of New Functional Markers
Antibody Avidity
Memory B cell responses
(Dauner & Pan, submitted)
89
Expanding our understanding of the humoral
immune response
• Functional aspects of B cell responses to HPV vaccines have not been
examined previously
– Avidity plays an important role in protection against infections
– Memory B cells are important for long-term protection against viral infection
• We are interested in understanding:
– The effect of vaccine on affinity and B-cell memory
– The correlation between affinity/B-cell memory measures and total antibody
levels generated by vaccination
• Ultimate goal: Evaluate role of antibody avidity and memory B-cells on
long-term protection against vaccine types and cross-related types.
90
Avidity ELISA
• Affinity is the measure of the strength of a single interaction
between molecules
• Avidity is the total strength due to multiple interactions
– Applies to antibodies because they are bivalent
• Technique
– ELISA based methods using a chaotropic agents disrupt proteinprotein interactions (between antibody and antigen)
91
Avidity Levels Increase With the Number
of Doses
Vaccine
Received
Sample
Collection
Month 0
Month 1
Month 0
Month 1
Month 6
Month 2
Month 7
92
Month 12
Avidity Levels and Correlations with Antibody
Titers Following Vaccination
Time
Avidity
Index*
(Median)
IQR
Correlation with
ELISA
(Spearman r)
p value
Month 1
0.96
0.75-1.25
0.08
0.56
Month 12
2.78
2.45-2.93
0.45
0.001
*Data reported as the Molar concentration that reduces bound antibody levels by 50%
(Dauner et al. Submitted)
93
Antibody Avidity Studies
• The avidity assay is highly reproducible.
• Avidity levels increase with increased number of
vaccination doses.
• Avidity levels do not correlate well with antibody
titers.
• Further evaluation of avidity is planned to better
understand its kinetics and potential role in longterm protection.
94
4 Critical Obstacles to
Reducing Cervical Cancer Incidence
1. Vaccination schedules need to be simplified and
adaptable for different populations.
2. One-day screening and treatment based on affordable
efficacious technologies must be instituted.
3. Cryotherapy must be improved to increase the
likelihood of full ablation of persistent infections and
precancerous lesions.
4. The two prevention strategies, vaccination and
screening, must studied together to understand the
integration of the two and the impact of vaccination on
screening.
HPV Screening
52 clusters
1200-3900 mujeres asignadas al azar
HPV
Cytology
VIA
Control
34,126
32,058
34,074 mujeres
31,488
79.7%
screened
79.7% screened
78.6% screened
7.0%
13.9% positive
10.3% positive
89.1% colposcopy
positive
87.9%
colposcopy
Osmanabed District, Maharashtra State, India,
Sankaranarayanan et al., NEJM, 2009
98.7%
colposcopy
Study Groups
• 200 girls aged 12-20 years (as of August 31, 2011) who received
only one dose of HPV vaccine in the period October 1, 2008October 31, 2009, as a part of the PATH-UNEPI HPV vaccine
demonstration project
• 200 girls aged 12-20 years (as of August 31, 2011) who received
only two doses of HPV vaccine in the period October 1, 2008October 31, 2009, as a part of the PATH-UNEPI HPV vaccine
demonstration project
• 200 girls aged 12-20 years (as of August 31, 2011) who received all
three doses of HPV vaccine from October 1, 2008-October 31,
2009, as a part of the PATH-UNEPI HPV vaccine demonstration
project.
In the right settings,
cervical cancer can be prevented with a
moderately sensitive test
• Forgiving disease: long pre-clinical detectable
phase
• Almost all precancer can be treated when
detected early
• With regular screening, an insensitive test will
detect all but the most rapidly developing
cases!
