Physical, Cognitive, and Behavioral Implications
advertisement

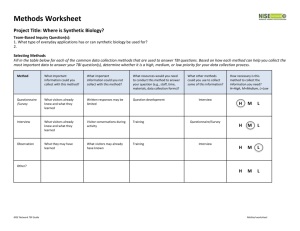
Traumatic Brain Injury: Physical, Cognitive and Behavioral Implications Anastasia Edmonston MS CRC TBI Projects Director Maryland Mental Hygiene Administration Training Agenda • The incidence and prevalence of TBI • What is brain injury? • What are the types of brain injury? Training Agenda • Common cognitive, behavioral and physical sequela of TBI • Ideal rehabilitation pathways for mild, moderate and severe TBI • The TBI, mental health and substance abuse connection Training Agenda • Why Screen? • How to Screen for a history of a TBI • Strategies to support individuals with TBI • Resources, medical, rehabilitation, community supports and employment Incidence of TBI CDC 2006 Worldwide, an estimated 10 million people incur a TBI serious enough to result in death or hospitalization each year Incidence of TBI CDC 2004 In the United States, at least 1.6 million sustain a TBI each year Incidence of TBI Of CDC 2004 those 1.6 million.. • 51,000 die; • 290,000 are hospitalized; and • 1,224,000 million are treated an released from an emergency department Annual Incidence of TBI with Disability AN ESTIMATED 124,000 American civilians Cited by Jean Langlois ScD,MPH NASHIA Conference 2007 Preliminary findings as analyzed by Selassie, et. al Returning Veterans • As of 11.07 VA officials reported that of 61,285 veterans screened since April 14, 2007 19% screened positive Honolulu Star-Bulletin Nov. 4, 2007 • Pentagon reported as of September 20, 2007, 4,471 of 30,327 wounded troops sustained brain injuries. • A September 2007 article in USA Today by Gregg Zoroya looked at data from a variety of military sources put the number as at least 5 times that much. (20,000) • In that same USA Today article, Rep. Bill Pascrell is quoted as saying more than 150,000 troops may have suffered brain injury in combat “Mild Traumatic Brain Injury in U.S. Soldiers Returning from Iraq” Hoge, McGurk, Thomas, et.al NEJM Volume 358:453-463 January 31, 2008 • 1 in 6 returning troops have had at least one concussion • 4.9% reported injuries with LOC of those, 43.9% met criteria for PTSD (3xs the rate found in those with other injuries) • 10.3% reported altered mental status, of those, 27.3% met criteria for PTSD • TBI with LOC also associated with major depression Incidence of TBI Maryland 2000 CDC Surveillance • 5,229 Marylanders sustained a moderate to severe TBI • 13 people a day • 5% of all hospitalizations TBI related Causes of TBI Unknown, 9% Suicide, 1% Other Transport, 2% Other, 7% Falls, 28% Pedal Cycle (non MV), 3% Assault, 11% Motor VehicleTraffic, 20% Struck By/Against, 19% CDC 2006 The Scope of the Problem By Age • Approximately 475,000 TBIs occur among children ages 0-14 • ED visits account for more than 90% of the TBIs in this age group • Adults age 75 years or older have the highest rates of TBI related hospitalization and death CDC 2004 Why are the Numbers so Big? • 30 years ago, 50% of individuals with TBI died, the number today is 22% • due to: • Improved medical technology and techniques • Safety features such as car seatbelts, child safety seats and airbags What are the Costs of TBI? CDC 2006 Direct medical costs and indirect costs such as lost productivity of TBI totaled an estimated 60 billion in the United States in 2000. (That is equal to the cost of building the international space center or 60 times the net worth of Oprah Winfrey )Jean Langlois of the CDC A Huge Public Health Issue…... With Very Little Public Awareness or Funding According to a 2000 Harris Poll... • 1 in 3 Americans interviewed were not familiar with the term “brain injury” • 2 in 3 or 66% believe that TBI occurs less frequently then breast cancer • 50% believe brain injuries happen less frequently than AIDS BIAA, 2000 In Fact……. • TBI results in 1 1/2 times more deaths each year then AIDS • Each year 1.5 million people sustain a TBI, that is 8 times the number of individuals diagnosed with breast cancer Public Funding for Brain Injury Outlook Magazine 2005 • 900,000 living with HIV/AIDS, Per person federally allocated $ = $18,111 • 4,557,000 living with MR/DD, Per person federally allocated $ = $4,635 • 3,000,000 living with Breast Cancer, Per person federally allocated $ = $295 • 5,3000,000 living with TBI, Per person federally allocated $ = $2.55 What happens in a TBI? • Mechanism – Acceleration/Deceleration – Differential movement of partially tethered brain within the skull • Results in: – Bruising of the brain surface against rough areas of the skull – Stretching and twisting of nerve axons Primary Injuries… Coup-Contra Coup Chuck Durgin 2007 Primary Injuries… Diffuse Axonal Injuries Rotational forces on the brain cause the stretching, snapping and shearing of axons …Primary Injuries Hematoma Epidural Hematoma Dura Hematoma or Blood Clot forms on top of the dura Dura …Primary Injuries Subdural Hematoma Dura Hematoma or blood clot forms under the dura Secondary Injuries Intracerebra l Hemorrhage Hydrocephalus (enlarged ventricles Edema (swollen brain tissue) Definitions: How brain injury may be defined in the Medical Record Traumatic Brain Injury is an insult to the brain caused by an external physical force Acquired Brain Injury is an insult to the brain that has occurred after birth, for example; TBI, stroke, near suffocation, infections in the brain, anoxia Types of TBI • Distribution of Severity: – Mild injuries = 80% (LOC < 30 min, PTA ,1 hour) – Moderate = 10 - 13% (LOC 30 min-24 hours, PTA 1-24 hours) – Severe = 7 - 10% (LOC >24 hours, PTA >24 hours) Using Post-Traumatic Amnesia (PTA) to Determine Severity of CHI Dr. Paul McClelland • When did you wake up from the head injury? Do you remember being transported to the hospital? Do you remember being in the trauma unit? Being transferred to the rehab unit? • PTA: period of time after the CHI for which the patient has no memory Types of TBI-Mild • Most common, 75%-85% of all brain injuries are mild • Individuals experience a brief (<15 minutes)or NO loss of consciousness • Normal neurological exam • 90% of individuals recover within 6-8 weeks, often within hours or days 2000 Epidemiological Study of Mild TBI J. Silver of NYU, cited in WSJ by Thomas Burton 1.29.08 http://online.wsj.com/article/SB120156672297223803.html?mod=googlenews_ • 5,000 interviewed • 7.2% recalled a blow to the head w/unconsciousness or period of confusion • Follow up testing found; 2x rate of depression, drug and alcohol abuse • Elevated rates of panic and and obsessive-compulsive DO “That first morning, wow, I didn’t want to move, I was thankful that nothing’s broken, but my brain was all scrambled” Ryan Church, NYT 3/10/08 “All he remembers from the collision with Anderson is the aftermath, being helped off the field by two people, although he said he did not know who they were until he saw a photograph later” Ben Shpigel NYT reporter Types of TBI-Moderate • LOC/Coma between 20-30 minutes to 24 hours, followed by a few days or weeks of confusion • EEG/CAT/MRI are positive for brain injury • 33-50% of individuals with moderate brain injury have long term difficulties in one or more areas of functioning Types of TBI-Severe • Almost always results in prolonged consciousness or coma of days,weeks, or longer • 80% of individuals with severe brain injury have multiple impairments in functioning Simplified Brain Behavior Relationships Frontal Lobe Parietal Lobe • Initiation • Problem solving • Judgment • Inhibition of behavior • Planning/anticipation • Self-monitoring • Motor planning • Personality/emotions • Awareness of abilities/limitations • Organization • Attention/concentration • Mental flexibility • Speaking (expressive language) • Sense of touch • Differentiation: size, shape, color • Spatial perception • Visual perception Temporal Lobe • Memory • Hearing • Understanding language (receptive language) • Organization and sequencing Frontal Lobe Parietal Lobe Occipital Lobe Temporal Lobe Occipital Lobe • Vision Cerebellum Cerebellum Brain Stem • Balance • Coordination • Skilled motor activity Brain Stem • Breathing • Heart rate • Arousal/consciousness • Sleep/wake functions • Attention/concentration Possible Changes-Physical • • • • • • • • Motor skills/Balance Hearing Vision Spasticity/Tremors Speech Fatigue/Weakness Seizures Taste/Smell Possible Changes-Thinking • • • • • Memory Attention Concentration Processing Aphasia/receptive and expressive language • • • • • • • Executive skills Problem solving Organization Self-Perception Perception Inflexibility Persistence Possible Changes-Personality and Behavioral • • • • • • • Depression Social skills problems Mood swings Problems with emotional control Inappropriate behavior Inability to inhibit remarks Inability to recognize social cues Personality and Behavioral cont.. • • • • • • Problems with initiation Reduced self-esteem Difficulty relating to others Difficulty maintaining relationships Difficulty forming new relationships Stress/anxiety/frustration and reduced frustration tolerance A memory deficit might look like trouble remembering or it might look like…… (Capuco & Freeman-Woolpert) • She frequently misses appointmentsavoidance, irresponsibility • He says he’ll do something but doesn’t get around to it • She talks about the same thing or asks the same question over and over-annoying perservation • He invents plausible sounding answers so you won’t know he doesn’t remember An attention deficit might look like trouble paying attention or it might look like … (Capuco & Freeman-Woolpert) • He keeps changing the subject • She doesn’t complete tasks • He has a million things going on and none of them ever gets completed • When she tries to do two things at once she gets confused and upset A deficit in executive skills might look like the inability to plan and organize or it might look like... (Capuco & Freeman-Woolpert) • Uncooperativeness, stubbornness • Lack of follow through • Laziness • Irresponsibility Unawareness might look like… (Capuco & Freeman-Woolpert) • Insensitivity, rudeness • Overconfidence • Seems