USMLE STEP I Review Week 6: Renal and Hematology Physiology
advertisement

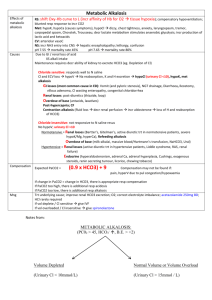
Steven Katz, MSIV Part 1: Hematology and Oncology (p.326-347) Blood Cell Differentiation Heme Terms (p. 327) Erythrocyte: anucleate, biconcave cell with large surface area for gas exchange. Macrophage: mature monocyte, phagocytic cell found in tissues Platelet: cytoplasmic fragment of megakaryocyte, involved in primary hemostasis. Aggregates and interacts with fibrinogen to form hemostatic plug. 1/3 platelet pool stored in the spleen. Heme terms (p.327) Leukocyte: two types granulocytes and mononuclear cells. Involved in defense against infections Basophil: Granulocyte, mediates allergic rxn, in blood Mast Cell: Granulocyte, binds IgE to membrane, found in tissue Eosinophil: Granulocyte, causes of eosinophilia (NAACP) Neoplasm, Asthma, Allergy, Collagen Vasc. Dz, Parasites Neutrophil: Granulocyte, acute inflammatory response cell Monocyte: mononuclear cell, “frosted glass cytoplasm” Heme Terms (p.327) Dendritic Cells: APC, has MHC II and Fc receptor, main inducer of 10 Ab response Lymphocyte: mononuclear cells mature into: B lymphocyte: humoral immunity Plasma cell: mature B Lymphocyte, produce Ab. (multiple myeloma is a plasma cell neoplasm) T lymphocyte: cellular immunity, matures in thymus ○ MHC x CD=8 (MHC2 x CD4 & MHC1 x CD1) Intrinsic Pathway Extrinsic Pathway * * * TF = thromboplastin * * Factor II is prothrombin (IIa is thrombin) * = Ca required Thrombogenesis Coag Cascade and platelet plug (p.330) Platelet plug formation 1. Adhesion: vWF mediates linking of platelet Gp1b receptor to subendothelial collagen 2. Aggregation: balance btw pro-aggregation and anti-aggregation factors TxA2 released by platelets incr aggregation PGI2 and NO from endothelial cells decr aggregation 3. Swelling: binding of ADP on platelet receptor insertion of G2b/3a on platelet memb which allows platelet cohesion, Ca strengthens platelet plug ASA inhibits cyclooxygenase which inhibits TxA2 synthesis Coag cascade: pro-coagulation (p.330) Vitamin K becomes activated by epoxide reductase and acts as a co-factor in the maturation of Factors II, VII, IX,, X, C, and S Warfarin inhibits epoxide reductase von Willebrand factor carries/protect VIII Binds GpIb to subendothelial collagen as well Coag cascade: anti-coagulation (p.330) Antithrombin III inactivates factors II, VII, IX, X, and XI Heparin activates ATIII Protein C is activated by Protein S and thrombomodulin (endothelial cells). APC (activated protein C) cleaves and inactivates Va and VIIIa Factor V Leiden mutation produces APC resistant Factor V Plasminogen –tPA-> plasmin cleavage of fibrin mesh Coag cascade and kinin (p.331) Hereditary Thrombosis Syndromes (p.329) Factor V Leiden: mutant factor V cannot be degraded by protein C Prothrombin gene mutation: Mutation in 3’ untranslated region associated with venous clots AT III deficiency: inherited deficiency of ATIII, reduced increase of PTT with heparin admin Protein C or S deficiency: decreased ability to inactivate factors V and VIII. Increased risk of hemorrhagic skin necrosis following warfarin admin Blood groups (p.331) Type A: has A Ag on RBC and B Ab in plasma Type B: has B Ag on RBC and A Ab in plasma Type AB: A and B Ag on RBC, no Ab in plasma “universal RECIEPIENT” Type O: No Ag on RBC, both AB in plasma, “universal DONOR” Rh: + indicates Ag is present, mothers who are neg, may make anti-Rh IgG that can cross the placenta and cause hemolytic dz of the newborn (in the subsequent pregnancy) RBC pathologies (p.332) Type Biconcave Spherocyte Elliptocyte Macro-ovalocyte Helmet cell, shistocyte Sickle Cell Bite Cell Teardrop cell Acanthocyte (spur cell) Target cell Burr Cell Basophilic stippling Pathology Normal spherocytosis, autoimmune hemolysis Hereditary elliptocytosis Megaloblastic anemia, marrow failure DIC, TTP/HUS, traumatic, hemolysis Sickle Cell anemia G6PD deficiency Myeloid metaplasia with myelofibrosis “Spiny”, in liver dz and abetalipoproteinemia HbC dz, Asplenia, Liver dz, Thalassemia (HALT) TTP/HUS Thalassemia, Anemia of chronic dz, IDA, Lead (TAIL) Anemias-VERY IMPORTANT (p.332) Microcytic Hypochromic: MCV <80 Iron deficiency anemia: serum iron, TIBC, ferritin (intracellular iron store) ○ Decreased heme synthesis Thalassmia: target cells ○ Mut leads to decr globin synthesis Lead poisioning ○ Inhibits ferrochelatase and ALA dehydrase (heme synthesis) Some sideroblastic anemias Anemia of chronic dz: release of iron to transferrin Anemias-VERY IMPORTANT (p.332) Macrocytic: MCV >100 