Final Lab Report - Personal.psu.edu
advertisement

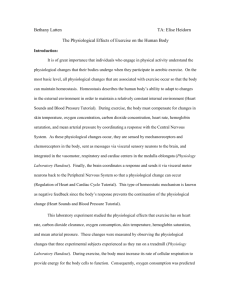
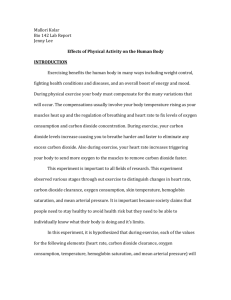
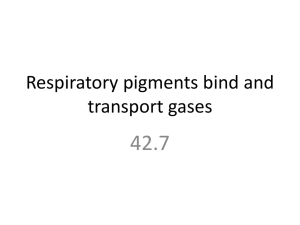
Grant Kovich BIOL142, Section 021 TA: Brenna Hill Exercise Physiology Lab Report 2 December 2011 The VO2 Max Test: An Indicator of Cardiovascular Fitness, Not Just for Athletes Introduction Exercise—considered to be stress relief by some, and torture by others. Many people are so concerned with their appearance and surroundings during exercise, they do not realize the incredible amount of activity that is happening physiologically in every cell of the body. Cardiovascular fitness can be measured by performing a test called a VO2 max test, in which a subject’s body is pushed to the limits of exercise, usually causing complete exertion. Although the main objective of the VO2 max test is to determine how physically fit an individual is, the test also measures many vital physiological changes throughout the body. Results from a VO2 max test can also provide insight to doctors who are pursuing a treatment plan for a patient suffering from cardiovascular or respiratory diseases, by showing if the treatment is effective or not. By recording these physiological changes as exercise intensity progresses, biologists can understand how the systems of the body compensate for an increased demand for oxygen and energy over time. The VO2 max test is marked by stages, with each stage having increased exercise intensity, which demands more output from the subject. When the body begins to undergo the process of exercise, many physiological changes occur. Body temperature, respiratory rate, heart rate, and blood concentration of both oxygen and carbon dioxide must change in order to maintain a homeostatic environment in the body throughout exercise (1). As the intensity level of exercise increases, these changes are more pronounced. From both personal experience and observed patterns of behavior from athletes, we feel that there are many noticeable changes that occur during increased intensity exercise. Differences in various physiological indicators can be seen when the body is at rest, during warm up, throughout exercise, and during recovery. We expect to see changes in heart rate, exhaled tidal carbon dioxide concentration, 1 oxygen concentration of exhaled air, body temperature, hemoglobin saturation, and mean arterial pressure. At rest, we expect the values for the physiological indicators to be at fairly normal levels i.e. body temperature of 37ºC, heart rate of 55-65 BPM, etc. During the warm up period, as the body is rapidly adjusting to exercise, we expect that all of the values will increase, in order to adjust to the physiological stress that is occurring. We feel that all of the values except hemoglobin saturation will increase linearly with an increase in exercise intensity, due to the body requiring more resources to adapt to a higher level of exercise intensity. We predict hemoglobin saturation will decrease linearly in response to increased exercise intensity, due to faster blood flow preventing hemoglobin stability in the blood. When exercise capacity has been reached, and the subject cannot perform at a high level anymore, we feel that the values will be at their highest levels, since the body will be at complete exhaustion. As the body recovers from intense exercise, we expect the values to slowly decrease as the time for recovery increases, with the exception of hemoglobin saturation, which we predict to slowly increase back to normal levels. However, we feel that the values will not return to the same levels during rest prior to exercise until a few hours after exercise. We believe that since high intensity exercise is extremely stressful on the body, it will take more than a few minutes for complete recovery to occur. Method Subjects were chosen on a volunteer basis, and were only allowed to participate in experimentation if they were in a completely healthy state. Prior to experimentation, age, height, weight, gender, and whether or not the subject smoked were recorded for each subject. Exercise heart rate was also calculated for subjects, by determining 80% of their maximal heart rate, which is calculated by 220 – age. Subjects were connected to a polar heart rate monitor and a skin thermometer prior to exercise, so that heart rate and body temperature could be measured throughout exercise. If at any point the subject’s heart rate surpassed the exercise heart rate, experimentation would be stopped immediately. Initial 2 measurements of tidal volume (spirometer), oxygen concentration of exhaled air (oxygen analyzer), exhaled tidal carbon dioxide concentration (capnometer), hemoglobin saturation (pulse oximeter), respiratory rate (capnometer) and blood pressure (sphygmomanometer) were taken while the subject was at rest. Resting measurements, taken between 0 and 3 minutes, served as control measurements upon which comparisons of the results of the experiment could be made. Subjects were given 1-2 minutes to adjust to the treadmill, and then experimentation began. The experiment consisted of exercise levels of increasing difficulty. Every three minutes, measurements of heart rate, tidal volume, respiratory rate, exhaled total carbon dioxide concentration, and oxygen concentration of exhaled air were recorded, just prior to moving onto the next stage of exercise. Visual observations concerning the subject’s appearance were also recorded regularly, as safety was of the utmost importance for the duration of the experiment. When subjects could no longer move onto the next stage of the test, researchers ended the test by lowering the treadmill speed to 3-4 miles per hour and lowering the treadmill angle to 0 