unconcerned about the extent of her problems • Doesn’t think she needs supports • Covering up problems (“everything’s fine…”) • Big difference in what he thinks and what everyone else thinks about his behavior • Blaming others for problems, making excuses Lack of Awareness A common and difficult to remediate hallmark of a brain injury Levels of Awareness Crossen et.al (1989) J Head Trauma Rehabilitation • Intellectual Awareness-individual is able to understand at some level, that a particular function or functions is impaired. A greater level of intellectual awareness is required to recognize some common thread in the activities in which they have difficulty • Emergent Awareness-individual is able to recognize a problem when it is actually happening. To do so, they must recognize a problem exists (intellectual awareness), and realize when it occurs • Anticipatory Awareness-individual is able to anticipate a problem will occur and plan for the use of a particular strategy or compensation that will reduce the chances that a problem will occur, e.g. keep and refer to a calendar to support memory for daily schedule Ideal Rehabilitation Pathway for Mild TBI • Diagnosed after injury and provided with education and follow-up • If they are of the approximately 10% of mild TBI sufferers who continue to experience difficulty functioning, there is evidence of appropriate rehabilitation, neurological/neuropsychiatric/neuropsych ol-ogical treatment or consultation Common and Less than Ideal Pathway-Mild TBI • Discharged and released from ER or not even seen in ER • Memory, emotional lability, visual, vertigo, headaches and or fatigue symptoms do not resolve after the first few weeks following injury • If subsequently seen by GP or in the ER often told to just”take it easy” Common and Less than Ideal Pathway-Mild TBI, cont.. • Can’t function at work or home • Spiral into depression and anxiety • Family, friends and co-workers loose patience • If seen by a GP or neurologist may be viewed as having a psychosomatic reaction or be labeled a malingerinappropriately medicated Common and Less than Ideal Pathway-Mild TBI, cont.. • • • • • Job loss Mental Health Problems Relationships and supports erode At risk for Substance Abuse At risk for entry into the criminal justice system Ideal Medical/Rehabilitation Pathway-Moderate to Severe TBI • Acute care delivered at a trauma center (Shock Trauma, Johns Hopkins) • Inpatient rehabilitation at a CARF accredited brain injury rehabilitation hospital(Sinai, Kernan, Maryland General) • Outpatient rehabilitation at a CARF accredited brain injury rehabilitation center offering a community reentry program and individual therapies (Sinai, Kernan, Total Rehab Care,Treatment and Learning Centers) Moderate to Severe TBI Pathway cont..... • Referral to a state vocational services counselor with a TBI caseload • Vocational services as appropriate can include: vocational evaluation, work adjustment training, vocational training, job placement and job coaching • Support services in the community-case management and individual/family therapy Common and Less than Ideal Pathway-Mod to Severe TBI- Scenario I • Discharged prematurely from Trauma or Acute care to a nursing home • Not followed for improvements, and timing of rehabilitation intervention • Suffer from behavioral outbursts, not well managed by nursing home personnel unfamiliar with TBI issues Common and Less than Ideal Pathway-Mod to Severe TBI Scenario II • Discharged from Trauma or Acute due to good physical recovery • Referrals not made for continuing rehabilitation (cognitive therapy) • Impulse control, memory problems affect home, community, work and school • Family is strained • At risk for mental health problems, substance abuse, criminal behavior, entry into a state hospital Common and Less than Ideal Pathway-Mod to Severe TBI Scenario III • Injured as a child • Go through ideal pathway thru outpatient rehabilitation • Return to school, behind peers • Struggle academically • Act out behaviorally, if the injury was several grades back, not recognized as TBI related Common and Less than Ideal Pathway-Mod to Severe TBI Scenario III, cont. • Trouble making the transition to post graduation roles and responsibilities • Get in with the “wrong” crowd • At risk for mental health issues, substance abuse, criminal activity, burn out families and supports • May end up in one of the state hospitals The Relationship Between Brain Injury and Mental HealthDepression • Depression is the most common Axis I psychiatric disorder after TBI followed by alcohol abuse, panic disorder, specific phobia and psychotic disorders (Gordon et. al 2004) • A 50 yr.. Follow-up of 1,198 WWII vets found that 520 had incurred a TBI. 18.5% of vets with brain injuries had a life time prevalence of major depression verses 13.4% rate of depression among on brain injured vets (Holsinger et.al 2002) The Post -Concussive Syndrome and PTSD Dr. Paul McClelland • Increased startle response; especially to loud sounds • Irritability • Avoidance of