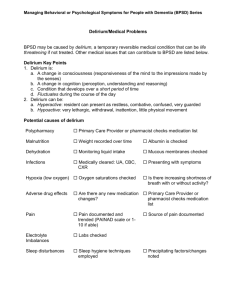
Presentation: Delirium

Delirium:
Recognition
Assessment
Prevention
Management
WRHA Surgical Program
Delirium Guidelines
Delirium
Definition:
A disturbance of consciousness with inattention that develops over a short time & fluctuates
What is Delirium?
• An acute confusional state
• Usually has a reversible cause
• Characterized by:
– Inattention
– Sudden onset
– ………………..
Why Should We Use Delirium
Guidelines ?
• Delirium can result in:
– morbidity and mortality
– length of stay
– rates of admission to long term care facilities
– 20% of patients discharged post hip # still had evidence of delirium
(Journal of American Geriatric
Society 2001 May;49(5):678-9).
Outcomes of Delirium
35%
40%
25%
Recovery Permanent Cognitive Impairment Mortality
(even with complete recovery, 30% dementia within 3 years = decreased brain reserve)
Recognition of Delirium
• Previous studies 32%-66% of cases are unrecognized by Medical Staff
Yale- New Haven study (
Inouye S. Ann Intern Med 1993: 119-
474)
– 65% unrecognized by Physicians
– 43% unrecognized by Nurses
Top 4 Independent Risk Factors for
Delirium
Vision impairment :
Any severe illness :
Cognitive impairment :
High Urea/Creatinine ratio:
Inouye S. Ann Intern Med 1993: 119-474
4 Independent Risk Factors for Nurse
Under-Recognition
• Hypoactive Delirium
• Age 80 yrs and over
• Visual Impairment
• Dementia
Types of Delirium
• Hyperactive
• Hypoactive
• Mixed
Causes of Delirium?
• Anything that hurts the brain or impairs its proper functioning can provoke a delirium!
• Brain
’ s way of demonstrating
“ acute organ dysfunction
”
Causes of Delirium:
1. Drugs
2. Infection
3. System failure/events
4. Metabolic Imbalance
5. Dehydration/Poor Nutrition
6. Surgery or general anaesthetic within the last 5 days
Causes of Delirium:
7. Pain
8. Uncorrected sensory or language impairment
9. Fecal Impaction
10. Urinary Retention/Catheter
11. Restraints
12. Sleep disruption
13. No factors can be identified
20% of the time
14. Recent severe illness or event involving hypoxia
Causes of Delirium Related to Surgery
Perioperativ e
Drugs
Anesthetics
Opioids
Benzodiazepines
Etc…
Risk Factors
Predisposing
Precipitating
Comorbidities
Diabetes
MI
Etc…
Theories for Post Op Delirium
• Acetylcholine interaction with medications used during surgery
• Increase of neurotransmitters, serotonin and dopamine during surgery
• Previous abnormality levels of melatonin
• Damage to neurons by oxidative stress or inflammation caused by a surgical procedure
• Post op abnormal brain waves
Medications Associated with
Delirium
• Any drug can potentially cause confusion
• Take a careful history of any new drug
STARTED or any old drug STOPPED recently
Medications Associated with
Delirium
• Over the counter drugs
– Cimetidine
– Cough/Cold Remedies
– Gravol/ Maxeran
– Sleeping medications
– Herbal meds
Reference List of Drugs with
Anticholinergic Effects
• Antidepressants
• Antipsychotics
• Antihistamines/
Antipruritics
• Antiparkinsonian
• Antispasmotics
• Antiemetics
• Opioids
• Anticonvulsants
• Antibiotics
• Corticosteroids
• Anticholinergics
Studies
In studies, drugs with anticholinergic side effects have been shown to:
• Lower cognitive scores in elderly subjects
• Cause/worsen severity of delirium
• Associated with more ADL decline in patients with dementia
• Associated with faster MMSE decline in patients with dementia
• If drugs reduced, be associated with improvements in dementia and delirium.
Full List of Safe Medications for the
Older Adult
Please see attachment at the end of this presentation
Assessing for Delirium
Pre-Admission Assessment
• Decision Tree
CAM – Confusion Assessment Method
–
Sensitivity (94 to 100%), specificity (90 to 95%)
Requirement for delirium = 1, 2 AND either 3 OR 4
1. Abrupt change?
2.
Inattention, can’t focus?
3. Disorganized thinking? Incoherent, rambling, illogical?
4. Altered level of consciousness? (Hyper-alert to stupor?)
AND
Trigger Questions
1. Acute change in behaviour?
2. Changes in function?
3. Changes in cognition? MMSE
4. Changes in medications?
5. Physiologically stable?
How Do We Assess for Inattention
• Recite the months backwards or days backwards
• Have the patient count backwards from
20 to 1.
• Use the CAM
Once You Identify Delirium, Now
What?
• Identify the acute medical problems that could be either triggering the delirium, or prolonging it!
• Clarify pre-morbid functional status, sequence of events and previous admission cognitive baseline
• Identify all predisposing and precipitating factors, and consider the differential
Physical Exam
– Vitals : normal range of BP, HR, Temp and pain
– Good physical exam: particular emphasis on
Cardiac, pulmonary and neurologic systems
– Hydration status
– Also rule out
• fecal impaction
• urinary retention
• Infected pressure ulcer, UTI or pneumonia
Delirium workup: Lab testing
• Basic labs most helpful !
– CBC, lytes, BUN/Cr, glucose,CO2, Ca+, Mg,
PO4
– TSH, B-12, LFTs & albumin
• Infection workup
(Urinalysis, CXR) +/blood cultures
• EKG
• O
2 sat/ABG
What About Prevention?
Yale Delirium Prevention Trial
Risk Factors
Cognitive Impairment
Intervention
Reality orientation / therapeutic activities program
Vision/Hearing impairment Vision / hearing aids / adaptive equipment
Immobilization Early mobilization / Reduce immobilizing equipment
Psychoactive medication Non pharmacologic approaches to sleep / anxiety / Restricted use of sleeping medication
Dehydration
Sleep deprivation
Early recognition / Volume expansion
Noise reduction strategies/sleep enhancement program
Ref: Inouye SK, NEJM. 1999;340:669-676
Prevention and Pre-Op Assessment
• Pre-op Clinic Form
• Pre- op- Questionnaire
What about Management?
Non Pharmacological Interventions
• Always apply non-pharmacological
interventions in your Care Plan. Examples
– Initiate toileting routines
– Mobilize ASAP
– Quiet room, soothing music
Pharmacological Interventions
• Only use medication if:
– Non-pharmacological interventions are not successful
– The patient is a danger to themselves or others
• You may see the physician order or a pharmacist suggest the following medications:
– Low dose Haloperidol or
– Low dose Risperidone or
– Low dose Olanzapine
– ** Avoid the use of benzodiazepines
Pharmacological Interventions
• It is important to remember that:
– Dosing is best given prn when agitation becomes a concern or becomes a safety issue
– Medications must be discontinued once the agitation from the delirium is resolved
Delirium Pamphlet
• This is to be given to Families so that they may better understand what their family member is going through.
• It is also recommended that it be displayed in any Pamphlet Holders for Patient and Family
Education.
• A copy of the pamphlet is found at the back of the presentation