Syringe Driver Policy - DCHS - Derbyshire Community Health Services
advertisement

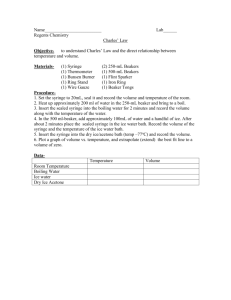
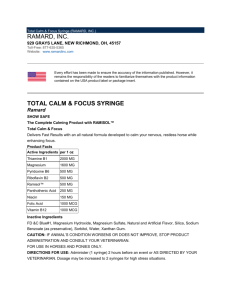
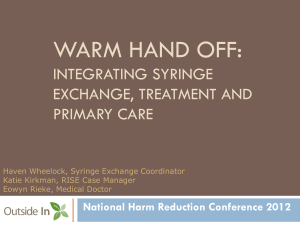
SYRINGE DRIVER POLICY Document History Version Date: July 2012 Version Number: 2 Status: Next Revision Due: Developed by: Approved Policy Sponsor: Assistant Director Integrated Community Based Services EQIA completed: EIA/CHANNAN/14062012 Approved by: Clinical Effectiveness Group Date Approved: 14th September 2012 July 2014 Workforce Development Lead Trainer Revision History Version 2 Revision Date June 2012 June 2012 2 Mar 2014 Summary of Changes Updated to reflect general practice and ease of use for practitioners. New format and update section 5.3 including: Added a sentence 'Please make a note of the rate ml/hr at this stage'. Added a sentence on when to apply the keypad lock after setting up the syringe driver; and section 10 for training. Changes to Syringe Driver allocation To help ensure that this policy is as accessible as possible, it has been left-aligned and is available in alternative formats and languages. To obtain a copy of the policy in large print, audio, Braille (or other format) or in a different language, please contact The Communications Team, by Tel: 01773 525099 or email communications@dchs.nhs.uk TABLE OF CONTENTS 1. Background ................................................................................................................. 3 2. Aim /Purpose .............................................................................................................. 3 3. Definitions and an Explanation of Terms Used........................................................ 3 4. Intended Users. ........................................................................................................... 4 5. Full Details of the Policy ............................................................................................ 4 5.1 20ml/30ml BD Plastipak luer lock syringes. ............................................................ 4 5.2 Administration line .................................................................................................. 4 5.3 BD Saf-T-Intima™ 22 Gauge cannula (blue), stores code number L003052. ......... 5 5.4 Choice of infusion site ............................................................................................. 5 5.5 Labelling ................................................................................................................. 6 5.6 Procedure: First time set up of the syringe pump. .................................................. 7 5.7 Reasons for Alarms: ............................................................................................. 10 5.8 Documentation and monitoring ............................................................................. 11 5.9 Transfer to another care setting. ........................................................................... 12 5.10 Risk management ............................................................................................... 13 5.11 Cleaning and Decontamination ........................................................................... 13 6. Support and Additional Contacts ............................................................................ 14 7. References and Associated Documents ................................................................ 14 8. Trust Accountability / Responsibilities ................................................................... 14 9. Monitoring & Performance Management of the Policy.......................................... 16 10. Equality Impact Statement ................................................................................... 16 11. Appendices ............................................................................................................ 16 Appendix 1 ....................................................................................................................... 17 Appendix 2 ....................................................................................................................... 17 Appendix 3 ....................................................................................................................... 17 Appendix 4 ....................................................................................................................... 17 Appendix 5 ....................................................................................................................... 