Ashish Sharma PGY
advertisement

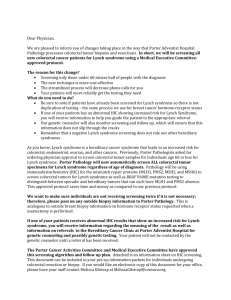
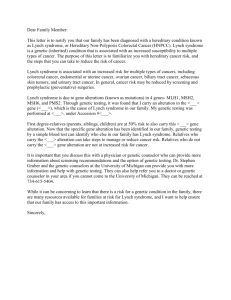
Ashish Sharma PGY-4 GI fellow Grand Rounds 12/11/14 Mentor- Milena Gould, MD Case Presentation • 31 y/o Hispanic male was seen in GI clinic as a referral for colonoscopy and EGD. • Patient referred by Genetics Clinic due to family history of hereditary colon cancer. • Denied hematochezia, melena, hematemesis, constipation, diarrhea, abdominal pain, weight loss. • PMH - GERD, asthma, obesity • PSH - None • SH – denies smoking, ETOH use, IVDA Maternal GM Maternal GF Uncle 1 Uncle 2 Aunt 1 Mother 54 Aunt 2 Colon Ca Cousins Cousins Cousin Father 55 Cousin Paternal GF Unknown Paternal GM Patient 31 Sister 38 LS LS Brother –in-law Amsterdam II criteria met Nephew 12 Brain cancer Niece Niece Cousins Case presentation • Patient’s mother underwent tumor testing and germline testing, and was found to have MLH1 MMR gene deleterious mutation consistent with Lynch Syndrome (LS). • Our patient was tested for the Known Family Mutation (KFM), and tested positive. He was diagnosed with LS. Case presentation • • • • • • GEN: No acute distress, alert and oriented HEENT: An-icteric, oropharynx clear, PERRLA, EOMI NECK: No lymphadenopathy CV: Regular rate and rhythm S1, S2 ,no m/r/g CHEST: Clear to auscultation bilaterally ABD: Obese, soft, non tender, no hepatosplenomegaly, bowel sounds present • EXT: No edema • NEURO: Grossly intact and non focal • Skin: No lesions Procedures• Colonoscopy – sigmoid diverticulosis, no polyps detected • EGD - Normal Clinical Questions 1. Diagnostic strategies in LS, and effectiveness of implementation of Universal Testing in LS 2. GI cancer surveillance in LS 3. Role of chemoprevention in LS Background • Henry T. Lynch , characterized the syndrome in 1966 and called it “cancer family syndrome”. • The term "Lynch syndrome" was coined in 1984 by other authors; Lynch named the condition Hereditary Nonpolyposis Colorectal Cancer (HNPCC) in 1985. • HNPCC is no longer used; Lynch syndrome is the preferred term. Douglas et. al. History and Molecular Genetics of Lynch Syndrome in Family G: A Century Later JAMA. 2005;294(17):2195-2202. Background • Approximately 3% of Colorectal Cancers (CRCs) are due to LS. • LS is caused by autosomal dominantly inherited mutations in the Mismatch Repair (MMR) genes MLH1, MSH2, MSH6 ,PMS2 and/or EPCAM gene. • First-degree relatives of individuals identified with a LS gene mutation have a 50% chance to carry the mutation. Douglas et. al. History and Molecular Genetics of Lynch Syndrome in Family G: A Century Later JAMA. 2005;294(17):2195-2202. Background - Definitions • What is ImmunoHistochemistry (IHC) testing? – Detects presence or absence of the protein products of MMR genes (protein carries same name as MMR gene). A missing protein suggests a mutation in gene that codes for that protein. • What is Micro Satellite Instability (MSI) testing?Detects abnormal number of microsatellite repeats, which indicates that the cancer more likely arose from cells with defective MMR genes. Umar et al. (2004). Revised Bethesda Guidelines for hereditary nonpolyposis colorectal cancer (Lynch syndrome) and microsatellite instability. J Natl Cancer Inst, 96(4), 261–268. Background – Definitions • • • • Lynch like syndrome Familial Colorectal Cancer Type X (FCRCTX) Muir Torre syndrome Turcot syndrome Giardiello et al. Guidelines on Genetic Evaluation and Management of Lynch Syndrome: A Consensus Statement by the US Multi-Society Task Force on Colorectal Cancer. Am J Gastroenterol advance online publication, 29 July 2014 Background- Colon cancer risk in LS Bonadona et al. Cancer risks associated with germline mutations in MLH1, MSH2 , and MSH6 genes in Lynch syndrome . AMA 2011 ; 30 : 2304 – 10 Background-Extracolonic cancers in LS Lynch et al. Genetics, natural history, tumor