Exercise Physiology Lab
advertisement

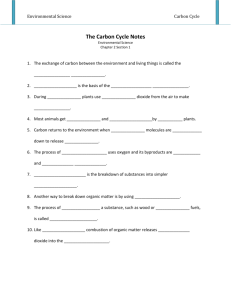
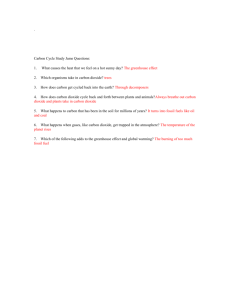
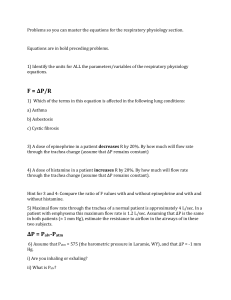
Bethany Latten TA: Elise Heidorn The Physiological Effects of Exercise on the Human Body Introduction: It is of great importance that individuals who engage in physical activity understand the physiological changes that their bodies undergo when they participate in aerobic exercise. On the most basic level, all physiological changes that are associated with exercise occur so that the body can maintain homeostasis. Homeostasis describes the human body’s ability to adapt to changes in the external environment in order to maintain a relatively constant internal environment (Heart Sounds and Blood Pressure Tutorial). During exercise, the body must compensate for changes in skin temperature, oxygen concentration, carbon dioxide concentration, heart rate, hemoglobin saturation, and mean arterial pressure by coordinating a response with the Central Nervous System. As these physiological changes occur, they are sensed by mechanoreceptors and chemoreceptors in the body, sent as messages via visceral sensory neurons to the brain, and integrated in the vasomotor, respiratory and cardiac centers in the medulla oblongata (Physiology Laboratory Handout). Finally, the brain coordinates a response and sends it via visceral motor neurons back to the Peripheral Nervous System so that a physiological change can occur (Regulation of Heart and Cardiac Cycle Tutorial). This type of homeostatic mechanism is known as negative feedback since the body’s response prevents the continuation of the physiological change (Heart Sounds and Blood Pressure Tutorial). This laboratory experiment studied the physiological effects that exercise has on heart rate, carbon dioxide clearance, oxygen consumption, skin temperature, hemoglobin saturation, and mean arterial pressure. These changes were measured by observing the physiological changes that three experimental subjects experienced as they ran on a treadmill (Physiology Laboratory Handout). During exercise, the body must increase its rate of cellular respiration to provide energy for the body cells to function. Consequently, oxygen consumption was predicted to increase in order to power increased levels of cellular respiration. Due to the body’s increased oxygen needs, hemoglobin saturation was predicted to decrease as the intensity of the exercise increased since more oxygen had to be released at cells. Moreover, heart rate was expected to steadily increase as the subjects exercised in order to pump oxygenated blood out to all body cells. Due to the body’s greater rate of cellular respiration, more carbon dioxide was expected to be produced as metabolic waste and cleared from the body during exhalation. Likewise, mean arterial pressure was expected to increase since a faster heart rate increases cardiac output and exerts more pressure on arterial walls. Finally, an increase in skin temperature was also expected to occur as the body increased its energy production and lost energy to the environment as heat in attempts to maintain a constant internal body temperature. Furthermore, since all aforementioned homeostatic control mechanisms are involved in negative feedback responses, the rates of all processes were expected to return back to resting levels as the experiment subjects recovered from exercise. Methods: (adapted from Physiology Laboratory Handout) In order to examine the physiological changes that occur as a result of exercise, several sets of data were recorded before, during, and after the experimental subjects engaged in exercise. The following measurements were recorded while the subject sat in a chair and rested: heart rate, tidal volume, respiratory rate, concentration of carbon dioxide in exhaled tidal air, concentration of oxygen in exhaled air, skin temperature, hemoglobin saturation, and blood pressure (systolic and diastolic). General observations of the subject’s physical appearance were also recorded, and the same measurements were taken three minutes later. This baseline set of data functioned as the control since it conveyed the physiological biomarkers of the subjects while they were not exercising. Furthermore, comparisons between the baseline data and the data collected during and after the subjects exercised allowed the physiological changes