What justifies the case-control design? - People.vcu.edu

Core Clinical Research
Concepts and Issues
Al M Best, PhD
Virginia Commonwealth University
Task Force on Design and Analysis in Oral Health Research
Satellite Symposium, AADR
Boston MA: March 9, 2015
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Outline
Core Concepts
– Defining the research question
– Causation vs. association
– Sources of error in clinical research
– Multiple outcomes: Primary & secondary outcomes
Prominent Design Issues in Clinical Research
– Randomization
– Masking/blinding
– Analysis: Intention-to-treat or Per Protocol?
– Biomarkers and surrogate measures
– Superiority, equivalence , or non-inferiority
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Outline
Intro to Multivariate Statistical Modeling
– Regression
Continuous outcomes: Linear …
Dichotomous outcomes: Logistic …
Counts: Poisson …
Time to event: Proportional hazards survival
– Unified management of confounding and effect modification in statistical models
– Propensity methods
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Core Concepts
Part 1
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Defining the research question
Conceptual progression from general to specific
General question
– Can GCF constituent levels distinguish active chronic adult perio sites from inactive and simple gingivitis sites?
Specific hypothesis
– Site GCF AST levels with active perio exceed those with inactive perio and simple gingivitis.
Testable consequence
– …
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Defining the research question:
Testable consequence
Context
– precise population: eligibility criteria*
– sampling: patient sources, recruitment, consent
– measurement definitions: detailed operational definitions
distinguishing active sites, inactive sites, gingivitis sites
GCF sampling, storage, and AST measurement procedures
Prediction: a relationship between exposure and outcome
Formalization: refutable hypotheses
* AKA: inclusion/exclusion criteria
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Defining the research question:
Prediction
Prediction: a statistical relationship between exposure and outcome
– GCF AST will be tend to be higher in active than in inactive or simple gingivitis sites within the same or different patients
Formalization: a refutable hypothesis
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Defining the research question:
Formalization
A refutable hypothesis
Statistical formalization:
Ho: Mean(Active) = Mean(Inactive) =
Mean(Gingivitis)
– Which may be disproved beyond a reasonable doubt through falsification by data via statistical hypothesis testing, in favor of:
Ha: Mean(Active) > Mean(Inactive) and
Mean(Active) > Mean(Gingivitis)
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Defining the research question:
Formalization
Estimating clinically relevant quantities
Clinical formalization:
– Mean(Active) – Mean(Inactive) > clinically important delta and
– Mean(Active) – Mean(Gingivitis) > clinically important delta
– Or, ROC AUC for distinguishing active perio > 0.75
These quantities may be estimated, and the clinically relevant hypotheses proven or disproved, using confidence intervals and associated statistical tests
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Characteristics of a well-framed clinical research question
FINER
– F easible
– I nteresting
– N ovel
– E thical
– R elevant
Source: Hulley, et al. (2007) Designing Clinical Research, Lippincot, Table 2.1
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
… a well-framed clinical research question
F easible
– Adequate subjects
– Adequate technical expertise
– Affordable in time and money
– Manageable in scope: logistics
I nteresting
– Generalizable to more than 1 application
– An answer would be intriguing to the investigator and at least some other folks
– Potentially fruitful, suggesting other hypotheses
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
… a well-framed clinical research question
N ovel
– New information
– Or in need of replication
E thical
– Avoids unacceptable risks
R elevant
– How might the various outcomes advance knowledge? Influence practice? Establish policy?
Or guide future research?
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Causation vs. Association
What do we mean by “Exposure
Disease B ”?
A causes
One approach: Logical consideration of evidence favoring causality
– Consistent association across studies and designs
– Strong association (big differences, strong trends)
– Dose response relationship
– Biologic plausibility
Note: investigators can come up with a plausible mechanism for virtually any
Causation vs Association
What do we mean by “Exposure
Disease B ”?
A causes
Empirical approach: http://xkcd.com/943/
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Causation vs Association
What do we mean by “Exposure
Disease B ”?
