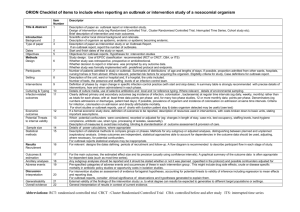
Table 5.1 Epidemiological field study: When do we investigate?
advertisement

Pan American Health Organization Pan American Sanitary Bureau, Regional Office of the World Health Organization Modules of the Principles of Epidemiology for Disease Control For the English-Speaking Caribbean Adapted Second Edition Unit 5.1:Field Epidemiology: the Study of Outbreaks MOPECD Unit 5: Epidemiologic field study 2 CONTENT AND OBJECTIVES This unit covers epidemiological field investigation as applied to local health outbreaks and epidemics. The unit presents procedures to collect data and develop information in a timely manner for the detection, characterization, confirmation, and control of outbreaks and epidemiological alert situations. The objectives of the present unit are: To recognize alert situations that require epidemiological field study To present the principles, methods, and basic procedures for epidemiological field study in the investigation of outbreaks To lay the foundation for organizing epidemiological field study at the local health level To analyze in detail the real case of an epidemiologic field study applied to the study of an outbreak in the community INVESTIGATION IN PUBLIC HEALTH Health services have expanded to not only include treatment and health promotion, but also the surveillance, prevention, and control of health problems. In the past health services only focused on communicable diseases but now often include surveillance and control programs for chronic diseases, lifestyle risk factors, genetic disorders, occupational health events, environmental risks, disabilities and many more areas of concern. The collection and analysis of data from public health surveillance systems are necessary for effective disease control. Control interventions for many emergent serious health problems often require additional information acquired through rapid focused epidemiological investigations. Identifying risk factors for risk of disease or adverse health events in the population is essential for the designing effective interventions for the prevention and control of disease or health event. In epidemiological alert situations, control measures require rapid efficient implementation to successfully suppress or eliminate sources of infection or exposure, interrupt transmission in the population and reduce susceptibility. Epidemiological field study is divided into descriptive and analytical epidemiology. These methods are used for investigating and controlling outbreaks and epidemics of Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study 3 infectious disease or other acute events. Descriptive epidemiology characterizes the disease or adverse events, the times and places of those events and the persons impacted. Analytical epidemiology generates inferences and predictions about the probable exposure and mode of transmission associated with risk of disease or health event. This information is used to plan appropriate interventions for the control of the health problem. The strength of the association between possible risk factors and disease or event, especially in outbreaks and epidemics, can provide biologically/socially plausible evidence for initiating effective control measures in the absence of laboratory confirmation. Thus, analytical epidemiology can be a driving force for successful public health action. Epidemiological field study is also used to identify why control measures may be ineffective. For example, every measles outbreak should be investigated routinely to evaluate the effectiveness of the vaccine and immunization program for measles. Generally, measures designed to control an outbreak should always be monitored for effectiveness. Epidemiological field study can sometimes conflict with socially and culturally sensitive issues in the community. Thus, the epidemiological field study should always ensure a balance between the need for rapid response and the need for responding in a sensitive and ethical manner, protecting the dignity and rights of the community. In outbreaks and emergencies, epidemiological investigations require rapid deployment. Rapid implementation of investigations leads to early interventions to protect the population. For example, prompt identification of contaminated foodstuff can prevent future cases, hospitalizations and deaths, avoid overloading health services and reduce the socio-economic costs to the community. The investigation of outbreaks is retrospective or at best concurrent. The success of a field investigation often depends on the memories and recollections of people about activities such as consumption of food, routes of travel taken and contacts. Memories fade, so data needs to be collected as soon as possible. Sometimes also, the window of opportunity for carrying out an investigation is limited to a few hours or days, especially where food or other evidence is discarded, where laboratory tests required freshly contaminated/infected samples, or where an outbreak occurs among travelers in transition. Rapid epidemiological assessment none-the-less must be balanced against conducting a careful comprehensive methodologically-sound investigation to avoid mistakes which might have serious consequences. Field epidemiologists may have to persuade local government authorities, industries, and/or the general public to take actions that may not necessarily be welcomed. Premature findings in error as a result of misleading spurious associations, biases or confounding factors negatively impact the credibility of local health team and produce ineffectual and costly interventions. Seriously mistaken findings could lead to the closure of schools and hospitals, bankruptcy of commercial establishments, labor and legal disputes, social stigma and civil disorders. The findings of epidemiological field studies can have a major impact on policy-making and the setting of safety standards on a national scale. In the Caribbean islands, outbreaks in hotels and on ships not only impact the health of the Caribbean people and island tourists, but also have negative economic Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study 4 consequences for the tourist trade. Thus care must always be taken in field investigation, balancing this with the demands of speed to resolve the problem and protect the population. The epidemiological study of outbreaks by local health teams can impact the immediate health of the community and provide opportunities for in-service training. The history of such investigations include many notable examples, from the famous study by John Snow of the cholera outbreak in London in the mid-1800’s to the more recent study of the firstrecognized Legionnaires’ disease outbreak in the United States. Both studies are found in the annex of this unit. Many epidemiological field studies are also underway in both the Caribbean countries and elsewhere to investigate emerging disease epidemics such as HIV/AIDS and remerging disease outbreaks of diseases such as dengue and malaria. There are two major design groups in epidemiological research. One is randomized trials or randomized controlled trials. Randomized trials such as clinical trials (where individuals are assigned exposures) and community trials (where communities are assigned exposure) attempt to control undue distorting influences on findings by random assignments of exposure. Clinical trials is considered the “gold standard” of epidemiological study designs but often cannot be implemented due to logistical, cost or ethical considerations. Randomized trials attempt to emulate very-controlled scientific experiment. The other study design group is observational studies. In observational studies there are no assignments of exposure to participants as there is in randomized trials; exposure status is only observed as it naturally occurs. One of the classifications of observational study designs is descriptive studies, which describe the characteristics of frequency and distribution of disease over time and space, and by person. The other classification of observational study designs is the analytical or comparative studies, which investigate determinants/risk factors of disease or health event and evaluate hypotheses (Figure 5.1). FIGURE 5.1 EPIDEMIOLOGICAL STUDY DESIGNS Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study 5 Clinical trial Therapeutic trial Prevention trial Intervention trial Field trial Randomized trial Community trial Descriptive study Case-report study Case series study Ecological study (correlation) Cross-sectional study (prevalence) Observational study Analytical study Case-control study Case-crossover study Case-cohort study Cohort study Outbreak epidemiological field studies investigate unexpected health problems that often require immediate response and timely intervention. Computer technology can support epidemiological field studies when used appropriately. As previously noted the software EpiInfo which is free as a download from the internet can be useful in the collection and analysis of outbreak data. Computerized geographic information systems (GIS) likewise can be helpful in producing maps of risk for an outbreak, among other applications. INVESTIGATION OF OUTBREAKS Local capacity to response to an outbreak in a timely manner requires that the public health surveillance system is capable of triggering an alert to investigate a potential outbreak and that the local health team has the capacity to systematically investigate and control the outbreak. This unit will cover these two areas. Any suspicion at the local level of an outbreak should be communicated immediately to the next highest health level. Communicating the suspicion that there may be an outbreak is important because: a local outbreak without early response and control could turn into a major epidemic of larger proportions and more harmful consequences, a local outbreak could be the first sign of an outbreak that is occurring in other locations and more threatening than initially believed, already extant control measures in other areas may be applied locally immediately for early control if the outbreak is identified early, and epidemiological technical assistance from higher levels can be mobilized early, including resources for epidemiological field study. Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study 6 Clusters, outbreaks, and epidemics It is important to define three related terms in alert emergency situations to have a common language for epidemiological field study and response. A cluster is an unusual concentration of cases geographically or over time. A cluster of cases would be greater in number than what would be expected by chance. A cluster of cases on investigation would be the earliest way of detecting an outbreak. In practice, the search for clusters can be based on rumors, surveillance reports, hospital or health center registries or by observations from health professionals. An outbreak is an epidemic limited geographical to one defined locality, such as a school, hospital, barracks or monastery. An outbreak is an unusual increase in the number of cases with at least two epidemiologically-related cases which appear suddenly and exhibit a localized spread in a defined area. Timely detection and response to an outbreak is an effective way of preventing a subsequent epidemic. In practice, the detection of outbreaks is a basic activity of surveillance systems and the investigation of outbreaks is a requisite for implementing timely and effective prevention and control measures at the local level. An epidemic is an “outbreak” exceeding the geographic and population limits of an outbreak, though these exceeded limits are not clearly defined. An epidemic is the occurrence of cases of disease or other health events with a greater than expected incidence for a given geographical area and time period. The expected incidence of disease varies according to the agent, the characteristics of exposed population, previous experience of exposure to the disease and the place and time of occurrence. Because acute polio due to wild poliovirus is eradicated in the western hemisphere, the incidence of even one confirmed case in the Caribbean exceeds expectations and is considered an epidemic. Unexpected increases in the incidence of disease are due an increase in the transmission of disease. Observed increases in the incidence of disease is often attributable to common cause(s) among the cases. Sometimes greater than expected increases in incidence may not be an outbreak or an epidemic. For example, changes in the case definition, notification procedures, type of surveillance (such as switching from a passive surveillance system to an active surveillance system), access to health services, or improvements in diagnostic procedures can lead to a sudden apparent "excess" of cases. Sometimes an epidemic or outbreak will not increase the overall total numbers of cases observed in the population. For example, health authorities concluded that there was no measles epidemic during epidemiological week 12 in 1992 because the number of observed cases of measles of 392 in one administrative area did not exceed the expected number of 412 for that week in that area; however, more than 65% of the observed cases (n=258) were in children older than two years-of-age, where the expected percent of cases from this age group out of the total is 14% (n=58). The epidemic of measles in this age group in this area for this week went unnoticed. Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study 7 WHEN TO INVESTIGATE The capacity to identify outbreaks requiring investigation generally depends on the ability of the local public health surveillance system to alert health teams of a problem. An investigation requires a significant investment of resources, so the decision whether to investigate should be made on set criteria. Table 5.1 offers a list of criteria to decide when to investigation. TABLE 5.1 EPIDEMIOLOGICAL FIELD STUDY: WHEN DO WE INVESTIGATE? When the disease or health event is a priority When the cases occurs more than expected When cases seem to have a common source When the health event seems to be more serious than expected When the disease is new, emerging or "unknown" in the area When the disease or health event is of public interest When the disease or health event is due to disaster When the disease or health event is a priority Health authorities sometimes prioritize diseases or health events and mandate that every reported case of a particular disease or health event be investigated. This requirement to conduct an investigation derives from general disease/event control objectives of the health system. Such disease priority lists are usually based on established national and international epidemiological criteria. Such diseases include those targeted for eradication and elimination, for which international notification is compulsory and those defined as reemerging. When cases occurs more than expected An investigation has to be made when the incidence of a disease or health event in a specific population in a given time period and geographic area is greater than expected. In general, a disease should be investigated in situations in which its frequency is greater than expected. For a specific population and time period it is also possible to detect increases in the determinants of disease, including risk behaviors and lifestyles, if the surveillance system is designed to monitor these determinants. The construction and maintenance of endemic corridors or channels and epidemic curves for diseases under surveillance helps determine when an epidemiological field study should be conducted. The identification of temporal clusters, unusual grouping of cases in Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study 8 over a short period of time, can trigger investigations of such clusters. Outbreaks are often identified early by investigating clusters of cases. When cases seem to have a common source Diseases or health events that have apparent common cause(s) should be investigated. Investigating the first occurrence of cases can lead to prompt identification and resolution of an outbreak before it grows. Prompt investigation is especially important for clusters caused by food or water borne disease and environmental toxins. Clusters may be identified by the notification by health professionals of unusual patterns of disease or health event. Clusters may also be discovered through analyses of surveillance data or morbidity reports of associations between factors such as sex, age, place of residence or work, surnames and date of onset with health event. A common date of onset of symptoms is especially suspicious. Mapping cases geographically may also reveal spatial clusters. Even rumors in the community can lead to clusters of cases, especially for outbreaks associated with social and public events. Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study 9 When the health event seems to be more serious than expected If the severity of disease increases, this should be investigated. If there is an increase in the case fatality based on the information from the surveillance system or hospitalization rates based on information from hospital records, this warrants investigation. The development of drug resistant pathogens is increasing the severity of certain diseases, thus drug surveillance systems are becoming more important. Declines in timely access to health services or therapies, or reduced quality of care can enhance the relative severity of disease in the community. Those diseases with declining severity should also be investigated. Such a decline in severity may reflect reduced quality of surveillance, thus the surveillance system and the cases should be investigated. When the disease is new, emerging or “unknown” in the area A disease that may have occurred for the first time or rarely should be investigated. Similarly, cases with clinical symptoms different from any known disease should be investigated. The majority of emerging, and re-emerging diseases should be investigated. Increasing numbers of emerging and re-emerging diseases require more sensitive health surveillance systems capable of detecting new syndromes and unexpected combinations of symptoms. Syndromic surveillance systems that monitor symptoms and combinations of symptoms are especially suited for such surveillance. Increased mobility of people and the expansion of trade of foodstuffs have globalized risks of diseases and health events. When the disease or health event is of public interest Certain health events or disease sometimes capture the attention of the public and raise concern about a particular disease or health event. Often public concern triggers a response by health authorities, leading to an investigation. When the disease or health event is due to disaster Emergencies and disasters are often accompanied by disease outbreaks due to the movement of populations and a failure of sanitary infrastructure leading to the contamination of water, curtailment of waste and refuse disposal and overcrowding. HOW TO INVESTIGATE The principal objective of an epidemiological field study is to identify the causal factors driving a disease outbreak. In general, this requires the determination of the causal agent, its Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study 10 source and mode of transmission, the population groups at greatest risk, and the exposures that predispose the population to the disease. The epidemiological field study for an outbreak has two objectives: 1) to describe the outbreak, determining the source and mode of transmission and identifying the individuals at risk. Hypotheses of risk associations are developed to support early rapid deployment of control measures and 2) to analyze associations for source, mode of transmission, risk factors, and major exposures with disease and to test hypotheses. Analysis compares groups of cases and healthy people to identify and quantify strengths of the association between exposures and risk of disease. Findings are used to fine-tuned control measures. The steps for epidemiological field study steps of outbreaks are as follows: TABLE 5.2 STEPS OF AN EPIDEMIOLOGICAL FIELD STUDY 1. Confirm the outbreak 2. Organize the field work 3. Establish an operational case definition 4. Carry out active case-finding 5. Characterize the outbreak in time, space, and person 6. Generate hypotheses for immediate deployment of control measures 7. Evaluate hypotheses and conduct analytical field study 8. Implement specific control measures 9. Evaluate the control measures 10. Prepare a technical report on the field study 1. Confirm the outbreak Confirming an outbreak requires 1) verification that the diagnosis of cases is accurate and 2) determination that the incidence rate of these cases is higher than expected. For diagnostic verification medical and laboratory records of the reported cases must be reviewed. A frequency table of symptoms and signs should be constructed and used to identify laboratory testing requirements to verify future cases and for excluding some reported cases from the case count. Once the clinical signs and symptoms and laboratory findings for cases have been defined and the final case count is completed, it must be determined if the observed Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study 11 incidence rate of disease exceeds the expected incidence rate to qualify as an outbreak. This analysis must also compare observed and expected incidence rates within subpopulations, such as specific age-groups or those residing in specific localities, and not only for the total number of cases. FIGURE 5.1 TYPHOID ENDEMIC CHANNEL 1989-1999 AND EPIDEMIC CURVE FOR 2000 IN COUNTRY X 70 60 case notifications 3rd Quartile 50 40 Median 30 1st Quartile 20 10 0 J F M A M J J A S O N D months Figure 5.1 displays a typhoid endemic corridor the epidemic curve for country X. This graph can be used to determine if observed incidence exceeded expected incidence and whether we have an outbreak/epidemic. Given that cases are already verified, from June to at least September 2000 there is an apparent outbreak/epidemic that warrants investigation. The possibility that observed incidence rate increases are due to factors other than true increases in disease counts need to be considered and excluded before concluding that this is a true outbreak/epidemic. 2. Organize the field work The local health team should plan the field work with attention to three requirements: Administrative needs. Adequate contact and coordination should be established with the health, political and civil authorities of the community. As needed, their active cooperation can be enlisted. Logistic needs. Field coordination should ensure the provision of minimum resources, organize people, distribute tasks properly and supervise the general execution of the field work. Technical needs. Pertinent technical information should be available, including reported data, demographic information, maps, standard questionnaires, outbreak investigation procedures manual, relevant clinical and laboratory information, and statistical and epidemiological technical assistance. Prior to implementation of the investigation, it is important to ensure a adequate supply of laboratory supplies for the verification of cases, including material for the collection, Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study 12 storage, and transportation of biological samples and for data processing and analysis. If investigation includes For any investigation conducted with healthy individuals and cases, the survey form should be standardized and previously field-tested. Confidentiality and security of the data collected should be guaranteed. The local health team should always be previously prepared to respond to outbreaks, epidemics and emergencies. Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study 13 Exercise 5.1 Analyze the information contained in Figure 5.2 and then answer the following questions. FIGURE 5.2 INCIDENCE RATE OF HIV INFECTION FOR WOMEN IN COUNTRY B IN 2000 incidence per million New HIV-Identified Cases per Million 30 25 20 15 10 5 0 1 4 7 10 13 16 19 22 25 28 31 34 37 40 43 46 49 52 Epidemiological epidemiologic Week weeks Question 1. Based on the information on the graph above, do you think that an epidemic of HIV infection started in the female population of country B in 2000? Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study 14 Question 2. In mid-month May 2000, the national office for the prevention and control of AIDS in country B announced a program promoting HIV-testing among pregnant women with the free distribution of antiretroviral treatment to every woman in this program testing HIV-positive. With this new information, do you think that an epidemic of HIV infection started in the female population of country B in 2000? Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study 15 3. Establish an operational case definition The third step in field study of outbreaks is to establish a case definition. A case definition for investigating outbreaks frequently differs from the definitions routinely used in the public health surveillance system. Case definitions used in field work are also subject to modifications. A case definition is a standard criteria used to classify a suspected case as a case or not. A case definition should be used systematically and uniformly to find additional cases and to ascertain the true magnitude of the outbreak. In general, the operational case definition includes the following criteria: Clinical criteria: the symptoms and signs of the disease most frequently observed in reported cases. These criteria can include the sequence with which the symptoms appear and their average duration. Laboratory criteria: the biochemical, pathological or microbiological test results of infection or disease for the verification of reported cases. Epidemiologic criteria: the distribution of reported cases over time, geography and by person and characteristics of the agent, host and environment. Inclusion/ exclusion criteria for being a case may be based on the incubation period, probable exposure period, contact with index case and secondary cases, common source, type of exposure and restriction to a defined time period and geographic area. The study of the outbreak of Legionnaires’ disease (see annex) offers an example of a case definition. As an example, the investigators of the Legionnaires’ disease outbreak (see annex) decided on a case definition with clinical criteria and epidemiological criteria. The clinical criteria included having an onset of symptoms between l July and 18 August of 1976, a fever of 39C or higher and a dry cough, or fever and pneumonia confirmed by a chest x-ray. Because this clinical definition was not very specific, with criteria symptoms typical of viruses, bacteria, rickettsiae, fungi and chemical toxins, epidemiological criteria restricted cases to persons having attended the American Legion Convention or to having been present in the Bellevue Stratford Hotel, headquarters of the convention and principal meeting site, after l July 1976. The case definition should be simple and clear. The sensitivity and specificity of the case definition should also be adequate for study purposes. Sensitivity is the capacity of the case definition (or test) to correctly identify true cases out of all true cases and is presented as a percent. It is calculated as the number of true cases identified by the case definition divided by all true cases (identified and not identified) multiplied by 100% to change to a percent. Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study 16 Specificity is the capacity of the case definition (or test) to correctly identify non-cases out of all true non-cases and is also presented as a percent. It is calculated as the number of true non-cases identified by the case definition divided by all true non-cases (identified and not identified) multiplied by 100% to change to a percent. Once the case definition is established it should be used equally and uniformly to investigate the outbreak in all the people under investigation. Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study 17 Exercise 5.2 Table 5.3 shows the frequency of signs and symptoms of the 46 cases of an acute disease initially reported to a local health center. All the cases turned out to be foreign health professionals who had attended a technical meeting of the national program for the control of leishmaniasis that was held at a nearby rural hotel complex. The meeting hosted 192 participants, lasted five days and was closed-door. The study of the outbreak eventually identified a total of 108 cases and implicated the consumption of a ham and cheese sandwich offered during the afternoon break on the second day of the meeting. The causal agent in the outbreak was identified as staphylococcal bacteria. TABLE 5.3 OUTBREAK OF STAPHYLOCOCCAL POISONING (N=46) Symptoms Nausea Vomiting Diarrhea Abdominal pain Intestinal bloating Headache Tenesmus Chills Thirst Dizziness Mucus in stools No. of cases 46 44 32 29 18 13 12 10 9 4 1 Question 1. What was the attack rate of the disease based on the local health center data? What was the attack rate of the disease based on the outbreak study findings? Question 2. Using the information available, what case definition would you propose? Compare your proposed case definition with those of the other members in the group and establish a case definition by consensus. Individual: Group: Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study 18 4. Carry out active case-finding If the outbreak has already been verified, the local team is already organized and an operational case definition has been established, the next step is to search for cases, which involves field work. To effectively find cases, an intensive focused surveillance system is necessary. Such a surveillance system may include switching from passive surveillance to active surveillance, expanding the frequency and means of reporting (such as daily telephone calls) and using case and contact investigation cards. Case-finding methods vary depending on the disease being investigated and the local setting. In general, outbreaks target certain groups more than others, so case-finding can be relatively focused on higher risk groups. Active case-finding through physicians, laboratories, hospitals, schools, factories or public media can locate many unreported cases. However, more intensive efforts are sometimes required to locate cases, including serological surveys, door-to-door interviews and surveys for professional health workers. Regardless of the method chosen, the local team develops an effective system for case finding and reporting during the investigation of the outbreak. 5. Characterize the outbreak in time, place, and person Time An epidemic curve is an effective presentation of an outbreak over time. Important characteristics of an outbreak to be measured over time include the duration of the outbreak, the nature of the outbreak, and the probable exposure period. The duration of an outbreak or epidemic depends on the following factors: The speed of the outbreak as it relates to infectivity of the agent and mode of transmission The size of the susceptible population The intensity of the exposure of the susceptible population The incubation period of the disease The effectiveness of the deployed control measures Figure 5.3 presents the epidemic curve of a rubella outbreak with 37 cases that occurred between the 21st and 29th of June, with a duration of 9 days. Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study 19 FIGURE 5.3 EPIDEMIC CURVE FOR A RUBELLA OUTBREAK, 10 9 Number of Cases c asos 8 7 6 5 4 3 2 1 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 días Days of June Mes de junio Duration Days duración == 99 días The nature of outbreaks/epidemics include: Epidemics with a common source are outbreaks where the source of exposure is the same for all persons at risk for disease. The common source of infection can be a singleexposure or continuous-exposure. In single-exposure common source or explosive epidemic, exposure is to a common source during a very brief moment in time, such as an exposure to contaminated food served at a social event or luncheon. The time of exposure to the onset of symptoms for median case is the median incubation period for this disease. (Figure 5.4). In a continuous-exposure common source outbreak, the duration of exposure to the common source is prolonged and can even be intermittent for persons exposed, such as the exposure to fecal contaminants in water supply networks. Person-to-person or propagated epidemics are where transmission of disease is from person to person (Figure 5.5). Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study 20 FIGURE 5.4 EPIDEMIC CURVE FOR A SALMONELLA SINGLE-EXPOSURE COMMON SOURCE OUTBREAK 20 18 Number of Cases cases 16 14 12 10 8 6 4 2 0 11 10 9 8 7 6 5 4 3 2 1 14 13 12 15 (August) Days days in August FIGURE 5.5 EPIDEMIC CURVE FOR A VIRAL HEPATITIS A PERSON-TOPERSON OUTBREAK 14 Number casos of Cases 12 10 8 6 4 2 0 7 JUN 21 June 5 19 JUL July 2 16 AGO Aug 30 13 27 Sept 11 25 Oct 8 22 Nov 6 20 DIC Dec 3 17 ENE Jan 31 14 Feb 28 14 Mar 28 11 25 Apr Semanas Weeks Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization May MOPECD Unit 5: Epidemiologic field study 21 In single-source common-exposure epidemics the median incubation period is the period of time from exposure to the median onset of symptoms. If the median incubation period is known for the disease from prior sources, this can be used to quickly estimate the probable exposure date to the causal agent of the outbreak by subtracting the time of the median incubation period from the peak of the epidemic curve. Figure 5.6 illustrates this method with the outbreak of rubella described, where the median incubation period of 37 cases was 18 days. FIGURE 5.6 RUBELLA EPIDEMIC CURVE WITH PROBABLE DATE OF EXPOSURE fecha probable de exposición 10 9 Date of Probable Exposure Numberc asos of Cases 8 7 6 5 4 3 2 Peak of pico del brote Epidemic Curve 18 días periodo de incubación Median Incubation Period = 18 Days 1 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 días Days Duration=9 duración = 9 Days días For a single-source common-exposure outbreak the probable exposure period to the causal agent during an outbreak is estimated using the range of the incubation period, available from published sources. The probable exposure period is computed by subtracting the minimum incubation period from the date of the occurrence of the first case of the outbreak and then subtracting the maximum incubation period from the date of the occurrence of the last case of the outbreak. The range of dates between these two limits is the probable period of exposure to the causal agent. Figure 5.7 illustrates this method with the rubella outbreak, with the range of the incubation period of rubella from 14 to 21 days. This method doesn’t apply to outbreaks with person-to-person transmission. Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study 22 FIGURE 5.7 RUBELLA OUTBREAK, EPIDEMIC CURVE PROBABLE PERIOD OF EXPOSURE 10 Number of Cases casos 9 8 21Maximum días: máximo Incubation Period = periodo de incubación 21 Days Probable periodo Exposure probable Period de exposición 7 Minimum Incubation Period = 14 días: mínimo periodo14 de Days incubación 6 5 4 3 2 1 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 Days in June días Duration= 9 Days The probable exposure period in Figure 5.7 corresponds to June 7th and duración = 98th. días Junio Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study 23 Exercise 5.3 Figure 5.8 shows the epidemic curve for a leptospirosis outbreak. A total of cases were reported during the outbreak. Based on this information, compute the duration of the outbreak and estimate the probable period of exposure to the causal agent. Leptospirosis has a range of reported incubation periods of 4 to 19 days. Answer the following questions and then discuss them with your group. FIGURE 5.8 THE EPIDEMIC CURVE FOR A LEPTOSPIROSIS OUTBREAK AT SITE X ON APRIL 2000 20 cases 16 12 8 4 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 days (April, 2000) Question 1. The duration of the outbreak was: ____________ Question 2. The probable exposure period was: ______________ Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study 24 Figure 5.9 shows the epidemic curve for an outbreak of meningococcal meningitis in the pediatrics ward of hospital M during the month of May 1999. There were nine cases. Based on this information, establish the duration of the outbreak and estimate the probable period of exposure to the causal agent. Meningococcal meningitis has a range of reported incubation periods of two to 10 days (range = eight days). Answer the following questions and then discuss them with your group. FIGURE 5.9 THE EPIDEMIC CURVE FOR MENINGOCOCCAL MENINGITIS HOSPITAL M FOR THE MONTH OF MAY 1999 5 4 cases 3 2 1 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 days (May, 1999) Question 3. The duration of the outbreak was: ________________ Question 4. The probable exposure period was: ________________ Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study 25 Place or Space Place in an outbreak is the geographical/spatial distribution of case counts, incidence rates and case characteristics. This information defines the geographical limits of the outbreak and clarifies the etiology, exposure, and spread of disease. Place can include the site of occurrence of the cases, the place of residence, workplace, the relevant geographical features geographical (such as rivers, spillways, wells, landfills, the neighborhoods), distance to health services and the place of medical care. Place descriptive information can be presented on tables such as table 5.4, on a bar chart such as figure 5.10, or on a map such as figure 5.11. TABLE 5.4: INCIDENCE RATE OF LEGIONNAIRES’ DISEASE BY LOCATION OF LODGING Location of Lodging Hotel A Hotel D Hotel E Hotel F Hotel G Another hotel Residence Unknown Total Number of Cases Number of Hosts Attack Rate (%) 75 21 19 12 4 7 8 3 1,161 1,046 403 312 104 210 294 153 6.5 2.0 4.7 3.8 3.8 3.3 2.7 2.0 149 3,683 4.0 On maps cases are often marked as points by hand or by using computer programs like EpiMap (EpiInfo) or more sophisticated programs like ArcView. Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study 26 FIGURE 5.10 TYPHOID OUTBREAK CASE DISTRIBUTION BY PARISH incidence per 100,000 inhabitants 0 10 20 30 40 50 60 70 80 90 100 San Andrés San Jorge Victoria Caroni San Patricio Nariva-Mayaro Maps with plotted cases help identify clusters and provide evidence for common sources of infection and risk exposures which can lead to the rapid deployment of control measures. The classic example of such application, shown in figure 5.11, was by John Snow to study and control the cholera epidemic in London between 1849 and 1854 (see annex). FIGURE 5.11 DEATHS FROM CHOLERA AND WATER SOURCES, SOHO, LONDON IN 1855 Commercial water pumps for domestic water use Cholera deaths Source: Snow J, 1885. Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study 27 Person Person includes the distribution of cases by relevant case characteristics. The following tables (tables 5.5 and 5.6) provide the distribution of cases by sex and age groups: TABLE 5.5 TYPHOID FEVER OUTBREAK DISTRIBUTION OF CASES BY AGE Age (years) Cases Population Attack Rate (per 100,000) 0-4 5-9 10 -14 15 - 19 20 - 29 30 - 39 40 - 49 50 - 59 60 and older Total 4 44 58 10 3 5 3 0 1 148,300 152,200 131,050 105,200 156,050 109,550 89,250 69,650 59,300 2.7 28.9 44.3 9.5 1.9 4.6 3.4 0.0 1.7 128 1,020,550 12.5 TABLE 5.6 TYPHOID FEVER OUTBREAK DISTRIBUTION OF CASES BY SEX AND AGE Age (years) Males Cases Population Females AR Cases population (per 100,000) AR (per 100,000) 0-4 5-9 10 -14 15 - 19 20 - 29 30 - 39 40 - 49 50 - 59 60 and older 1 19 18 5 1 1 1 0 1 75,150 77,550 65,800 52,900 76,600 55,400 43,950 35,750 27,050 1.3 24.5 27.4 9.5 1.3 1.8 2.3 0.0 3.7 3 25 40 5 2 4 2 0 0 73,150 74,650 65,250 52,300 79,450 54,150 45,300 33,900 32,250 4.1 33.5 61.3 9.6 2.5 7.4 4.4 0.0 0.0 Total 47 510,150 9.2 81 510,400 15.9 Not only are numerator data important for the calculation of rates, but population-at-risk data for the denominator is also essential. 6. Generate hypotheses for immediate deployment of control measures Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study 28 Generating hypotheses for immediate response is based on the synthesis of available evidence. We have two sources for this evidence: General medical information on the disease or health condition that could be causing the outbreak. Descriptive epidemiological information on the time, place and person of the outbreak. The hypotheses (plausible conjectures or provisional explanations) should attempt to resolve the following: The probable source of the causal agent of the outbreak The probable mode of transmission in the outbreak The exposure associated with a greater risk of developing disease These hypotheses should lead directly to provisional control measures for immediate deployment. Such control measures should target the removal, isolation, suppression, elimination, or correction of the suspected common source. Where transmission is personto-person and the agent is highly pathogenic or virulent, control measures should focus on cases and the protection of susceptible persons. 7. Evaluate hypotheses and conduct analytical field study Epidemiologists compare population groups to determine underlying determinants for developing diseases or health events, translating into effective control measures and health interventions. During most outbreaks more information is needed than can be provided by surveillance. To fill this knowledge gap, an epidemiological analytical study design called case-control is often conducted during outbreaks. A case-control study design compares outbreak cases with a usually easily accessible population of healthy people in the vicinity. These epidemiological studies can rapidly produce findings leading to the protection of the community health and the effective planning of health authorities. They also provide stimulating opportunities for in-service training of local health teams. The case-control study requires the selection of two groups, a case group who have the disease and a control group without the disease. The history of exposure to the source(s) of disease and suspected risk factors are investigated in both cases and controls using a standardized questionnaire. The results can be arranged in 2x2 tables, one table for each source and suspected risk factor. Thus the prevalence of exposure in both groups for each of the exposures and suspected risk factors are compared. If a suspected factor is associated with the outbreak, then the prevalence of exposure to this factor will be higher in cases (people with disease) than in controls (people without disease). In case-control studies the odds ratio (OR) is the measure of the strength of association between the exposure and disease, and the statistical significance of the association can be tested using the chi-square statistic. Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study 29 To conduct a case-control study, cases, controls and suspected risk factors must be selected by the investigator. Cases should be verified using the case definition for the investigation. Cases and controls should be comparable in factors that are not under study. For comparability, controls should be representative of the population from where the cases derive. It is important that all study factors be measured in the same way for both cases and controls. The number of suspected risk factors included in the study should be kept to a necessary minimum for testing the hypotheses. The selected study factors and their categories should have been field-tested prior to use and operational definitions of each should be included with the study survey. This survey form should be field-tested before being used with cases and controls. A basic analytical tool for case-control studies is the 2x2 table. These case-control study tables have the following components (Table 5.7): TABLE 5.7 CROSS-TABULATION TABLE FOR A CASE-CONTROL STUDY Case Control Exposed a b a+b Not Exposed c d c+d a+c b+d n a = number of exposed cases b = number of exposed controls c = number of unexposed cases d = number of unexposed controls a + c = case total b + d = control total a + b = exposed total c + d = unexposed total n = a + b + c + d== total cases and controls For case-control studies, the prevalence of exposure of the cases and the controls are compared: a Prevalence of Exposure in the Case Group = ac Prevalence of Exposure in the Control Group = Second Edition, MOPECD 2001 b bd Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study 30 If the suspected factor is a true risk factor, then the prevalence of exposure to this factor will be higher in cases than in controls. The statistical significance of the association between exposure and disease is determined with the chi-square test: χ 2 n.(ad bc) 2 (a c).(b d).(a b).