Megaloblastic-vit B12 and/or folate deficiency Drugs that block DNA synthesis (e.g sulfa, phenytoin, AZT) Marked reticulocytosis (bigger than mature RBC’s) Anemias-VERY IMPORTANT (p.332) Normocytic, normochromic Acute hemorrhage Enzyme defects (e.g. G6PD) RBC membrane defects (e.g. spherocytosis) Bone marrow disorders (e.g. aplastic anemia, leukemia) (macrocytic as well) Hemoglobinopathies (e.g. sickle cell) Autoimmune hemolytic anemia Anemia of chronic dz: TIBC, ferritin, increased storage in marrow macrophages Lab values in anemia IDA Serum Iron Chronic Disease (10) (10) Transferrin/ TIBC Ferritin % transferrin saturation (serum Fe/TIBC) Ferritin=iron storage; Transferrin=iron transport in blood Hemo- Pregnancy chroma- /OCP use tosis (10) - Porphyria (p.333) Lead poisioning: build up coproporphyrin and ALA 2/2 inhibition of ferrochelatase and ALAL dehydrase Acute intermittent porphyria: build up of porphobilinogen and d-ALA 2/2 inhibition of iroporphyrinogen I synthase Porphyria Cutanea Tarda: build up of uroporphyrin (tea-colored) 2/2 inhibition of uroporphyrinogen decarboxylase Hemoglobin synthesis Blood Dyscrasias (p.334) Sickle Cell: mut of beta-globin chain. Low O2 or dehydration precipitates sickling. Complications: ○ aplastic anemia (parvo B19) ○ Autosplenectomy ○ incr risk of encapsulated org infect ○ Salmonella osteomyelitis ○ vaso-occlusive crises ○ renal papillary necrosis, etc. Therapies include hydroxyurea (incr HbF), bone marrow transplant, folate, etc. “Crew cut” on skull XR 2/2 marrow expansion from incr erythropoeisis Newborns are initially asymptomatic 2/2 high HbF levels Blood Dyscrasias (p.334) a-thalassemia: there are 4 a-globin chains and clinical dz depends on how many chains are under-produced. HbH: b4-tetramers, lacks 3 a-globin genes Hb Barts: g4-tetramers, lacks all 4 a-globin genes ○ Results in hydrops fetalis and intrauterine fetal death Most prevalent in Asian and African populations Blood Dyscrasias (p.334) b-thalassemia: Minor (heterozygotes): beta-chain is under- produced Major (homozygotes): beta-chain is absent ○ Require transfusions and get 2ndary hemochromatosis (need iron chelator) HbF production is increased but inadequate HbS/B-thal heterozygotes have increased propensity to have sickling. Hemolytic Anemias (p.335) Usually results in increased serum bilirubin (indirect/unconjugated) and reticulocytosis INTRAvascular hemolysis hemoglobinuria EXTRAvascular jaundice Hemolytic Anemias (p.335) Autoimmune Warm agglutinin (IgG) chronic anemia seen in SLE, CLL, and with certain drugs (e.g. amethyldopa). Mostly extravascular hemolysis (RBC’s destroyed by Kupffer cells and spleen) Cold agglutinin (IgM) ACUTE anemia triggered by cold, seen with Mycoplasma pneumoniae or mono (EBV). Erythroblastosis fetalis: in newborns 2/2 Rh or other blood group incompatibility. Ab from Mom destroy baby’s RBC’s. Hemolytic Anemias (p.335) Hereditary spherocytosis: Extravascular hemolysis 2/2/ defect in ankyrin, band 3.1, or spectrin. RBC are round and have no central pallor Increased MCHC and RDW Associated with splenomegaly, aplastic crisis, and Howell-Jolly bodies Coombs negative, use osmotic fragility test for confirmation of disease Howell-Jolly Body Hemolytic Anemias (p.335) Paroxysmal nocturnal hemoglobinuria: Intravascular hemolysis 2/2 membrane defect. The RBC’s have an increased sensitivity to the lytic activity of complement (impaired synthesis of GPI anchor/decayaccelerating factor in RBC membranes) Lab tests show increased urine hemosiderin (iron storage complex similar to ferritin) Hemolytic Anemias (p.335) Microangiopathic Anemia: Intravasular hemolysis seen in DIC TTP/HUS SLE Malignant hypertension Disseminated Intravascular Coagulation (DIC) (p.335) Activation of the coagulation cascade leading to microthrombi and global consumption of platelets, fibrin, and coagulation factors. Causes: Sepsis, Trauma, Obstetric complications, acute Pancreatitis, Malignancy, Nephrotic syndromes, Transfusion (STOP Making New Thrombi) Lab Findings: Incr PT, PTT, fibrinogen, and fibrin split products (D-dimer) Decr platelet count Helmet cells and shistocytes on blood smear Bleeding disorders (p.336) Platelet abnormality causes: ITP: peripheral platelet destruction, anti-GpIIb/IIIa Ab, incr megakaryocytes) ○ May have onset after a viral infection ○ Definitive treatment in splenectomy TTP: deficiency in vWF cleaving metalloproteinase, incr platelet aggregation, thrombosis and shistocyte formation, incr LDH, neurologic and renal sx, fever Aplastic anemia Drugs: immunosuppressive agents Bleeding disorders (p.336) Coagulation Factor Defects/Coagulopathies: Hemophilia A: factor VIII deficiency Hemophilia B: Factor IX deficiency Von Willebrand’s disease: fairly mild it is the most common bleeding disorder ○ Cause of bleeding is deficiency of von Willebrand’s factor which leads to a defect of platelet adhesion and decreased factor VIII survival ○ *Remember vWF helps protect Factor VIII! Hemorrhagic Disorders (p.336) DISORDER Platelet count Bleeding time Thrombocytopenia Hemophilia A or B N/C von Willebrand’s disease N/C N/C PT PTT N/C N/C N/C N/C * N/C or DIC Vitamin K deficiency N/C Bernard-Soulier disease (BS) Glanzmann’s thrombansthenia (GT) N/C N/C N/C N/C N/C N/C Hemorrhagic Disorders Defects in platelet plug formation lead to increased bleeding time GT: decr GpIIb/IIIa (defect in platelet-platelet adhesion) BS: decr GpIb (defect in platelet-collagen adhesion) vWD: decr vWF (defect in platelet-collagen adhesion) DIC and thombrocytopenia: decreased platelet count Defects in extrinsic coag cascade lead to increased PT Defects in intrinsic coag cascade lead to increased PTT Reed-Sternberg cells (p. 337) Distinctive giant cell associate with Hodgkin’s lymphoma Bilobed or binucleate cell appear as “owl eyes” The cells are CD30+ and CD15+ of B-cell origin Necessary but not sufficient for dx of Hodgin’s dz Lymphomas (p.337) Hodgkin’s Non-Hodgkin’s Reed-Sternberg cells Localized, single group of nodes May be associated with HIV and immunosuppression Extranodal dz is rare Contiguous spread (stage is strongest predictor of prognosis) Multiple peripheral nodes Extranodal dz is common Non-contiguous spread Constitutional “B” si/sx: low grade feve, night sweats, weight loss Majority involve B cells (except those of lymphoblastic T cell origin) Mediastinal lymphadenopathy 50% of cases associated with EBV Bimodal distribution—young and old Fewer constitutional si/sx More common in men except for nodular sclerosing type Peak incidence for certain subtypes at 20-40 years of age Good prognosis = increased lymphocytes and decreased RS Hodgkin’s Lymphoma (p. 337) Type Nodular Sclerosing (65-75%) RS Lymphocyte Prognosis Comments Most common Collagen banding and lacunar cells Women>men ,10 young adults + +++ Excellent Mixed Cellularity (25%) ++++ +++ Intermediate Numerous RS cells Lymphocyte predominant (6%) + ++++ Excellent < 35 year olds RS high v. lympho -cyte + Poor Older males with disseminated disease Lymphocyte depleted (rare) Non-Hodgkin’s Lymphoma (p.339) Type Small lymphocytic lymphoma Follicular lymphoma (small cleaved cell) Diffuse large cell lymphoma Mantle Cell Lymphoma Occurs in Adults Adults Cell type Genetics Like CLL with focal mass B cells B cells -Difficult to t(14:18) cure bcl-2 expression -bcl-2 inhibits apoptosis - Most common - Aggressive but many are curable Usually older 80% B cells adults, but 20% T cells 20% in kids (mature) Adults B cells Comments t(11:14) Poor prognosis CD5+ Non-Hodgkin’s Lymphoma (p.339) Type Lymphoblastic lymphoma Burkitt’s lymphoma Occurs in Cell type Genetics Comments Most often in T cells kids (immature) - Most common in kids, commonly with ALL and mediastinal mass - Very aggressive Tcell lymphoma Most often in B cells kids - “Starry-sky” appearance (l-cytes with interspersed macrophages), associated with EBV - Jaw lesions endemic in Africa t(8:14) c-myc gene moves next to heavy-chain Ig gene (14) Multiple Myeloma (p.338) Monoclonal plasma cell cancer that arises in the marrow and produces IgG (55%) or IgA (45%). Most common 10 tumor arising within the bone in the elderly (> 40-50 y/o) Symptoms: destructive bone lesions and consequent hypercalcemia Renal insufficiency Increased susceptibility to infection Anemia Also associated with 10 amyloidosis and punched out lytic lesions on x-ray. Think CRAB: hyperCalcemia, Renal insuff, Anemia, Back and Bone pain Multiple Myeloma (p.338) Labs: SPEP (serum protein electrophoresis) shows monoclonal Ig spike (M protein) UPEP (urine protein electrophoresis) shows Ig light chains (aka Bence Jones protein) Peripheral Smear shows RBC’s stacked like poker chips (Rouleaux formation) Compare to Waldenström’s macroglobulinemia M spike is IgM (not IgG or IgA) Also hyperviscosity symptoms, no lytic bone lesions If asymptomatic dx is monoclonal gammopathy of undetermined significance (MGUS) Chromosomal Translocations (p. 339) Translocation Associated Disorder t(9;22) Philadelphia chromosome CML (bcr-abl hybrid) t(8;14) Burkitt’s lymphoma (c-myc activation) t(14;18) Follicular lymphoma (bcl-2 activation) t(15;17) M3 type of AML (responsive to