17 12. . Equality and Impact Assessment ........................................................................ 17 SYRINGE DRIVER POLICY 1. BACKGROUND The use of a portable battery operated syringe driver for subcutaneous medications is now a well established technique in palliative care; this view is supported by Dickman et al 2005. The syringe driver “allows for a minimally invasive route of drug administration, which produces relatively constant levels of medication which avoids peaks, which can result in reduced symptom control” (Twycross and Wilcock, 2002). Palliative care patients often present with multiple symptoms that can necessitate the need for several drug treatments. If the patient’s condition deteriorates and the oral route cannot be used a continuous subcutaneous infusion via the syringe driver provides a simple and effective way to control symptoms (Dickman et al 2005). In 2010 the National Patient Safety Agency (NPSA) issued an alert which asks NHS organisations to ensure that syringe pumps have: a) Rate settings in ml per hour; b) Mechanisms to stop infusion if the syringe is not properly and securely fitted; c) Alarms that activate if the syringe is removed before the infusion is stopped. Derbyshire Community Health Services (DCHS) NHS Trust, after consultation, opted for the McKinley T34 syringe pump, which will replace the Graseby MS16A and MS26. This pump is small in size, and has a large LCD display which provides error messages and context sensitive instructions. The device includes a rolling 512 date and time stamped event log, mechanical syringe sensors that interlock with the syringe and provision of alarms during incorrect operation thus complying with IEC 60601-2-24 standards. The McKinley T34 is calibrated in ml/hour. 2. AIM /PURPOSE A subcutaneous infusion pump is an effective method of administering therapeutic drugs via subcutaneous route, which can no longer be tolerated orally or rectally by the patient. The aim of this policy is to provide guidance for staff in the use of the McKinley T34 pump across adult services. Using a uniform policy will reduce the level of risks associated with syringe pump management and will facilitate the introduction of the McKinley T34 Syringe pump within DCHS NHS Trust. 3. DEFINITIONS AND AN EXPLANATION OF TERMS USED A syringe pump is a medical device, which is a small portable, battery operated infusion pump. It is used to deliver medication via the subcutaneous route over a calculated period of time providing a continuous level of medication. Version Number 2 Page 3 of 17 Policy date June 2012 SYRINGE DRIVER POLICY 4. INTENDED USERS. Table of Intended Users: DCHS Finance Performance and Information Quality Strategy Service Delivery Human Resources Medical Directorate Leicester Employees No No No Yes No Yes No Within this policy where it states “all employees”, please note that it relates to all the employees who are highlighted in the table above 5. FULL DETAILS OF THE POLICY Equipment required 5.1 20ml/30ml BD Plastipak luer lock syringes. This provides sufficient dilution to reduce the risk of adverse site reactions and incompatibility, without providing too large a volume for comfortable administration. If the medications total is greater than 10ml before dilution, it may be necessary to use a 30ml syringe and dilute further. Size of BD Plastic Luer Lock Syringe 20ml syringe 30ml syringe 50ml syringe (Exceptional circumstances) Maximum fill volume as stated in user manual 18ml 23ml 34ml 5.2 Administration line A 100cm luer lock Codan manometer line is recommended (Code FSB066) it requires 0.8ml to prime. NB this manometer line has been identified as cost effective and in line with medicine administration requirements. Version Number 2 Page 4 of 17 Policy date June 2012 SYRINGE DRIVER POLICY 5.3 BD Saf-T-Intima™ 22 Gauge cannula (blue), stores code number L003052. The BD Saf-T-Intima cannula, shown above, is the choice of cannula for SC medications at DCHS. The rationale for this preference is: Site reactions are less common Insertion is less traumatic Needle stick injury is reduced to patient and staff Less expensive that alternative Teflon devices Can remain in situ longer than other devices (Dawkins et al, 2000) Note: The BD Saf-T-Intima cannula has a dead space of 0.2ml. It is NOT primed before or after insertion. If a patient is started on a continuous SC infusion they will require a separate BD Saf-T-Intima cannula for bolus medications. The medication should be flushed with at least 0.2ml of Water for Injection to accommodate the dead space. 