many social events • Intolerance of new situations Organic Personality Disorder & Anti-Social or Hysterical Personality Traits Dr. Paul McClelland • • • • Decreased impulse control Labile and superficial affect Impaired insight and self awareness Decreased empathy and social awareness • Impaired initiative (Depression?) Partial Seizures & Panic Attacks or Dissociative States Dr. Paul McClelland • Most common type of post-traumatic epilepsy • Temporal lobe damage and complex partial seizures • “Spells” starting suddenly & lasting a few minutes • Olfactory (smell) or gustatory (taste) hallucinations • Déjà vu or jamais vu • Micropsia, macropsia and other symptoms Obsessive-Compulsive Traits after TBI: PreExisting Conditions or Adaptation to Cognitive Deficits & Other Changes? Dr. Paul McClelland • Compulsive behaviors as adaptations for memory loss • Temper tantrums and other adaptations • Non-pharmacological management of brain-injured patients Other Mental Health Disorders Related to TBI • PTSD is noted in some individuals following TBI even if there is no memory of the incidence (Klein, Caspi 2003) • Rapid cycling bipolar is rare but noted in the literature for individuals with temporal lobe damage (Murai, Fujimoto 2003) • Psychotic syndromes occur more frequently in individuals who have had a TBI then in the general population (McAllister, Ferrell 2002) TBI & Suicide • “The risk of attempted or completed suicide in neurological illness is strongly related to depression, feelings of hopelessness or helplessness, and social isolation” (Arciniegas & Anderson, 2002) • Simpson and Tate (2002) screened 172 individuals for suicidal ideation and hopelessness. Findings using the Beck Suicide Ideation and Hopelessness Scales found 35%felt hopeless and 23%expressed suicide ideation. 18% had attempted suicide post injury Alcohol Use & TBI-Incidence Analysis of the Literature (Corrigan 1995) • Alcohol, the drug of choice-Corrigan and his colleagues report that for 70% of the individuals they work with who use substances, alcohol is the preferred substance • Intoxication at time of injury-7 studies looked at incidence of intoxication (BAL equal or exceeding 100mg.dL)at time of injury. Intoxication ranged from 36% to 50% • History of Substance Abuse-Findings suggest that for adolescents and adults in rehabilitation following a TBI, as much as 60% of this population have histories of alcohol use or dependence. Alcohol TBI-How does Incidence and History Impact on Recovery & Outcomes? Studies Suggest….. • Alcohol may negatively affect the process of dendrite profusion thus impede ability of the remaining neurons to compensate for the neurons that have been damaged (Corrigan, NASHIA webcast 2003) • Alcohol use after brain injury may increase the risk of seizure post TBI • Increased brain atrophy observed in patients with a positive BAL and or history of moderate to heavy pre-injury use (Bigler et al 1996 & Wilde et.al 2004) • Performance on neuropsychological outcome variables by this group was generally worse, though not statically significant compared to other TBI groups (Wilde et.al 2004) The “Honeymoon” Effect-The Year Following Injury • Bombardier reports (1997) that in comparison with a separate medical patient sample, individuals with a recent TBI were more motivated to change their alcohol use. Motivational Interviewing was utilized and of 50 post TBI patients, 84% fell into the contemplation or action phases. Greater willingness to change was noted in those with alcohol involved injuries and higher daily consumption pre-injury The “Honeymoon” Effect-The Year Following Injury • In 197 individuals treated at a Level I trauma center, alcohol use diminished in the first year following TBI (Bombardier et.al 2003) • Kreutzer and colleagues (1996)Followed the pre-and post-injury patterns of alcohol and illicit drug use of 87 individuals at 8 and 28 months post TBI. Decline in use was noted at first follow-up. Use at second follow-up were similar to pre-injury use Honeymoon Factors • Individual in an inpatient and/or highly structured outpatient setting resulting in detoxification • Physical and cognitive disabilities make access to substances difficult • Families are instructed to provide supervision due to physical needs and judgement concerns • Individual is remorseful over past use, related behavior, blames self for accident and vows to change Subsequent Use-Risk Factors • Male • Younger age • History of substance abuse prior to injury • Diagnosis of depression since TBI • fair/moderate mental health • better physical functioning (Kreutzer 1996, Horner et.al 2005) Subsequent Use • 10-20% of those with TBI develop substance abuse problems after their injury (NASHIA Webcast 2001) • “A person with a preinjury history of two drinks a day would not have had a reason to seek alcohol-related treatment before his or her accident. But once that same person becomes brain-injured, the continuation of that drinking pattern has the potential to cause major problems” Robert Karol, Ph.D. Co-concurring with