Children's Speech
Sound Disorders
QUESTIONS AND ANSWERS
Copyright © 1998 Caroline Bowen All rights
reserved
Citing this article
This page contains an article about
children's speech sound
disorders. Cite it as:
Bowen, C. (1998). Children's speech sound
disorders: Questions and answers. Retrieved from
http://www.speech-languagetherapy.com/phonol-and-artic.htm on (date).
Introduction
What is speech?
Speech is the spoken medium of language. The other two "mediums" or "forms" of
language are writing and gestures. Gestures range from simple iconic movements,
like pretending to drink, through to complex finger-spelling and sign systems.
What is phonology?
Phonology is a branch of linguistics. It is concerned with the study of the sound
systems of languages.
The aims of phonology are to demonstrate the patterns of distinctive sound contrasts
in a language, and to explain the ways speech sounds are organised and represented
in the mind.
The term "phonology" is used clinically as a referent to an individual’s speech sound
system - for example, "her phonology" might refer to "her phonological system", or
"her phonological development".
What is phonological development?
The gradual process of acquiring adult speech patterns is called phonological
development.
Putting it another way, the emergence in children of a properly organised speech
sound system is called phonological development.
Phonological development involves three aspects:
the way the sound is stored in the child’s mind;
the way the sound is actually said by the child;
the rules or processes that map between the two above.
How easy should it be to understand young children's speech?
Table 1 provides a rough rule of thumb for how clearly your child should be
speaking. Bear in mind that there is considerable individual variation between
children. If you are in doubt about your own child's speech sound development an
assessment by a speech-language pathologist will quickly tell you if your child is 'on
track' and making the right combination of correct sounds and 'errors' for their age.
TABLE 1: How well words can be
understood by parents
By 18 months a child's speech is normally
25% intelligible
By 24 months a child's speech is normally
50 -75% intelligible
By 36 months a child's speech is normally
75-100% intelligible
Lynch, Brookshire & Fox (1980), p. 102, cited in Bowen
(1998).
Intelligibility to Parents
(18-36 months)
Table 1, above, provides a rough rule of
thumb for how clearly a child should be
speaking in the age-range 18 to 36
months. It is important to bear in mind
that there is considerable individual
variation between children. If, as a
parent, you are in doubt about your own
child's speech sound development or
speech clarity, an assessment by a
speech-language pathologist will quickly
tell you if your child is 'on track' and
making the right combination of correct
sounds and 'errors' for their age
What are the characteristics of young children's speech?
All children make predictable pronunciation errors (not really 'errors' at all, when you
stop to think about it) when they are learning to talk like adults. These 'errors' are
called phonological processes, or phonological deviations. Table 2 displays the
common phonological processes found in children's speech while they are learning
the adult sound-system of English. Further detail is provided on the typical speech
acquisition page.
Phonological Processes
COPYRIGHT 1999 CAROLINE BOWEN
All children make predictable pronunciation errors (not really 'errors' at all, when you
stop to think about it) when they are learning to talk like adults. These 'errors' are
called phonological processes, or phonological deviations. In Table 2 are the common
phonological processes found in children's speech while they are learning the adult
sound-system of English.
TABLE 2: Phonological Processes in Typical Speech Development
PHONOLOGICAL
PROCESS (Phonological
Deviation)
EXAMPLE
DESCRIPTION
Context sensitive voicing
"Pig" is pronounced and "big"
A voiceless sound is replaced by a
voiced sound. In the examples given, /p/
is replaced by /b/, and /k/ is replaced by
/g/. Other examples might include /t/
being replaced by /d/, or /f/ being
replaced by /v/.
"Car" is pronounced as "gar"
Word-final devoicing
"Red" is pronounced as "ret"
"Bag" is pronounced as "bak"
Final consonant deletion
"Home" is pronounced a "hoe"
"Calf" is pronounced as "cah"
Velar fronting
"Kiss" is pronounced as "tiss"
"Give" is pronounced as "div"
"Wing" is pronounced as "win"
Palatal fronting
"Ship" is pronounced as "sip"
"Measure" is pronounced as
"mezza"
Consonant harmony
"Cupboard" is pronounced as
"pubbed"
A final voiced consonant in a word is
replaced by a voiceless consonant.