5.4 Choice of infusion site Acceptable SC cannula insertion sites (see diagram 1): Anterior aspect of the upper arms or anterior abdominal wall Anterior aspect of thigh The scapula if the patient is distressed and /or agitated Anterior chest wall (least common) Sites not suitable for insertion: Skin folds and breast tissue Directly over a tumour site Lymphoedematous limb or oedema – absorption may be reduced The abdominal wall if ascites is present Bony prominences – little SC tissue, absorption reduced Previously irradiated skin – skin may be sclerosed, poor blood supply Sites near a joint – uncomfortable, increased risk of displacement Infected, broken or bruised skin If a local reaction occurs, the cannula should be recited using a fresh cannula and administration set. If this recurs, consider further diluting the drug(s). Version Number 2 Page 5 of 17 Policy date June 2012 SYRINGE DRIVER POLICY The cannula may remain in place for up to seven days, unless removal is indicated Diagram 1 – Acceptable SC Cannulation sites 5.5 Labelling All syringes containing drug additives must be fully labelled. If there is any doubt as to the contents of a syringe, the contents should be discarded. (This is particularly important for continuity of care, especially where patients transfer from one care setting to another). Complete the label details in black ink The label should state: The name, Date of Birth and NHS Number of the patient for whom it is intended. The date and time of preparation The initials of the persons preparing and checking the contents The name and dose of all the drugs The name of the diluent Attach label to the syringe. Ensure the label does not interfere with the mechanism of the infusion device, i.e. where there is contact with the barrel clamp arm. Flag the label at the tip end of the syringe, leaving the scale visible so that it can still be read. Version Number 2 Page 6 of 17 Policy date June 2012 SYRINGE DRIVER POLICY McKinley T34 Syringe Pump Syringe Flange/Collar sensor Barrel Clamp Arm and Sensor Plunger sensor Actuator Infusion light status indicator: Green running Red - stopped Power ON/OFF INFO Scroll UP/DOWN YES/NO NO/STOP Actuator movement Forward (FF)/Back Best Practice Point: For many patients the setting up of a syringe driver is a response to unrelieved symptoms. Following initial set-up of the driver it takes 4-6 hours for drugs to reach therapeutic blood levels. Therefore, if the patient is experiencing unrelieved symptoms, consider the use of a PRN breakthrough dose which can be administered before the syringe pump is set up. 5.6 Procedure: First time set up of the syringe pump. Wash hands with bactericidal soap and water. Adhere to Aseptic Non-Touch Technique (ANTT) principles throughout the procedure. Ensure that the Saf-T-Intima cannula has been inserted/ or reassessed that it is in good condition for use. Procedure. 1. Ensure barrel clamp arm is down and no syringe in place. 2. Press ON/OFF key to power up for 2 to 3 seconds - the actuator moves (preloading) and the first four screens display automatically. ALWAYS allow the pre-loading programme to complete and the flashing syringe icon to appear BEFORE loading the syringe onto the pump. 3. Software version and pump identification is then displayed. T34 Version NCAT xxxxxx ID: (hospital number) Version Number 2 Page 7 of 17 Policy date June 2012 SYRINGE DRIVER POLICY The actuator is moving to the position of the syringe that was in place at the start of the previous infusion. The pump will then display the default settings Check Battery level: Press blue INFO key then YES. In the community, batteries reading less than 40% at the start of a 24 hour infusion should be changed. For community hospitals this will be when ‘low battery alert displayed’. Pre-loading USE NO to interrupt Occlusion 750mmHg Max rate 5ml/hr Program lock ON Battery status 85% Load syringe * flashing syringe image* Load Syringe - Secure the syringe onto the pump ensuring that the syringe is placed correctly in the plunger and collar sensors. If Necessary, align syringe to sensors and use the FF/BACK keys to move the actuator for syringe placement 4. If the syringe size/brand displayed matches the one used, confirm by pressing YES. 5. Infusion summary displays. DO NOT CONFIRM, remove the syringe. Please make a note of the rate ml/hr at this stage. Volume 15.0ml Duration 24:00 Rate 0.62ml/hr Confirm, Press YES 6. Attach syringe to the extension set and prime the set manually. Slide clamp across the administration set to prevent siphoning. 