HPV
Testing
Group
Cytologic
Testing
Group
Rate (N)
Rate (N)
VIA Group
Rate (N)
Control
Group
Rate (N)
Incidence of 47.4 (127)
all cervical
cancer
60.7 (152)
58.7 (157)
47.6 (118)
Incidence of 14.5 (39)
stage II or
higher
cervical
cancer
23.2 (58)
32.2 (86)
33.1 (82)
Cancer
death
21.5 (54)
20.9 (56)
25.8 (64)
12.7 (34)
Sankaranarayanan et al. NEJM. 2009
B. Competitive Luminex
Immunoassay (cLIA)
A. HPV16 ELISA
C. Pseudovirion Neutralization Assay
PE
H16.V5
HRP
HRP
HRP
HRP
SEAP
SEAP
VLP
VLP
293TT
SEAP
B. Competitive Luminex
Immunoassay (cLIA)
A. HPV16 ELISA
C. Pseudovirion Neutralization Assay
PE
H16.V5
HRP
HRP
HRP
HRP
SEAP
SEAP
VLP
VLP
293TT
SEAP
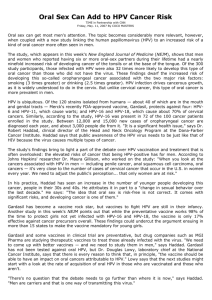
Figure X. HPV-16 VLP specific-IgG ELISA, competitive Luminex ImmunoAssay (cLIA) and pseudovirion neutralization assays.
Illustration is a schematic representation of the 3 assays that were used to measure HPV16 antibodies from the placebo arm
of the HPV 16/18 vaccine trial performed in Costa Rica. A. HPV 16 ELISA measures both non-neutralizing and neutralizing
serum IgG that binds to baculovirus expressed L1 VLP 16 coated on ELISA plates. Human IgG bound to the VLPs is detected
with a horse-radish peroxidase (HRP) conjugated xxx anti-human IgG. Antibody levels are reporeted in ELISA units/mL. B.
HPV 16 cLIA measures serum IgM, IgA and IgG that compete with a phycoerythrin-labeled (PE) neutralizing monoclonal
antibody, H16.V5, for binding to a neutralizing epitope on L1 VLP 16 conjugated to a Luminex microsphere. Antibody levels
are reported in milli-Merck Units/mL (mMU/mL). C. Pseudovirion neutralization assay measures serum IgM, IgA and IgG
that can neutralize SEAP expressing L1+L2 pseudovirions from binding to and infecting 293TT cells. SEAP expression is
measured 72 hrs after infection and antibody titers are reported reflect the reciprocal of the dilution that results in a 50%
reduction in SEAP activity compared to control wells. Antibody levels are reported in titer units (TU).
HPV Immunoepidemiology Studies
Natural History
Vaccination
Studies at the HPV Immunology Lab
HPV VLP Vaccine
Cellular Immune Responses
Humoral Immune
Responses
Neutralizing Abs
Affinity
Systemic
Local
B cell memory
T cell proliferative Th1; Th2;
responses
inflammatory
cytokines
Cross-reactivity
?
Correlates/Mechanisms ?
Long-Term Protection
Cross Protection
Host Gene
Expression
Profiles
HPV16/18 Immunogenicity
106
Vaccine Immunogenicity - CVT
HPV16 & HPV18 ELISA GMT: by vaccination arm
Antibody Levels (GMT) EU/mL
10000
1000
HPV Vaccinated
100
Naturally Infected
Not infected
10
1
0
1
6
7
12
24
36
48
Safaeian et al. in preparation
I. Natural History
Background
• HPV vaccine evokes high levels of antibodies
that are protective for HPV16/18 infections and
associated lesions
• Neutralizing antibodies are demonstrated to be
sufficient for protection in animals
Do antibodies produced following HPV infection
protect against subsequent HPV infections?
Impact of antibodies on future infection
- Methods
Costa Rica HPV16/18 Vaccine Trial (CVT): Control Arm
Control Arm: N=3736
Exclusions: N=923
HPV16 DNA- N=2813
HPV16 Sero+ (N=699; 25%)
HPV16 Sero- (N=2114; 75%)
Impact of antibodies on future infection
- Methods
• Exposure: anti-HPV16 (or 18) serostatus at
entry among HPV16 (or 18) DNA-negatives at
enrollment
– Tertiles
• Outcome: Rates of newly detected HPV16 (or
18) infections during follow-up
• Direct (polyclonal) ELISA used to measure
seropositivity
Multivariate Rate Ratio
Elevated antibody levels associated with decreased risk of
infection compared with seronegatives for both
HPV16 (50%) and HPV18 (60%)
10
Seronegative: Reference
Seropositive: Low tertile
Seropositive: Medium Tertile
Seropositive: High Tertile
Sero-
1
0.5
0
HPV16
HPV18
Safaeian et al., JNCI, 2010
Implications
• High levels of vaccine evoked antibody
Median HPV 16 AB in the high tertile group
133 (85-255)
Median HPV16 AB among vaccinated women
At 7 months
At 12 months
3631 (1823-5520)
At 48 months
2304 (1381-4308)
1212 (623-2449)
• Duration of current vaccine protection may be
long.