A causes
Empirical approach: Ruling out spurious associations
Statistical association
– Tendency of characteristics to vary together, so information on one allows guessing or predicting the other more accurately
– BUT: there are lots of ways we may be fooled
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Associations are common, and most are worthless
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
How we measure statistical associations
Associations are what we observe, as
– Differences or ratios of:
means or medians
proportions
odds
rates
– Slopes of trends in statistical models
– Correlation, regression coefficients
Causation → association, but not the other way
No measure of association, in itself, implies causation
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
www.phdcomics.com/comics/archive.php?comicid=1156
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Example of causal relationships
We think: influenza deaths less common in immunized groups
MI less common in hyperlipidemics on statins than in untreated hyperlipidemics
Stroke probability ↑ with ↑ SBP, ↑ LDL
↑ exercise, ↓ DBP
↑ sugar consumption, ↑ DMFS
↑ cigarette smoking, ↑ alveolar bone loss
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Example of non-causal or unproven relationships
We are not sure:
Antioxidant supplementation can lower US cancer risk
Calcium supplements reduce demineralization after 65
Treating chronic periodontitis reduces CVD risk
Scaling and root debridement in pregnant women will reduce preterm births
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
http://www.phdcomics.com/comics/archive.php?comicid=1452
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Clinical
research
is a
search
causes and predictors for
Comparison (control) is critical!
– Comparisons are needed to distinguish real from bogus causes
– Comparisons between groups are needed to escape the particular and possibly idiosyncratic
– Statistical associations are how one summarizes comparisons among groups
– Causal pathways imply statistical associations
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Clinical re
search
is a
search
causes and predictors for
Clinical research is about finding and distinguishing causal (or consistently prognostic) associations from those due to
– Reverse causation
– Measurement bias
– Selection bias
– Confounding
– Chance
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Sources of error in clinical research
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Reverse causation?
Does the outcome proceed from the clinical variable?
We observe: Prevalence of a disease is higher in those from whom a microbe is successfully cultured than in those from whom it is not
Is the microbe statistically associated with the disease
– because the microbe causes the disease?
– or because the disease makes the site more hospitable to colonization or infection by the microbe?
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Measurement (information) bias
Definition, Bias:
– Systematic distortion of the estimated intervention effect away from the “truth,” caused by inadequacies in the design, conduct, or analysis of a trial
Definition, Measurement bias:
– Systematic or non-uniform failure of a measurement process to accurately represent the measurement target
– Examples …
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Measurement (information) bias
Examples, Measurement bias:
– different approaches to questioning, when determining past exposures in a case-control study
– more complete medical history and physical examination of subjects who have been exposed to an agent suspected of causing a disease than of those who have not been exposed to the agent
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Measurement bias?
NHANES III: “We estimate that at least 35% of the dentate US adults aged 30 to 90 have periodontitis, with 21.8% having a mild form and 12.6% having a moderate form” 1
– Mesial and buccal surfaces
– Two randomly selected quadrants
– CAL≥3mm
Or: Full mouth prevalence= 64.7% vs partial =
39.1% 2
1 JM Albandar, JA Brunelle, A Kingman (1999) "Destructive periodontal disease in adults 30 years of age and older in the United States, 1988-1994".
Journal of Periodontology 70 (1): 13–29.
2 A Kingman & JM Albandar (2002) “Methodological aspects of epidemiological studies of periodontal diseases.” Periodontology 2000 29, 11–30.
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Recall bias
Is frequent sugar consumption related to childhood caries? Results using the British National Diet and Nutrition Survey (1995):
Conclusion “overall, the benefits of frequent brushing of teeth did not outweigh the damaging effect of frequent sugar consumption ”
Hinds & Gregory (1995)
National diet and nutrition survey: Children ages 1.5 to
4.5 years. Report of the Dental
Survey, vol. 2, London: HMSO .