7. Reload the syringe; use the FF key to adjust actuator. 8. If the syringe size/brand displayed matches the one used, confirm by pressing YES. 20ml BD Plastipak Select ↑↓, press YES 9. Press YES to resume 10. Check all settings displayed on screen and confirm by pressing YES. Version Number 2 Page 8 of 17 Press YES to resume, No for New Syringe Volume 14.1ml Duration 22:40 Rate 0.62ml/hr Confirm, Press YES Policy date June 2012 SYRINGE DRIVER POLICY Connect the primed administration line to the Saf-T-Intima cannula. 11. Press YES to start the infusion when ready to do so. Start Infusion? 12. Infusion running. (Alternating last line messages) Time Remaining 22.40 Rate 0.62ml/hr 20ml BD Plastipak Time Remaining 22.40 Rate 0.62ml/hr <<<Pump Delivering Press and hold down the blue info key and wait for the keypad lock to be activated. The syringe pump panel must be locked when not in use by a staff member. The McKinley T34 syringe pump should be secured in the locked box provided – this will protect the syringe from accidental knocks. Each ward will have two keys, one per team, located on the CD keys. In the community each community nurse will have their own key, which they are responsible for. This key should not be left in the patient's home. What to do when changing the syringe: When a new syringe is due to be loaded into the pump; Stop the infusion. Press and hold the info key to deactivate the keypad lock facility. The pump should be turned off and the infused syringe removed. Switch pump back on again, allowing pre-loading programme to complete. This is to ensure that the previous programme is cleared. Follow steps 1 – 6 At step 7 press yes to confirm. The reason for this is the administration line is already primed. If the syringe pump does not undergo the preloading sequence and gives the option of resuming a previous programme. THIS OPTION MUST NOT BE TAKEN. A new programme MUST be set for each syringe change. If this occurs, staff must check that the keypad lock function is off and turn off the syringe pump. Turn the syringe pump back on The syringe pump will then undergo the preloading sequence. Continue to set up the syringe pump. When the pump is no longer required: Stop the infusion – note how many millimetres remain in the syringe and that this corresponds with the syringe infusion summary. Version Number 2 Page 9 of 17 Policy date June 2012 SYRINGE DRIVER POLICY Press and hold the info key to deactivate the keypad lock facility. Switch off the pump. Remove the battery Clean as specified in section 5.10 Follow DCHS Medicine Code for the correct removal and disposal of parental drug therapy. 5.7 Reasons for Alarms: Screen Low battery Program nearly complete Pump paused too long End battery End program Syringe syringe displaced, Description Alert: Battery is almost depleted Alert: Infusion will end soon Alarm: Pump has been left in STOP mode (on hold) for 2 minutes Alarm: Battery is depleted Alarm: Infusion is complete Check Alarm: One or more of the syringe detection sensors is not detecting Occlusion Alarm: Patient access Check line and syringe – device is blocked, occluded, see below for further clamped or kinked information. Implication/action Prepare to change the battery. Prepare to change syringe or turn pump off Either start the infusion, continue pause or turn the pump off Change battery Close down or start a new infusion Check screen messages for assistance. Check the syringe and reseat as necessary Replace access device, release the clamp or un-kink tubing. Changing the battery in the middle of an infusion: Make a note of rate ml/hr, volume to be infused and volume left to be infused and duration left Stop the syringe pump Deactivate keypad lock and turn the syringe pump off Replace battery Turn syringe pump back on There will be no preloading sequence as the syringe has not been removed from the syringe pump. The syringe pump will ask a prompt question Press YES to resume. NO for a New Syringe Press YES to resume Infusion summary displays Volume 12.0ml Duration 16.25 Rate 0.70ml/hr Confirm, Press YES Version Number 2 Page 10 of 17 Policy date June 2012 SYRINGE DRIVER POLICY Check this information with what was documented before turning off the pump, if all matches, press YES to confirm. What to do in the event of an occlusion: If the pump alarms, indicating an occlusion, press