degrees. Measurements of skin temperature, hemoglobin saturation, and blood pressure were taken as soon as the test ended. Subjects were then instructed to walk on the treadmill for no fewer than 6 minutes. At each 3-minute interval of the recovery period, measurements of heart rate, tidal volume, respiratory rate, exhaled tidal carbon dioxide concentration, oxygen concentration of exhaled air, skin temperature, hemoglobin saturation, and blood pressure were taken. At the conclusion of the recovery period, no further measurements were taken, and final visual observations of the subject’s appearance were made. Upon completing measurements of exhaled tidal carbon dioxide concentration, oxygen concentration of exhaled air, and blood pressure, further calculations were performed to determine carbon dioxide clearance, oxygen consumption, and mean arterial pressure, respectively. Carbon dioxide clearance, the amount of carbon dioxide being expelled by the body every minute, was calculated by the following formula: CO2 Clearance = (%CO2 of Exhaled Air) x (Tidal Volume) x (Respiratory Rate) (1). Oxygen consumption, the amount of oxygen used by the body cells every minute, was calculated by the 3 following formula: O2 Consumption = (%O2 of Exhaled Air) x (Tidal Volume) x (Respiratory Rate) (1). Finally, mean arterial pressure, the average arterial pressure during a single cardiac cycle, was calculated using the following formula: MAP = Diastolic Pressure + 1/3(Systolic Pressure – Diastolic Pressure) (2). Results Figure 1. Observed changes in heart rate with increasing exercise intensity. Heart Rate (BPM) 250 200 150 Subject 1 100 Subject 2 50 0 0 5 10 15 20 25 Time (min) Heart rate increased rapidly as exercise began, slowly increased throughout exercise, and drastically decreased at the end of exercise. It did not, however, reach resting levels prior to exercise in both subjects. CO2 Clearance (L/min) Figure 2. Observed changes in CO2 clearance with increasing exercise intensity. 2.5 2 1.5 1 Subject 1 0.5 Subject 2 0 0 5 10 15 20 25 Time (min) Carbon dioxide levels fluctuated as exercise began, and then increased throughout exercise. At the completion of exercise, levels sharply declined and were very close to the resting levels seen at rest. 4 O2 Consumption (L/min) Figure 3. Observed changes in oxygen consumption with increasing exercise intensity. 1.2 1 0.8 0.6 Subject 1 0.4 Subject 2 0.2 0 0 5 10 15 20 25 Time (min) Oxygen consumption gradually increased at the beginning and throughout exercise, with variation occurring at the end of exercise. Post-exercise levels varied among the subjects, being above and below resting levels. Table 1. Observed changes in body temperature, hemoglobin saturation, and mean arterial pressure with increasing exercise intensity. Time points correspond to the following periods: rest = 0, warm up = 3 minutes, exercise = 18 minutes, and recovery = 21-24 minutes. Time (min) Body Temperature (ºC) Hemoglobin Saturation Mean Arterial Pressure (%) (mmHg) Subject 1 Subject 2 Subject 1 Subject 2 Subject 1 Subject 2 0 34 35 98 97 77 85 3 35 35 100 96 77 87 6 9 Due to the manner in which these measurements were made, we felt it was unsafe to record measurements while the subjects were performing the experiment. 12 15 18 37 36 79 84 107 113 21 36 36 86 96 103 83 24 36 37 95 96 80 78 Body temperature increased slightly at the onset of exercise in both subjects, increased significantly during exercise, then failed to return to resting levels at the conclusion of exercise. Hemoglobin saturation varied when exercise began, drastically decreased during exercise, then gradually increased back to near normal levels during the recovery period in both subjects. Mean arterial pressure in both subjects increased slightly as exercise began, increased at a higher rate as exercise took place, and then slowly lowered to levels comparable to those seen during the resting period. 5 Overall, observed data featured a similar trend in that during rest, measurements were low, and gradually increased as exercise commenced. As exercise intensity increased, most of the data increased in response to intensity. At the conclusion of exercise, during the recovery period, most of the data lowered in values, returning to levels near what they were prior to exercise. In the case of hemoglobin saturation, the data showed an opposite trend—values were normal at resting levels, decreased with increasing exercise intensity, and then increased back to near normal levels during recovery. Discussion Prior to experimentation, predictions were made about how the following physiological factors would change with exercise of an increasing intensity: heart rate, carbon dioxide clearance, oxygen consumption, temperature, hemoglobin saturation, and mean arterial pressure. A general hypothesis was made for all physiological tests--normal levels prior to exercise, a linear increase in levels during increased exercise intensity, and a slow decline back to near resting levels during recovery, while the opposite trend was predicted with hemoglobin saturation. Heart rate displayed by the subjects followed a pattern that which strongly supports our hypothesis. During the warm up period, heart rate slowly increased as the body adjusted to exercise. As exercise intensity increased, heart rate also increased linearly to allow for more blood flow, fulfilling the requirement of a larger need for oxygen and removal of carbon dioxide in the muscles. During recovery, heart rate slowly declined to levels that were slightly higher than those seen during rest prior to exercise (Fig. 1). In theory, the results for carbon dioxide clearance and oxygen consumption are dependent on each other. If the muscles are consuming more oxygen, this means