that resulted from exercise to be discerned. During the experiment, exercise heart rate was measured by a heart rate monitor wrapped around the subject’s chest. It was important to keep track of exercise heart rate in order to discern whether or not the subject had reached his or her maximum heart rate, which would indicate that he or she should stop running. Maximum heart rate was determined by the following equation: .8 x (220-subject’s age). Furthermore, tidal volume was measured by having the subject exhale into a spirometer; concentration of tidal carbon dioxide in the exhaled air was determined by a capnometer; the concentration of oxygen in the exhaled air was measured by an oxygen analyzer; skin temperature was measured by a thermometer headband; the amount of oxygen in the subject’s blood, his or her hemoglobin saturation, and his or her heart rate were measured by a pulse oximeter; and finally, the subject’s systolic and diastolic blood pressure was measured by using a sphygmomanometer and stethoscope. After recording the resting measurements, the subject began running on a treadmill at five miles per hour at zero degrees incline. Every three minutes, heart rate, tidal volume, respiratory rate, concentration of tidal carbon dioxide in the exhaled air, concentration of oxygen in the exhaled air, and observations of the subject’s physical appearance were recorded. Skin temperature, hemoglobin saturation, and blood pressure were not recorded while the subject was running because such measurements require that the subject is not moving. Once each set of data was collected, the incline of the treadmill was increased. This process was repeated until the subject no longer wanted to keep running. Immediately after the subject stopped running, all measurements (including skin temperature, hemoglobin saturation, and blood pressure) were taken again, and the subject began walking on the treadmill at a pace of two miles per hour. After three minutes, the subject stopped walking so that all measurements could be taken, and the subject was then allowed to sit down. After another three-minute interval, the last set of data for all measurements was collected. This procedure was followed for each of the three subjects who ran on the treadmill. Using the data from the experiment, further measurements were calculated. First, the percentage of carbon dioxide in the exhaled air was found. %CO2 of exhaled = ETCO2 x 760mmHg Using the values found by the previous formula, carbon dioxide clearance could be determined. Carbon dioxide clearance (liters CO2/min) = (%CO2 of exhaled air) x tidal volume (L/breath) x respiratory rate (breaths/min) Next, oxygen consumption was found by using the following formula: O2 consumption (liters O2/min)= (20.9% - %O2 of exhaled air) x tidal volume (liters/breath) x respiratory rate (breaths/min) Finally, arterial blood pressure was determined by using the values obtained when systolic and diastolic blood pressure were measured. MAP (mmHg) = Diastolic blood pressure + (Systolic blood pressure – Diastolic blood pressure)/3 Results: The following results reflect the measurements obtained when each of the three subjects rested, ran, and recovered from running on the treadmill. However, not all of the subjects ran for the same amount of time. Subject 1 ran for 15 minutes and 7 seconds and reached 15 degrees of incline; Subject 2 ran for 10 minutes and 20 seconds and reached 10 degrees of incline; Subject 3 ran for 6 minutes due to a time constraint and only reached 3 degrees of incline. All subjects rested and recovered for the same amount of time. As demonstrated by Figure 1 on the next page, the heart rate of all subjects increased during exercise, gradually decreased during recovery, but did not reach resting heart rate before the end of the experiment. Fig. 1: Changes in Heart Rate Beats per Minute 250 200 150 100 Subject 1 50 Subject 2 0 Subject 3 Time Figure 1: Heart rate increased during exercise and decreased during recovery. As demonstrated by Figure 2, carbon dioxide clearance increased as exercise intensity increased. During recovery, carbon dioxide clearance decreased so that it almost reached resting levels. Liters Carbon Dioxide Figure 2: Changes in Carbon Dioxide Clearance 7 6 5 4 3 2 1 0 Subject 1 Subject 2 Subject 3 Time Figure 2: Carbon dioxide clearance increased during exercise and decreased during recovery. The