II. Vaccination
Cross-protection
Vaccine Efficacy Against Related HighRisk HPV Types
Vaccine HPV type
HPV16
HPV18
Meerck
GSK
CVT
Gardasil
Cervarix
Cervarix
Related type
6-month
persistence
12-month
persistence
12-month
persistence
HPV31
33.6%
80.5%
45.7%
HPV33
22.5%
41.0%
37.3%
HPV52
2.3%
−7.8%
−20.0%
HPV58
2.8%
−17.7%
−6.3%
HPV45
20.1%
60.0%
52.0%
Which marker to follow-up?
• 48 women
– Randomly selected, 3 doses of the vaccine received
• Sera from enrollment, 1m and 12m visits
• SEAP (an assay to measure neutralizing
potential) with:
– HPV16, HPV18 (positive control)
– HPV31, HPV45 (vaccine efficacy observed)
– HPV52, HPV58 (no vaccine efficacy)
– BPV (negative control)
Cross-Protection Pilot Study
*
*
*
*
*p<0.001
Kemp…Safaeian et al., Vaccine, 2011
Cross-Protection Pilot Study
*
*
*
*p<0.001
Kemp…Safaeian et al., Vaccine, 2011
Cross-Protection Pilot Study
*
*
*
*
*p<0.001
Kemp…Safaeian et al., Vaccine, 2011
Cross-Protection Pilot Study
*
*
*
*
*p<0.001
Kemp…Safaeian et al., Vaccine, 2011
Cross protection findings
• Characterized and optimized the SEAP for
several phylogenetically related HPV types
• Neutralizing antibodies may be responsible
Cross-protection
Nested Case-control Study
• HPV vaccinated arm only
• Compare immune responses of:
– Cases: HPV vaccinated women with an incident
infection with HPV types 31 (n=97), 45 (n=55), and 58
(n=100)
– Controls: HPV vaccinated women without infection
with these types (n=120)
• Serum from multiple time-points will be tested
ALTS ASCUS Conclusions
• HPV triage (sensitivity 92% with 53% of women referred to colposcopy)
– detects as much CIN 3 as immediate colposcopy
– spares approx half of women the cost and anxiety of colposcopy
• Repeat cytology (sensitivity 95% with 67 % of women referred to
colposcopy)
– safe option at a threshold of ASCUS
– women must be compliant with follow-up visits
– however, the trade off of sensitivity with specificity is not as
favorable as with HPV testing.
Geographic distribution of the world ASIR of cervical cancer, by country, estimated for 2008
(per 100 000 women-years).
Arbyn M et al. Ann Oncol 2011;22:2675-2686
© The Author 2011. Published by Oxford University Press on behalf of the European Society for
Medical Oncology. All rights reserved. For permissions, please email:
journals.permissions@oup.com
HPV
NEGATIVE
Younger age
Increasing # sex partners
HPV type (HPV-16)
“Male factor”*
Host immune response
Exogenous factors eg.
Smoking?
HPV
POSITIVE
HPV type
HPV
PERSISTENCE
CIN-3
Increasing
age
INVASIVE
CANCER
Increasing age
HPV type (HPV-16), Multiple HPV
types?
Smoking
Multiparity? OC use?
Chlamydia? No use of condoms?
HLA? Nutrients?
