p - UCF Psychology
advertisement

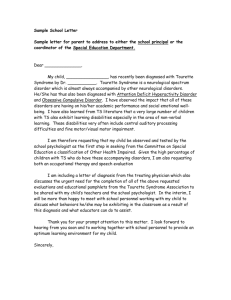
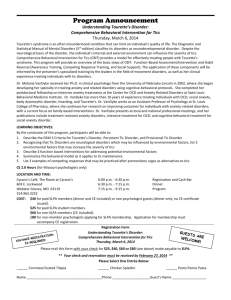
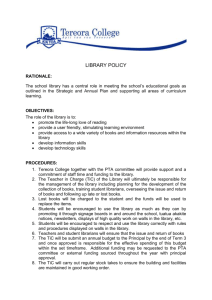
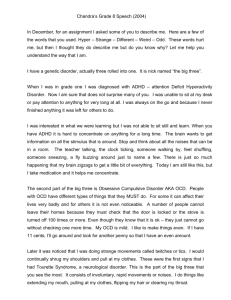
Tourette Syndrome (TS) Michael Gramlich Child Psychopathology Fall 2014 Outline DSM-5 description of Tourette syndrome Literature review Conclusion: recommended revisions to the DSM-5 Tourette Syndrome: Diagnostic Criteria Tourette Syndrome Criteria A. Multiple motor and one or more vocal tics that have been present at some time during the illness, although not necessarily concurrently. B. The tics may wax and wane in frequency but have persisted for more than 1 year since first tic onset. C. Onset is before age 18 years. D. The disturbance is not attributable to the physiological effects of a substance (e.g., cocaine) or another medical condition (e.g., Huntington’s disease, postviral encephalitis). (American Psychiatric Association, 2013) Tic Disorders DSM-5 Classification: “Neurodevelopmental Disorders” “Motor Disorders” 1. Tourette Syndrome (a.k.a. Tourette’s Disorder) 2. Persistent (Chronic) Motor or Vocal Tic Disorder Motor OR vocal tics Specify: “motor tics only” or “vocal tics only” 3. Provisional Tic Disorder Motor AND/OR vocal tics Tics < 1 year 4. Other Specified/ Unspecified Tic Disorder Specified: criteria for tic disorder not met. Ex: onset after age 18 years Unspecified: chooses not to specify reason or insufficient information (American Psychiatric Association, 2013) Clinical Manifestations Simple motor tics / simple vocal tics Short duration (i.e., milliseconds) Eye blinking, shoulder shrugging; throat clearing, grunting Complex motor tics / complex vocal tics Longer duration (i.e., seconds) Often present as a combination of simple tics Touching, squatting, jumping Words and phrases Echolalia / Palilalia Coprolalia Echopraxia Copropraxia HBO: Tourette Syndrome Clip (American Psychiatric Association, 2013) Development and Course Premonitory urge Sensation that precedes tics Unpleasant itch, tingle, or tension This urge is released following expression of the tic Vulnerability toward certain co-occurring conditions changes with the course of tic disorders Prepubertal children: ADHD, OCD, and *Separation Anxiety Disorder Teenagers & Adults: MDD, Substance Use Disorder, or Bipolar Disorder (American Psychiatric Association, 2013) Risk and Prognostic Factors Temperamental (Exacerbating/Alleviating) Factors Tics are worsened by anxiety, excitement, and exhaustion Tics are better during calm and focused activities Environmental People may incorrectly interpret a tic (e.g., repeating the last-heard word or phrase – echolalia) as purposeful Problem when interacting with authority figures (e.g., substitute teachers) Genetic Important risk alleles for Tourette syndrome Rare genetic variants in families with tic disorders have been identified Physiological Obstetrical complications (i.e., difficulties during labor or delivery) Older paternal age Lower birth weight Maternal smoking during pregnancy (American Psychiatric Association, 2013) Functional Consequences Sometimes mild to moderate symptom severity involves no distress or impairment in functioning The presence of co-occurring conditions (e.g., ADHD or OCD) can have a greater impact on functioning Tic disorders can result in social isolation, interpersonal conflict, peer victimization, inability to work or go to school, and lower quality of life Rare complications of Tourette syndrome can include: physical injury (e.g., from hitting oneself in the face) orthopedic and neurological injury (e.g., disc disease related to forceful head and neck movements) (American Psychiatric Association, 2013) Differential Diagnosis Disorder Description Primary Difference Prolonged Duration (seconds to minutes) Lack of a premonitory urge Motor Stereotypies Involuntary, rhythmic, repetitive, movements Chorea Brief, purposeless, appears “dance-like” Vocal tics are not characteristic Movements are usually worsen during attempted voluntary action Dystonia Muscles contract involuntarily, severe twisting or distorted postures Often triggered by attempts at voluntary movement s Not seen during sleep Myoclonus Unidirectional movement, nonrhytmic, occur during sleep Rapidity Lack of suppressibility Absence of premonitory urge OCD Obsessions, and/or compulsions Cognitive-based drive (e.g., fear of contamination) Perform actions a certain number of times, equally on both sides of the body (American Psychiatric Association, 2013) DSM-5 Model of Tourette Syndrome Genetic & Physiological Factors o Risk alleles o Older paternal age o Lower birth weight o Obstetrical complications o Maternal smoking during pregnancy Exacerbating Factors o Anxiety o Excitement o Exhaustion o Stressful events Alleviating Factors o Focused activities Core Features o Motor Tics & o Vocal Tics Environmental Factors o Perception by others Functional Consequences o Social isolation o Interpersonal conflict o Peer victimization o Inability to work/ go to school o Physical injury Secondary Features o Premonitory Urges o ADHD o OCD Literature Prevalence/Onset of TS Clinical Features Heritability + Genetics Comorbidity Risk Factors Brain Structures Neurotransmitters Tic Suppression Exacerbating/Alleviating Factors Quality of Life Treatment Prevalence and Onset of TS United States prevalence, ages 5 – 18 years: ~ 1% (range 0.5 – 3.8%) (Comings D., Himes, Comings B., 1990; Kurlan et al., 2001; Robertson, 2008) International prevalence, ages 5 – 18 years: ~ 1% (Robertson, 2008) Mean age at onset of tics: ~ 4 years - 6.4 years (Freeman et al., 2000; McMahon, Carter, Fredine, & Pauls, 2003) Motor tic onset ~ 4 – 6 years Vocal tic onset ~ 8 – 15 years Simple tics usually precede complex tics (Leckman, Bloch, Scahill, & King, 2006) Mean age at diagnosis