Here, /d/ has been replaced by /t/ and /g/
has been replaced by /k/.
The final consonant in the word is
omitted. In these examples, /m/ is
omitted (or deleted) from "home" and /f/
is omitted from "calf".
A velar consonant, that is a sound that is
normally made with the middle of the
tongue in contact with the palate towards
the back of the mouth, is replaced with
consonant produced at the front of the
mouth. Hence /k/ is replaced by /t/, /g/ is
replaced by /d/, and 'ng' is replaced by
/n/.
The fricative consonants 'sh' and 'zh' are
replaced by fricatives that are made
further forward on the palate, towards
the front teeth. 'sh' is replaced by /s/,
and 'zh' is replaced by /z/.
The pronunciation of the whole word is
influenced by the presence of a
particular sound in the word. In these
"dog" is pronounced as "gog"
Weak syllable deletion
Telephone is pronounced as
"teffone"
"Tidying" is pronounced as
"tying"
Cluster reduction
"Spider" is pronounced as
"pider"
"Ant" is pronounced as "at"
Gliding of liquids
"Real" is pronounced as "weal"
"Leg" is pronounced as "yeg"
Stopping
"Funny" is pronounced as
"punny"
"Jump" is pronounced as "dump"
examples: (1) the /b/ in "cupboard"
causes the /k/ to be replaced /p/, which
is the voiceless cognate of /b/, and (2)
the /g/ in "dog" causes /d/ to be replaced
by /g/.
Syllables are either stressed or
unstressed. In "telephone" and "tidying"
the second syllable is "weak" or
unstressed. In this phonological process,
weak syllables are omitted when the
child says the word.
Consonant clusters occur when two or
three consonants occur in a sequence in
a word. In cluster reduction part of the
cluster is omitted. In these examples /s/
has been deleted form "spider" and /n/
from "ant".
The liquid consonants /l/ and /r/ are
replaced by /w/ or 'y'. In these examples,
/r/ in "real" is replaced by /w/, and /l/ in
"leg" is replaced by 'y'.
A fricative consonant (/f/ /v/ /s/ /z/, 'sh',
'zh', 'th' or /h/), or an affricate consonant
('ch' or /j/) is replaced by a stop
consonant (/p/ /b/ /t/ /d/ /k/ or /g/). In
these examples, /f/ in "funny" is replaced
by /p/, and 'j' in "jump" is replaced by
/d/.
Typical Speech Development
THE GRADUAL ACQUISITION OF THE SPEECH SOUND SYSTEM
Copyright © Caroline Bowen 1998 All rights reserved
Citing this article
This page contains an article about speech development. Cite it as: Bowen, C. (1998).
Typical speech development: the gradual acquisition of the speech sound system.
Retrieved from http://www.speech-language-therapy.com/acquisition.html on (date).
Anyone who has been around children who are under 5 years of age will
know that their speech sounds are not pronounced correctly all the time.
In fact a small, typically developing child's speech can be quite difficult to
understand because his or her sound system is not yet organised like adult
speech.
Articulation and Phonology Norms
Many researchers have studied children's acquisition of individual speech
sounds (phonetic development), and the way they organise these sounds
into speech patterns (phonemic or phonological development). Drawing on
this vast a varied body of research, Dr Sharynne McLeod of Charles Sturt
University in Australia compiled the pdf file here,[Adobe Reader
Required]. It contains an overview of typical speech development from a
range of researchers around the world, working from a variety of
theoretical perspectives.
Developmental norms and target selection
Gregory L. Lof PhD presented a fascinating poster entitled Confusion
about speech sound norms and their use in an online conference
sponsored by Thinking Publications in 2004, exploding a few myths about
normal (or 'normative') expectations and when to start therapy for
particular speech sounds.
Critical information
For Speech-Language Pathologists providing assessment and intervention
for Speech Sound Disorders, a detailed understanding of typical
('normal') development is critical to the understanding of delayed and
disordered development.
Intelligibility
Table 1 provides a rough rule of thumb for how clearly your child should
be speaking. If you are in doubt about your own child's speech sound
development an assessment by a speech-language pathologist will quickly
tell you if your child is 'on track' and making the right combination of
correct sounds and 'errors' for their age. Table 1 is available separately
here. See also: speech intelligibility from 12 to 48 months for a more
detailed discussion.