Subsequent Use….. • • • • Worse employment outcomes More likely to be living alone & isolated Greater criminal activity Lower subjective well-being or life satisfaction (NASHIA Webcast 2001) Suggested Strategies for Professionals Working with Individuals with TBI • Review if available any neuropsychological or neuropsychiatric records • Attend 12-Step meetings with a “buddy” or staff member, review meeting highlights • “90 meetings in 90 days” may be too stimulating or fatiguing after a TBI, balance so benefits of structure, social group can be gained • If the individual plans to share at a meeting, have them jot down before hand what they want to say on an index card Suggested Strategies for Professionals Working with Individuals with TBI • Avoid approaches that are confrontational (Sparadeo, NASHIA Webcast 2003) • Insight oriented treatment approaches may not work for individual’s whose thinking is very concrete after a brain injury • Offer “The Big Book” and other books with a recovery or inspirational theme on tape • “Where the body goes, the mind follows”, “One day at a time” etc. powerful Suggested Strategies for Professionals Working with Individuals with TBI • Use “Change Plan” & “Staying Clean, Staying Sober” Worksheets • Prepare for slip ups-”Emergency Plan”& “Personal Emergency Plan: Lapse” • Judicious use of drug testing • For additional strategies, see hand out; Substance Abuse Education and Intervention: Tips and Tools for Clinicians Working with Individuals with a History of Brain Injury Why Screen? What other TBI Screening efforts have found Findings from the Literature…Criminal Justice System • Researchers at Indiana State University found that 83% of felons studied reported a head injury that predated their first encounter with the law (1998) • Adults who had frontal lobe damage prior to age 8 exhibited recurrent impulsive and aggressive behavior • 14% of the subjects in the Vietnam Head Injury Project with frontal lobe lesions engaged in fights or damaged property compared to 4% of controls without TBI Domestic Violence TBI Findings • Batterers fared worse on three neuropsychological indicators of cognitive functioning then a nonbatterer control group (Cohen et. Al 1999) • Corrigan et.al., (2003) found that of 167 individuals treated for domestic violence related health issues, 30% experienced a loss of consciousness on at least one occasion, 67% reported residual problems that were potentially TBI related • Valera and Berenbaum, (2003) assessed 99 battered women. Of these, 57 had brain injured related symptomatology TBI Among Individuals with Persistent Mental Illness • Kathleen Torsney (2004) found in one mental health treatment setting 13% of individuals served had a history of TBI • These same individuals had been treated in various mental health settings but not received specific brain injury treatment Homelessness & Brain Injury A little studied population, however….. • A University of Miami study found that 80% of 60 homeless individuals had high incidence of neuropsychological impairment • Researchers in Milwaukee found possible cognitive impairment in 80% of 90 homeless men evaluated. • Dr. LaVecchia of the MA Statewide Head Injury Program reported in 2006 that of 140 homeless individuals evaluated, 83.6% of males and 16.4% of females had an acquired brain injury • Other studies in the UK and Australia show similar rates of brain injury among homeless individuals In Maryland- Screening Results from the MD TBI Post Demo II Project-2005 – Summary of TBI Incidence Among all Screened at 7 public mental health agencies in Frederick and Anne Arundel counties – N=190 – 39% no reported history of TBI (78) – 58.94% of individuals with a history of TBI (112) – 35.78% of individuals with a history of a single incidence of TBI (68) – 23% of individuals with a history of 2 or more TBIs (44) TBI Screening, Adapted From: Ohio Valley Center for Brain Injury Prevention and Rehabilitation John Corrigan Ph.D Have you ever been injured following a blow to the head? • As a child? • Playing sports? • From a fall? Have you ever been hospitalized or treated in an emergency room following an injury? • Treated and released? • Evaluated by a neurologist? • Had a CAT scan, MRI or EEG done while in the emergency room? Have you ever been unconscious following an accident or injury? • Have no memory for the event? • Felt dazed or confused? • Experienced a head ache, fatigue, dizziness, or changes in vision? Have you ever been injured in a fight? • Taken a direct blow to the head • Experienced a violent shaking of the head and neck? Have you ever been injured by a spouse or family member? • • • • Pushed Punched Shaken Choked Have you ever had any major surgeries? • Heart Bypass • Transplant • Brain surgery to treat a tumor, aneurysm, stroke Illnesses? • • • • • • Toxic Shock Syndrome Meningitis Encephalitis Hydrocephalous Seizure disorder Lead poisoning Additional comments and observations of the interviewer • • • • • • • • • Any visible scars? Walks with a limp? Uses a cane or