of TS: 13.2 years (51.4% 6 -10 years) (Freeman et al., 2000) Children – male to female 5:1 Adults – male to female 3:1 (Freeman et al., 2000) Course of Tic Severity (Leckman et al., 1998) Temporal Nature of Tics (Figure 1. Adapted from Leckman, 2002) Coprophenomena Freeman et al. (2009) N = 597 TS patients (children, n = 506; adults, n = 91) Coprolalia: lifetime prevalence Males: 19.3% Females: 14.6% Mean onset: 5 years, 4 months after the onset of tics Copropraxia: lifetime prevalence Males: 5.9% Females: 4.9% Mean onset: 4 years, 10 months after the onset of tics Coprophenomena 18.4% of children and 28.6% of adults Coprolalia: 6.8% mildly-rated tics and 42.6% rated severe tics Heritability: First-degree Relatives TS TS = 8.7% (± 1.6%) Controls 0% CTD = 17.3% (± 2.1%) 2.7% (± 2.7%) OCD = 11.5% (± 1.9%) 2.5% (± 2.5%) TS - OCD TS + OCD TS = 9% (± 2.0%) 8.1% (± 2.6%) CTD = 17.6% (± 2.7%) 17.6% (± 3.6%) OCD = 10.4% (± 2.3%) 13.6% (± 3.6%) Note: 10.4% OCD among TS only probands was significantly greater than 2.5% among Controls Twins TS Concordance Rate: Monozygotic twins 53% vs. Dizygotic twins 8% (Price, Kidd, Cohen, Pauls, & Leckman, 1985) Hyde, Aaronson, Randolph, Rickler, and Weinberger (1992) 16 MZ twins (M = 12.8 years, SD = 1.4, range = 8 – 26 years; 75% males) At least one twin with TS Concordance rate: 56% TS and 94% tic disorder 13 MZ pairs had different birth weights 12/13: lower birth-weight twin had a higher tic severities (both: YGTSS and Shapiro Symptom Check List) Genetics Although family and twin studies have demonstrated high relative risk, researchers have difficulty mapping the genes responsible. Genome scan among affected sibling pairs (N = 1,052 participants) and multigenerational families (N =15 families). Overall, this study found strong linkage on chromosome 2p. However, this linkage was absent in some families. In addition, some families appear to have stronger associations on specific markers along chromosome 2 (e.g., DS2S319 or D2S305). (The Tourette Syndrome Association International Consortium for Genetics, 2007) Gene studies have found mixed support on candidates involved in neurotransmission. Dopamine receptor D2 (DRD2), receptor D4 (DRD4), Monoamine oxidase A (MAOA), and Serotonin receptor (5-HT2A) However, results have not been clearly replicated. (O’Rourke, Scharf, Yu, & Pauls, 2009) GWAS of Tourette Syndrome 1,285 TS cases and 4,965 ancestry-matched controls of European descent No markers achieved a genome-wide threshold of significance (other neuropsychiatric GWAS have needed at least 5,000 cases to identify common risk alleles; see Sullivan, 2010) Top signal marker rs7868992 on chromosome 9q32, gene COL27A1 (Scharf et al., 2013) Comorbidity TS alone: 10% ~ 20% among children and adults (Freeman et al., 2000; Khalifa and von Knorring 2006; Mol Debes, Hjalgrim, & Skov, 2008) OCD: 16% ~ 50% (Khalifa et al., 2006; Mol Debes et al., 2008) ADHD: 43% ~ 68% (Khalifa et al., 2006; Mol Debes et al., 2008) Both OCD & ADHD: 21.7% (Mol Debes et al., 2008) Depressive Disorder: 20% Anxiety Disorder: 18% Conduct Disorder: 8% ~ 15% Learning Disorder (i.e., dyslexia): 16% Intellectual Disability (IQ ≤ 70): 16% Sleep Disorder: 25% ~ 28% Stuttering: 8% ~ 15% (Freeman et al., 2000; Khalifa et al., 2006; Mol Debes et al., 2008) Comorbid ADHD: Functioning Carter et al. (2000) TS + ADHD (n = 33; M = 11.10 years; SD = 1.56; males = 76%) TS alone (n = 16; M = 10.40 years; SD = 1.41; males = 56%) Controls (n = 23; M = 10.80 years; SD = 1.77; males = 48%) No significant differences in OCD and OC symptoms between TS + ADHD and TS alone Measures Kaufman Brief Intelligence Test CBCL Vineland Adaptive Behavior Scales – Survey Form Children’s Depression Inventory (CDI): child-rated Self-Perception Profile for Children Family Environment Scale (FES) Dyadic Adjustment Scale (DAS) 20-Item Leyton Survey YGTSS CY-BOCS Continuous Performance Test (CPT) Results (Carter et al., 2000) Comorbid OCD Tic-related OCD has a higher rate among males, an earlier age of onset, poorer treatment responses to SSRI medication, and higher heritability among firstdegree relatives. (Cohen, Leckman, & Bloch, 2013) (Bloch et al., 2006a) Comorbid Sleep Disorders Ghosh et al. (2014) 123 TS children (13.6 years, SD = 3.8) Clinical interview with TS child and guardian TS-only group: 31 of the 48 (65%) had DSM-V coded sleep disorder 10 of the 31 (32%) had primary insomnia disorder Represents a 2.5–fold increase in comparison to the general pediatric population ~ 20% of the entire TS-only sample 0% had insomnia secondary to medication TS + ADHD group: 48 of the 75 (64%) had DSM-V coded sleep disorder 20 of the 48 (42%) had primary insomnia disorder 16 of 48 (33%) had insomnia secondary to medication (e.g., extensive use of stimulant medications) Prenatal Risk Factors Chao, Hu, and Pringsheim (2014) Systematic review on 21 studies Most data were ascertained retrospectively 5 studies collected data prospectively Results No significant association for demographic factors of parents (i.e., age, education, SES, and marital status) with onset of TS, symptom severity, or comorbidity. Most consistently reported factors were maternal smoking during pregnancy and low birth weight. Maternal smoking was associated with TS onset and comorbid ADHD and OCD, and symptom severity of ADHD and OCD. Low birth weight: comorbid ADHD and tic severity Note: Although these factors are related to tics, they do not necessarily cause tics. PANDAS Theory Pediatric Autoimmune Neuropsychiatric Disorder Associated with Streptococcus (PANDAS) Infection: Group A beta hemolytic streptococci (GABHS) Patients may develop tics in reaction to recurrent strep infections Mell, Davis, and Owens (2005) Examined the rates of streptococcus infection among children (N = 144) prior to OCD, Tourette’s Syndrome (TS), or