TABLE 1: How well words can be understood by parents
By 18 months a child's speech is normally 25% intelligible
By 24 months a child's speech is normally 50 -75% intelligible
By 36 months a child's speech is normally 75-100% intelligible
Source: Lynch, J.I., Brookshire, B.L., and Fox, D.R. (1980). A Parent - Child Cleft Palate Curriculum: Developing
Speech and Language. CC Publications, Oregon. Page 102
Phonological development
The gradual process of acquiring adult speech patterns is called
phonological development.
Phonological processes
All children make predictable pronunciation errors (not really 'errors' at all,
when you stop to think about it) when they are learning to talk like adults.
These 'errors' are sometimes called phonological processes, or
phonological deviations.
In Table 2 are the common phonological processes found in children's
speech while they are learning the adult sound-system of English. Table 2
is available separately here.
TABLE 2: Phonological Processes in Normal Speech Development
PHONOLOGICAL
PROCESS
(Phonological
Deviation)
EXAMPLE
DESCRIPTION
Context sensitive "Pig" is pronounced and "big" A voiceless sound is replaced
voicing
by a voiced sound. In the
"Car" is pronounced as "gar" examples given, /p/ is replaced
by /b/, and /k/ is replaced by /g/.
Other examples might include /t/
being replaced by /d/, or /f/
being replaced by /v/.
Word-final
devoicing
"Red" is pronounced as "ret"
Final consonant
deletion
"Home" is pronounced a "hoe" The final consonant in the word
is omitted. In these examples,
"Calf" is pronounced as "cah" /m/ is omitted (or deleted) from
"home" and /f/ is omitted from
"calf".
Velar fronting
"Kiss" is pronounced as "tiss" A velar consonant, that is a
sound that is normally made
"Give" is pronounced as "div" with the middle of the tongue in
contact with the palate towards
the back of the mouth, is
"Wing" is pronounced as "win"
replaced with consonant
produced at the front of the
mouth. Hence /k/ is replaced by
/t/, /g/ is replaced by /d/, and 'ng'
is replaced by /n/.
Palatal fronting
"Ship" is pronounced as "sip"
A final voiced consonant in a
word is replaced by a voiceless
"Bag" is pronounced as "bak" consonant. Here, /d/ has been
replaced by /t/ and /g/ has been
replaced by /k/.
"Measure" is pronounced as
"mezza"
Consonant
harmony
The fricative consonants 'sh'
and 'zh' are replaced by
fricatives that are made further
forward on the palate, towards
the front teeth. 'sh' is replaced
by /s/, and 'zh' is replaced by
/z/.
"Cupboard" is pronounced as The pronunciation of the whole
"pubbed"
word is influenced by the
presence of a particular sound
"dog" is pronounced as "gog" in the word. In these examples:
(1) the /b/ in "cupboard" causes
the /k/ to be replaced /p/, which
is the voiceless cognate of /b/,
and (2) the /g/ in "dog" causes
/d/ to be replaced by /g/.
Weak syllable
deletion
Telephone is pronounced as
"teffone"
"Tidying" is pronounced as
"tying"
Cluster reduction "Spider" is pronounced as
"pider"
"Ant" is pronounced as "at"
Gliding of liquids
"Real" is pronounced as
"weal"
"Leg" is pronounced as "yeg"
Stopping
"Funny" is pronounced as
"punny"
"Jump" is pronounced as
"dump"
Syllables are either stressed or
unstressed. In "telephone" and
"tidying" the second syllable is
"weak" or unstressed. In this
phonological process, weak
syllables are omitted when the
child says the word.
Consonant clusters occur when
two or three consonants occur
in a sequence in a word. In
cluster reduction part of the
cluster is omitted. In these
examples /s/ has been deleted
form "spider" and /n/ from "ant".
The liquid consonants /l/ and /r/
are replaced by /w/ or 'y'. In
these examples, /r/ in "real" is
replaced by /w/, and /l/ in "leg" is
replaced by 'y'.
A fricative consonant (/f/ /v/ /s/
/z/, 'sh', 'zh', 'th' or /h/), or an
affricate consonant ('ch' or /j/) is
replaced by a stop consonant
(/p/ /b/ /t/ /d/ /k/ or /g/). In these
examples, /f/ in "funny" is
replaced by /p/, and 'j' in
"jump" is replaced by /d/.
