ASKING THE QUESTION ABOUT
VIOLENCE AND ABUSE IN
ADULT MENTAL HEALTH
ASSESSMENTS
Third Edition November 2014
INTRODUCTION
Aims
To enable staff to take the first step towards
providing better support to service users, through
routinely enquiring about experience of abuse and
violence in mental health assessments
Course outline
Morning
• Why routinely enquire about violence and
abuse?
Afternoon
• How should you ask clients whether they’ve
experienced violence or abuse?
• What should happen next?
Learning outcomes
Participants will:
• Have greater knowledge and awareness of the
potential consequences of violence and abuse
• Have the confidence to routinely ask about
violence and abuse as part of assessments
• Be able to respond appropriately to disclosures
Before we begin…
•
•
•
•
Introductions
Practical arrangements
Looking after yourself
Confidentiality
WHY ASK THE QUESTION?
What are we talking about?
Child sexual abuse
Domestic violence
Female Genital
Mutilation
Coercive control
Forced marriage
Interpersonal violence
Partner abuse
‘Honour’ killings
Physical abuse & neglect
Sexual assault
Rape
Who are we talking about?
People who have past experiences of violence and
abuse – as children or adults, or who are currently
involved in violent and abusive relationships, and
who are often referred to as victims or survivors
Social inequalities, power and risk:
“Whenever one person or group has
more power than the other(s) in a relationship,
the danger of harm increases” (p. 375) 1
So, can you identify the people who are most ‘at
risk’ of violence and abuse?
Baker-Miller, J. (2008). "VI. Connections, Disconnections, and Violations." Feminism and
Psychology 18: 368-380.
1
How did violence & abuse get
recognised as a mental health issue?
1970’s: Named by feminism
1980’s: Media recognition of abuse and violence
1990’s: User voice; social action
2000’s: Policy response; greater focus on men
Service context
• Increased numbers of adult survivors seeking
support
• Services developed in the voluntary sector
e.g. Rape Crisis, Survivors UK, Women’s Aid
• But many mental health services still not
offering service users opportunities to talk
about experiences of abuse and violence
CPA guidance states that:
“Questions should be asked by suitably trained
staff at assessment about the experience of
physical, sexual or emotional abuse at any time in
the service user’s life. The response, with brief
details, should be recorded in case records/care
plans. If the specific question is not asked, the
reason(s) for not doing so should be recorded.”
Refocusing the Care Programme Approach, Policy and
Positive Practice Guidance, Section 4, March 2008
Barriers to implementing the guidance in
Mental Health Services include:
• Few staff have had relevant training
• Many are anxious about saying the
wrong thing
• Sexual abuse in particular is seen as an
issue to be dealt with by specialists
How common is violence and abuse in
the general population ?
• 17.5% of girls and 11.6% of boys have experienced severe
maltreatment by a parent during childhood1
• 7.8% of girls and 5.1% of boys have experienced contact
sexual abuse1
• 1 in 25 of the population has experienced extensive
physical and sexual violence, with an abuse history
extending back to childhood. Over 80% are women 2
Radford, L, S. Corral, C. Bradley, H. Fisher, C. Bassett, N. Howat and S. Collishaw (2011). Child abuse and neglect in the UK
today. London, NSPCC: 2 Scott, S, Williams, J, Kelly, L, McNaughton Nicholls C, McManus, S (2013) REVA Briefing No 1:
Violence, abuse and mental health in England. London, NatCen.
1
How common is violence and abuse in
the general population: ?
• 35% of women worldwide have experienced IPV or non•
•
partner sexual violence1
1in 10 of the population have experienced violence from
a partner and 1 in 50 extensive violence and coercive
control - Over 80% of these are women 2
Women who experience abuse from a partner typically
experience more severe violence and control, fear and
serious psychological consequences3
1 World
Health Organization (2013). Global and regional estimates of violence against women: prevalence and health violence
(Summary). Geneva, World Health Organization. 2 Scott, S, Williams, J, Kelly, L, McNaughton Nicholls C, McManus, S (2013)
REVA Briefing No 1: Violence, abuse and mental health in England. London, NatCen. 3Ansara, D. L. and M. J. Hindin (2011).