tic disorder diagnosis. Children with OCD, TS, or tic disorder were more likely than controls to have a streptococcus infection 3 months before date onset. The highest risk was multiple streptococcus infections within 12 months of diagnosis (OR: 3.10; 95% CI: 1.77, 8.96). Published reports linking GABHS with pediatric neuropsychiatric symptoms: onset of OCD/tics symptoms, hyperactivity, and even disrupted handwriting (Murphy, Kurlan, & Leckman, 2010). However, these studies are mostly retrospective. PANDAS Pathogenesis Model: Frequent GABHS infections anti-GABHS antibodies crossing blood-brain barrier dopamine release inflammation within basal ganglia OCD, tics and other neuropsychiatric symptoms (Murphy et al., 2010) Cluster Analysis of Tic Symptoms and Tx Outcome McGuire et al. (2013) 142 youths (M = 12.45 years; SD = 2.83); 97 Adults (M = 35.17 years; SD = 13.09) TS (n = 212), Chronic Tic Disorder – motor (n = 25) – vocal (n = 2) Woods et al., 2008; Piacentini et al., 2010; Wilhelm et al., 2012 Cognitive Behavioral Intervention for Tics (CBIT) Yale Global Tic Severity Scale (YGTSS): clinician-rated instrument Checklist of 40 possible tic symptoms Tics during the past week: 1. 2. 3. 4. 5. Number (0-5) Frequency (0-5) Intensity (0-5) Complexity (0-5) Interference (0-5) Total Motor Tic (0-25) severity Total Phonic Tic (0-25) severity Total Tic score (0-50) severity YGTSS Impairment scale (0-50) Clinical correlates No significant differences in cluster membership across various TS/OCD/ADHD profiles [Cluster 1: F (3, 235) = 1.36, p = 0.26; Cluster 2: F (3, 235) = 2.06, p = 0.11; Cluster 3: F (3, 235) = 0.70, p = 0.55; Cluster 4: F (3, 235) = 1.54, p = 0.21]. Treatment Responses Cluster membership did not predict treatment response [Cluster 1: OR = 0.95, 95 % CI = 0.64 – 1.41; Cluster 2: OR = 1.18, 95% CI = 0.81 – 1.72; Cluster 3: OR = 0.97, 95% CI = 0.65 – 1.46; Cluster 4: OR = 1.26, 95% CI = 0.85 – 1.86] Cluster membership did not predict reductions in total tic severity [F (4, 115) = 0.47, p = 0.77, R2 = .02] or individual motor tic severity [F (4, 115) = 0.47, p = .77, R2 = .02] or phonic tic severity [F (4, 115) = 1.64, p = .17, R2 = .05]. Review TS Characteristics: mean age of onset between 4 – 6 years, tic severity peaks ~ 10 years, and the frequency is sporadic. Motor tic onset typically precedes vocal tics and simple tics commonly start before complex tics. Males have a higher rate of prevalence. Coprophenomena only occurs in about 1 in 5 TS patients Heritability: having a first-degree relative with TS significantly increases the risk of having TS, CTD, and/or OCD. In addition, rates of TS and tic disorder were significantly higher for monozygotic twins (~ 50% and 94%) in comparison to dizygotic twins. Genetics: genetic linkage studies, candidate genes, and GWAS have suggested some genes that are responsible. However, these findings are limited and need replication. Perinatal Risk Factors and PANDAS: the most consistent findings point to low birth weight and maternal smoking during pregnancy as correlates with TS and tic severity. However, these do not imply causation, only association. Furthermore, PANDAS has shown evidence, but this is only among a small group of tic disorder patients. Comorbidity: ~ 10% - 20% have TS alone. High rates of co-occurring ADHD, OCD, and sleep disorders. Furthermore, comorbid ADHD significantly increases problems with behavior. Four-cluster tic symptoms: no differences among TS/ADHD/OCD profiles. Cluster membership did not predict treatment response to CBIT and did not predict reduction in tic severity (total, motor, or vocal). Literature Prevalence/Onset of TS Clinical Features Heritability + Genetics Comorbidity Risk Factors Brain Structures Neurotransmitters Tic Suppression Exacerbating/Alleviating Factors Quality of Life Treatment Fine-motor Skills Bloch, Sukhodolsky, Leckman, and Schultz (2006b) 32 TS children (M = 11.4 years, SD = 1.5) and 9 age-matched controls Follow-up clinical assessment at an average of 7.4 years later Time 1 OCD and Tic severity Neuropsychological Tests: Kaufman Brief Intelligence Test: short form intelligence Beery-Buktenica Visual Motor Integration Test (VMI): visual motor integration Rey-Osterreith Complex Figure Task (RCFT): visual memory Purdue Pegboard: fine motor skill Time 2 OCD and Tic severity Results: Purdue Pegboard ‘Dominant’ (p = .012, R2 = .19), ‘non-dominant’ (p = .003, R2 = .26), and ‘bimanual’ (p = .045, R2 = .13) were positively correlated with current tic severity at Time 1. Poor performances on the ‘dominant’ predicted worse tic severity at Time 2 (OR = .59, p = .04, R2 = .13). Structural Imaging: Basal Ganglia Peterson et al. (2003) Functional magnetic resonance imaging (fMRI) examining 154 TS and 130 control participants (18.7 years ± 13.4 vs. 21.0 years ± 13.5; p = .14) 173 (60.9%) were children 111 (39.1%) were adults 33.1% had TS + OCD 26.6% had TS + ADHD Results TS vs. Controls Significantly smaller basal ganglia volumes for TS participants than controls (p = .04) TS x Region (p < .001) Relatively greater reductions in the caudate (p = .009) than in the putamen (p = .16), and globus pallidus (p = .31) relative to controls Children Only Smaller volumes in the caudate (p = .06) than in the globus pallidus (p = .09), and the putamen (p = .30) in comparison to controls Adults Only Smaller volumes in the caudate (p = .04), globus pallidus (p = .13), and the putamen (p = .11) in comparison to controls (Peterson et al., 2003) Structural Imaging: Basal Ganglia Bloch, Leckman, Zhu, and Peterson (2005) Prospective, longitudinal study assessing 43 TS patients at baseline and follow-up Baseline Average age = 11.4 years, range = 8.5 – 13.9, SD = 1.6 Yale Global Tic Severity Scale (YGTSS) Children’s Yale-Brown Obsessive-Compulsive Scale (CY-BOCS) [35% OCD] Kaufman