Elimination of phonological processes
Phonological processes have usually 'gone' by the time a child is five
years of age, though there is individual variation between children.
Table 3 lists the ages by which each of the processes are normally
eliminated. Ages are expressed as years;months. For example, 3;6
means 3 years 6 months. Table 3 is available separately here.
TABLE 3: Ages by which Phonological Processes are Eliminated
PHONOLOGICAL PROCESS
EXAMPLE
GONE BY
APPROXIMATELY
years ; months
Context sensitive voicing
pig = big
3;0
Word-final de-voicing
pig = pick
3;0
Final consonant deletion
comb = coe
3;3
Fronting
car = tar
3;6
ship = sip
Consonant harmony
mine = mime
kittycat = tittytat
3;9
Weak syllable deletion
elephant = efant
potato = tato
television =tevision
banana = nana
4;0
Cluster reduction
spoon = poon
train = chain
clean = keen
4;0
Gliding of liquids
run = one
leg = weg
leg = yeg
5;0
Stopping /f/
fish = tish
3;0
Stopping /s/
soap = dope
3;0
Stopping /v/
very = berry
3;6
Stopping /z/
zoo = doo
3;6
Stopping 'sh'
shop = dop
4;6
Stopping 'j'
jump = dump
4;6
Stopping 'ch'
chair = tare
4;6
Stopping voiceless 'th'
thing = ting
5;0
Stopping voiced 'th'
them = dem
5;0
Phonetic development
Table 4 outlines the ages by by which 75% of children in a carefully conducted
study accurately use individual speech sounds in single test-words. These
norms were established for a population of Australian children by Kilminster
and Laird (1978).
In column 3, the term 'voiced' refers to the vibration of the vocal cords while
the sound is being made. The term 'voiceless' is applied to sounds that are
made without vocal cord vibration. The terms fricative, glide, stop, nasal, liquid
and affricate refer to the way the sounds are made, or the "manner of
articulation". The International Phonetic Alphabet Charts summarise this
information here. Table 4 is available separately here.
Table 4: Normal phonetic development
Column 1
Column 2
Ages by which 75% of children Speech sounds
tested in a study accurately
used the speech sounds listed
in Column 2 in single words.
Column 3
The manner in
which the speech
sounds are
produced
3 years
Voiceless fricative
h as in he
zh as in measure
Voiced fricative
y as in yes
Voiced glide
w as in we
Voiced glide
ng as in sing
Voiced nasal
m as in me
Voiced nasal
n as in no
Voiced nasal
p as in up
Voiceless stop
k as in car
Voiceless stop
t as in to
Voiceless stop
b as in be
Voiced stop
g as in go
Voiced stop
d as in do
Voiced stop
3 years 6 months
f as in if
Voiceless fricative
4 years
l as in lay
Voiced liquid
sh as in she
Voiceless fricative
ch as in chew
Voiceless affricate
j as in jaw
Voiced affricate
s as in so
Voiceless fricative
z as in is
Voiced fricative
5 years
r as in red
Voiced liquid
6 years
v as in Vegemite
Voiced fricative
8 years
th as in this
Voiced fricative
8 years 6 months
th as in thing
Voiceless fricative
4 years 6 months
References
Bowen, C, (1998). Developmental phonological disorders. A practical guide
for families and teachers. Melbourne: ACER Press.
Grunwell, P. (1997). Natural phonology. In M. Ball & R. Kent (Eds.), The new
phonologies: Developments in clinical linguistics. San Deigo: Singular
Publishing Group, Inc.
Kilminster, M.G.E., & Laird, E.M. (1978) Articulation development in children
aged three to nine years. Australian Journal of Human Communication
Disorders, 6, 1, 23-30.
Lof, G.L. (2004). Confusion about speech sound norms and their use.
Thinking Publications Online Conference.
www.thinkingpublications.com/LangConf04/OLCIntro.html Accessed April 21
2004.
Lynch, J.I., Brookshire, B.L., & Fox, D.R. (1980). A Parent - Child Cleft Palate
Curriculum: Developing Speech and Language. CC Publications, Oregon.