(c d) If this statistic is greater than 3.84, then the null hypothesis is rejected and it is concluded that there is an association between exposure and disease, with statistical significance lower than 5%. The odds ratio (OR) is computed as the ratio of cross-products in the 2x2 table: OR ad bc The odds ratio (OR) is the measure that we can calculate for case-control studies and is a good estimate of the relative risk for rare diseases (prevalence<10%). An OR= 1 indicates that there is no association between exposure and disease; an OR greater than 1 indicates an association between exposure and increased risk, and an OR less than 1 indicates a protective association between exposure and risk of disease. Let us consider the following example. During the second week of an outbreak of listeria infection the possibility that exposure to unpasteurized butter was a determinant of the outbreak was examined. A case-control study was conducted with 40 cases and 120 selected controls of the community. The results were the following: Exposed Not Exposed Case 31 Control 61 9 59 40 120 92 68 160 Prevalence of Exposure in Case Group: 31 100 77 .5% 40 Prevalence of Exposure in Control Group: 61 100 50 .8% 120 As an example, to explore the association between unpasteurized butter and listeria infection we design a case-control study with the following results (listeria infection is rare): Using the chi-square statistic we have Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study X2 31 160 [(31 59 ) (61 9)] 2 8.73 40 120 92 68 Because 8.73 is greater than 3.84, we conclude that there is a statistically significant association between exposure to the unpasteurized butter and the presence of listeria infection (p<0.05). The odds ratio between exposure to unpasteurized butter and the listeria infection is: OR 31 59 3.3 61 9 In short, the case-control study found a statistically significant association between the consumption of unpasteurized butter and the presence of listeria infection; furthermore, the group who consumed unpasteurized butter had approximately 3.3 times the risk of developing listeria infection compared those that did not consume the unpasteurized butter. Outbreaks in confined quarters such as hotels, ships, hospitals, schools and barracks occur with relative frequency. Outbreaks often occur in social activities where exposure to a single common source is suspected, usually a contaminated food. In such situations where the entire at-risk population is well-defined, a cohort study can be readily used for the investigation. For a cohort study of outbreaks, a standardized survey is applied to the entire population at risk (sick and not sick) to determine history of exposure to each suspected risk factor. Then the attack rates between exposed and unexposed groups for different exposures are compared. The exposure with the largest attack rate in the exposed will often be the source of illness. The following is a 2x2 table for cohort studies: TABLE 5.8 CROSS-TABULATION TABLE FOR A COHORT STUDY Cases Non Cases Exposed a b a+b Not Exposed c d c+d a+c b+d n a = number of exposed cases b = number of exposed non-cases c = number of not exposed cases d = number of not exposed non-cases a + b = total exposed c + d = total not exposed Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study 32 a + c = total number of cases b + d = total number of non-cases n = a + b + c + d== total number of exposed and not exposed Cohort studies compare attack rates in people exposed and not exposed: Attack Rate among Exposed People = Attack Rate among Not Exposed People a ab = c cd If the exposure is a risk factor for disease, then the attack rate or incidence rate will be higher in the exposed people than in the not exposed people. The statistical significance of the association between exposure and disease can be tested with the chi-square test. The measure of the strength of association for a cohort study is the relative risk (RR), the ratio of the incidence rates of exposed persons to unexposed as follows: RR a/(a b) c/(c d) Using the outbreak example in Exercise 5.2, we have 192 participants at a technical meeting with information collected using a survey on what foods they consumed during the first three days. The results for the ham and cheese sandwich served during the afternoon break on the second day of the meeting are presented below: Case Exposed Not exposed 89 Noncase 23 19 61 108 84 112 80 192 Attack Rate among Exposed People= 89 100 79 .5% 112 Attack Rate in Not Exposed People= 19 100 23 .8% 80 To determine the statistical significance of the association between eating the sandwich and diarrhea we use the chi-square statistic, as follows: Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study χ2 33 192 [(89 61) (23 19 )]2 58 .86 108 84 112 80 Because 58.86 is much greater than 3.84 (p<<.05), we conclude that there is a statistically significant association between exposure to the ham and cheese sandwich and the presence of acute diarrheal disease. The strength of this association is measured by the relative risk as follows: RR 79 .5% 3.3 23 .8% Findings indicate that the group who consumed the sandwich had 3.3 times greater risk of developing diarrhea than those who did not eat it. 8. Implement specific control measures All available evidence should be considered to plan final control measures, including information on outbreak characteristics and the effectiveness of the earlier control measure. Sources of disease should be removed, isolated, suppressed or eliminated. In person-toperson transmission, control measures should be directed toward patients and the protection of susceptible persons, such as immunization, treatment, and prophylaxis. Health education and promotion campaigns can be very effective in control and prevention of future outbreaks and epidemics. 9. Evaluate the efficacy of the control measures The epidemiological field study should also monitor and evaluate control measures. We should continue surveillance of disease as an outcome measure of evaluation, being especially watchful for modifications in disease patterns. Control measures can be evaluated by comparing observed disease patterns and trends with expected disease patterns and trends if control measures were effective. 10. Prepare a technical report of the field study During the investigation and implementation of control measures for the outbreak, valuable information is generated. The health team involved in the outbreak is advised to synthesize this information into a consistent, understandable, and convincing technical report that documents the process and its context. The technical report is an instructional document disseminated to agencies and institutions responsible for public health. It is an ideal teaching tool. The technical research report should include an introduction and background, justification, materials and methods, results, discussion, recommendations, control measures, and references. It should communicate the results in a scientifically objective way Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study 34 using clear and convincing language and justify the appropriate recommendations for action. The technical report can also serve as basis for the publication of a scientific article to contribute to the knowledge of epidemiology and public health. It also serves as a guide for presentations and summaries for local authorities, press and the general public. This Unit is accompanied by the Comprehensive Exercise in Epidemiologic Field Study: “Outbreak of icteric disease in a rural area” Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study 35 Unit 5.1:Field Epidemiology: the Study of Outbreaks Annex: Supplementary Readings Complementary Reading No. 1: Classic methods in epidemiological research Cholera Epidemic in London John Snow (1813-1858) Adapted from: Terris M. Bank of epidemiology exercises; New York Medical School, 1967. The problem Cholera was not recognized outside of India until almost 1820 when it spread widely throughout the world, causing numerous epidemics. One such cholera epidemic occurred at the end of August in 1854 in a subdistrict of the city of London. As a result of thorough study, John Snow formulated a hypothesis of the transmission of disease and produced recommendations for its control. Below is an extract of the classic and fascinating monograph of Snow “On the Mode of Communication of Cholera”, second edition, 1854 (Snow on Cholera. The Commonwealth Fund, New York, 1936), which allows the reader to see how Snow compiled evidence and how it was evaluated. “...A long time would be needed to report the advance of cholera in different parts of the world, in some of which it produced great devastation, while it passed lightly through others, and even left some untouched. Unless this account could be accompanied by a description of the physical conditions of the places and the habits of the people, which is impossible, it would be of little use to attempt this. However, there are certain circumstances related to the progression of cholera that can be established as general rules. Cholera spreads through the major routes of transit, never as rapidly as people do, but almost always more slowly. Its exact route between one town and another cannot always be mapped, but it never has appeared in places where it could not have been taken by the movement of people.” Person-to-person transmission “There are also countless examples that convincingly show the transmission of cholera by individual or unique cases; these examples are free of any source of error, as will be seen below. I went to take reports on the death of the wife of a worker that occurred at New Leigham Road, Streatham. I knew that one of her sons had traveled to its house afflicted with an intestinal disease, of which he died one or two days later, on 18 August. His mother, who had attended him, began to feel ill the next day and died one day later, on 20 August. During the disease of the lady, whose family name was Barnes, her mother (who lived in Tockwith, a healthy community five miles from Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study 36 Moor Monkton) was called to care for her. She arrived at house of her daughter and remained for two days caring for her and washing her linens, after which she returned to Tockwith in apparently good health. However, while on the road she became ill and collapsed. She was transported home and placed in bed beside her husband; he and a daughter who lived with them acquired the disease and all three died in the course of two days. A nurse who attended the patient became ill and died when she returned to her house, near Everton. The nurse who attended her also was attacked and died. No case had occurred beforehand in that neighborhood and none appeared in the next fifteen days.” “In addition to the aforementioned facts, which demonstrate that cholera is transmitted from one person to another, there are others that show: first, that living with a patient in the same room and attending the patient does not necessarily expose the person to the action of the morbid poison; and second, that it is not always an indispensable requisite that the person come very close to the patient to be attacked, because the morbid matter can be transmitted over a distance. If it is accepted that cholera is a contagious or communicable disease, it should spread through the effluvia that emanate from the patient into the air that surrounds the patient and penetrating the lungs of those who inhale them. This assumption has produced very contradictory opinions about the illness. However, by reflecting a little we can see that we do not have the right to limit the ways by which a disease can spread, since the communicable diseases of which we have correct knowledge spread in very different ways, as occurs with pruritus and other diseases of the skin, syphilis, and intestinal parasitic infestations, all which have ways of spreading that differ from each other.” Spread of the morbid material through the digestive tract “Considering the cholera pathology, it is possible to find the way in which it is transmitted. If it started with fever or any other general symptom, we would not obtain any clue about the route of entry of the morbid substance into the organism; it could enter by the digestive tract, lungs, or in some other form; however, this point must be determined by circumstances unrelated to the pathology of the disease. From all that I have been able to learn about cholera, both by personal observation and from the descriptions of other authors, I can state that cholera starts invariably with disorders of the digestive system that often are preceded by only mild malaise, which makes the patient not realize the danger that he is running, or to consult, or to request advice about his health until the disease is already very advanced. In