"Psychosocial Consequences of Intimate Partner Violence for Women and Men in Canada." Journal of Interpersonal Violence
26(8): 1628-1645.
How common is violence and abuse amongst
people using mental health services?
A review1 of 46 studies of women and 31 studies of men
using in-patient and outpatient MH services found:
Women
(n=2604)
Men
(n=1536)
1 Read,
Sexual
Abuse
46%
Physical
Abuse
48%
28%
50%
J; van Os, J; Morrison, A et al (2005) Childhood trauma, psychosis and schizophrenia. A literature
review with theoretical and clinical implications. Acta Psychiatrica Scandinavia, 112, 330-350
How common is violence and abuse amongst
people using mental health services?
• Studies of severe domestic violence report lifetime
prevalence rates amongst MH service users ranging from
30% to 60%1
• Studies find that over 95% of women with major mental
health problems including those using forensic services,
have long histories of sexual and physical violence2
• Women using services are at increased risk of violent
victimisation and sexual exploitation3
1 Howard
LM, et al (2010). "Domestic violence and severe psychiatric disorders: prevalence and
interventions." Psychological Medicine. 40(6): 881-893: 2 Goodman, L. A., et al (2001). "Recent
victimization in women and men with severe mental illness: Prevalence and correlates." Journal of
Traumatic Stress 14(4): 615-632: 3 Trevillion, K. et al (2013). Domestic violence and mental health. In
Domestic Violence and Mental Health London, RCP Publications.
Understanding differential impacts of
violence and abuse
-
What happened?
+
-
Who did it?
+
-
How many times?
+
-
How long for?
+
-
Did they tell?
+
-
Were they believed?
+
-
Were they blamed?
+
-
Were they protected?
+
Psychological consequences
When significant others are violent or abusive, or
appear to be complicit in, or indifferent to what is
happening :
• The victim may feel fearful, silenced, shamed and
stigmatized
• Their abuser may foster the belief that they are
responsible for the abuse and their isolation
• The victim may cope with the trauma by
disconnecting from themselves and others
• Their efforts to survive may subsequently be
diagnosed and labelled as pathologies
A strong association with mental health
The impact on mental health is very evident from analysis of
the Adult Psychiatric Morbidity Survey1 This general
population study showed that:
• Over half the people with extensive abuse histories going
back to childhood (1 in 25 of the population) were
experiencing common mental health disorders (CMDs)
• 37% of the people who had experienced extensive
physical violence and coercive control in an adult
relationship (1 in 50 of the population) also had a CMD
1 REVA Briefing 1 Violence, Abuse and mental health in England. London: NatCen
Long-term consequences of trauma
•
•
•
•
•
•
•
•
•
•
Anxiety / fear
Anger / aggression
Unhappiness / depression
Lack of confidence / self-esteem
Feeling dirty / damaged / guilty
Physical health problems
Sleep disturbance
Intrusive memories
Inability to trust others
Problems with sex and relationships
A Respond Tree
Leaves = presenting difficulties
Branches = emotions and
psychological effects
Roots = cause(s) of distress
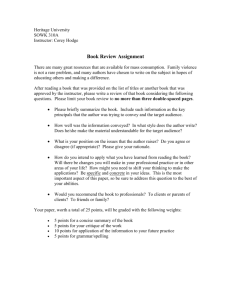
An Example Respond Tree
Violence
Self-harm
Sexual problems
Eating disorder
Phobias
Nightmares
Anxiety
Depression
PTSD
Compulsive
behaviour
fear
anger
pain
guilt
inability
to trust
shame
low selfesteem
Physical abuse
Sexual abuse
Emotional abuse
Ways of trying to cope with the impacts
of trauma
•
•
•
•
•
•
•
•
Dissociation
Avoiding relationships
Pursuing intense relationships
Keeping busy / self-distraction
Self-medication e.g drugs / alcohol
Self-harm / self injury
Somatisation
Watchfulness
Common service response: diagnosis
•
•
•
•
•
•
•
•
Depression
Obsessive-Compulsive Disorder
Eating Disorder
Bi-polar Disorder
Phobias
Psychosis / Schizophrenia
Borderline Personality Disorder
Post-Traumatic Stress Disorder
Post-Traumatic Stress Disorder
PTSD symptoms spell TRAUMA
• Traumatic event(s) occurred
• Re-experience of traumatic events as intrusive
thoughts, nightmares, flashbacks
• Avoidance of anything associated with the trauma and
emotional numbing
• Unable to function – significant social, occupational,
and interpersonal impairment
• One Month or more duration of symptoms
• High Arousal: startle reaction, poor concentration,