Brief Intelligence Test fMRI Follow-up Average age = 18.7 years, range = 16-23 years, SD = 1.7 YGTSS CY-BOCS Global Assessment Scale Results TIME 1: Tic and OCD Severity at time of Childhood MRI No association between caudate volume and Tic severity (p = .08) or OCD severity (p = 0.59) TIME 2: Tic and OCD Severity at time of Early Adulthood follow-up Volumes of caudate correlated inversely with Tic severity Total Caudate (χ2 = 11.3, p = .0008) Left Caudate (χ2 = 13.2, p = .0003) Right Caudate (χ2 = 8.8, p = .003) Volumes of caudate correlated inversely with OCD severity Total Caudate (χ2 = 6.9, p = .009) Left Caudate (χ2 = 7.2, p = .007) Right Caudate (χ2 = 6.3, p = .012) The putamen and the globus pallidus were not correlated with Tic or OCD severity (Bloch et al., 2005) Functional Imaging: Tic Suppression Peterson et al. (1998) 22 TS adults without significant head tics and who could voluntarily suppress their tics. 11 men and 11 women (these groups did not differ significantly in tic severity). Compared functional images during tic suppression and free expression of tics. 40-second sessions of “suppression” and “free expression” of tics within the scanner. Results BOLD Signal Changes “Free” Motor Tics “Suppression” Events and Severity of Right Caudate Nucleus (r = - .46, p < .02) Putamen Right (r = - .54, p < .009) Globus Pallidus Left (r = - .47, p < .03) Right (r = - .52, p < .03) Thalamus Left (r = - .44, p < .02) Right (r = - .41, p < .02) Left Sensorimotor Cortex (r = - .36, p < .05) Left Inferior Parietal (r = - .43, p < .02) Key Finding: TS participants whose signal change exhibited reduced activation between events, had more severe symptoms. (Peterson et al., 1998) Structural Imaging: Sensorimotor Cortices Sowell et al. (2008) The average cortex in the TS group was 0.45 mm thinner than the controls. Age-by-diagnosis interaction where cortices thickened with increasing age in control children, but not in those with TS. Supplemental Motor Area (SMA) Hampson, Tokoglu, King, Constable, & Leckman (2009) Neurotransmitters GABAergic neurons and Cholinergic neurons (a.k.a., acetylcholine) Individuals with TS showed a reduction in up to 60% of the GABAergic and cholinergic interneurons in the caudate nucleus and putamen. In addition, the GABAergic neurons were markedly decreased in the external segment of the globus pallidus (GPe), while significantly increased in the globus pallidus interna (GPi). (Kalanithi et al., 2005; Kataoka et al., 2010) Dopaminergic Systems Dopamine (D2) receptor antagonist pharmaceuticals such as haloperidol have been found to be successful at suppressing tics temporarily. (Scahill et al., 2006) Tetrabenazine (TBZ) acts as an inhibitor of dopamine (D2) and other monoamines (norepinephrine and serotonin) and has demonstrated tic suppression. Also has showed little to no reports of TBZ-induced tardive dyskinesia. (Kenney, Hunter, & Jankovic, 2007) Increases in tics following exposure to increased dopaminergic activity in the central nervous system (CNS) such as L-dopa (Anderson, Leckman, & Cohen, 1998. As cited in Leckman, Bloch, Smith, Larabi, & Hampso, 2010) Neurotransmitters Noradrenergic System Alpha-2 adrenergic agonists such as clonidine, have reported to reduce tic severity Clonidine’s primary action is inhibition of norepinephrine (results in reduced dopamine in the striatum). Fewer side effects and long term risk potential in comparison to traditional dopamine antagonists (Bloch, Panza, Landeros-Weisenberger, & Leckman, 2009) Adult TS patients have showed elevated levels of cerebrospinal fluid (CSF) norepinephrine and higher levels of norepinephrine in their urine in response to lumbar puncture stress relative to healthy controls (Chappell et al., 1994; Leckman et al., 1995; As cited in Leckman et al., 2010) Serotonergic System Although serotonin reuptake inhibitors (SRIs) are effective in treating OCD, SRIs are less effective in treating tics and tic-related OCD. (March et al., 2007; Scahill et al., 2006) Inconsistencies in the literature regarding abnormalities of serotonin between TS alone subjects and healthy controls (Leckman et al., 2010) Literature Prevalence/Onset of TS Clinical Features Heritability + Genetics Comorbidity Risk Factors Brain Structures Neurotransmitters Tic Suppression Exacerbating/Alleviating Factors Quality of Life Treatment Tic Suppression: Verbal Instructions and Reinforcement Woods and Himle (2004) N = 4 (3 boys, 1 girl) Token dispenser (“Tic detector”) Remote controlled operant token dispenser. BL condition: Tic freely VI condition: Verbal instructions not to tic DRO condition: Verbal instructions not to tic Told every10-secs of tic-free intervals, token would be awarded. Results Adding reinforcement to verbal instructions reduced tics by 76% Consequences can affect tic expression BL: Baseline VI: Verbal Instruction DRO: Reinforced Suppression “Tic Detector” Premonitory Urges… Negative Reinforcement? Situational Antecedents Premonitory Urge (unpleasant) Expression of TIC Termination of URGE Figure by Piacentini J., “New Thoughts on Behavioral Treatment of Tourette Syndrome.” February, 2006 Tic Suppression and Premonitory Urge Himle et al. (2007) 5 TS children (ages 8, 10, 13, 14, and 17) Inclusion: presence of premonitory urges, tic rate at least 1/min, and no previous behavioral treatment for tic suppression Measures Anxiety Disorders Interview Schedule-4th Edition (ADIS-IV) Child Behavior Checklist (CBCL) Yale Global Tic Severity Scale (YGTSS) Premonitory Urge for Tics Scale (PUTS) Direct-observation Materials “Tic Detector” (established by Woods et al., 2004). Laptop computer displayed a 9-point “urge thermometer” every 30s Design (ABAB withdrawal) – 5-minute conditions Baseline: “feel free to tic” Suppression: earn a token for each 10s tic-free intervals. Interval resets