truth, there are few cases that present dizziness, intense weakness, and general abatement before the gastrointestinal discharges appear. However, there is no doubt that these symptoms depend on exudation from the mucous membrane, which immediately is abundantly evacuated. In all cases of cholera that I have attended, the loss of fluids from the stomach and intestine was sufficient to produce collapse; the previous general condition of the patient should be taken into account together with the abrupt appearance of fluid loss and the fact that absorption processes seem to have been suspended.” “We have seen that cholera starts as a disease of the digestive tract, and that at the beginning of the disease, the blood is not under the action of any poison; as a result, it can be thought that the material or morbid substance that produces the disease penetrates the organism by the digestive tract, being swallowed accidentally by people who would not swallow it purposely; the increase of this morbid substance or poison must then be carried out in the stomach and intestine. It would seem that when the aforementioned poison is produced in sufficient quantity, it acts as an irritant for the gastrointestinal mucous membrane; or, what is more likely, by removing fluid from the circulating blood of the capillaries by a mechanism analogous to that which the epithelial cells of Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study 37 several organs use to absorb different secretions in the healthy body. Since the morbid substance of cholera has its own way of reproducing, it must have a structure similar to that of a cell. This viewpoint is not contradicted by the fact that the cholera poison cannot be recognized by microscope, since the materials of chickenpox and chancre can only be recognized by their effects, and not by their physical properties.” “The time elapsed between the entry of the morbid substance into the organism and the beginning of the disease is called the incubation period, which is actually the period of reproduction of the morbid substance; thus, the disease results from the action of a small quantity of poison initially introduced. In cholera, this incubation or reproduction period is much shorter than in other epidemic or communicable diseases. Such a short incubation period, as well as the amount of morbid substance transported in the feces, means that sometimes cholera spreads with a speed unknown in other diseases.” Cholera near the Golden Square “The most terrible outbreak of cholera that has occurred in this kingdom is probably the one that appeared on Broad Street (Golden Square) and contiguous streets a few weeks ago. Within 250 yards of the place where Cambridge Street joins Broad Street, 500 fatal cases of cholera occurred in a period of ten days. Such a high mortality in such a small area had never occurred in the country, not even in the time of the plague; its appearance was very fast and a large number of cases died within a matter of hours. The mortality surely would have been greater if the population had not fled. The first ones to escape were those who lived in inns, followed by those of other houses; they abandoned their furniture and household effects that they had moved after finding a place where to store them. Many houses were closed upon the death of their owners and a large number of merchants sent their families away; thus, in less than six days after the onset of the outbreak, the streets most attacked were deserted, with only one fourth of their inhabitants.” ”There were a few cases of cholera on the last days of August among the neighbors of Broad Street (Golden Square); the outbreak that started on the night between 31 August and 1 September was, as in similar examples, only a violent increase of the disease. As soon as I learned about the existence and spread of cholera, I thought about the contamination of the water from the pump most frequented on Broad Street, which is located near the corner with Cambridge Street; but upon examining the water on the afternoon of 3 September, I found so few impurities of an organic nature that I refused to draw that conclusion. However, later research demonstrated to me that there were no other circumstances or common agents that could explain the rapid increase confined to a certain locality and not disseminated to others, except for the water from the aforementioned pump. I also found that the amount of organic impurities in the water in the form of white particles, which were visible to the naked eye when examined closely, varied on the next two days; this suggested to me that at the beginning of the outbreak, the water was even more impure. I decided to request permission from the General Office of Registry to prepare a list of all those dead from cholera in the subdistricts of Golden Square—Berwick, St. Ann, and Soho—during the week that ended on 2 September, and was kindly given permission. In the three subdistricts, 89 deaths were registered during that week; of these, only 6 occurred on first four days of the week and 4 on Thursday, 31 August; the remaining 79 occurred on Friday and Saturday. Thus, I had to assume that the outbreak had started Thursday and I carefully investigated the 83 deaths that occurred on the last three days of the week.” ”Examining the area, I found that almost all the deaths had occurred in the houses close to the Broad Street well, and that only l0 deaths had occurred in houses closer to the wells of other Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study 38 streets. In 5 of these cases, the relatives of the dead informed me that they always fetched water from the well on Broad Street because they preferred it, despite having other wells closer to their households. Another 3 of these cases were children who attended school close to the well mentioned; in 2 of them it was confirmed that they drank this water and the parents of the third child thought that their child also drank it. The other 2 deaths that occurred in the district distant from the well mentioned represented the mortality from cholera that occurred before the outbreak started. Upon reviewing the deaths that occurred in the vicinity of the Broad Street well, they informed me that 61 of those who died took water from the aforementioned well, either regularly or occasionally. In 6 cases I could not obtain any information about this point because the people connected with the death had gone elsewhere; in another 6 cases I found that the people who died had not taken water from that well before becoming ill. The investigation demonstrated that there was no increase or other cholera outbreaks in this part of London, except in people who had the habit of taking water from the well mentioned.” “On the afternoon of Thursday, 7 September, I had a meeting with the Council of Guards of the jurisdiction of St. James and I described and explained the circumstances. As a result of what I told them, they removed the pump handle from the well the next day. The Table shows the chronologic features of this terrible cholera outbreak:” “date August 19 20 21 22 23 24 25 26 27 28 29 30 31 September 1 2 3 4 5 6 7 8 9 10 No. of fatal cases 1 1 1 0 1 1 0 1 1 1 1 8 56 143 116 54 46 36 20 28 12 11 5 deaths 1 0 2 0 0 2 0 0 1 0 1 2 3 70 127 76 71 445 37 32 30 24 18 Date 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 unknown date TOTAL No. of fatal cases 5 1 3 0 1 4 3 3 0 0 2 1 1 1 1 1 1 0 0 0 45 617 deaths 15 6 13 6 8 6 5 2 3 0 0 2 3 0 0 2 0 2 1 0 0 1016 ”Of the 56 cases that appeared on 31 August, it is certain that very few started in the late hours of the afternoon. The appearance of the outbreak was extremely rapid (as I was informed by a physician who lives in the center of the district where the attack occurred) and began in the night between 31 August and 1 September. Only a few of those who became ill in the first three days presented a history of diarrhea and the physicians who attended them informed me that very few recovered.” Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study 39 “The first of September—immediately after the onset of the outbreak—was the day on which the largest number of cases (143) occurred; a day later, the number declined to 116, and on the following day, to 54. When studying the table, we see that the number of cases continued to decrease day by day. On 8 September, the day on which the pump handle was removed, 12 cases occurred; on day 9, 11 cases; 10, 5 cases; 11, 5 cases; and on day 12 only 1 case. After this, no more than 4 cases occurred on the same day. As the epidemic declined, the daily deaths were more numerous than the new cases and they occurred in people who had suffered fever for several days. There is no doubt that mortality declined, as I already mentioned, due to the flight of the population as soon as the outbreak appeared. Nevertheless, the attacks only decreased until use of the water was stopped; this makes it impossible to determine if the well continued to contain the cholera poison in active state, or, by some cause had been freed of it.” “There is a beer brewery on Broad Street, near the well, where none of the workers died of cholera. When I found out about this I visited Mr. Huggins, the owner of the brewery, who informed me that he had close to 70 men working in the brewery, of which none suffered cholera, or at least the severe form, and only 2 workers felt mildly indisposed when the disease was prevalent. The men were assigned an amount of malt liquor and Mr. Huggins believed that they did not drink water at all and did not use water from the Broad Street well.” “A survey conducted among 418 people of the 896 residents on Broad Street revealed the relations between the disease and consuming water from the incriminated pump, as follows: among the consumers, 80 became ill and 57 did not; among the people who did not take water from the Broad Street pump, 2 became ill and 279 did not become ill. This means that among the patients with cholera, the relation between consumption and nonconsumption was 80/2. Among those who escaped the disease, the relation was 57/279.” became ill did not become ill consumed water 80 57 137 did not consume water 2 279 281 82 336 418 “The total case rate [attack rate] was 19.6% (82/418x100). In order to establish the importance of the water pump as a source of contamination, it is necessary to compare the case rate of those who took water with the case rate of those who did not take water:” 80 100 58% 137 2 care rate among those who did not consume water 100 0.7% case 281 case rate among those who consumed water case relative risk = 58 % 82 .9 0. 7 % “This study demonstrated the transmission by water of the outbreak.” Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study 40 “While contamination of the water of Broad Street with the evacuations of the disease exactly explains the terrible outbreak of the jurisdiction of St. James, there is no other circumstance that offers another explanation, no matter what hypothesis is adopted about the nature and cause of the disease....” Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study 41 Complementary Reading No. 2: Contemporary methodology of epidemiologic investigation Legionnaires’ Disease Adapted from Sharrar RC. Legionnaire’s disease: stalking a killer epidemic. A scientific detective team discovers the Philadelphia Killer. Encyclopedia Britannica, Book of Science and the Future, 1979. The problem When the American Legion Convention of the State of Pennsylvania, which had been convened from 21 to 24 July 1976 at the Hotel Bellevue Stratford in Philadelphia, was almost reaching its end some of the participants became ill. Almost all of them attributed it to the intense program of the convention. Upon returning to their respective cities, however, some of them complained about headache, high fever, chills, a dry cough, and muscular pains, symptoms of acute infectious disease. On the 27th of July, an elderly legionnaire died in Athens, Pennsylvania. However, not much attention was paid to the case because the individual suffered heart problems. By Friday, the 30th of July, five more legionnaires had already died and others had been hospitalized. Over that weekend five more died. On the morning of Monday, the 2nd of August, the epidemiologist of the State of Pennsylvania called the head of the Unit of Communicable Disease Control of the Department of Health of Philadelphia and declared an alert for the entire State. The alert stated that “there have been 11 deaths due to pneumonia recorded and all the people who died attended the American Legion Convention last week in Philadelphia.” In that same period, the country was preparing to combat a possible epidemic of swine flu and the public health authorities in all the states were preparing to implement a federal program of mass vaccination. The epidemiologists immediately considered swine flu and initiated epidemiological investigations as recommended by the Centers for Disease Control in Atlanta, Georgia. The search involved the participation of hundreds of people from various professions and became the most intense epidemiological investigation carried out in the modern history of medicine since the advent of AIDS. Beginning the search As a response to the extensive coverage provided by the communications media, which called this respiratory disease “Legionnaires’ disease” and the “Philadelphia Killer”, each suspected case was reported and investigated. The existence of an epidemic was confirmed rapidly. However, it was impossible to confirm the diagnosis with laboratory tests because the pathogen was unknown. Many cases of pneumonia were being reported to the health authorities and it was necessary to distinguish between disease from the outbreak and other diseases. Therefore, the investigators established a case definition: the first symptoms occurred between the 1st of July and the 18th of August 1976, including a fever of 39ºC or more and a dry cough, or fever and pneumonia confirmed by x-rays of the lungs. This clinical definition was very broad and included symptoms that could be attributed to a virus, bacterium, rickettsia, fungus, or a chemical toxin. Thus, the Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study 42 following was added to the case definition: an individual had to have attended the American Legion Convention or to have been in the Bellevue Stratford Hotel, headquarters of the convention and principal site of the meeting, after the first of July. Those falling under the case definition were called “cases of legionnaires’ disease.” One other case definition was also used: Cases with pneumonia and were a block from the hotel on Broad street, the principal access to the hotel, were “cases of Broad Street pneumonia”. All the other cases occurring in Philadelphia were classified as common pneumonia. The people who participated in the July convention came from every corner of the State and could be classified into four groups: delegates with the right to vote, non-delegates, relatives of the participants and members of the Women’s Auxiliary Group. The latter was holding its 56th Annual Convention concurrently. Participants were lodged primarily in five main downtown hotels. Most of the activities of the American Legion Convention took place in the Bellevue Stratford Hotel, while those of the Women’s Auxiliary Group were held in the Benjamin Franklin Hotel, about seven blocks away. The legionnaires rarely ate or drank in the restaurants and bars of the hotel. Instead, they frequented the restaurants around the hotel and drank at their private meetings, so it was very difficult to identify all the activities in which they participated over the four days. The hotel building had several intermediate floors with storerooms, restaurants, bars, offices, a ballroom and meeting rooms. Between floors 2 and 16 there were 725 guest rooms. Floor 18 had several conference rooms and a banquet hall. Under the vestibule there were three more floors: the kitchen, the basement containing several cabinets and storerooms, and the lower basement with an incinerator, machine room, water coolers for the air conditioning system, electric power distribution equipment, sewer pipes and water pumps. Finally, on the terrace of the hotel was the chimney of the incinerator, several air outlets and an air conditioning plant. The air conditioning system was investigated because it could potentially disseminating pathogens by air. A child had tossed powder used by magicians in an air conditioning outlet of the hotel a week before the convention. The powder was examined and it was found to be innocuous. The drinking water in the hotel, originating from the Philadelphia municipal system was also examined. In addition, detailed inspections of kitchens, elevators and waste and sanitation equipment were made and samples of suspicious substances were collected throughout the hotel. The bars and restaurants located outside the hotel were also thoroughly examined. By the 6th of August, 22 people had died and 130 had been hospitalized. Characteristics of person, place, and time The investigators needed information on cases and all others who had attended the Convention. Neither the American Legion nor the hotels could identify with certainty all of the Convention participants. Accordingly, a survey was conducted to determine who had attended the Convention and their activities during the Convention, with questions such as “were you sick before attending the convention?”, “when did you begin to feel ill?”, “what room did you stay in?” and “what restaurants did you go to?” Ten thousand two-page questionnaires were delivered to the 1002 American Legion posts throughout the State. The commanders of each post received instructions to deliver the questionnaire to each participant so that they could fill it out and return it. Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study 43 To determine if the outbreak was citywide, investigators reviewed the admissions records of three downtown hospitals and those of patients seen for diseases similar to the legionnaires’ disease in the emergency services of 11 hospitals. The number of deaths from pneumonia and flu reported weekly was compared with the corresponding weeks of the three previous years. None of the studies showed a notable increase in the number of cases of pneumonia in Philadelphia. Apparently, the legionnaires’ disease outbreak was not citywide. Other studies were conducted to determine if the problem of legionnaires’ disease was continuing. No secondary cases were detected among the relatives of the Convention participants or among the medical personnel who attended the outbreak cases at different hospitals. Fortunately, it appeared that the disease was not transmitted person-to-person. The people who stayed at the four hotels between the 6th of July and the 7th of August were surveyed to determine if new cases were occurring. No new cases were verified among the guests who arrived after the week of the 18th to the 24th of July, the week of the Convention. The findings indicated that legionnaires’ disease outbreak was not continuing and was limited to the dates of the Convention. Based on the investigations and a flow of information from medical and hospital sources, a clear clinical description of Legionnaires’ disease was gradually pieced together. The typical case started from 2 to 10 days after being exposed to the agent (incubation period) and the majority of the victims became ill after returning home. The first symptoms consisted of malaise, muscular pains, headache, and a dry cough. Shortly afterwards, a fever of 39 to 41ºC and chills appeared. Many patients had symptoms of respiratory distress, chest pain and gastrointestinal disorders. In general, they saw a physician two or three days after the onset of symptoms. At that time the chest X-ray revealed abnormal respiratory sounds, but up to that time there were no signs of condensation, when the lung tissue fills with fluid and cellular matter as in the case of pneumonia. More than 80% of the cases were hospitalized and 29 patients died, which represented a case-fatality rate of 16%. Deaths occurred mainly in elderly patients who had chronic diseases and short incubation periods for legionnaires’ disease. Patients treated with erythromycin and tetracycline had greater odds of surviving. Laboratory test results for cases did not help in diagnosis. Lab findings included some abnormalities that indicated a recent infection, but the information was not specific. Symptoms of low blood oxygen saturation were observed. Ninety percent of the cases had abnormal chest radiographs, mainly lung edema, that terminated with general condensation of the lungs. About 50% of the most advanced cases presented radiographic abnormalities in a single lung. On examining the lungs of the dead, several inflamed and condensed areas were observed that suggested a diagnosis of pneumonia. No abnormalities were observed in any other organ or system. Figure 5.1A shows the distribution of cases in time and the epidemic curve for the 182 cases classified as legionnaires’ disease and the 39 cases of Broad Street pneumonia. The cases of legionnaires’ disease included 149 Convention participants and 33 non-participants. The similarity of the two curves indicated that both groups were part of the same outbreak. The persistence of the disease among people who did not participate in the Convention during the first part of the month of August indicated that the source of infection remained active but less intense. In Tables 5.1A and 5.2A, the results of the survey among the legionnaires are presented. Table 5.1A shows the case rate by subgroup of participants and place of lodging. The 3,683 questionnaires processed included those of 1,849 delegates. Based on the number of delegates who voted in the Convention, it is estimated that between 80% and 85% of the forms were returned. The table also shows that the attack rate was higher among the delegates and their families and lower Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study 44 among the non-delegates and the members of the Women’s Auxiliary Group. This group held its meetings seven blocks away from the Bellevue Stratford. The guests of hotel “A”, the Bellevue Stratford, had the highest attack rate. Table 5.1A shows the attack rate by age and sex. This increased with age and was greater for men than for women. The general attack rate was 4%. Source and mode of transmission Findings from the investigation conducted after the Convention among the relatives of the legionnaires indicated no person-to-person transmission. Likewise, there was no cluster of cases within rooms of the hotel, as would have been expected if the transmission were person-to-person. Number of Cases cases FIGURE 5.1A EPIDEMIC CURVES FOR LEGIONNAIRES’ DISEASE 6 Broad Street Broad Street pneumonia Pneumonia 5 4 3 2 1 0 26 Legionnaires’ Legionnaires' disease Disease 24 Convention Participants Convention Non-Participants 22 20 Convention Number of Cases cases 18 16 14 12 10 8 6 4 2 0 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 1 2 JUL 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 AUG July August no participantes participantes A study of the 28 restaurants