irritability, insomnia, and hyper-vigilance
Borderline personality disorder
Five or more of the following (DSM V, 2013):
• Frantic efforts to avoid real or imagined abandonment
• Unstable and intense interpersonal relationships
• Unstable self-image or sense of self
• Self-damaging impulsive behaviour
• Suicidal and self-mutilating behaviour
• Affective instability
• Chronic feelings of emptiness
• Inappropriate, intense anger or difficulty controlling anger
• Stress related paranoid thoughts or severe dissociative
symptoms
When services ignore violence and abuse
Clients:
• Don’t get the help they need
• Can be re-victimised by services
• Can have unnecessarily long contact with
services
• Staff don’t get the satisfaction of really helping
people and seeing their lives change
Why routine enquiry is important
• Asking is the essential starting point
• It creates the possibility of people getting the
•
•
•
help they need
It gives people permission to speak about their
experiences
It tells people that these types of experiences
are relevant to their distress
It provides services with evidence that can
inform their development
Why is it important to ask at assessment?
• Survivors want to be asked
• By asking the question at assessment, you are
saying it is OK to talk about violence and abuse
• If the question is not asked at assessment it
tends not to be asked later
• It reduces the likelihood that these experiences
will be challenged, should a case go to court
What survivors want
•
•
•
•
•
•
Ask as early as possible
Ask because you really want to know
Keep asking the question
Don’t be selective about who you ask
Respond helpfully
Follow up with good services
REVA Briefing 3 (2014) Why asking about abuse matters to service users. London: NatCen
LUNCH
HOW TO ASK THE QUESTION
Preparing the service user:
At the start of an assessment:
• Acknowledge that some questions might be
difficult or not relevant to them
• Make the boundaries of confidentiality clear:
‘What we talk about is confidential unless
you tell me about any serious risk of harm to
yourself or other people’
Asking the question
“Have you experienced physical, sexual or
emotional abuse at any time in your life?”
Yes
None stated
Not asked
If ‘Yes’, record brief details
If question not asked, please state reason
Trial run
Ask the question:
“Have you experienced any kind of
physical, sexual or emotional abuse in your
life?”
Record Keeping: Evidence
• Keep records, even if questions haven’t led to disclosure
•
•
•
they might in the future
Careful record keeping can enable people get justice,
welfare benefits and housing
Careful record keeping supports the efficient flow of
information
Ensure the record can only be accessed by those
directly involved in the person’s care
‘The solicitors said there just wasn’t enough evidence on my health records.
Nothing to suggest my ex was to blame for my injuries. I was so let down. I
thought my doctor had written down everything I said.’ (p. ADD)
Department of Health (2014). Responding to domestic abuse: a handbook for health
professionals. London, Department of Health.
Record Keeping: Service development
‘Asking the question’ makes it possible for data to be
gathered that can help managers to:
• Estimate the size of the NHS violence and sexual abuse
•
•
•
workload
Evaluate the effectiveness of current responses
Identify gaps in service delivery
Suggest ways to improve service commissioning
Why children don’t tell
•
•
•
•
•
•
•
Not asked or no-one safe to tell
Do not recognise it as abuse
Attached to the abuser
Threatened by the abuser
Believe they are to blame
Afraid of family break up, being sent away or
put into care
Lack the words to describe what’s happening
Why adults don’t tell
• Same reasons as children
• Fear of not being believed or getting negative
•
•
•
•
responses
Feel they should have told when it was
happening
Have repressed the memories
Fear the offender’s reaction
Worried about the impact of disclosure on their
family / community
Particular reasons why men don’t tell
• Difficulty in talking about emotional matters
• Fear of humiliation in court, and/or newspapers
• Ashamed that they weren’t ‘man enough’ to
•
•
•
prevent it
Believing they are the only one
Afraid people will think they are gay
If gay, being accused of "asking for it“
Will I become an abuser?
victims
abusers
Why adults do tell
• They now feel safe to do so e.g.