if tic occurs. Results 10 Year Old Female 14 Year Old Male 17 Year Old Male 4/5 children displayed a clear and reliable suppression effect 3/4 children reported more intense premonitory urges during suppression (DRO) in comparison to BL conditions. The older children (e.g., Randy) had a greater ability to suppress the tics. (Himle et al., 2007) Development of Premonitory Urge Woods et al. (2005) Premonitory Urge for Tics Scale (PUTS): 9-item self-report 42 TS children (8 to 16 years old) Young: 8 – 10 years old vs. Old: 11 – 16 years old PUTS Scores: Young vs. Old Total PUTS scores (M = 18.5 ± 6.5 vs. M = 18.6 ± 7.3, p = ns) Frequency of urges (items 7 and 8, p = ns) PUTS Consistency Internal consistency: Young vs. Old (α = 0.57 vs. α = 0.89) CONCLUSION: Researchers suggested the sensations are present and temporally stable in Young and Old youths, but Old youths can reliable notice and describe it. Literature Prevalence/Onset of TS Clinical Features Heritability + Genetics Comorbidity Risk Factors Brain Structures Neurotransmitters Tic Suppression Exacerbating/Alleviating Factors Quality of Life Treatment Antecedents Tics Consequences Happen immediately before tics and make them more or less likely to occur Events after tics that make the frequency or intensity of tics more or less likely to happen Internal (e.g., premonitory urges, anxiety, or boredom) Internal (e.g., embarrassment, or relief from premonitory urge) External (e.g., sports, the presence of other people, or being home from school) External (e.g., attention from family or peers, escape from activities) Contextual Factors Conelea and Woods (2008a) (Table 6 adapted from Cohen et al., 2013) Reinforcement and Context Woods, Walther, Bauer, Kemp, and Conelea (2009) 10 children with TS (n = 9) or Chronic Tic Disorder (n = 1) Mean age of 10.8 years (9-15 years old) 4 Training sessions, consisting of 3 conditions 1. Purple light (verbal instructions to suppress, reinforced suppression) 2. Orange light (verbal instructions to suppress, no reinforced suppression) 3. No light (baseline, verbal instructions to tic freely) Each 5-min condition replicated 3 times in random order during each training session 5th session was a test of acquisition Verbal instructions to suppress (or not suppress) were not provided Purple light, orange, no light condition presented 3 times No reinforcers delivered * (Reinforcement via “Tic Detector” protocol utilized by Woods et al., 2004). Results TRAINING PHASE Mean Tics Per Minute (TPM): BL > SUP-Purple (p = .002, d = 1.10) 63.6% reduction in TPM was found during the training phase for SUP-Purple Mean Tics Per Minute (TPM): Training Phase SUP-No Reinforcement-Orange > SUP-Purple (p = .03, d = 0.47) TEST – 5th Session TPM: BL-Test condition > Test-Purple (p = .003, d = 0.66) Key Finding: Situation where previous reinforcement took place can be learned and applied to later tic expressions Impact of Attention on Tics Conelea and Woods (2008b) 9 TS children (M = 11.5 years, range = 9 – 15) ADHD 4/9 (ADIS-IV ratings; 6, 4, 4, 4) Followed protocol performed by Woods et al., 2004 (e.g., token dispenser and one-way mirror observation). Continuous Performance Test Audio presentation of letters (200 single-letter trials) ‘A-L’ sequence was the target among 10 non-target letters Completed CPT at pre- and post-experiment and SUP + DIS conditions Conditions 1. 2. 3. Baseline (BL): tic freely, told tic detector was on but would not dispense tokens Suppression (SUP): reinforced via tokens Suppression and Distraction (SUP + DIS): reinforced via tokens + complete auditory CPT Results Suppression findings Tic frequencies BL > SUP (p = .02, d = 1.34) and SUP + DIS (p = .03, d = 1.29) Tic frequencies between SUP (a.k.a. DRO) and SUP + DIS did not differ CPT accuracy findings Pre and post scores did not differ so they were combined Hits: SUP + DIS < Pre/Post (p = .04, d = .77) Errors: did not differ between Pre/Post and SUP + DIS (Conelea et al., 2008) Impact of Stress on Tic Frequencies Conelea, Woods, and Brandt (2011) 8 TS and 2 Persistent (Chronic) Tic Disorder (ages 9-17 years) Followed protocol performed by Himle et al., 2007 (e.g., token dispenser, “urge thermometer”) STRESS Task Timed mental math task 4 sets that increased in difficulty (e.g., “9 – 3 – 2” to “7y – 10 = 18”). Conditions 1. 2. 3. 4. Baseline (BL) Reinforced Suppression (SUP) Reinforced Suppression plus Stress Induction (SUP + STRESS) Stress Induction (Stress) - Each condition was 5 minutes, each condition was performed twice Results Mean Tics Per Minute SUP < BL (p = .01, r = -.69) BL = STRESS (p = .79) SUP + STRESS > SUP (p = .01, r = -.69) Stress Rating STRESS > BL (p = .03, r = .57) SUP < SUP + STRESS (p = .03, r = .57) Urge Rating (Try to ignore data – collected every 5-mins previous study Himle et al., 2007 was 30-secs) Key finding: stress might disrupt suppression, not increase tics overall (Conelea et al., 2011) Literature Prevalence/Onset of TS Clinical Features Heritability + Genetics Comorbidity Risk Factors Brain Structures Neurotransmitters Tic Suppression Exacerbating/Alleviating Factors Quality of Life Treatment Peer Relationships Stokes, Bawden, Camfield, Backman, & Dooley (1991) Evaluated 29 TS youngsters (M = 11.4 years) TS participants completed self-esteem scales and neuropsychological testing Teachers and parents completed behavior rating scales (i.e., CBCL) Classmates completed the Pupil Evaluation Inventory (PEI) Provides measures of aggression, withdrawal, and likeability Classmates served as the control group Peer Relationships Rated as more withdrawn (p < .02) by their classmates Rated as less popular (p < .005) by their classmates 35% of TS sample received the lowest rating in the class on 1 or more PEI factors Teachers rated TS children as more aggressive (p < .025) and more withdrawn (p < .005) Comorbid ADHD diagnosis were rated as more aggressive by their classmates than TS children without ADHD (p < .02) Note: these social problems were not predicted by the frequency or duration of tics. Social Functioning Champion, Fulton, and Shady (1988) 210 TS participants (ages 3-60+; 70% were school-aged children) Survey examining type and frequency of tics, degree and nature of sleep disorders, the degree and nature of associated behavior problems, the TS individual’s perceived level of psychosocial functioning, and perceived level of support from others. 