walker? Has a foot brace? Limited use of one hand? Appears to have difficulty focusing vision? Difficulty answering questions? Answers are unorganized and/or rambling Becomes easily distracted, agitated or is emotionally labile What you are looking for…..And Why • Any reported or suspected functional difficulties that are interfering with home, work or community activities • With the identification a history of brain injury, professionals can better support the individuals served and make informed referrals to brain injury specialists when appropriate Strategies to support individuals with TBI Restoration Verses Compensation Spontaneous restoration of functioning occurs most rapidly and dramatically in the first year following a brain injury. Generally speaking, the greater the time from the injury the more rehabilitation efforts will focus on compensation Environmental & Internal Aides Creative cognitive strategies will employ both kinds of aides depending on individual need Environmental, AKA Prosthetic external memory strategies and devices Changing or modifying the environment to support and/or compensate for a injury imposed deficit For Example: labeling kitchen cabinets Internal The strategy is “in your head” For Example: “I have to work the memory muscle by counting everything, like how many times I pedal when I am on a bike” Actor George Clooney discussing the use of internal memory strategies in The London Sunday Times10. 23.05 Oftentimes a strategy can transition with practice from the external to the internal For Example: Preparing remarks on paper with “pauses” written in to slow down impulsive speech can eventually segue into a internal strategy, “At the end of every 2-3 sentences, I will take a breath and check in with my listener” Strategies for Remediation and Compensation • • • • • Use of a journal/calendar Create a daily schedule “To do” lists and shopping lists Labeling items Learning to break tasks into small manageable steps • Use of a tape recorder Strategies cont.…. • Encourage use of rest and low activity periods • Work on accepting feedback or coaching from others • Work on generalizing strategies to new situations • Use of a high lighter • Alarm watch Strategies cont….. • Review schedule each day • Post signs on the wall etc. • Try to “routinize” the day as much as possible Teach a variety of strategies for individuals to incorporate into their daily routines • Safety checklist (e.g. for use of stove)reinforces attention • Checklists- “things to do before leaving the house” (turn off all the appliances?, lock all the doors?, did I take my morning medications? turn down the heat/turn off the air conditioner?, do I have money or keys?, where am I going?, how will I get there? What time should I leave? Etc.) Very good for routine tasks, reinforces memory • Place visual cues in the environment (cupboard labels, written directions, calendars, list of emergency phone numbers) reinforces memory Even for individuals with poor new learning capacity, the three R’s Review Rehearse & Repeat Can lead to mastery of tasks as they eventually enter into memory Memory Strategies Adapted from: Parente & Herman in Retraining Cognition 1996 Aspen Publishers Memory Strategies Adapted from: Parente & Herman in Retraining Cognition 1996 Aspen Publishers SOLVE Mnemonic • • • • • “S” (S)pecify the problem “O” (O)options-what are they? “L” (L)isten to advice from others “V” (V)ary the solution “E” (E)valuate the effect of the solution, did it solve the problem? Setting GOALS Executive Skills Training • “G” (G)o over your goals every day-helps memory and awareness • “O” (O)rder your goals-short and long term • “A” (A)sk yourself two questions each day: “what did I do today to achieve my goals?” and “What could I have done differently to achieve my goals” • “L” (L)ook at your goals each day. Post goals and progress on the wall, refrigerator etc. The use of Prosthetic external memory devices • Car Finder-low tech, install a longer radio antenna with a day-glow flag, high tech, Design Tech International by DAK Corp. • Electronic pill boxes • “Cheat sheet” or album of pictures of family members and other important individuals with their names By Structuring the environment, memory, organization, and attention are supported, enhancing independence, reducing frustration, and freeing up cognitive and psychological energy to tackle new challenges at home, work and community Enhance Communication • Model how to paraphrase during conversations to maximize comprehension • Instruct how to reduce injury imposed tendency to be impulsive in word and/or action by using breaks and pauses • Speak in short, simple sentences and phrases Communication…. • Request that the individual jot down notes regarding discussions that he/she has with others and other important information • When giving instructions, do it verbally and in writing and when possible, physically model the task Minimize confusion/socially unacceptable behavior • Don’t use the word inappropriate. Rather, give useful and specific feedback