Child speech professional discussion
Phonological Therapy is a discussion group for clinicians, including student
clinicians, speech and language researchers and university teachers. Most
participants are Speech-Language Pathologists and Linguists. Members explore
theoretical and research issues related to developmental phonological
disorders, childhood apraxia of speech, and other childhood speech sound
disorders, and their clinical management. Although interested consumers are
most welcome to join, please note that the group is for professional discussion
not consumer advice and support.
By what ages are phonological processes typically eliminated?
Phonological processes have usually 'gone' by the time a child is five years of age,
though there is individual variation between children. Table 3 lists the ages by
which each of the processes are normally eliminated.
Phonological
Development
THE GRADUAL ACQUISITION OF THE
SPEECH SOUND SYSTEM
COPYRIGHT 1999
CAROLINE BOWEN
TABLE 3: Elimination of Phonological
Processes
Phonological processes are typically gone by these ages (in
years ; months)
PHONOLOGICAL
PROCESS
EXAMPLE
Context
pig = big
GONE BY
APPROXIMATELY
3;0
sensitive
voicing
Word-final devoicing
pig = pick
3;0
Final
consonant
deletion
comb =
coe
3;3
Fronting
car = tar
ship = sip
3;6
Consonant
harmony
mine =
mime
kittycat =
tittytat
3;9
Weak syllable
deletion
elephant =
efant
potato =
tato
television
=tevision
banana =
nana
4;0
Cluster
reduction
spoon =
poon
train =
chain
clean =
keen
4;0
Gliding of
liquids
run = one
leg = weg
leg = yeg
5;0
Stopping /f/
fish = tish
3;0
Stopping /s/
soap =
dope
3;0
Stopping /v/
very =
berry
3;6
Stopping /z/
zoo = doo
3;6
Stopping 'sh'
shop =
dop
4;6
Stopping 'j'
jump =
dump
4;6
Stopping 'ch'
chair =
tare
4;6
Stopping
thing =
5;0
voiceless 'th'
ting
Stopping
voiced 'th'
them =
dem
5;0
What is articulation?
Articulation is a general term used in phonetics to denote the physiological
movements involved in modifying the airflow, in the vocal tract above the larynx, to
produce the various speech sounds. Sounds are classified according to their place
and manner of articulation in the vocal mechanism (Crystal,1991).
VPM
VOICE-PLACE-MANNER
of articulation
In the International Phonetic Alphabet consonant (pulmonic) chart you will see that
eleven places of articulation are displayed: bilabial (consonants made with both lips
in contact); labiodental (consonants made with contact between the lower lip and
upper teeth); and so on.
These places of articulation are cross referenced with the way, or manner in which
the sounds are produced. There are eight manners of articulation: plosive (or stop)
consonants in which the air-flow is stopped abruptly by the articulators; nasals, in
which the air flows down the nose; fricatives in which friction is created by the air
passing through lightly touching articulators; and so on.
The chart also indicates which consonants are voiced (like b, d, g, v, z, etc.) and
which are voiceless (like p, t, k, f, s, etc.). Where you see pairs of sounds (or
voiced and voiceless cognates) the voiceless sound is on the left, and the voiced one
on the right. When a voiced sound is produced the vocal cords in the larynx (voice
box) vibrate. When a voiceless sound is produced the vocal cords do not vibrate.
All the consonants of English can be classified in terms of "VPM" (voice-placemanner). For instance, /f/ is a voiceless labiodental fricative, and /b/ is a voiced
bilabial plosive (stop).
Click here for the 2005 version of the full chart
The International Phonetic Alphabet may be freely copied on condition that acknowledgement is made to the International
Phonetic Association (Department of Theoretical and Applied Linguistics, School of English, Aristotle University of Thessaloniki,
Thessaloniki 54124, GREECE).
Page updated
What are articulation development and phonetic development?
The terms 'articulation development' and 'phonetic development' both refer to
children's gradual acquisition of the ability to produce individual speech sounds. In
Table 4 is an outline the ages by which children use individual consonants with 75%
accuracy during conversation. more here
Phonetic Development
COPYRIGHT 1999 CAROLINE BOWEN
Table 4 outlines the ages by which 75% of the children in a study pronounced
individual consonants accurately. These norms were established for a population of
Australian children by Kilminster and Laird (1978).