alltrans retinoic acid) t(11;22) Ewing’s sarcoma t(11;14) Mantle cell lymphoma Leukemoid Rxn (p.340) Increased white blood count with LEFT shift (e.g. 80% bands) Increased leukocyte alkaline phosphatase Leukemias (p.340) General signs and symptoms: Increased number of circulating leukocytes Bone marrow infiltrates of leukemic cells Marrow failure can cause anemia Infection (decreased mature WBC’s) Hemorrhage (decreased platelets) Leukemic cell infiltrates in liver, spleen and lymph nodes are possible as well Leukemias (p.340) ALL: Most common in < 15 y/o Bone marrow replaced by large increase in lymphoblasts TdT+ (marker of pre-T and pre-B cells) Most responsive to therapy May spread to CNS and testes AML: Median onset ~60 y/o, Auer rods seen on smear Large increase in circulating myeloblasts M3 responds to all-trans retinoic acid (Vit A) (induces differentiation of myeloblasts) Leukemias (p.340) CLL: seen in > 60 y/o Lymphadenopathy, hepatosplenomegaly Few symptoms and generally indolent course Smudge cells on smear Warm Ab autoimmune anemia Similar to SLL (small lymphocytic lymphoma) CML: Age range 30-60 y/o Defined by the Philadelphia chrom, myeloid stem cell proliferation Presents with increased neutrophils, metamyelocytes, basophils, splenomegaly May accelerate and transform into ALL (1/3) or AML (2/3) “blast crisis” Left shift with all stages of myeloid maturation on smear Very low leukocyte alk phos (vs. leukomoid rxn) ○ Responds to imatinib (anti bcr-abl) Leukemias (p.340) Hairy cell leukemia—mature B-cell tumor in the eldery. Cells have filamentous, hair like projections. Stains TRAP (tartrate-resistant acid phosphatase) positive Auer rods (p.340) Peroxidase positive cytoplasmic inclusions in granulocytes and myeloblasts Commonly seen in acute promyelocytic leukemia (M3) Treatment of M3 AML can release Auer rods Langerhans cell histiocytoses/ Histocytosis X (p.340) Proliferative disorders of dendritic (Langerhans) cells from the monocyte lineage Defective cells express S-100 and CD1a Birbeck granules (“tennis rackets” on EM) are characteristics Older terms for different clinical conditions with same basic disorder ○ Letterer-Siwe dz, Hand-Schuller-Christian dz, eosinophilic granulomas Myeloproliferative disorders (p.341) RBC’s WBC Platelets Philadelphia chromosome Polycythemia Vera (PCV) Essential Thrombocytosis Myelofibrosis CML -- -Variable Variable JAK2 mutations Neg Pos Neg Pos (30-50%) Neg Pos (30-50%) Pos Neg The myelofibroproliferative disorders represents an overlapping spectrum classic findings below: PCV-Abnl hematopoeitic stem cells that are sensitive to growth factors ET-Similar to PCV, but specific for megakaryocytes Myelofibrosis-Fibrotic obliteration of bone marrow CML-bcr-abl transformation leads to incr cell division and inhib of apoptosis. JAK2 is involved in hematopoeitic growth factor signaling. Mutations are important in disorders other than CML Heme Pharmacology Heparin: catalyzes the activation of ATIII, decr thrombin, and Xa Must monitor PTT LMWH: Acts more on Xa, can be administered subQ, can not be given to renal failure pts. PTT monitoring not needed Warfarin: interferes with Vit K dependant clotting factors. Increases PT ASA: Irreversibly inhibits COX-1 and COX-2 Increases bleeding time Part 2: Renal (p.436-452) Quick Anatomy Review Ureters: Course (p.436) Ureters pass UNDER the uterine artery and UNDER the ductus (vas) deferens (retroperitoneal) Water UNDER the bridge Fluid Compartments (p.437) 1/3 60% TB weight 2/3 Osmolarity: 290 mOsm Plasma = ¼ ECF, Interstitial vol = ¾ ECF 60-40-20 rule (% of TB weight) Plasma vol measured by radiolabeled albumin ECF measured by inulin Renal Clearance (p.437) Cx = UxV/Px = volume of plasma from which the substance is completely cleared per unit time Cx < GFR: net tubular reabsorption of X Cx > GFR net tubular secretion of X Cx= GRF no net secretion of X Cx = clearance of X (units are mL/min) Ux = urine concentration of X Px = plasma concentration of X V = urine flow rate Glomerular Filtration (p.437) Barrier: responsible for filtration of plasma according to size and net charge Composed of: Fenestrated capillary endothelium Fused BM with heparan sulfate (neg charge) Epithelial layer with podocyte foot processes Charge barrier is LOST in nephrotic syndromes albuminuria, hypoproteinemia, edema (generalized), and hyperlipidemia Glomerular Filtration (p.437) Rate: Use inulin to calculate as it is not secreted or resorbed and it is FREELY filtered. GFR = Uinulin x V/Pinulin = Cinulin = Kf[(PGC – PBS) – (pGC - pBS)] Kf = filtration