about a behavior • Treat the individual like an adult in context, tone and body language • Ask the individual for permission to coach him/her Behavior …. • Be clear on your expectations of the individual and his/her behavior • Give feedback immediately using the sandwich technique • Utilize positive reinforcement/feedback • Formalize your expectations by negotiating a written contract, signed by all involved parties • Refer to the contract frequently, update as needed Strategies for Supporting Individuals with Behavioral Problems Adapted from Capuco and Freeman-Woolpert’s Strategies for Supporting an Individual with ABD Environmental Triggers for Behavioral Problems • • • • Too much stimulation Rapid pacing Lack of predictability and clear structure Overwhelming physical and cognitive demands • Negative social input TIP: If you manage the environment, you can prevent many problems And always practice a “Adult to Adult” Communication Style Bill Kerrigan, Humanim Guidelines for Behavior Management • Increase rest time. Fatigue is a common problem • People have limited coping skills, reduce stress Guidelines for Behavior Management • Keep the environment simple. People with brain injuries are easily overstimulated • Decrease interruptions and distractions • Be consistent • Decrease surprises Guidelines for Behavior Management • Keep instructions simple, concrete • If the person has problems processing language, try gesturing or cueing • Write things down Guidelines for Behavior Management • Give feedback and set goals • Feedback should be direct, caring, nonjudgmental, but not subtle • Avoid criticism • Give supportive encouragement • Have a positive attitude Guidelines for Behavior Management • Be calm, cool and friendly during an incident • This can reduce agitation • Avoids reinforcing misbehavior Guidelines for Behavior Management • Redirection works. When the person is upset, agitated, aggressive, focus attention on some other topic, task, person • Provide choices Guidelines for Behavior Management • Decrease chance of failure • Keep success rate above 80% • Watch for frustration and Behavioral momentum Guidelines for Behavior Management Expect the unexpected. People with brain injuries can have great variability from day to day. Mood swings are common. People with TBI are sensitive to changes, disruptions in routine, lack of sleep, alcohol, minor illnesses, fatigue and other stressors Keep in Mind • Progress can be inconsistent and unpredictable • What works today may not work tomorrow, but may work the following day • Reduced stamina and fatigue may persist • Impairment of memory may hinder new learning • Transitions may be especially difficult The Goal is to…... • Enhance the Predictability of the Daily Routine There are limits to what can be changed-Staff can accommodate the injury related behaviors by modifying the individual’s environment, and their own interpersonal interactions with the individual Biological Limits to Behavioral Recovery Farrell & Hooper (1995) Glossary of Brain Injury Rehabilitation Specialists Speech Therapist: Speech therapists are trained in the evaluation and treatment of deficits in attention, organization, sequencing, thinking, problem solving, judgement, memory, writing and talking. They can teach and help individuals implement compensatory strategies. It is important to note that speech therapists working with individuals with brain injuries can and do address the mechanics of speech, e.g., breath control, volume and pitch, but also play a big role in addressing cognitive and functional skills. They can make visits to the home, community and workplace to help design and implement strategies. TBI Rehabilitation Specialists continued…….. Occupational Therapist: Occupational therapists address skills of daily living to enhance independence to include those skills necessary to bath, cook, and run a household. Occupational therapists address functional memory, visual perceptual and problem solving skills. Occupational therapists work to maintain flexibility of the arms and hands through exercise and custom made splints. They can make visits to the home, community and workplace to help individuals with the design and use of strategies to improve independence. Individuals With Brain Injuries May Also be Seen by the Following Rehabilitation Specialists……. • • • • • Physiatrist Neurologist Neuropsychologist Neuropsychiatrist Special Educator • Physical Therapist • Vocational Rehabilitation Counselor • Cognitive Therapist • Social Worker Resource Coordination Services provided by MHA’s Brain Injury Project in the following counties • Frederick and Washington CountiesCharlotte Wisner 301-682-6017 • Montgomery County-Catherine Rinehart Mello 301-586-0900 X159 • Baltimore and Howard CountiesLauren Dorsey 301-529-1508 Training: for professionals provided by MHA’s Brain Injury Project • • • • Overview of Brain Injury Mental Health and Brain Injury Substance Abuse and Brain Injury Traumatic Brain Injury: causes, Impact, and Implications for the Criminal Justice