In column 3, the term 'voiced' refers to the vibration of the vocal cords while the
sound is being made. The term 'voiceless' is applied to sounds that are made without
vocal cord vibration. The terms fricative, glide, stop, nasal, liquid and affricate refer
to the way the sounds are made, or the "manner of articulation". The International
Phonetic Alphabet Charts summarise this information here.
Table 4: Typical phonetic development
Age by which 75% of children
accurately use the speech
sound listed
Speech sounds
The manner in which the
speech sounds are produced
3 years
h as in he
Voiceless fricative
zh as in measure
Voiced fricative
y as in yes
Voiced glide
w as in we
Voiced glide
ng as in sing
Voiced nasal
m as in me
Voiced nasal
n as in no
Voiced nasal
p as in up
Voiceless stop
k as in car
Voiceless stop
t as in to
Voiceless stop
b as in be
Voiced stop
g as in go
Voiced stop
d as in do
Voiced stop
f as in if
Voiceless fricative
3 years 6 months
4 years
l as in lay
Voiced liquid
sh as in she
Voiceless fricative
ch as in chew
Voiceless affricate
j as in jaw
Voiced affricate
s as in so
Voiceless fricative
z as in is
Voiced fricative
5 years
r as in red
Voiced liquid
6 years
v as in Vegemite
Voiced fricative
8 years
th as in this
Voiced fricative
8 years 6 months
th as in thing
Voiceless fricative
4 years 6 months
References
Bowen, C. (1998). Developmental phonological disorders. A practical guide for
families and teachers. Melbourne: ACER Press.
.
Grunwell, P. (1997). Natural phonology. In M. Ball & R. Kent (Eds.), The new
phonologies: Developments in clinical linguistics. San Deigo: Singular Publishing
Group, Inc.
.
Kilminster, M.G.E., & Laird, E.M. (1978) Articulation development in children aged
three to nine years. Australian Journal of Human Communication Disorders, 6, 1, 2330.
The difference between an
articulation disorder and a
phonological disorder
Copyright 2002 Caroline
Bowen
Citing this article
This page contains an article about
speech disorders. Cite it as:
Bowen, C. (2002). The difference between an
articulation disorder and a phonological disorder.
Retrieved from www.speech-languagetherapy.com/phonetic_phonemic.htm on (date).
Familiar questions
A question from the parent of a four
year old with difficult-to-understand
speech:
What is the difference between an
articulation disorder and a phonological
disorder? How can you tell the difference?
Are they treated differently?
A question from a colleague:
Although I have been a school-based SLP
for over 20 years I have to say I am
confused about the distinction between
phonetic speech sound disorders, and
phonemic speech sound disorders. In
simple terms, what exactly is the
difference?
Speech
Speech is the spoken medium of
language. Speech has a phonetic level and
a phonological (or phonemic) level.
Phonetic (articulation) level
The phonetic level takes care of the motor
act of producing the vowels and
consonants, so that we have a repertoire
all the sounds we need in order to speak
our language.
Phonological (phonemic) level
The phonological or phonemic level is in
charge of the brainwork that goes into
organising the speech sounds into
patterns of sound contrasts so that we can
make sense when we talk.
Articulation (phonetic) disorder
In essence, an articulation disorder is a
SPEECH disorder that affects the
PHONETIC level. The child has difficulty
saying particular consonants and vowels.
The reason for this may be unknown (e.g.,
children with functional speech
disorders who do NOT have serious
problems with muscle function); or the
reason may be known (e.g., children with
dysarthria who DO have serious problems
with muscle function).
Typical speech development
Speech-Language Pathologists make a
detailed study of all aspects of normal
human communication and its
development in the areas of voice,
speech, language, fluency and
pragmatics. A thorough knowledge and
understanding of what science reveals
about typical speech development is
critical to our understanding of children's
speech sound disorders.
Language
Language has been called the
symbolisation of thought. It is a learned
code, or system of rules that enables us to
communicate ideas and express wants
and needs. Reading, writing, gesturing
and speaking are all forms of language.
Language falls into two main divisions:
receptive language (understanding what is
said, written or signed); and, expressive
language (speaking, writing or signing).