coefficient/GC = glomerular capillary/BS = Bowman’s space Creatinine clearance slightly overestimates GFR as it is secreted in the renal tubules Effective Renal Plasma Flow (ERPF) (p.437) ERPF can be estimated using PAH clearance as it is both filtered and actively secreted by the tubule. ALL PAH entering the kidney is excreted RBF = RPF/(1-HCT) ERPF underestimates true RPF by about 10% Filtration (p.438) Filtration fraction = GFR/RPF Filtered load = GFR x plasma conc Prostaglandins dilate afferent arteriole Increase RPF and GFR so FF constant NSAID’s block this action Angiotensin II preferentially constricts efferent arteriole Decr RPF but incr GFR so FF increases ACE inhibitor blocks this action Changes in Renal Fxn Effect RPF Afferent arteriole constriction GFR FF NC Efferent arteriole constriction Incr plasma protein conc NC Decr plasma protein conc NC Constriction of ureter NC Clearance (p.438) Free Water: Ability to dilute urine CH 20 = V- Cosm V = urine flow rate; Cosm = UosmV/Posm With ADH: CH < 20 0 (retention of free water) Without ADH CH 0 > 0 (excretion of free water) 2 Isotonic urine CH 0 = 0 (seen with loop diuretics) 2 Clearance (p.438) Glucose is FULLY reabsorbed in the proximal tubule at normal plasma levels At or above 200 mg/dL glucosuria begins (threshold) At 350 mg/dL transport mechanism is saturated (Tm) Amino Acids: reabsorption by 3 different carrier systems, with competitive inhibition with each group Secondary active transport occurs in in proximal tubule and is SATURABLE (p. 439) Early Proximal Tubule: •Contains brush border which resorbs •ALL of the glucose and amino acids •MOST of the HCO3, Na, and water •ISOtonic absorption • Secretes ammonia acts as buffer for secreted hydrogen ions PTH: Inhibits Na/PO4 co-transport phosphate excretion ATII: stimulates Na/H exchange Increased Na and water excretion (can cause contraction alkalosis) reabsorption (p. 439) Thick ascending loop of Henle: • Actively resorbs Na, K, and Cl • Indirectly induces the paracellular reabsorption of Mg and Ca • Impermeable to water • DILUTING seegment • Makes urine HYPOtonic (p. 439) • Passively resorbs water via medullary hypertonicity. Thin descending loop of Henle: • The walls are impermeable to sodium • Makes urine HYPERtonic (p. 439) Early DCT: •Actively resorbs Na, Cl •Diluting segment •Makes urine HYPOtonic PTH: Increases Ca/Na exchange Increased Ca resorption (p. 439) Collecting Tubule: •Resorbs Na in exchange for K and H (regulated by aldosterone) Aldosterone: •Leads to insertion of Na channel on LUMINAL side ADH: acts at V2 receptors •Insertion of aquaporin channel on LUMINAL side Relative concentrations along renal tubule (p. 440) Renin-Angiotensin-Aldosterone System (p.440) Juxtaglomerular apparatus (p.441) JG cells (modified smooth muscle of afferent arteriole) and macula densa (Na sensor, part of DCT) JG cells secrete renin (leading to increased angiotensisn II and aldosterone levels) in response to decreased renal BP, decreased Na delivery to distal tubule, and increased sympathetic tone. Endocrine Fxns of the Kidney (p. 441) Endothelial cells of the peritubular capillaries secrete EPO in response to hypoxia Prox tubule cells convert Vit D to its active form (indirect stim from PTH) PTH acts directly on the kidney to increase Ca reabsorption and decr PO4 reabsorption JG cells secrete renin in response to decr renal arterial pressure and increase sympathetic discharge (B1 effect) Endocrine Fxns of the Kidney (p. 441) Secretion of prostaglandins to vasodilate afferent arterioles to incr GFR. NSAID’s can cause renal failure by inhibiting the renal production of prostaglandins. Hormones acting on the kidney (p. 442) Acid/Base—VERY IMPORTANT (p.442) pH PCO2 [HCO3] Compensatory mech Met acidosis Hyperventilation Met alkalosis Hypoventilation Resp acidosis Increase renal HCO3 reabsorption Resp alkalosis Decrease renal HCO3 reabsorption Henderson-Hasselbach equation pH= pKa + log [HCO3]/0.03*PCO2 Approach to Acid/Base (p.442) NORMAL VALUES: 1. pH = 7.40 HCO3 = 24 mEq/L AG = 12 Does the pH indicate an alkalosis or acidosis? ○ 2. PCO2 = 40mmHg Acidosis pH < 7.40; Alkalosis pH >7.40 Is the primary disorder respiratory or metabolic? ○ Acidosis: ○ Respiratory if PCO2 > 40 Metabolic if HCO3 < 24 Alkalosis: Respiratory if PCO2 < 40 Metabolic if HCO3 > 24 Approach to Acid/Base (p.442) 3. What is the Anion gap? Na – (Cl + HCO3) If AG > 20, AGMA is present regardless of pH ○ ○ 4. Is there proper compensation? Winter’s Formula: used to check for resp. compensation when met. acid is present ○ ○ ○ ○ Expected