stop. Check the administration line for kinks or damage and check the cannula site. What to do if the cannula is no longer viable: (note all infusion summary information) Place clamp on administration line. Disconnect the administration set from the Saf-T-Intima cannula. A new cannula should be sited. Reconnect the administration line to the cannula, remove the clamp and press yes to start. What to do if the administration line is no longer viable: (note all infusion summary information) Place clamp on the Saf-T-Intima cannula. Detach the administration line from the Saf-T-Intima cannula and syringe. Attach a new administration line and prime. Use FF key to realign the actuator, reload on to the pump. Press start on the syringe pump Press YES to resume. NO for a New Syringe Press YES to resume. The pump will recalculate the volume and keep the infusion time the same. 5.8 Documentation and monitoring The Subcutaneous Infusion Monitoring Form (Appendix 1 for Hospital staff and Appendix 2 for Community staff) must be used to record details of preparation and subsequent administration and monitoring. The following must be documented: details of preparation and commencement checks at 1 hour after commencement or syringe change and at 4 hourly intervals in Community Hospitals and 24 hourly intervals if patients are being cared for by community nursing services: site appearance (no redness, pooling swelling, pain, hardness) Rate of infusion(according to infusion chart) Syringe/line contents appearance (absence of clouding, crystallisation or colour change) Volume remaining: check the amount displayed to be infused corresponds with the amount within the syringe pump Volume infused Battery status (shown as a percentage on the display panel on the front of the syringe pump). Any problem noted and action taken. Disposal of any remaining syringe contents. Version Number 2 Page 11 of 17 Policy date June 2012 SYRINGE DRIVER POLICY 5.9 Transfer to another care setting. It is essential to contact the relevant health professional who will be receiving the patient, i.e. District Nursing Team, ward team as soon as the admission/discharge date/time is known and inform them of plan to admit/discharge patient with a McKinley T34 syringe driver. For community/hospital staff receiving patients with a syringe pump insitu, they will need to change the pump on first visit and return to the discharging service (e.g. DHU, acute hospital, hospice or community hospital). Spare syringe pumps will be located at the following sites: Hospital/ Area Babington Hospital Baron Ward Ilkeston Community Hospital Oakwell Ward Cavendish Hospital Fenton Ward Ashgate Hospice (The Ward) Address Derby Road, Belper, Derbyshire DE56 1WH Heanor Road, Ilkeston, Derbyshire DE7 8LN Contact Number 01773 824171 Manchester Road, Buxton, Derbyshire SK17 6TE Ashgate Road, Old Brampton, Chesterfield S42 7JD 01298 212800 Bolsover Hospital Rowan Ward Swadlincote Health Centre. Only until 6.30pm. After this time care homes would contact 111 or Rightcare if the patient is registered. Welbeck Road, Bolsover, Chesterfield S44 6DH Civic Way, Swadlincote, Derbyshire DE11 0EA 01246 827901 01159 305522 01246 568801 01283 818000 Hospital staff to complete the Syringe Pump Loan Sheet (Appendix 3), it is the wards responsibility to follow up the loan of any equipment if it has not been returned to the ward. For patients who are residents (regardless of status, nursing or residential) in care homes then community nursing teams are the first contact for a syringe pump. If all community nursing teams syringe driver are in use, then care home staff should contact the nearest hospital or health centre to obtain a syringe driver. This should be collected by care home staff with valid identification. It is recommended that all equipment used in the community setting for setting up a syringe pump and for the administration of PRN anticipatory doses are kept together in a designated syringe pump box. DO NOT LEAVE A KEY TO THE SYRINGE PUMP IN THE PATIENTS HOME. Version Number 2 Page 12 of 17 Policy date June 2012 SYRINGE DRIVER POLICY 5.10 Risk management Care must be taken to ensure that The McKinley T34 is NOT immersed in water In the event of an incident, an incident form must be completed. Annual service and maintenance must be carried out. What defines an incident? Administration of incorrect medication, dose and /or diluent Infusions completing ahead of time or carrying on beyond intended time of completion Device not alarming Any other incident or near miss which may compromise patient safety or comfort. Where there has been a problem with the syringe pump it must be sent to the Medical Engineering Department for investigation. The medical engineering department will have access codes to access the pumps event logs. You need to ensure that the pump has been decontaminated prior to going for inspection. A completed certificate of decontamination must be completed (see appendix 5) and kept with the pump for the medical engineering department. The certificate can be located within the Medical Devices Policy. 