•
•
•
- being in a new relationship
- living away from home
Life events trigger memories
Concerned the abuser poses a risk to others
They are asked the question at assessment
RESPONDING TO A
DISCLOSURE
Hearing a disclosure – Part one
•
•
•
•
•
•
•
Re-assure the client that it was a good thing to tell
Have they told anyone before? How did that go?
Is it an issue that they need help with?
Is this the right time to deal with it?
Do not try to gather all the details
At the end of the assessment ask them how they
are feeling
Check they can access any immediate support
they need
After disclosure of past abuse
• People need to feel safe and supported
• Not all survivors want or need ongoing
help or therapy
• An empathic response may be enough
Hearing a disclosure – Part two
Don’t presume:
• They no longer have a relationship with
their abuser
• The abuser was a man
• They were abused by just one person
• You know what they feel or think about it
• Children are being protected
Providing support to survivors
Longer-term
therapy
Survivor support groups,
counselling
Guided self-help, support from nonspecialist staff, helplines etc
Self-help,
friends & family support
Providing support
“The GP did not provide my counselling – it is provided by a
local charity. They advised me that I need people around
me. Where I live I don’t have friends there. It affects you,
you have no support. You have no one to talk to you are
just all by yourself. That’s why this women’s group at the
Refugee Council is so important for me. They keep me
sane, knowing I will see other women here when I come.
Otherwise I wouldn’t see anyone for weeks.” (p. ADD)
Department of Health (2014). Responding to domestic abuse: a handbook for health
professionals. London, Department of Health.
Current risks?
• Any immediate implications for their care
• Are they still at risk / in contact?
• Are there safeguarding implications for
children?
Assessing Safety
Useful questions:
• Is it safe to go home?
• What has s/he threatened to do?
• What are you afraid might happen?
• Have they hurt the children?
• What helps you to keep safe? E.g.
people, places
Safety Planning
• Review crisis management tactics:
- how do they know it might happen?
- what do they do to reduce the impact?
- how do they manage afterwards?
• Help plan ahead in small practical and
•
•
•
achievable steps
Help identify what they need to stay safe
Validate their efforts no matter how small
Encourage them to be proactive when they can
Form a list of safe contacts
• Who do they feel safe talking to – family, friends,
professionals, helplines?
• Make a list of names and phone numbers to use in a
crisis including when they are available – keep the list
at hand.
• Ask friends about their contact limits – how much
support are they able to give, how late at night?
What the trust can offer
What other support is available
• SARCs - Sexual Abuse Referral Centres
• Rape Crisis Centres
• ISVAs/IDVAs – Independent Sexual/Domestic
Violence Advisors
• Refuges – Women’s Aid
• Legal Advice – Rights of Women
• Services for men
• The Survivor’s Trust
• Local rape support centres and National Helplines
Local voluntary sector services
Safeguarding Children Requirements
• Record what is disclosed and any
subsequent actions
• Note the whereabouts of the abuser and
whether they could pose a risk to children
• If there is any possibility of child protection
concerns contact the Safeguarding Lead
Support for staff
Staff who are well supported will support their clients well.
This includes:
• Team support
• Formal supervision
• Access to specific expertise in abuse
• Continuing professional development
Support for staff
• The prevalence of violence and abuse means
•
•
that there are NHS staff who have past or
current experience of domestic violence and
childhood abuse and staff who are abusers
Staff should feel able to disclose abuse and ask
for confidential support
Health services must demonstrate zero
tolerance of perpetrators in the workplace
DH, 2014
What is going to be different after
today?
Tell the person next to you:
• One thing you are going to do differently from
now on
• One thing you would like to do differently in the
future
And finally…
• Thank you
• Any final questions or comments?
• Please take 5 minutes to complete the
evaluation form