42% of respondents reported problems in forming and maintaining friendships. ~ 50% reported problems with dating as a result to having TS. Family members, including spouses when applicable, and physicians were rated as most supportive. Teachers who were educated about TS were found to be more supportive than teachers who lacked knowledge about TS. Literature Prevalence/Onset of TS Clinical Features Heritability + Genetics Comorbidity Risk Factors Brain Structures Neurotransmitters Tic Suppression Exacerbating/Alleviating Factors Quality of Life Treatment Habit Reversal Training (HRT) Arzin and Nunn (1973) Introduced “Habit-Reversal” treatment Treated 12 individuals with habits or tics 90% symptom reduction after 1 session 99% symptom reduction at 3 month follow-up 1. Awareness Training Detect pre-tic warning signs (e.g., premonitory urges) 2. Competing Response Training Blocks tics and sustainable Ex: crossing arms so that a certain motor tic cannot take place or breathing a certain way that is incompatible with a vocal tic Perform CRT for 1-3 minutes following temptation to perform tic 3. Motivational and/or Ancillary Techniques – includes social support and behavioral reward system Ex: praise from family, friends, or teachers for successful effort Comprehensive Behavioral Intervention for Tics (CBIT) 1. Psychoeducation 2. Habit Reversal Training 3. Functional Intervention 4. Reward System 5. Relaxation Training CBIT Study Piacentini et al. (2010) 126 TS or CTD children (age range: 9 -17 years) studied at 3 sites (UCLA, Johns Hopkins University, and U. of Wisconsin – Milwaukee) Study Treatments 1. CBIT 2. Psychoeducation/Supportive Therapy – Therapists were prohibited from providing direct instructions about tic management. At 10 weeks evaluation + positive responders continued treatment to 3 months At 3 months evaluation + treatment sessions discontinued At 6 months follow-up evaluation Primary Outcome Measures YGTSS - Total Tic Score [0-50] YGTSS - Impairment [0-50] Clinical Global Impressions (CGI) - Improvement Scale [1-8]: determined by clinician Results 10 Weeks YGTSS Total Tic Score CBIT > PST reduction in tics (p < .001, d = .68) 10 Weeks CGI Improvement (Very Much Improved “1” or Much Improved “2”) CBIT > PST positive treatment response (52.5% vs. 18.5%, p < .001) CBIT = 32/61 participants PST = 12/65 participants 10 Weeks YGTSS Impairment CBIT > PST reduction in impairment from tics (51% vs. 30%, p < .01, d = 0.57) Continued “Positive Responders” Evaluated at 3 months CBIT: 24/28 (85.7%) PST: 11/12 (91.7%) Continued “Positive Responders” Evaluated at 6 months CBIT: 20/23 (86.9%) PST: 6/8 (75.0%) Available Treatments CBIT RCT: YGTSS - ES = 0.57 – 0.68 (Piacentini et al., 2010) Dopamine Antagonists: ES = 0.58 Averse effects: sedation, cognitive dulling, weight gain, and metabolic problems No significant differences on the efficacy of 4 antipsychotics tested (haloperidol, pimozide, risperidone and ziprasidone) Alpha-2 agonists: ES = 0.31 (ES = 0.68 w/ADHD; ES = 0.15 w/o ADHD) Averse effects: sedation and low blood pressure (Weisman, Qureshi, Leckman, Scahill, & Bloch, 2013) DSM-5 Model of Tourette Syndrome Genetic & Physiological Factors o Risk alleles o Older paternal age o Lower birth weight o Obstetrical complications o Maternal smoking during pregnancy Exacerbating Factors o Anxiety o Excitement o Exhaustion o Stressful events Alleviating Factors o Focused activities Core Features o Motor Tics & o Vocal Tics Environmental Factors o Perception by others Functional Consequences o Social isolation o Interpersonal conflict o Peer victimization o Inability to work/ go to school o Physical injury Secondary Features o Premonitory Urges o ADHD o OCD New Model of Tourette Syndrome Genetic & Physiological Factors o Risk alleles o Lower birth weight o Maternal smoking during pregnancy o PANDAS Exacerbating Factors o Anxiety o Excitement o Exhaustion o Stressful events Alleviating Factors o Focused activities Complex Phonic Impulse Control Complex Motor o GABA o DA o NE Core Features o Motor Tics & o Vocal Tics o Cortico-striatalthalamic-circuit o Sensorimotor cortex Premonitory Urges Antipsychotics CBIT Simple Head Motor/ Vocal Simple Motor Functional Consequences o Social isolation (e.g., dating) o Interpersonal conflict o Peer victimization o Inability to work/ go to school o Physical injury o Perception by others Sleep Disorders OCD ADHD α-2 agonists o Attention o Aggression References Azrin, N. H., & Nunn, R. G. (1973). Habit-reversal: a method of eliminating nervous habits and tics. Behav Res Ther, 11(4), 619-628. Bloch, M. H., Leckman, J. F., Zhu, H., & Peterson, B. S. (2005). Caudate volumes in childhood predict symptom severity in adults with Tourette syndrome. Neurology, 65(8), 1253-1258. doi: 10.1212/01.wnl.0000180957.98702.69 Bloch, M. H., Panza, K. E., Landeros-Weisenberger, A., & Leckman, J. F. (2009). Meta-analysis: treatment of attentiondeficit/hyperactivity disorder in children with comorbid tic disorders. J Am Acad Child Adolesc Psychiatry, 48(9), 884-893. doi: 10.1097/CHI.0b013e3181b26e9f Bloch, M. H., Peterson, B. S., Scahill, L., Otka, J., Katsovich, L., Zhang, H., & Leckman, J. F. (2006a). Adulthood outcome of tic and obsessive-compulsive symptom