5.11 Cleaning and Decontamination Carry out cleaning of the syringe pump and lockbox with Clinell wipes as per DCHS Patient Equipment Cleaning policy. If any additional cleaning is required e.g. contamination with bodily fluids or cleaning the threads of the screws the actuator moves along, contact your local Medical Engineering Department and/or Infection Prevention & Control Team for advice. Do not use chemicals such as Xylene, acetone/similar solvents as this will damage components and labels. Lockboxes should not be cleaned with alcohol-based products as this causes the lockbox to become more brittle. Lock boxes (figure 1) must be cleaned with Acticlor if contaminated with blood or body fluids or in contact with a patient with a known infection, refer to DCHS Decontamination Policy. Figure 1 - Lock Box The syringe pump must never be submerged in water, and if it is accidentally dropped in water, it must be withdrawn from use immediately and sent to the Medical Engineering Department. The re-usable pouch can be cleaned with detergent based wipes containing water or alcohol. When thorough cleaning is required machine wash at 30ºc. Do not bleach or iron. Version Number 2 Page 13 of 17 Policy date June 2012 SYRINGE DRIVER POLICY 6. SUPPORT AND ADDITIONAL CONTACTS Yvonne Jackson Workforce Development Lead Trainer - Tel: 01246 515627 Donna Wilson Workforce Development Lead Trainer - 07500993779 Malcolm Steward Head of Medicines Management - Tel: 01246 253056 North County - Medical Engineering Department - Tel: 01629 812525 South County - Clinical Engineering Department The Royal Derby Hospital Tel 01332 788031 7. REFERENCES AND ASSOCIATED DOCUMENTS DCHS Hand Hygiene Policy DCHS Consent Policy DCHS Medical Devices Policy DCHS Record Keeping Policy DCHS Patient Equipment Cleaning Policy Dickman A. et al. (2005) The Syringe Driver. University Press, Oxford. Hunt T. (2002) in: Pension J. Fisher R. Palliative care for people with Cancer. Arnold, London: National Patient Safety Agency Rapid Response Report (2010) NPSA/2010/RRR019 Safer Ambulatory Syringe Drivers McKinley T34 Ambulatory Syringe Pump Operation Manual, March 2006 8. TRUST ACCOUNTABILITY / RESPONSIBILITIES 8.1 Individuals: 8.1.1 Chief Executive The Chief Executive has responsibility for the DCHS Board for ensuring that there are safe and effective systems in place to deliver high quality services. 8.1.2 Director of Service Delivery The Director of service Delivery is responsible for the high quality, efficient and effective community services provided by the four Service Delivery divisions within the Trust, ensuring that they meet and exceed performance standards. 8.1.3 Director of Quality / Chief Nurse The Director of Quality / Chief Nurse is responsible for the professional leadership of non medical clinicians across the Trust and for ensuring the highest possible quality of care for patients and service users. The Director of Quality is also responsible for the development and implementation of effective strategies and systems to improve patient safety and patient experience across the Trust 8.1.4 Assistant Director Version Number 2 Page 14 of 17 Policy date June 2012 SYRINGE DRIVER POLICY The Assistant Director of Integrated Community Based Services is responsible for service delivery. 8.1.5 Operational Managers The Operational Managers have a responsibility to ensure that the policy is implemented within their area and that their teams are aware of the policy and have received the appropriate training. 8.1.6 Employees Professionally registered employees; all employees are accountable for their professional practice and hold individual responsibility to maintain their knowledge and skills. All employees have a responsibility to be aware of and read policies appropriate to their roles and others where necessary. They should be aware of, and comply with, their responsibilities within the individual policies of the Trust. 