PCO2 = 1.5 (HCO3) + 8 +/- 2 < expected resp alkalosis is present > expected resp acid is present Quick and Dirty method: if last two digits of pH = PCO2 then there is likely appropriate compensation Met alkalosis: increase in PCO2 = 0.75(DHCO3) Acute Resp: change in PCO2 of 10 = pH change of 0.08 in opposite direction Chronic Resp: change in PCO2 of 10 = pH change of 0.03 in opposite direction Approach to Acid Base: 5. If there is an AGMA, is there another disorder? Use the corrected serum HCO3 equation: ○ Excess anion gap = measured – normal ○ Corrected HCO3 = Excess AG + measured HCO3 If HCO3 > normal then met alkalosis is present If HCO3 < normal then NAGMA is present If HCO3 = normal then no other disorder is present Common Causes of Each Disorder Respiratory acidosis: CNS depression, neuromuscular d/o, airway obstruction, severe PNA, lung dz (acute and chronic), opioids and narcotics Respiratory alkalosis: Hyperventilation (high altitude), pregnancy, sepsis, mechanical ventilation, ASA ingestion (early) AGMA: MUDPILES Methanol, Uremia, DKA/starvation, Paraldehyde or Phenformin, INH or Iron, Ethylene glycol (oxalic acid), Salicylates Common Causes of Each Disorder NAGMA: GI bicarb loss (diarrhea), or renal bicarb loss (early renal failure, RTA, aldosterone inhibitors), Glue sniffing, hyperchloremia Metabolic Alkalosis: Vomiting, NG suction, diuretics, volume contraction, mineralocorticoid excess, antacid use Renal Tubular Acidosis (p.444) Type 1: Defect in H/K ATPase of collecting tubules inability to secrete H. ○ Can lead to hypokalemia Type 2: Defect in proximal tubule HCO3 reabsoprtion. ○ Can lead to hypokalemia Type 4: Hypoaldosteronism hyperK inhibition of ammonia excretion in proximal tubule. ○ Leads to decreased urine pH 2/2 decr buffering capacity Casts and what they mean (p.444) RBC casts: Glomerular inflammation (nephritic syndromes) Ischemia Malignant hypertension WBC casts: Tubulointerstitial dz Acute pyleonephritis Glomerular disorders Granular “muddy Brown” casts: Acute tubular necrosis Waxy casts: advanced renal dz/CRF Hyaline casts: nonspecific MISCELLANEOUS: Bladder Ca: RBC no casts Acute cystitis: WBC no casts Casts continued (p.444) Above: RBC Below: Granular Above: WBC Below: Hyaline Nephritic (p. 445) An inflamatory process involves the glomerulus azotemia, hematuria, RBC casts, oliguria, HTN, and proteinuria Acute post-strep glomerulonephritis (GN) LM-glomeruli enlarged and hypercellular, “lumpy-bumpy” EM-subepithelial immune complex (IC) humps Immunofluorescence (IF)-granular Most freq seen in children. Periph and periorbital edema. Resolves spontaneously Rapidly progressive GN (Cresentic) LM and IF-crescent moon 1. Goodpasture’s-type II hypersensitivity, Ab to GBM=linear IF 2. Wegener’s granulomatosis 3. Microscopic polyarteritis Male-dominant dz Hematuria/hemoptysis (lung involved) Diffuse proliferative GN (due to SLE) Subendothelial DNA-anti-DNA IC’s “wire-looping” of capillaruies IF-granular Most common cause of death in SLE. SLE can present as nephrotic syndrome Berger’s disease Increased synthesis of IgA. IC’s deposit in mesangium Often follows URI, often presents as nephrotic syndrome Mutation in type IV collagen split basement membrane Nerve disorders, ocular disoders, deafness also 2/2 mutation in type IV collagen (IgA glomerulopathy) Alport’s syndrome c-ANCA p-ANCA Nephrotic (p.445) Nephrotic syndrome presents with passive proteinuria (>3.0-3.5 g/day, frothy urine), hyperlipemia, edema Also can have increased coagulation as proteins C and S are lost in urine as well Membranous glomerulonephritis (Diffuse membranous glomerulopathy) LM-diffuse capillary and GBM thickening EM-”spike dome” appearance IF-granular SLE nephrotic presentation Minimal change disease (Lipoid nephrosis) LM- normal glomeruli EM-foot process effacement Caused by drugs, infections, and SLE Most common cause (MCC) of adult nephrotic syndrome Nephrotic pics (p. 445) Granular IF in membranous GN “spike and dome” on EM Minimal change dz: note appearance is fairly normal Nephrotic (p.445) Amyloidosis LM-Congo red stain, apple-green birefringence Associated with multiple myeloma, chronic conditions, TB and RA Diabetic glomerulonephropathy Non-enzymatic glycosylation (NEG) of GBM permeability, thickening, NEG of efferent arterioles GFR mesangial damage, wire looping LM-Kimmelsteil-Wilson “wire loop” lesions Focal segmental glomerulosclerosis LM- segmental sclerosis and hyalinosis Most common glomerular dz in HIV pts. More severe in these pts as well. Membranoproliferative glomerulonephritis Subendothelial