Phonological disorder
A phonological disorder is a LANGUAGE
disorder that affects the PHONOLOGICAL
(phonemic) level. The child has difficulty
organising their speech sounds into a
system of sound contrasts (phonemic
contrasts).
What is the difference
between an articulation
disorder and a
phonological disorder?
In an articulation disorder the child's
difficulty is at a phonetic level. That is,
they have trouble making the individual
speech sounds.
In a phonological disorder the child's
difficulty is at a phonemic level (in the
mind). This "phonemic level" is sometimes
referred to as "the linguistic level" or "a
cognitive level".
Co-occurrence
An articulation disorder and a phonological
disorder can co-occur. That is, the same
child can have BOTH.
Assessment and diagnosis
Because of their knowledge-base, SpeechLanguage Pathologists (SLPs) are able to
distinguish between the many speech and
language disorders they have to assess
(or "differentially diagnose") in the course
of their work.
The assessment process typically involve
screening the child's communication skills
in a general way, and then forming an
hypothesis about the nature of any
apparent difficulties.
If speech clarity is a problem the SLP will
examine both the PHONETIC and the
PHONOLOGICAL aspects of the child's
speech. The tests chosen will depend on
the child's presentation and the theoretical
beliefs of the clinician.
Use of terminology
Some SLPs use the term "articulation
disorder" very loosely, especially when
they are explaining these complex ideas
to people who do not have a background
in linguistics or speech pathology. Indeed,
they may refer to a "phonological
disorder" as an "articulation disorder".
It can often be quite helpful for parents to
ask their SLP what they mean by the
particular terms they use.
"Functional"?
The term "functional" speech disorder' is
usually equated with the concept of
"cause unknown" and these disorders are
often referred to as speech disorders of
unknown origin.
Although we cannot "prove" or
"demonstrate" what has "caused" a
speech sound disorder in a particular
child, we can often form justifiable
hypotheses regarding the likely cause,
given a child's history (Flipsen, 2002).
Factors such as family history, frequent
otitis media, developmental apraxia of
speech, and psychosocial factors
(Shriberg, 1993) may be considered.
Developmental?
The word "developmental" in
"developmental phonological disorders",
"developmental dysarthria", and
"developmental apraxia of speech" (the
preferred term is "childhood apraxia of
speech") simply denotes that the
disorders occur in children. The word
"developmental" is not appended to
functional speech disorders, which occur
in both children and adults.
Intervention
There is information about the treatment
of children's speech sound disorders here.
Discussion
The phonological therapy discussion
group provides communication disorders
professionals with an opportunity to ask
and answer questions and explore
theoretical and research issues related to
young children's speech sound disorders
in general, and developmental
phonological disorders, articulation
disorders, and developmental apraxia of
speech in particular. The emphasis is on
theoretically sound, evidence-based
clinical assessment and intervention
How are phonological and phonetic development related?
There is a complex relationship between phonological and phonetic development.
Normal speech development involves learning both phonetic and phonological
features.
The bulk of recent research into children’s speech development has dealt with
phonology: exploring and attempting to explain the process of the elaboration of
speech output into a system of contrastive sound units. In recent years, there has
also been a considerable body of research into the acquisition of motor speech
control, bringing with it a renewed interest in the nexus between phonological
development and phonetic development.
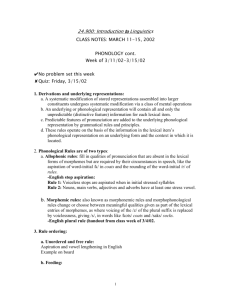
Phonological development and phonetic mastery do not synchronise precisely. A
common example of this asynchrony, referred to by Smith (1973) as the puzzle
phenomenon, is provided by children who realise /s/ and /z/ as 'th' sounds, while
producing "th-words" with [f] in place of voiceless 'th', and [d] or [v] in place of /ð/.
The Puzzle
Phenomenon
ASYNCHRONY BETWEEN
PHONETIC and PHONOLOGICAL
DEVELOPMENT
Caroline Bowen
Citing this article
This page contains an article about
speech development. Cite it as:
Bowen, C. (1998). The puzzle phenomenon:
Asynchrony between phonetic and phonological
development. Retrieved from http://www.speechlanguage-therapy.com/asynchrony.htm on (date).