8.1.7 Policy Sponsor The policy sponsor is responsible for ensuring that: the policy is developed in line with this framework the policy is disseminated to its target audience; appropriate training is given in the use of the policy; the policy is properly implemented. its implementation is monitored and reviewed on a regular basis. The policy sponsor is the Assistant Director of Integrated Community Based Services. 8.2 Committees: 8.2.1 DCHS Board The DCHS Board has ultimate responsibility for DCHS. The Board’s prime duty is to ensure good governance throughout the Trust and act in the best interests of the public for the services DCHS provides. 8.2.2 Governance Committee The Governance Committee (GC) has delegated authority from the DCHS Board and is responsible for ensuring that controls are in place to support the achievement of DCHS’ business objectives, whilst minimising its exposure to corporate, financial and clinical risks. 8.2.3 Quality Committee The Quality Committee is responsible for ensuring the delivery and integration of the clinical governance agenda across DCHS including monitoring ongoing compliance with the CQC Registration. 8.2.4 Risk Committee The Risk Committee is responsible for providing strategic leadership on the management of risks and ensuring that controls are in place to support the achievement of DCHS business objectives, while minimising its exposure to all risks. 8.2.5 Safety Committee The Safety Committee is responsible for providing overall assurance on the safety management systems (integrating patient safety and health & safety) within DCHS and ensuring processes are in place, to meet statutory, mandatory and legislative safety requirements. Version Number 2 Page 15 of 17 Policy date June 2012 SYRINGE DRIVER POLICY 8.2.6 Education Development & Learning Committee Education Development and Learning Committee is responsible for ensuring that there is a robust strategy to enable the workforce of DCHS to be competent to deliver the highest quality of professional services to the people of Derbyshire. 9. MONITORING & PERFORMANCE MANAGEMENT OF THE POLICY Training All staff using the McKinley T34 syringe driver must be competent and professionally accountable in the use and operation of this device. Staff must have attended a McKinley T34 pump training session and complete the competency workbook, this is provided by Workforce Planning and Development Team. Staff can utilise the e-learning package provided by CME for the Mckinley T34, as an update. http://www.dchs.nhs.uk/assets/public/dchs/dchs_staff_zone/your_development/elea rning%20/E%20Learning%20Algorythm%20June%202011.doc Records of staff training will be held on electronic staff record (ESR). All staff must complete bi-annual updates. Training will be advertised on the Learning and Development intranet site. Minimum Requirement Duties/Responsibilities Monitoring Who Frequency Review Review of policy Policy Development Group 2 Yearly – Policy review Clinical Effectiveness Group Process including any flow charts Training Monitoring Appendices (If required) Equality Impact Assessment (EIA) 10. EQUALITY IMPACT STATEMENT We welcome feedback on this policy and the way it operates. We are interested to know of any possible or actual adverse impact that this policy may have on any groups in respect of age, disability, gender reassignment, marriage and civil partnership, pregnancy and maternity, race, religion or belief, sex and sexual orientation. The person responsible for equality impact assessment of this policy is Caroline Hannan Tel 01159316200 This policy has been screened to determine equality relevance for the following equality groups: age, disability, gender reassignment, marriage and civil partnership, pregnancy and maternity, race, religion or belief, sex and sexual orientation. The policy is considered to have high equality relevance. A full impact assessment will be conducted by August 2012 11. APPENDICES Version Number 2 Page 16 of 17 Policy date June 2012 SYRINGE DRIVER POLICY Appendix 1 Subcutaneous Infusion Monitoring Form – Hospital Appendix 2 Subcutaneous Infusion Monitoring Form - Community Appendix 3 Syringe Pump Loan Sheet Appendix 4 T34 Lock On Load and Prime Quick User Guide T34 Lock On Load Prime QUG v1 May 2011.pdf Appendix 5 Certificate of Decontamination 12. Certificate of Decontamination.doc EQUALITY AND IMPACT ASSESSMENT The EIA has been determined as low rated. Click here to access the EIA web page. Version Number 2 Page 17 of 17 Policy date June 2012