IC with granular IF EM-”tram-track” appearance due to GBM splitting caused by mesangial ingrowth Can present as nephritic syndrome Usually progresses slowly to CRF Associated with HBV > HCV Glomerular histopathology (p.446) 1. Subepi: membranous nephropathy 2. Large irregular subepi “humps”: acute GN 3. Subendo deposits in lupus GN 4. Mesangial deposits in IgA nephropathy 5. Ab binding to GBM— linear pattern on IF (Goodpasture’s) 6. Effacement of epithelial foot processes (in all with proteinuria, imp for minimal change dz (may be only sign on EM)) Kidney Stones (p.446) Can lead to severe complications (e.g. pyelonephritis, and hydronephrosis) 4 Major types: Calcium: Most common stone and tend to recur (75-85%) ○ Radio-opaque and contain CaPO4 and/or Ca oxalate ○ Conditions that cause hyperCa (cancer, PTH, Vit D, milk-alkali syndrome) can lead to hypercalciuria and stones. Ammonium magnesium phosphate (struvite): ○ 2nd most common ○ Caused by infection with urease-positive bugs (Proteus, Staph, Klebsiella) ○ Can form staghorn calculi that can be a nidus for UTI’s ○ Rasio-opaque or lucent. Worse with alkauria Kidney Stones (p.446) Can lead to severe complications (e.g. pyelonephritis, and hydronephrosis) 4 Major types: Uric Acid: Radio-lucent ○ Strong association with hyperuricemia (e.g. gout) ○ Often seen as a result of disease with increased cell turnover E.g. Leukemia and myeloproliferative disorders Cystine: Faintly radio-opaque, treat with urine alkalinization ○ Most often secondary to cystinuria. ○ Hexagonal shape ○ Rarely may form cystine staghorn calculi Renal cell carcinoma (p.447) Most common renal malignancy and in men age 50-70 Originates in renal tubule cells polygonal clear cells Invades IVC and spreads hematogenously. Associated with von Hippel-Lindau and chromosome 3 gene deletion, increased incidence w/smoking and obesity Clinically manifests with hematuria, palpable mass, secondary polycythemia, flank pain, fever, and weight loss Also associated with paraneoplastic syndromes Ectopic EPO, ACTH, PTHrP, and prolactin Wilms’ tumor (p.447) Most common renal malignancy of early childhood (ages 2-4) Genetic: Deletion of tumor suppressor gene WT1 on chromosome 11 Contains embryonic glomerular structures Clinically presents with huge palpable flank mass, hemihypertrophy. May be associated with WAGR copmplex Wilms’ tumor Aniridia Genitourinary malformation mental motor Retardation Transitional Cell Ca (p. 447) Most common tumor of urinary tract system Can occur in renal calyces, renal pelvis, ureters, and bladder (all places where there are transitional cells) Painless hematuria is suggestive of bladder cancer Associated with problems in Pee SAC: Phenacetin, Smoking, Aniline dyes, and Cyclophosphamide Pyelonephritis (p. 447) Acute: Affects cortex with relative sparing of glomeruli/vessels White cell casts are pathognomonic Presentation: fever, CVA tenderness Chronic: Coars, asymmetric corticomedullary scarring Blunted calyx Tubules can contain eosinophilic casts Diffuse Cortical Necrosis (p.447) Acute generalized infarction of cortices of both kidneys Likely 2/2 combo of vasospasm and DIC Associated with obstetric catastrophes (e.g. abruptio placentae) and septic shock Drug-Induced Interstitial Nephritis (p.447) Acute interstitial renal inflammation Causes: Drugs (e.g. PCN derivatives, NSAID’s, diuretics) act as haptens (a small molecule that can elicit an immune response) inducing hypersensitivity Signs/Symptoms: Fever, rash, eosiniophilia, hematuria 2 WEEKS after administration Acute Tubular Necrosis (p.447) Cellular: Loss of cell polarity, epithelial cell detachment, necrosis, granular “muddy brown” casts 3 stages: Inciting event maintenance (low urine) recovery MCC of iatrogenic ARF Reversible but fatal if untreated (tx with dialysis) Associated with renal ischemia, crush injury (myoglobinuria), and toxins Death occurs most often during initial oliguric phase Recovery in 2-3 weeks Renal Papillary Necrosis (p.447) Sloughing of renal papillae Gross hematuria and proteinuria Associated with Diabetes Mellitus Acute pyelonephritis Chronic phenacetin use (acetaminophen is derivative) Sickle Cell Anemia Acute Renal Failure (p.448) Normally BUN is reabsorbed but Cr is NOT ARF is defined as an abrupt decrease in renal fxn with increase in Cr and BUN over a period of several days. Acute Renal Failure (p.448) 1. 2. Prerenal azotemia: decr RBF decr GFR. Na/water and urea retained by the kidney , so BUN/Cr ratio incr in attempt to comserve volume Intrinsic renal: generally due to acute tubular necrosis or ischemia/toxins. 