severity in children with Tourette syndrome. Arch Pediatr Adolesc Med, 160(1), 65-69. doi: 10.1001/archpedi.160.1.65 Bloch, M. H., Sukhodolsky, D. G., Leckman, J. F., & Schultz, R. T. (2006b). Fine-motor skill deficits in childhood predict adulthood tic severity and global psychosocial functioning in Tourette's syndrome. J Child Psychol Psychiatry, 47(6), 551-559. doi: 10.1111/j.1469-7610.2005.01561.x Carter, A. S., O'Donnell, D. A., Schultz, R. T., Scahill, L., Leckman, J. F., & Pauls, D. L. (2000). Social and emotional adjustment in children affected with Gilles de la Tourette's syndrome: associations with ADHD and family functioning. Attention Deficit Hyperactivity Disorder. J Child Psychol Psychiatry, 41(2), 215-223. Champion, L. M., Fulton, W. A., & Shady, G. A. (1988). Tourette syndrome and social functioning in a Canadian population. Neurosci Biobehav Rev, 12(3-4), 255-257. Chao, T. K., Hu, J., & Pringsheim, T. (2014). Prenatal risk factors for Tourette Syndrome: a systematic review. BMC Pregnancy Childbirth, 14, 53. doi: 10.1186/1471-2393-14-53 Cohen, S. C., Leckman, J. F., & Bloch, M. H. (2013). Clinical assessment of Tourette syndrome and tic disorders. Neurosci Biobehav Rev, 37(6), 997-1007. doi: 10.1016/j.neubiorev.2012.11.013 Comings, D. E., Himes, J. A., & Comings, B. G. (1990). An epidemiologic study of Tourette's syndrome in a single school district. J Clin Psychiatry, 51(11), 463-469. Conelea, C. A., & Woods, D. W. (2008a). The influence of contextual factors on tic expression in Tourette's syndrome: a review. J Psychosom Res, 65(5), 487-496. doi: 10.1016/j.jpsychores.2008.04.010 Conelea, C. A., & Woods, D. W. (2008b). Examining the impact of distraction on tic suppression in children and adolescents with Tourette syndrome. Behav Res Ther, 46(11), 1193-1200. doi: 10.1016/j.brat.2008.07.005 Conelea, C. A., Woods, D. W., & Brandt, B. C. (2011). The impact of a stress induction task on tic frequencies in youth with Tourette Syndrome. Behav Res Ther, 49(8), 492-497. doi: 10.1016/j.brat.2011.05.006 Freeman, R. D., Fast, D. K., Burd, L., Kerbeshian, J., Robertson, M. M., & Sandor, P. (2000). An international perspective on Tourette syndrome: selected findings from 3,500 individuals in 22 countries. Dev Med Child Neurol, 42(7), 436-447. Freeman, R. D., Zinner, S. H., Muller-Vahl, K. R., Fast, D. K., Burd, L. J., Kano, Y., . . . Berlin, C. M., Jr. (2009). Coprophenomena in Tourette syndrome. Dev Med Child Neurol, 51(3), 218-227. doi: 10.1111/j.1469-8749.2008.03135.x References Ghosh, D., Rajan, P. V., Das, D., Datta, P., Rothner, A. D., & Erenberg, G. (2014). Sleep disorders in children with Tourette syndrome. Pediatric Neurology, 51(1), 31-35. doi: 10.1016/j.pediatrneurol.2014.03.017 Hampson, M., Tokoglu, F., King, R. A., Constable, R. T., & Leckman, J. F. (2009) Brain areas coactivating with motor cortex during chronic motor tics and intentional movements. Biological Psychiatry, 65, 594-599. Himle, M. B., Woods, D. W., Conelea, C. A., Bauer, C. C., & Rice, K. A. (2007). Investigating the effects of tic suppression on premonitory urge ratings in children and adolescents with Tourette's syndrome. Behav Res Ther, 45(12), 2964-2976. doi: 10.1016/j.brat.2007.08.007 Hyde, T. M., Aaronson, B. A., Randolph, C., Rickler, K. C., & Weinberger, D. R. (1992). Relationship of Birth-Weight to the PhenotypicExpression of Gilles-De-La-Tourettes Syndrome in Monozygotic Twins. Neurology, 42(3), 652-658. Kalanithi, P. S., Zheng, W., Kataoka, Y., DiFiglia, M., Grantz, H., Saper, C. B., . . . Vaccarino, F. M. (2005). Altered parvalbumin-positive neuron distribution in basal ganglia of individuals with Tourette syndrome. Proc Natl Acad Sci U S A, 102(37), 13307-13312. doi: 10.1073/pnas.0502624102 Kataoka, Y., Kalanithi, P. S., Grantz, H., Schwartz, M. L., Saper, C., Leckman, J. F., & Vaccarino, F. M. (2010). Decreased number of parvalbumin and cholinergic interneurons in the striatum of individuals with Tourette syndrome. J Comp Neurol, 518(3), 277291. doi: 10.1002/cne.22206 Kenney, C., Hunter, C., & Jankovic, J. (2007). Long-term tolerability of tetrabenazine in the treatment of hyperkinetic movement disorders. Movement Disorders, 22(2), 193-197. doi: Doi 10.1002/Mds.21222 Khalifa, N., & von Knorring, A. L. (2006). Psychopathology in a Swedish population of school children with tic disorders. J Am Acad Child Adolesc Psychiatry, 45(11), 1346-1353. doi: 10.1097/01.chi.0000251210.98749.83 Kurlan, R., McDermott, M. P., Deeley, C., Como, P. G., Brower, C., Eapen, S., . . . Miller, B. (2001). Prevalence of tics in schoolchildren and association with placement in special education. Neurology, 57(8), 1383-1388. Leckman, J. F. (2002). Tourette's syndrome. Lancet, 360(9345), 1577-1586. doi: 10.1016/S0140-6736(02)11526-1 Leckman, J. F., Bloch, M. H., Scahill, L., & King, R. A. (2006). Tourette syndrome: the self under siege. J Child Neurol, 21(8), 642-649. Leckman, J. F., Bloch, M. H., Smith, M. E., Larabi, D., & Hampson, M. (2010). Neurobiological Substrates of Tourette's Disorder. Journal of Child and Adolescent Psychopharmacology, 20(4), 237-247. doi: 10.1089/cap.2009.0118 Leckman, J. F., Walker, D. E., & Cohen, D. J. (1993). Premonitory urges in Tourette's syndrome. Am J Psychiatry, 150(1), 98-102. doi: 10.1176/ajp.150.1.98 Leckman, J. F., Zhang, H., Vitale, A., Lahnin, F., Lynch, K., Bondi, C., . . . Peterson, B. S. (1998). Course of tic severity in Tourette syndrome: the first two decades. Pediatrics, 102(1 Pt 1), 14-19. Lin, H., Katsovich, L., Ghebremichael, M., Findley, D. B., Grantz, H., Lombroso, P. J., . . . Leckman, J. F. (2007). Psychosocial stress predicts future symptom severities in children and adolescents with Tourette syndrome and/or obsessive-compulsive disorder. J Child Psychol Psychiatry, 48(2), 157-166. doi: 10.1111/j.1469-7610.2006.01687.x