*no circumcision, increasing number of sex partners, visits to prostitutes, no
condom use
OC: Oral contraceptives
**data from case-control studies
HLA: Human leukocyte antigen
Vaccine, Vol 24 Supplement 3, 2006. © 2006 Elsevier Limited. All rights reserved. Chapter 05, Figure 7
OVERVIEW OF FACTORS MOST CONSISTENTLY REPORTED TO
PLAY A ROLE AT DIFFERENT STAGES IN THE NATURAL
HISTORY OF THE HPV AND CERVICAL NEOPLASIA
CIN: Cervical intraepithelial neoplasia
Phase III Trials--Main Results
•Design: double blind, placebo controlled trials of
>10,000 women
•Main Finding: protection against cervical precancer
caused by HPV16/18 among women naïve to these
types during the vaccination period: VE ~100%
•Tolerability: slightly more injection site pain than
control vaccine
•Immunogenicity: 99.5% seroconversion with titers
10-50 fold higher than natural infection
•Safety: no evidence of elevated adverse events
among vaccinees
Burden of HPV in all cancers
Site
Attributable
to HPV
(%)
Of which,
HPV16/18
(%)
Total Cancers
Attributable
to HPV
% of all
cancers
Cervix
100
70
492,800
492,800
4.54
Penis
40
63
26,300
10,500
0.1
Vulva, vagina
40
80
40,000
16,000
0.15
Anus
90
92
30,400
27,300
0.25
Mouth
3
95
274,300
8200
0.08
Oropharynx
12
89
52,100
6200
0.06
10,862,500
561,100
5.17
All sites
Adapted from Parkin and Bray, Vaccine 2006
30
20
10
5
1955 1960 1965 1970 1975 1980 1985 1990 1995
YEAR
Denmark
Finland
Norway
Parkin DM, et al. Cancer incidence in five continents, vol. I–VIII. Lyon: IARC CancerBase No. 7; 2005.
Sweden
Vaccine, Vol 24 Supplement 3, 2006. © 2006 Elsevier Limited. All rights reserved. Chapter 02, Figure 8
AGE-STANDARDIZED RATES PER 100,000 (WORLD)
TIME TRENDS IN AGE-STANDARDIZED (WORLD) INCIDENCE
RATES OF CERVICAL CANCER INCIDENCE IN FOUR NORDIC
COUNTRIES
Two Broad Classes of HPV Vaccines
Prophylactic
•
•
Antibody-mediated
protection
Rely on IR to structural
proteins (L1 VLPs)
Therapeutic
• CMI-mediated protection
• Rely on IR to proteins
required for maintenance
of infection &
transformation (E2/E6/E7)
129
Methods
• Cohort- between an ITT and ATP
– Excluded those with zero follow-up time or HPV16
and18 DNA+ at enrollment
• Endpoint- Event defined as newly detected
HPV16 or 18 infection that persisted 1+ years
• Statistical analysis
– Dose-specific VE and 95%CI
Efficacy Against Incident Infection by
Other High Risk HPV Types
High-risk
HPV types
31
16 35 33 58 52
X
X X
34
18 45 39 68
26 51
30 53 56 66
Dose- stratified VE after 4-yrs follow-up
# of
Doses
Arm
#
Women
# with
persistent
HPV16/18
infection
Control
3010
133
% with
persistent
HPV16/18
infection
4.4%
3
HPV16/18 VE (95%CI)
80.9% (71.1% to 87.7%)
HPV
2957
25
0.9%
Control
380
17
4.5%
2
84.1% (50.2% to 96.3%)
HPV
422
3
0.7%
Control
188
10
5.3%
1
100% (66.5% to 100%)
HPV
196
0
Kreimer AR et al Provisionally accepted JNCI
0.0%
Dose- stratified VE after 4-yrs follow-up
# of
Doses
Arm
#
Women
#
persistent
HPV16/18
infection
Control
3010
133
% with
persistent
HPV16/18
infection
4.4%
3
HPV16/18 VE (95%CI)
80.9% (71.1% to 87.7%)
HPV
2957
25
0.9%
Control
380
17
4.5%
2
84.1% (50.2% to 96.3%)
HPV
422
3
0.7%
Control
188
10
5.3%
1
100% (66.5% to 100%)
HPV
196
0
Kreimer AR et al Provisionally accepted JNCI
0.0%
")