spectrum, and pathology of hereditary nonpolyposis colorectal cancer: an update review. Gastroenterology 1993; 104:1535 – 49. Diagnostic tools • Clinical criteria – Amsterdam II, Revised Bethesda Guidelines • Clinical prediction models – MMRpredict, MMRpro, PREMM (>5% cut off) • Colorectal cancer risk assessment tool • Tumor testing – MSI, IHC • Genetic testing – MLH1, MSH2, MSH6, PMS2 and EPCAM • Universal testing and Traditional testing Diagnostic tool -Amsterdam Criteria Vasen et al. 1999. New clinical criteria for hereditary nonpolyposis colorectal cancer (HNPCC,Lynch syndrome) proposed by the International Collaborative Group on HNPCC. Gastroenterology, 116(6), 1453–1456. Diagnostic tool – Revised Bethesda Guidelines Umar et al. (2004). Revised Bethesda Guidelines for hereditary nonpolyposis colorectal cancer (Lynch syndrome) and microsatellite instability. J Natl Cancer Inst, 96(4), 261– 268. Universal Testing • Definition – Tumor testing all CRCs diagnosed <70/= yrs or CRCs diagnosed in individuals > 70 yrs if they meet Revised Bethesda Guidelines. (NCCN guideline) • EGAPP working group endorses tumor testing all CRCs diagnosed. 1. Ladabaum et. Al.Strategies to identify the Lynch syndrome among patients with colorectal cancer: a cost-effectiveness analysis. Ann Intern Med. 2011 Jul 19;155(2):69-79 2. NCCN Clinical Practice Guidelines in Oncology. Version I.2014 3. Recommendations from EGAPP Working Group 2009 Traditional Testing • Selective tumor and/or germline testing. This is particularly useful when no tumor is available for testing. Giardiello et al. Guidelines on Genetic Evaluation and Management of Lynch Syndrome: A Consensus Statement by the US Multi-Society Task Force on Colorectal Cancer. Am J Gastroenterol advance online publication, 29 July 2014 MSI/IHC Testing – Interpretation NCCN Clinical Practice Guidelines in Oncology. Version I.2014 Universal Testing Algorithm May be more cost effective to perform IHC testing only Giardiello et al. Guidelines on Genetic Evaluation and Management of Lynch Syndrome: A Consensus Statement by the US Multi-Society Task Force on Colorectal Cancer. Am J Gastroenterol advance online publication, 29 July 2014 Traditional testing in affected individual or at risk family memberMutation Known Our patient was diagnosed using this approach. Giardiello et al. Guidelines on Genetic Evaluation and Management of Lynch Syndrome: A Consensus Statement by the US Multi-Society Task Force on Colorectal Cancer. Am J Gastroenterol advance online publication, 29 July 2014 Traditional Testing in at risk family member- Mutation Unknown Giardiello et al. Guidelines on Genetic Evaluation and Management of Lynch Syndrome: A Consensus Statement by the US Multi-Society Task Force on Colorectal Cancer. Am J Gastroenterol advance online publication, 29 July 2014 Diagnostic tools in LS- Diagnostic Accuracy Giardiello et al. Guidelines on Genetic Evaluation and Management of Lynch Syndrome: A Consensus Statement by the US Multi-Society Task Force on Colorectal Cancer. Am J Gastroenterol advance online publication, 29 July 2014 Colorectal cancer risk assessment toolUseful for routine use in GI clinic Kastrinos et al. Development and validation of a colon cancer risk assessment tool for patients undergoing colonoscopy .Am J Gastroenterol 2009 ; 104 : 1508 – 18 . Outcomes of effective implementation of Universal Testing in safety net hospital Key points – 1. Role of genetic team 2. Participation rate of at risk family members 1. Beamer et al. Reflex Immunohistochemistry and Microsatellite Instability Testing of Colorectal Tumors for Lynch Syndrome Among US Cancer Programs and Follow-Up of Abnormal Results. JCO April 1, 2012 vol. 30 no. 10 1058-1063 2. Marquez et al. Implementation of routine screening for Lynch syndrome in university and safety-net health system settings: successes and