Conclusion: “for children who brushed their teeth twice a day or more, consumption of sugars and sugary foods did not appear to be associated with caries”
Gibson & Williams (1999)
Dental caries in pre-school children: associations with social class, tooth brushing habit and consumption of sugars and sugar-containing foods.
113.
Caries Research 33,101–
Harris, et al. (2004) Risk factors for dental caries in young children: a systematic review, Community Dental Health, 21(S); 71-85
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Lead-time bias
Bias in evaluating screening programs
– If time to outcome (e.g., death) is measured from point of diagnosis, then early diagnosis will increase the estimated survival time by the interval between diagnosis-by-screening and when diagnosis would have occurred by ordinary means
– This can make early diagnosis appear to increase survival time, even when it has no effect … or even a damaging effect
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Lead-time bias
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Selection bias
Definition: Bias from the use of a nonrepresentative group as the basis of generalization to a broader population
Can distort: disease frequency measures, exposure-disease associations
Example: Estimate prognosis from patients newly diagnosed and infer to patients hospitalized with the disease
– Newly diagnosed patients have a much broader spectrum of outcomes
“Selection bias” is also used to describe the systematic error that can occur when allocating patients to intervention groups.
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Selection (=sampling) bias
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Admission rate bias
Definition: When admission rates vary between exposed cases and unexposed controls
Diseases of bones and organs of movement
Respiratory disease
Yes
No
Totals
In the general population
Yes No Totals %Yes
17 207 224 7.6
184 2376 2560 7.2
201 2583 2784
Relative risk= 1.06
Odds ratio= 1.06
Subset: those hospitalized in the prior 6 months.
Yes
5
No Totals %Yes
15 20 25.0
18 219 237 7.6
23 234 257
Relative risk= 3.29
Odds ratio= 4.06
Adapted from: Roberts, Spitzer, Delmore, Sackett (1978)
J Chron Dis (31) 119-128
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Admission rate bias
AKA: Berkson’s bias
Respiratory disease
Yes
No
Totals
Diseases of bones and organs of movement
In the general population
Yes No Totals %Yes
17 207 224 7.6
184 2376 2560
201 2583 2784
7.2
Relative risk= 1.06
Odds ratio= 1.06
Subset: those hospitalized in the prior 6 months.
Yes
5
No Totals %Yes
15 20 25.0
18 219 237 7.6
23 234 257
Relative risk= 3.29
Odds ratio= 4.06
Adapted from: Roberts, Spitzer, Delmore, Sackett (1978)
J Chron Dis (31) 119-128
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
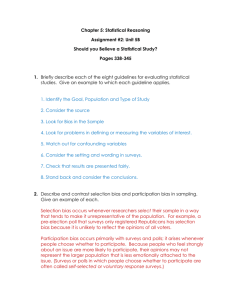
Length-time bias
Bias in evaluating screening programs: two cases
– a slowing progressing disease vs.
– a rapidly progressing disease
In standard clinical practice: The observed proportion of those with the disease will be higher for the rapidly progressing disease because they have a shorter asymptomatic phase
In a screening program: The observed proportion of those with the disease will be higher for the slowly progressing disease because they are detectable over a wider range of time
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Length-time bias
Patients diagnosed by screening will, as a group, progress more slowly than those diagnosed by conventional means. Even if early treatment has no impact.
O N W E A L T H U N I V E R S I T Y
Sources of bias
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Confounding
Informal definition: distortion of the true biologic relation between an exposure and a disease outcome of interest
Usually due to a research design and analysis that fail to properly account for additional variables associated with both
– Such variables are referred to as confounders or, less formally, as lurking variables
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Confounding examples
“Honey, it’s not my fault!