1. 2. 3. 3. Patchy necrosis leads to debris obstructing the tubule and fluid backflow across necrotic tubule decreased GFR Urine has epithelial/granular casts. BUN resorption is impaired decreased BUN/Cr ratio Postrenal: outflow obstruction (stones, BPH, neoplasia) 1. Stones as cause only develops with bilateral obstruction Acute Renal Failure (p.448) Variable Prerenal Renal Postrenal Urine osmolality > 500 < 350 < 350 Urine Na < 10 > 20 > 40 FENa < 1% > 2% > 4% > 20 < 15 > 15 FENa = (UNa * PCr/ PNa * UCr) x 100 Serum BUN/Cr Renal Failure (p.448) Inability to make urine and make nitrogenous waste. Leads to uremia Clinical syndrome marked by increased Bun and Cr and other associated sx’s (confusion, HTN, coma, fibrinous pericarditis, etc.) 2 forms of renal failure Acute: often due to ATN Chronic: MCC’s diabetes and HTN Renal Failure (p.448) Consequences: Anemia (failure of EPO production) Renal osteodystrophy (failure of Vit D production) HyperK cardiac arrhythmias (peaked T waves) Metabolic Acidosis: 2/2 decreased acid secretion and decreased production of HCO3 Uremic encephalopathy confusion, AMS, coma Sodium and water excess CHF and pulm edema Chronic pyelonephritis HTN Pericarditis Fanconi’s syndrome (p.448) Decreases tubule transport of AA, glucose, PO4, Uric acid, protein and electrolytes Can be acquired or congenital Causes include Wilson’s Dz, glycogen storage dz, and drugs (cisplatin, expired tetracycline) Defect Complications Decr PO4 reabsorption Rickets Decr HCO3 reabsorption Metabolic acidosis Decr early Na reabsorption Incr distal Na reabsorption hypoK Cysts (p.449) ADPKD -Multiple, large b/l cysts that ultimately destroy the parenchyma. Enlarged kidneys. -Presents with flank pain, hematuria, HTN, UTI, progressive renal failure. -AD mut in APKD1 or APKD2. -Death from uremia or HTN ARPKD Infantile presentation in parenchyma. AR, associated with hepatic cysts and fibrosis Dialysis cysts Cortical and medullary cysts resulting from long standing dialysis Medullary cystic dz Medullary cysts. U/S shows small kidneys. POOR prognosis Medullary sponge dz Collecting duct cysts. GOOD prognosis Simple Cysts Benign, incidental finding. Cortex only Electrolyte Disturbances (p.449) Electrolyte Low serum conc Disorientation, coma, stupor Na High serum conc Neurologic: irritability, delirium, coma Cl 2/2 met alk, hypoK, hypovol, incr aldosterone 2/2 NAGMA K U waves in EKG, flattened T waves, arrhythmias, paralysis Peaked T waves, wide QRS, arrhythmias Ca Tetany, neuromuscular irritability Delirium, renal stones, abd pain, not necessary calciuria Mg neuromuscular irritability, arrhythmias Delirium, decreased DTR, cardiopulm arrest PO4 Low-mineral ion product causes bone loss, osteomalacia High-mineral ion product causes renal stones, metastatic calcifications Diuretics: Site of Action ACE inhibitors “-pril”(p.452) Mechanism: Inhibits ACE reduces levels of AGII and prevents inactivation of bradykinin (a potent vasodilator) Renin release is increased 2/2 loss of feedback inhibition. Clinical use: HTN, CHF, diabetic renal dz Toxicity: Cough, Angioedema, Proteinuria, Taste changes, hypOtension, Pregnancy problems (fetal renal damage), Rash, Increased renin, Lower AGII (CAPTOPRIL) HyperK Avoid in bilat renal artery stenosis because ACE inhib significantly decr GFR by preventing constriction of efferent arterioles Diuretics: Loop v. Thiazides Loop Diuretic (furosemide) Inhibits cotransport (Na,K,2Cl) of Thick Mechanism ascending LOH. Abolishes hypertonicity of medulla, prevents urine concentration Clinical use Toxicity Thiazide (HCTZ) Inhibits NaCl resorption in early distal tubule, reduces diluting capacity of the nephron. Decr Ca excretion Edematous states, (CHF, cirrhosis, nephrotic syndrome, pulm edema) HTN, hyperCa HTN, CHF, idiopathic hypercalciuria, nephrogenic diabetes insipidus Ototoxicity, HypoK, Dehydration, Allergy (sulfa), Nephritis, Gout OH DANG! Hypokalemic met alk, hypoNa, hyperGlycemia, hyperLipidemia, hyperUricemia, hyperCalcemia. Sulfa allergy. hyperGLUC Diuretics: K+ sparing Spironolactone, Triamterene, Amiloride Mechanism: Spironolactone is a competitive aldosterone receptor antagonist in the cortical collecting tubule (CCT). Triamterene and amiloride act at the same part of the tubule by blocking Na channels in the CCT. Clinical Use: Hyperaldosteronism, K depletion, CHF Toxicity: HyperK, endocrine effects of aldosterone antagonists ○ Gynecomastia, antiandrogen effects Note: Spironolactone can also be used to treat acne in females, it is from the anti-androgen side effect!