results presented in Figure 3 demonstrate that oxygen consumption also decreased during exercise and increased during recovery to levels even greater than the resting levels in Subjects 1 and 3. In Subject 2, not all measurements for oxygen consumption were recorded. Liters Oxygen Fig. 3: Changes in Oxygen Consumption 8 7 6 5 4 3 2 1 0 Subject 1 Subject 2 Subject 3 Time Figure 3: Oxygen consumption increased during exercise and decreased during recovery. The following table shows the changes in skin temperature (Skin Temp.), hemoglobin saturation (Hemog. Sat.), and mean arterial pressure (MAP) experienced by each of the subjects before, during, and after exercise. Table 1: Effects of Exercise on Temperature, Hemoglobin Saturation, and Mean Arterial Pressure Subject 1 Time Subject 2 Subject 3 Skin Hemog. MAP Skin Hemog. MAP Skin Hemog. MAP Temp. Sat. (mmHg) Temp. Sat. (mmHg) Temp. Sat. (mmHg) (°C) (%) (°C) (%) (°C) (%) Rest 0 34 97 91 33 96 87 34 99 96 Rest 3 34 98 92 33 96 85 34 96 94 End of exercise 38 92 108 37 97 13 Recovery 3 36 96 111 37 94 95 Recovery 6 36 96 103 105 35 96 96 34 96 91 Table 1: Skin temperature and mean arterial pressure increased during exercise and decreased during recovery. Conversely, hemoglobin saturation decreased during exercise and increased during recovery. As demonstrated by the values in Table 1, temperature, hemoglobin saturation, and mean arterial pressure increased during exercise and then gradually decreased during recovery. However, recovery mean arterial pressure and hemoglobin saturation did not reach resting levels in any of the subjects. Recovery skin temperature only reached resting temperature of one subject; the other two subjects did not regain their resting skin temperatures before the experiment ended. Discussion: As presented by the previous figures and table, not all data was collected for Subjects 2 or 3. In the future, students should be more organized to ensure that all measurements are taken at the appropriate time. Nevertheless, enough data was collected to verify that the hypothesis that heart rate, carbon dioxide clearance, and mean arterial pressure would increase during exercise and then gradually decrease after exercise ended. The subjects’ bodies first became aware of exercise by the movement of proprioceptors, which are mechanoreceptors that continuously provide information to the brain about limb position and movement (Martini et al. 502). Before the increased metabolic demands associated with exercise started, proprioceptors informed the brain of changes in physical activity, thus activating the sympathetic division of the autonomic nervous system (Martini et al. 522). The autonomic nervous system, which is responsible for regulating vital physiological processes that sustain life, controls cardiovascular and respiratory functions (Martini et al. 517). While the parasympathetic division of the autonomic nervous system is active during sedentary activity and promotes energy storage, the sympathetic division is activated when the body experiences any stressful activity, such as exercise. Activation of the sympathetic nervous system in the experimental subjects promoted increased activity in the cardiovascular and respiratory centers in the medulla oblongata of the brain. In turn, blood pressure, heart rate, breathing rate, and depth of respiration increased. The sympathetic nervous system also mobilized the subjects’ energy reserves and stimulated the breakdown of glycogen into glucose that was ultimately used to make energy through cellular respiration (Martini et al. 524). However, in order to support increased rates of cellular respiration, more oxygen was needed; thus, both respiration and heart rate increased to deliver more oxygen to the subjects’ cells. Another type of mechanoreceptor that was involved in coordinating the body’s physiologic response to exercise was baroreceptors. The primary function of baroreceptors is to monitor the blood pressure at organs and major vessels near the heart, such as the carotid artery and aorta. When the proprioceptors triggered the cardiac center to increase heart rate, the resulting increase in cardiac output put more pressure on baroreceptors. Consequently, the free nerve endings of the baroreceptors changed in shape and increased the rate of action potentials to the vasomotor center in the brain. Although the vasomotor center may