that carbon dioxide is produced at the same rate, signifying the need for more rapid removal from the muscles. Our results do not strongly support our original hypothesis, as the measurements fluctuated throughout the experiment (Figs. 2 & 3). We feel that the outlying measurement at 10 minutes is a possible source of error, due to the fact that exercise intensity increased, not decreased, from 5 to 10 minutes. The extremely low values at 20 minutes, and the fluctuations that occurred in Subject 2 between 15 and 20 minutes are also erroneous in 6 our opinion, because exercise intensity was still increasing during this time (Figs. 2 & 3). Carbon dioxide clearance and oxygen consumption should increase linearly with exercise intensity, as the body requires more oxygen and needs to remove more carbon dioxide when muscles are performing greater work. We feel that the source of error behind these outlying measurements is the method in which oxygen consumption and carbon dioxide clearance were measured. Since the nose was not clipped during experimentation, subjects expelled air through both the nose and mouth. This signifies that complete exhalations were not being sent through the sensors, because some of the air was expelled through the nose. We believe that a larger volume of air being expelled through the nose, rather than the mouth caused the outlying data points. We predict that had the nose been clipped during experimentation, the results would have corresponded with our hypothesis. At the beginning of exercise, body temperature increased, just as when exercise intensity increased, which strongly supports our hypothesis. However, during recovery, body temperature dropped very slightly, and measurements were different for both subjects, which does not very strongly support our hypothesis (Table 1). We do not feel that this is a source of error, but rather a physiological difference in each subject. The rate at which body temperature is lowered can depend on many factors including the amount of clothing the subject is wearing, the temperature of the exercise environment, and the amount of fluid intake during recovery, and the cardiovascular fitness level of the subject. We believe that it can take upwards of 30 minutes for body temperature to return to levels seen prior to exercise. Overall, the observations seen when measuring body temperature follow a similar pattern to what we hypothesized; body temperature just did not decline as much as we would have expected during the recovery period. The results for hemoglobin saturation can be related to the changes in heart rate. As exercise intensity increases, heart rate also increases, sending more blood to the muscles. This causes less hemoglobin molecules to stay together in red blood cells, which lowers hemoglobin saturation. We predicted that levels would drop linearly with increasing exercise intensity, and then return to normal 7 levels during recovery. Hemoglobin saturation observed throughout experimentation did in fact strongly support our hypothesis, due to the fact that an increased heart rate caused lower hemoglobin saturation. Since mean arterial pressure is calculated from diastolic and systolic pressure, and there is a relationship with heart rate and blood pressure, we predicted that mean arterial pressure would increase with increased intensity of exercise, and then decrease back to levels seen during rest prior to exercise. Due to the heart pumping a greater volume of blood at a faster rate, blood pressure must increase as a result of these changes. Blood pressure measurements allowed for mean arterial pressure to be calculated, and it can be seen in the results that mean arterial pressure did in fact strongly support our hypothesis (Table 1). Conclusion The aforementioned experiment displayed data that is extremely valuable in not only determining the cardiovascular fitness of an individual, but the different physiological changes that occur during exercise as well. Data can not only be used to assess the cardiovascular fitness from an athletic standpoint, but also to compare individuals who suffer from respiratory diseases such as asthma, COPD, and emphysema, as well as cardiovascular diseases such as hypertension. We feel that with more advanced equipment our measurements could have been more precise. We also believe that more frequent measurements would have allowed for more consistent data. However, with the resources at hand, we feel that experimentation went smoothly, and valuable data was collected and analyzed. Although all of our hypotheses were accepted, we feel that changes can be made to allow the experiment to run more smoothly and provide more valuable data. We feel there should be three groups of subjects sorted by their activity level--sedentary, moderately active, and very active. With a random sample of a larger subject pool, correlations and comparisons can be made not only within each group, but among the groups as well. Also, our experiment featured only women subjects. For a complete experiment, subjects can also be separated by gender. Valuable insights into exercise physiology can be drawn from a comparison of the physiological changes that occur across different activity levels. We feel 8 that this experiment was a step in the right direction, and future studies concerning exercise physiology will only yield more exciting and significant findings. References 1. Waters J. 2011. Exercise Physiology Handout: https://cms.psu.edu/Merge/2009/MRG-110708152625-JRW8/_assoc/009D3BC2BF154BC081CCD6FAD577D7DB/exercise_physio.pdf. 2. Waters J. 2011. Heart Sounds and Blood Pressure Handout: https://cms.psu.edu/section/content/ default.asp?WCI=pgDisplay&WCU=CRSCNT&ENTRY_ID=3E29AB3B7FD74F1FAD552C99 EB191DBA. 9