It’s the one-night stand gene”
“The D4 mutation of the human dopamine receptor gene is linked with: gambling, alcoholism, drug use, overeating, political liberalism, passion for horror films, ADHD, extreme extraversion, impulsiveness”
Garcia et al. (2010) Associations between Dopamine D4 Receptor
Gene Variation with Both Infidelity and Sexual Promiscuity. PLoS
ONE 5(11): e14162
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Confounding examples
Misidentified carcinogen
Prior to the discovery of HPV, HSV-2 was associated with the cervical cancer
It is now well established that HPV is central to the pathogenesis of invasive cervical cancer.
And HSV-2 appears to increase the risk
Hawes & Kiviat (2002) Are Genital Infections and Inflammation Cofactors in the Pathogenesis of Invasive Cervical Cancer? JNCI 94(21): 1592-159
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Perio and CVD
Cigarette smoking is associated with adult perio and CVD
This produces an association between perio and
CVD
Control for smoking to see the perio-CVD relationship clearly
Scannapieco et al. (2003) Associations Between Periodontal Disease and
Risk for Atherosclerosis, Cardiovascular Disease, and Stroke. A Systematic
Review. Annals of Periodontology (8)38-53
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Confounding
7
6
5
9
8
4
3
2
1
0
Amount of dental care
Less
More
Total
Annual %
Less (n=393) More (n=322)
Amount of dental care
One year loss of any teeth
Survival
Yes
20
No
373
Total loosing teeth
393
Annual %
5.1
6
26
316
689
322
715
Relative risk=
Odds ratio=
1.9
2.73
2.82
Note: artificial data
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Amount of dental care
Less
More
Total
Amount of dental care
Less
More
Total
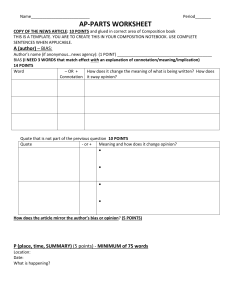
Confounding
One year loss of any teeth: Clinic A
Survival Annual %
Yes
3
4
7
No
176
293
Total loosing teeth
179
297
1.7
1.3
469 476
Relative risk=
Odds ratio=
1.24
1.25
One year loss of any teeth: Clinic B
Survival Annual %
Yes
17
2
19
No
197
23
220
Total loosing teeth
214 7.9
25
239
8.0
Relative risk=
Odds ratio=
0.99
0.99
Annual %
7
6
9
8
5
4
1
0
3
2
A, Less
(n=179)
A, More
(n=297)
B, Less
(n=214)
Amount of dental care
B, More
(n=25)
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Confounding:
Simpson’s paradox
Statistical associations in entire groups can differ from statistical associations in their subgroups
Worse: statistical associations in whole groups can be in the opposite direction from statistical associations in every subgroup!!!
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Multiplicity effects
http://xkcd.com/882/
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Multiplicity effects
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Multiplicity effects
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Multiplicity effects
N=47 perio,
N=20 healthy
Analyzed for the presence of
300 species
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Controlling multiplicity effects
Multiplicity: The proliferation of possible comparisons in a trial. Common sources of multiplicity are:
– multiple outcome measures, assessment at several time points, subgroup analyses, or multiple intervention groups
Multiple comparisons: Performance of multiple analyses on the same data. Multiple statistical comparisons increase the probability of a type I error: “finding” an association when there is none
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Controlling multiplicity effects
Analysis of multiple outcome variables that reflect different disease manifestations, any of which might signal a spurious association due purely to chance
Analysis of the same variable at multiple time points after treatment initiation
Periodic analysis of accumulating partial results to see how a study is progressing, and whether there’s reason to stop collecting data earlier than initially planned
Post hoc subgroup comparisons are especially likely not to be confirmed in following studies
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Multiple outcome examples
Caries
– visual exam
– x-ray interpretation
– Fiberoptic Transillumination (FOTI)
– Electrical Caries Meter (ECM)
– DiagnoDent (DD)
Perio
– alveolar bone loss
– clinical attachment level
– pocket depth
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Multiple comparisons
If we control the chance of a false positive answer in evaluating a single outcome by a conventional statistical method, which permits a 5% chance of claiming a statistical association when none exists,
– then by the time we’ve compared treatments on
4 outcomes our chance of an error is MUCH