System • Vocational Issues and Brain Injury: How to Support Individuals with Brain Injury in the Workplace • Brain Injury: An Overview of the Problem and Supports and Strategies for Educators Resources • Brain Injury Association of America 703-2366000, www.biausa.org • Brain Injury Association of Maryland 410-4482924, www.biamd.org • Ohio Valley Center For Brain Injury Prevention and Rehabilitation, 614-293-3802, www.ohiovalley.org. • www.headinjury.com. Good resource for memory aides and tips Resources • Http://www.jan.wvu.edu/media/BrainInjury.html. The Job Accomodation Network offers useful articles about working with individuals with brain injury on the job, and simple accommodations that can be used to maximize success on the job • Http://www.neuro.pmr.vcu.edu/ National Resource Center for Traumatic Brain Injury, developed by the Medical College of Virginia and Virginia Commonwealth University. Offers useful articles that are very user friendly, and a catalogue of nicely priced resources for working with people with brain injury Resources, Voice Recorders, Watches Alarms, and Radiopaging • www.attainmentcompany.com-”StepPad” $29.00, Records up to 72 seconds for step by step directions • www.olympus-global.com-Digital and Microcassette hand help recorders • www.forgettingthepill.com- has alarm watches, pillbox organizers with timers, alarms • www.timex.com-Watch that can keep appointment schedules, phone numbers, contacts $90.00 • www.watchminder.com-Watch with reminder functions, 30 alarm settings with viewable messages, $79.50 Resources, Voice Recorders, Watches Alarms, and Radiopaging • www.dynamic-living.com-carries the Cadex Alarm watch (12 alarm settings) for $50.00, as well as low vision devices, key finders, and more • www.neuropage.nhs.uk-Radiopaging system to send reminders of things to do. Monthly fee, arranged in conjunction with treating physician if medication involved Resources • Http://www.abledata.com/, An online resource catalogue that lists different types of assistive technology available to help individuals with all types of disabilities • http://www.biausa.org/Pages/AT/, Catalogue of assistive technology for people with cognitive impairments. The devices listed have been reviewed by experts in the field of brain injury. Product information, and information about manufacturers, and more offered in this catalogue Resources…. Central Maryland TAP, access to a variety of adaptive devices, loans to consumers available Contact Susan Levi Workforce Technology Center 2301 Argonne Drive Baltimore, MD 21218 Voice: (410) 554-9213 Voice/TTY: 1 (800) 832-4827 TTY: (410) 554-9204 Fax: (443) 260-0833 EMAIL: slevi@charm.net http://www.mdtap.org/loan.html Resources The University of Alabama Traumatic Brain Injury Model System has created the UAB Home Stimulation Program. This program offers many activities for use by individuals with brain injuries, their families and the professionals who work with them. The activities are designed to help support cognitive skills and can be done in the home setting. The Home Stimulation Program can be accessed from the Internet at htt://main.uab.edu/show.asp?durki=49377. For further information contact: Research Services, Dept. of Physical Medicine and Rehabilitation, University of Alabama at Birmingham, 619 19th St. S SRC 529, Birmingham, AL 35249-7330/ 206-934-3283. Tbi@uab.edu. The Michigan Department of Community Health Web-Based Brain Injury Training for Professionals www.mitbitraining.org This free training consists of 4 module that take an estimated 30 minutes each to complete. The purpose of the training is twofold, to “ensure service providers understand the range of outcomes” following brain injury and to “improve the ability of service providers to identify and deliver appropriate services for persons with TBI” More on staff training…. As of April 2004, the Defense and Veterans Brain Injury Center at Walter Reed Army Medical Center is offering an online learning course on traumatic brain injury through the Veterans Health Initiative. For more information contact:http://www1.va.gov/vhi/docs/TBIfinal_www.pdf http://www.webaim.org/simulations/cognitive - this is a site that can be used in staff training. It is a simulation of the effects of cognitive disabilities. You will be asked to complete simple tasks, but other tasks will get in the way. http://www.biausa.org/Pages/related_articles.html - links to many online articles, written not for professionals in the field, but for people learning about brain injury. The y cover all types of topics, from substance abuse and brain injury to cognition and brain injury. Written by various experts in the brain injury field. Certified Brain Injury Specialist (CBIS) Training offered through the American Academy for the Certification of Brain Injury Specialists, www.biausa.org Acknowledgments This presentation is based on training materials developed by the staff and consultants of the Maryland TBI Projects 2003-present Thank You Anastasia Edmonston aedmonston@dhmh.state.md.us 410-402-8478