References Lin, H., Yeh, C. B., Peterson, B. S., Schahill, L., Grantz, H., Findley, D. B., Katsovich, L., Otka, J., Lombroso, P. J., King, R. A., & Leckman, J. F. (2002). Assessment of symptom exacerbations in a longitudinal study of children with Tourette’s syndrome or obsessive compulsive disorder. The American Academy of Child and Adolescent Psychiatry, 41(9), 1070-1077. March, J. S., Franklin, M. E., Leonard, H., Garcia, A., Moore, P., Freeman, J., & Foa, E. (2007). Tics moderate treatment outcome with sertraline but not cognitive-behavior therapy in pediatric obsessive-compulsive disorder. Biol Psychiatry, 61(3), 344-347. doi: 10.1016/j.biopsych.2006.09.035 McGuire, J. F., Nyirabahizi, E., Kircanski, K., Piacentini, J., Peterson, A. L., Woods, D. W., . . . Scahill, L. (2013). A cluster analysis of tic symptoms in children and adults with Tourette syndrome: clinical correlates and treatment outcome. Psychiatry Res, 210(3), 1198-1204. doi: 10.1016/j.psychres.2013.09.021 McMahon, W. M., Carter, A. S., Fredine, N., & Pauls, D. L. (2003). Children at familial risk for Tourette's disorder: Child and parent diagnoses. American Journal of Medical Genetics Part B-Neuropsychiatric Genetics, 121B(1), 105-111. doi: 10.1002/Ajmg.B.20065 Mell, L. K., Davis, R. L., & Owens, D. (2005). Association between streptococcal infection and obsessive-compulsive disorder, Tourette's syndrome, and tic disorder. Pediatrics, 116(1), 56-60. doi: 10.1542/peds.2004-2058 Mol Debes, N. M., Hjalgrim, H., & Skov, L. (2008). Validation of the presence of comorbidities in a Danish clinical cohort of children with Tourette syndrome. J Child Neurol, 23(9), 1017-1027. doi: 10.1177/0883073808316370 Murphy, T. K., Kurlan, R., & Leckman, J. (2010). The immunobiology of Tourette's disorder, pediatric autoimmune neuropsychiatric disorders associated with Streptococcus, and related disorders: a way forward. J Child Adolesc Psychopharmacol, 20(4), 317331. doi: 10.1089/cap.2010.0043 O'Rourke, J. A., Scharf, J. M., Yu, D., & Pauls, D. L. (2009). The genetics of Tourette syndrome: a review. J Psychosom Res, 67(6), 533545. doi: 10.1016/j.jpsychores.2009.06.006 Pauls, D. L., Raymond, C. L., Stevenson, J. M., & Leckman, J. F. (1991). A family study of Gilles de la Tourette syndrome. Am J Hum Genet, 48(1), 154-163. Peterson, B. S., & Leckman, J. F. (1998). The Temporal dynamics of tics in Gilles de la Tourette syndrome. Biological Psychiatry, 44(12), 1337-1348. Peterson, B. S., Skudlarski, P., Anderson, A. W., Zhang, H., Gatenby, J. C., Lacadie, C. M., . . . Gore, J. C. (1998). A functional magnetic resonance imaging study of tic suppression in Tourette syndrome. Arch Gen Psychiatry, 55(4), 326-333. Peterson, B. S., Thomas, P., Kane, M. J., Scahill, L., Zhang, H., Bronen, R., . . . Staib, L. (2003). Basal Ganglia volumes in patients with Gilles de la Tourette syndrome. Arch Gen Psychiatry, 60(4), 415-424. doi: 10.1001/archpsyc.60.4.415 Piacentini, J., Woods, D. W., Scahill, L., Wilhelm, S., Peterson, A. L., Chang, S., . . . Walkup, J. T. (2010). Behavior therapy for children with Tourette disorder: a randomized controlled trial. JAMA, 303(19), 1929-1937. doi: 10.1001/jama.2010.607 Price, R. A., Kidd, K. K., Cohen, D. J., Pauls, D. L., & Leckman, J. F. (1985). A twin study of Tourette syndrome. Arch Gen Psychiatry, 42(8), 815-820. References Robertson, M. M. (2008). The prevalence and epidemiology of Gilles de la Tourette syndrome. Part 1: the epidemiological and prevalence studies. J Psychosom Res, 65(5), 461-472. doi: 10.1016/j.jpsychores.2008.03.006 Scahill, L., Erenberg, G., Berlin, C. M., Jr., Budman, C., Coffey, B. J., Jankovic, J., . . . Tourette Syndrome Association Medical Advisory Board: Practice, C. (2006). Contemporary assessment and pharmacotherapy of Tourette syndrome. NeuroRx, 3(2), 192-206. doi: 10.1016/j.nurx.2006.01.009 Scharf, J. M., Yu, D., Mathews, C. A., Neale, B. M., Stewart, S. E., Fagerness, J. A., . . . Pauls, D. L. (2013). Genome-wide association study of Tourette's syndrome. Mol Psychiatry, 18(6), 721-728. doi: 10.1038/mp.2012.69 Sowell, E. R., Kan, E., Yoshii, J., Thompson, P. M., Bansal, R., Xu, D., . . . Peterson, B. S. (2008). Thinning of sensorimotor cortices in children with Tourette syndrome. Nat Neurosci, 11(6), 637-639. doi: 10.1038/nn.2121 Stokes, A., Bawden, H. N., Camfield, P. R., Backman, J. E., & Dooley, J. M. (1991). Peer problems in Tourette's disorder. Pediatrics, 87(6), 936-942. Sullivan, P. F. (2010). The psychiatric GWAS consortium: big science comes to psychiatry. Neuron, 68(2), 182-186. doi: 10.1016/j.neuron.2010.10.003 Tourette Syndrome Association International Consortium for, G. (2007). Genome scan for Tourette disorder in affected-sibling-pair and multigenerational families. Am J Hum Genet, 80(2), 265-272. doi: 10.1086/511052 Weisman, H., Qureshi, I. A., Leckman, J. F., Scahill, L., & Bloch, M. H. (2013). Systematic review: pharmacological treatment of tic disorders--efficacy of antipsychotic and alpha-2 adrenergic agonist agents. Neurosci Biobehav Rev, 37(6), 1162-1171. doi: 10.1016/j.neubiorev.2012.09.008 Woods, D. W., & Himle, M. B. (2004). Creating tic suppression: comparing the effects of verbal instruction to differential reinforcement. J Appl Behav Anal, 37(3), 417-420. doi: 10.1901/jaba.2004.37-417 Woods, D. W., Piacentini, J., Himle, M. B., & Chang, S. (2005). Premonitory Urge for Tics Scale (PUTS): initial psychometric results and examination of the premonitory urge phenomenon in youths with Tic disorders. J Dev Behav Pediatr, 26(6), 397-403. Woods, D. W., Walther, M. R., Bauer, C. C., Kemp, J. J., & Conelea, C. A. (2009). The development of stimulus control over tics: a potential explanation for contextually-based variability in the symptoms of Tourette syndrome. Behav Res Ther, 47(1), 41-47. doi: 10.1016/j.brat.2008.10.013