have initially responded to the increase in blood pressure by temporarily increasing parasympathetic action, baroreceptors can adapt very quickly. Thus, the baroreceptors stopped responding to the continuous stimulation of increased blood pressure, and increased mean arterial pressure during exercise was observed. As demonstrated by the results of the experiment, blood pressure continued to increase while the subjects exercised. Nevertheless, the subjects’ blood pressures steadily decreased as expected towards resting blood pressure as their heart rate, cardiac output, and blood pressure decreased during the recovery period. Moreover, the termination of exercise allowed the vasomotor center in the brain to trigger vasodilation of the blood vessels to decrease blood pressure further (Heart Sounds and Blood Pressure Tutorial). Baroreceptors also play an important role in the regulation of the respiratory center in the brain. As aforementioned, exercise increased the subjects’ oxygen needs, which caused their tidal volumes to increase. Due to the increase in lung expansion, baroreceptors in the lungs signaled these changes to the respiratory center, which caused respiratory rate to change (Martini et al. 501). As expected, when more oxygenated blood travelled to body cells, the rate of cellular respiration increased, which led to increased production of heat and carbon dioxide inside the body. Due to this increase in carbon dioxide, more carboxylic acid was made and decomposed into bicarbonate and hydrogen ions. Furthermore, this influx in hydrogen ions was immediately noticed by chemoreceptors that monitor the pH of the cerebral spinal fluid that surrounds the brain. As the pH of the cerebral spinal fluid decreased due to the increase in hydrogen ions, the respiratory rate was further increased in order to increase carbon dioxide clearance from the body to prevent further decomposition of carboxylic acid (Respiratory System Tutorial). As demonstrated by the results obtained during the experiment, the original hypothesis that oxygen consumption would increase to match the body’s increased oxygen needs during exercise was also correct. Due to the increased consumption of oxygen experienced during exercise, the anticipated results that hemoglobin saturation would decrease were also accurate. As the amount of oxygen released at cells increased, hemoglobin’s oxygen saturation was forced to decrease. Nevertheless, hemoglobin saturation began to increase during recovery as more oxygen was consumed by the subjects. Hemoglobin binding is a form of positive feedback since the binding of oxygen to hemoglobin makes it easier for the next oxygen molecule to bind the protein (Martini et al. 843). It is important to understand exercise physiology in order to appreciate the beneficial effects that exercise has on the human body. Regular aerobic exercise has been shown to decrease risk for cardiovascular disease by enhancing oxygen circulation, which allows the heart, lungs, and other components of the cardiovascular system to function more efficiently. Exercise also decreases risk for cardiovascular disease by promoting increased levels of high-density lipoproteins and decreased levels of low-density lipoproteins (“Exercise: 7 Benefits of Regular Physical Activity”). Furthermore, regular exercise has been shown to delay mortality and even extend life by at least two years (Straub 176). References: Exercise Physiology, Physiology Laboratory Handout Bio 142 Spring 2013. Pages 65-74. “Exercise: 7 Benefits of Regular Physical Activity.” Mayo Clinic. Mayo Foundation for Medical Education and Research, n.d. Web. 31 March 2013. http://www.mayoclinic.com/health/exercise/HQ01676 Martini, Nath, and Bartholomew. Fundamentals of Anatomy and Physiology. 9th ed. Sanfrancisco: Pearson, 2012. Print. Straub, Richard. Health Psychology, a Biopsychosocial Approach. 3rd ed. New York, NY: Worth Publishers, 2012. Print. Waters, John. Physiology Laboratory Manual 2nd Ed: Heart Sounds and Blood Pressure Tutorial. The Pennsylvania State University. McGraw-Hill Company, Inc, 2003. Waters, John. Physiology Laboratory Manual 2nd Ed: Regulation of Cardiac and Heart Cycle Tutorial. The Pennsylvania State University. McGraw-Hill Company, Inc, 2003. Waters, John. Physiology Laboratory Manual 2nd Ed: Respiratory System Tutorial. The Pennsylvania State University. McGraw-Hill Company, Inc, 2003.