HIGHER
We can’t stop asking questions, so three strategies are used to control this
– Require stronger evidence to claim an effect
– Hierarchy of outcomes
– Composite outcome
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Require stronger evidence to claim an effect
Example: When asking 5 questions
Require stronger evidence for each question so that the chance of claiming statistical association when none exists is only 1% instead of p < 5%
This insures that, overall, no more than 5% false positive errors
– Various methods guide how much stronger one should require evidence to be in different circumstances
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Composite outcome
Combine multiple outcomes into one index, and use that as a single outcome
Multivariate → Univariate
– Meld several outcomes into one question, by asking whether any function of any of them is associated with the exposure, e.g., treatment, and seeking a single yes or no
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Outcome hierarchy
Order outcomes from most to least important
Crucial decisions in planning and analyzing the study are based on the primary outcome atop the hierarchy
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Multiple outcome variables
Requiring stronger evidence to claim an effect is often overly conservative
– Also, it’s hard to get folks to implement it sincerely
– Somehow lots of ‘buts’ get into the interpretation
Composite outcomes and outcome hierarchies require choices clinical researchers are not always comfortable making
– Results may be hard to interpret
– Composite outcome methods are being gradually adopted in some fields, e.g., stroke
Disclose “data snooping”
Only pre-specified comparisons are to be believed
BUT, in a frankly “pilot study” the purpose is to find the subgroup, “dose”, time point, and outcome where the difference is largest
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Effect of Systemic Matrix Metalloproteinase Inhibition on Periodontal
Wound Repair: A Proof of Concept Trial
Background: The adjunctive use of matrix metalloproteinase (MMP) inhibitors with scaling and root planing (SRP) promotes new attachment in patients with periodontal disease. This pilot study was designed to examine aspects of the biological response brought about by the MMP inhibitor low dose doxycycline (LDD) combined with access flap surgery (AFS) on the modulation of periodontal wound repair in patients with severe chronic periodontitis.
Methods: Twenty-four subjects were enrolled into a 12-month, randomized, placebo-controlled, double-masked trial to evaluate clinical, biochemical, and microbial measures of disease in response to 6 months therapy of either placebo capsules + AFS or LDD (20 mg b.i.d.) + AFS.
Clinical measures including probing depth (PD), clinical attachment levels (CAL), and bleeding on probing (BOP) as well as gingival crevicular fluid bone marker assessment (ICTP) and microbial
DNA analysis (levels and proportions of 40 bacterial species) were performed at baseline and 3,
6, 9, and 12 months.
Results: Patients treated with LDD + AFS showed more potent reductions in PD in surgically treated sites of >6 mm (P <0.05, 12 months).
Furthermore, LDD + AFS resulted in greater reductions in ICTP levels compared to placebo + AFS. Rebounds in ICTP levels were noted when the drug was withdrawn. No statistical differences between the groups in mean counts were found for any pathogen tested.
Conclusions: This pilot study suggests that LDD in combination with AFS may improve the response of surgical therapy in reducing probing depth in severe chronic periodontal disease. LDD administration also tends to reduce local periodontal bone resorption during drug administration.
The use of LDD did not appear to contribute to any significant shifts in the microbiota beyond that of surgery alone. Gapski, Barr, Sarment, Layher, Socransky, Giannobile
2004;75:441-452.
J Periodontol
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Concepts
You need a testable, FINER research question
Try to rule out bias, confounding, chance
Consider multiple outcome measures and multiple predictors
Disclose what you did [and why] with enough detail so others may replicate
Mark Twain: There is something fascinating about science.
One gets such wholesale returns of conjecture out of such a trifling investment of fact.
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y
Thanks
… for your participation
Acknowledgement: I’m grateful to Peter B Imrey, PhD for sharing his previous version of this talk.
V I R G I N I A C O M M O N W E A L T H U N I V E R S I T Y