challenges. Genetics in Medicine (2013) Volume: 15, Pages:925–932 Clinical Questions 1. Diagnostic strategies in LS, and effectiveness of implementation of Universal testing in LS 2. GI cancer surveillance in LS 3. Role of chemoprevention in LS Cancer surveillance in LS TAH-BSO by 40 years Giardiello et al. Guidelines on Genetic Evaluation and Management of Lynch Syndrome: A Consensus Statement by the US Multi-Society Task Force on Colorectal Cancer. Am J Gastroenterol advance online publication, 29 July 2014 Evidence supporting colorectal cancer surveillance Evidence supporting gastric cancer surveillance - Majority of gastric cancers in LS are Intestinal type - However, there is no difference in the frequency of premalignant lesion in the stomach on biopsy in MMR positive versus MMR negative patients - Mallorca group strategy Clinical Questions 1. Diagnostic strategies in LS, and effectiveness of implementation of Universal testing in LS 2. GI cancer surveillance in LS 3. Role of chemoprevention in LS Chemoprevention- CAPP2 2008 1071 LS patients from 43 centers Randomized, placebo-controlled, 2 × 2 design 727 randomized to resistant starch (30 g / d) or placebo; 693 randomized to aspirin (600 mg / d) or no aspirin No effect on incidence of colorectal adenoma / cancer by starch or aspirin or both at mean follow-up of 29 months Burn et al. Effect of aspirin or resistant starch on colorectal neoplasia in the Lynch syndrome. N Engl J Med 2008; 359:2567 – 78. Chemoprevention – CAPP2 2012 918 LS patients from 43 centers Long-term follow-up report on randomized, placebocontrolled, 2 × 2 design 463 randomized to resistant-starch; 455 randomized to placebo No effect on incidence of CRC by starch at median follow-up of 52.7 months Mathers et al. Long-term eff ect of resistant starch on cancer risk in carriers of hereditary colorectal cancer: an analysis from the CAPP2 randomized controlled trial.Lancet Oncol 2012;13:1242–9. Chemoprevention – CAPP2 2011 861 LS patients from 43 centers Long-term follow-up report on randomized, placebocontrolled, 2 × 2 design 427 randomized to aspirin (600 mg / d); 434 randomized to placebo 600 mg aspirin / d for mean of 25 months reduced cancer incidence after 55.7 months Time to first CRC hazard ratio (HR) by per protocol analysis, 0.41 (95 % CI: 0.19 – 0.86; P =0.02);intention-to treat analysis of all LS cancers, HR=0.65; 95 % CI: 0.42 – 1.00; P =0.05) Burn et al. Gerdes AM , Macrae F et al. Long-term effect of aspirin on cancer risk in carriers of hereditary colorectal cancer: an analysis from the CAPP2 randomized controlled trial. Lancet 2011 ; 378 : 2081 – 7. Conclusion of Chemoprevention in LS • Mortality benefits in CRC in LS patients can be seen from longer use of aspirin (2-4 yrs), and after longer term (5-10 yrs) follow up. • Patients with cardiovascular problems benefit the most with aspirin use. • Optimal dose of aspirin for CRC prevention in LS not clear from current trials. • CAPP3 study underway to assess optimal dose and duration of aspirin to prevent CRC in LS. Rothwell et al. Effect of daily aspirin on long term risk of death due to cancer: analysis of individual patient data from randomized trials.Lancet 2011;377:31 – 41. Back to our patient • Colonoscopy 1-2 yrs • EGD 2-3 yrs (possibly every 5 yrs), check for H pylori; treat and eradicate if positive • UA every year • No aspirin for chemoprevention at this time Take home points • Use colorectal cancer risk assessment tool in clinics/endoscopy lab routinely to identify possible LS patients • Universal testing of all colorectal cancers in patients < 70 yrs of age. If the MSI/IHC is positive on tumor testing, refer to genetics • Refer to US Multi-Society Task Force Guidelines, 2014 for cancer surveillance/management in LS • Await results of CAPP3 trial before routine aspirin use for chemoprevention in LS Questions?