and bars in the neighborhood of the Bellevue Stratford found no associations between consumed food and drink and risk of disease. Likewise, the investigation of the two banquets at the Convention also yielded no association between consumed food and drink and risk of disease. Though a case-control study found that cigarette smokers had a greater risk of contracting disease, smokers were generally more susceptible to respiratory tract disease. No link Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study 45 was found between disease and consumption of alcoholic beverages or drinking water in the Bellevue Stratford. Likewise, the investigators found no association between insect bites or exposure to animals and disease. With no evidence emerging to point to the source of disease, speculators filled the gap with favorite theories like sabotage, biological warfare, several toxins and even paranormal and occult phenomena. The news media drew attention to some of these theories. Unfortunately, none of these speculations were supported by the epidemiological, clinical, and laboratory evidence. TABLE 5.1A LEGIONNAIRES’ DISEASE DISTRIBUTION BY TYPE OF PARTICIPATION AND LODGING Category Number of Cases Number of Responses Attack Rate (%) Delegate Auxiliary Companion Non-Delegate Stranger Total 125 4 17 3 0 149 1,849 701 268 762 103 3,683 6.8 0.6 6.3 0.4 0.0 4.0 Hotel A Hotel D Hotel E Hotel F Hotel G Another Hotel House Stranger Total 75 21 19 12 4 7 8 3 149 1,161 1.046 403 312 104 210 294 153 3,683 6.5 2.0 4.7 3.8 3.8 3.3 2.7 2.0 4.0 TABLE 5.2A LEGIONNAIRES’ DISEASE DISTRIBUTION BY SEX AND AGE Category Number of Cases Number of Responses Attack Rate (%) less than 40 years 40 to 49 years 50 to 59 years 60 to 69 years 70 and more years Unknown Total 11 25 58 36 19 0 149 610 805 1,428 538 254 48 3,683 1.8 3.1 4.1 6.7 7.5 0.0 4.0 Male Sex Female Sex Unknown Total 123 26 0 149 2,292 1,380 11 3,683 5.4 1.9 0.0 4.0 Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study 46 Identification of the agent The search for the cause of Legionnaires’ disease involved obtaining and analyzing hundreds of biological samples from patients. The search for a possible microbiological agent included nine methods of visual microscopic screening, 14 different culture media to isolate bacteria and fungi, and 13 host systems for isolating viruses. In addition, tests of blood sera were made with 77 known infectious agents to seek the presence of antibodies. Tissue and urine samples were examined to detect abnormal concentrations of over 30 metals and several toxic organic compounds. Though these tests excluded many causal agents, none was able to identify the cause of Legionnaires’ disease. One by one, all known agents were excluded as possible causes of legionnaires’ disease. At the end of December in the year of the outbreak, two microbiologists from the Division of Leprosy and Rickettsiae in the Centers for Disease Control, Joseph E. McDade and Charles C. Shepard, in tissue samples isolated a new agent suspected as the cause of legionnaires’ disease. These findings were published in January 1977. The agent was isolated with the laboratory techniques commonly used to detect rickettsiae. Samples of lung tissue from a dead victim were homogenized and injected in guinea pigs. After a period of incubation of one to two days, the young guinea pigs presented symptoms of fever, teary eyes and prostration. Suspensions from the spleen of the symptomatic animals were prepared and used to inoculate chicken embryo vitelline sacs. These embryos died after 4-6 days and microscopic examination of stained sections of the vitelline sac revealed rod-shaped bacteria. Once the causal agent was isolated, a laboratory test was developed to detect the presence of antibodies to the agent in the blood serum of cases. This test could detect disease events long after the disease was resolved. Thus, five and a half months after the epidemic began the epidemiologists finally had a laboratory test that could confirm diagnoses. In the year after the outbreak, using the new blood test for this disease the following findings were reported: 1. The bacterium was isolated in five cases of pneumonia recorded in Philadelphia, 4 met the investigators’ case definition of legionnaires’ disease and one was a Broad street pneumonia case. 2. The antibody assay showed that more than 90% of the cases of legionnaires’ disease and 64% of the cases of Broad street pneumonia from specimens of blood serum were positive for the pathogen. 3. The samples of blood serum of patients who were exposed for a single day on the 21st , 22nd or 23rd of July, and two of the nine victims of the disease who attended another meeting in Philadelphia from August 1st to the 8th confirmed the existence of a recent infection of this disease, indicating that the source of infection infected persons for at least two weeks. 4. Blood samples were collected from over 500 people who lived or worked in central Philadelphia to determine the prevalence of antibodies against the bacterium. The studies demonstrated that less than the 5% of the general population had an appreciable concentration of antibodies of that class. Testing at the national level of patients diagnosed with pneumonia of non-bacterial origin found that 1% to 2% of these cases could be legionnaires’ disease. These studies found that legionnaires’ disease was caused by a biological agent and not by a toxin and that the victims of Broad street pneumonia who never entered the Bellevue Stratford were part of the epidemic. It was concluded that the period of exposure of the microorganism was at least two weeks. Although this bacterium can cause major epidemics, it maintains a low endemic level. It’s Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study 47 improbable that this pathogen would maintain high rates of disease continually in a given geographic region. Protection of the public The investigation initiated in August 1976 finally led to the discovery of a biological pathogen that until then had been unknown. Later studies revealed that this organism has caused epidemics in the past and that it has low-grade endemic activity during the year over a broad geographical area. Current situation With time, legionnaire’s disease was recognized as an acute bacterial disease with two clinicalepidemiological manifestations: Legionnaires’ disease Pontiac fever Pontiac fever is not associated with pneumonia or death and patients recover spontaneously within 2 to 5 days without treatment; it’s more similar to an allergic reaction elicited by inhaling an antigen than a bacterial invasion. The responsible pathogen, a gram-negative bacillus, was named Legionella pneumophila. Eighteen serogroups of L. pneumophila are currently recognized. The one most associated with disease is serogroup 1. The earliest known case of legionnaire’s disease occurred in 1947 and the earliest known outbreak occurred in 1957 in Minnesota. The disease has been identified in North America, Australia, Africa, South America and Europe. Cases and sporadic outbreaks occur throughout the year, although it is more common in summer and fall. The attack rate of legionnaires’ disease in community outbreaks generally ranges from 0.5% to 5%. On the other hand, Pontiac fever has shown a high attack rate of around 95% in several outbreaks. The pathogen’s primary reservoir is water. It frequently spreads through hot water systems such as showers. The mode of transmission is through the air. The incubation period can range from 2 to 10 days but most often falls between 5 to 6 days. Person-to-person transmission is not significant. The disease appears in older patients; the majority of cases are at least 50 years old. It’s more likely to cause disease in smokers, patients with chronic diseases and men, with a man-woman ratio of 2.5:1. It is extremely rare in people under 20 yearsof-age, though some outbreaks have been recorded in hospitalized patients in this age group. There are now effective control measures and treatment for the disease. The investigation of the legionnaires’ disease outbreak demonstrates how epidemiology can clarify problems early and lay the foundation for control and treatment even when the disease is not fully understood. Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study 48 REFERENCES Abramson JH. Making sense of data: a self-instruction manual on the interpretation of epidemiological data. Second Edition. Oxford University Press; New York, 1996. Beaglehole R, Bonita R, Kjellström T. Epidemiología básica. Organización Panamericana de la Salud. Publicación Científica N° 551. Washington DC, 1994. Buck C, Llopis A, Nájera E, Terris M [Editores]. El desafío de la epidemiología. Problemas y lecturas seleccionadas. Organización Panamericana de la Salud; Washington DC, 1988. Centers for Disease Control and Prevention. Guidelines for investigating clusters of health events. Mortality and Morbidity Weekly Report 1990;39(RR-11); 1-16. Dever AGE. Epidemiología y administración de servicios de salud. Organización Panamericana de la Salud; Washington DC, 1991. Galbraith MS. The application of epidemiological methods in the investigation and control of an acute episode of infection. En: Holland W, Detels R, Knox G. Oxford textbook of public health, volume 3. Oxford University Press; Oxford, 1985. García J, Morales ML, Ramírez R, Rosado M, Ruiz M. Investigación de brotes epidémicos. Primera edición. Consejería de Salud y Servicios Sociales; Junta de Andalucía, 1988. Gomes Pereira, M. Epidemiologia teoria e prática. Editora Guanabara Koogan S.A; Rio de Janeiro, 1995. Goodman RA, Buehler JW, Koplan JP. The epidemiologic field investigation: science and judgement in public health practice. American Journal of Epidemiology 1990;132(1):9-16. Gregg MB [Editor]. Field epidemiology. Oxford University Press; New York, 1996. Kelsey JL, Thompson WD, Evans AS. Methods in observational epidemiology. Oxford University Press; New York, 1986. Mausner JS, Kramer S. Mausner & Bahn epidemiology. An introductory text. W. B. Saunders company; Philadelphia, 1985. McKenzie WR, Goodman RA. The public health response to an outbreak. Current Issues in Public Health 1996;2:1-4. Miettinen OS. Theoretical epidemiology. Principles of occurrence research in medicine. Delmar Publishers Inc.; New York, 1985. Morton RF, Hebel JR, McCarter RJ. A Study Guide to Epidemiology and Biostatistics. Third Edition. Aspen Publishers, Inc; Gaithersburg, 1989. Palmer SR. Outbreak investigation: the need for "quick and clean" epidemiology. International Journal of Epidemiology 1995;24(3-Suppl.1):S34-S38. Palmer SR. The identification and investigation of epidemics. En: Dunstan F, Pickles JJ [Editores]. Statistics in medicine. Clarendon Press; Oxford, 1991. Polit DF. Investigación científica en ciencias de la salud. Tercera edición. Nueva Editorial InteramericanaMcGraw-Hill; México, 1987. Reingold AL. Investigaciones de brote – una perspectiva. Boletín Epidemiológico OPS 2000 Junio 21(2):1-7. Silva LC. Cultura estadística e investigación científica en el campo de la salud: una mirada crítica. Ediciones Díaz de Santos, S.A.; Madrid, 1997. Stolley PD, Lasky T. Investigating disease patterns. The science of epidemiology. Scientific American Library; New York, 1998. Vaughan JP, Morrow RH [Editores]. Manual of epidemiology for district health management. World Health Organization; Geneva, 1989. Second Edition, MOPECD 2001 Special Program for Health Analysis. Pan American Health Organization MOPECD Unit 5: Epidemiologic field study Second Edition, MOPECD 2001 49 Special Program for Health Analysis. Pan American Health Organization