Phonological development and phonetic
mastery do not synchronise precisely. A
common example of this asynchrony,
referred to by Smith (1973) as the puzzle
phenomenon, is provided by children who
realise /s/ and /z/ as 'th' sounds, while
producing "th-words" with [f] in place of
voiceless 'th', and [d] or [v] in place of
/ð/. The following classic example of
phonetic ability preceding phonological
execution came from a client, Andrew,
aged 4;6. The word on the left in each
case is the target word, and the word on
the right reflects Andrew's production.
some = thumb
thumb = fum
yellow = lello
zoo = thoo
then = den
those = doze
glove = gwub
breathe = bweeve
brother = bwuzzer
globe = blobe
rabbit = brabbit
Lexical selection
Evidence from studies of lexical selection
provides support for the view that children
are "aware" of their phonetic limitations
very early (i.e., during the first 50 words
stage) (Ferguson & Farwell, 1975;
Schwartz & Leonard, 1982). How
conscious the awareness is, of course is
uncertain, but children do seem to reflect
limitations of motor speech control in their
early word choices.
Does this mean that the speech motor
mechanism of young children is in fact
immature? Studies of duration, coarticulation (Kent, 1982; Hawkins, 1984)
and variability (Smith, Sugarman & Long,
1983) in children’s speech have
demonstrated that this is likely to be the
case. Hawkins (1984) reviewed a series of
comparative studies of child and adult
segment and phrase durations, concluding
that children tend to have longer
durations, and hence slower speech rate.
Hawkins also found that children show
greater intrasubject variability of speech
segment and phrase durations than
adults. Smith, Sugarman and Long (1983)
demonstrated that such variability was
due in large part to immaturity of the
neuromotor mechanism for the control of
speech movements.
Co-articulation
Co-articulatory ability, or the normal
capacity to produce an overlap between
speech sounds, caused by an overlapping
in the sequence of gestures which produce
them, has been thought by Kent (1983)
and others, to increase with age. Later
studies of co-articulatory ability (Repp,
1986, Sereno and Liebermann, 1987),
suggest that speech rate and variability
are more relevant predictors than the age
of the child. They showed that the
development of co-articulatory ability
varied widely from child to child, and that
the length of time a sound had been in a
child’s repertoire may be more significant
than chronological age in predicting coarticulatory ability. Sereno and
Liebermann (1987), in a study of children
aged 2;8 to 7;1, found no correlation
between age and co-articulatory ability.
Further evidence that phonetic development is
implicated in the development of phonological
contrasts comes from the frequent observation
that phonological contrasts are realised in the
child’s speech, albeit inaccurately, as they
gradually perfect their phonemic realisations of
target forms.
Children’s progress towards the adult targets of
/s/ and /r/, commonly via interdental and
labialised versions, respectively, are examples
of the "perfecting" process that takes place.
Menn (1983) summed up the complex (and
fascinating) interplay between the levels of
development and learning of phonological and
phonetic processing:
The mismatches between adult model and child
word are the result of the child’s trial and error
attempts; they are shaped by the child’s
articulatory and auditory endowments (and this
to that extent are ‘natural’) and by the child’s
previous success in sound production. All rules
of child phonology are learned in the sense that
the child must discover for herself each
correspondence between the sounds she hears
and what she does with her vocal tract in an
attempt to produce these sounds. (p. 44)
Developmental Phonological Disorders
What are developmental phonological disorders?
Developmental Phonological Disorders are a group of language disorders, whose
cause is unclear, that affect children’s ability to develop easily understood speech
patterns by the time they are four years old. Developmental phonological disorders
can also affect children's ability to learn to read and spell.
Developmental
Phonological Disorders
INFORMATION FOR FAMILIES
Copyright © 1998 Caroline Bowen
Citing this article
This page contains an article about phonological
disorder. Cite it as:
Bowen, C. (1998). Developmental phonological disorders:
Information for families.
Retrieved from http://www.speech-languagetherapy.com/parentinfo.html on (date).
What are developmental
phonological disorders?
Developmental Phonological Disorders (also called
"phonological impairments" or "phonological
disorders") are a group of language disorders that
affect children’s ability to develop easily understood
speech by the time they are four years old, and, in
some cases, their ability to learn to read and spell.
Phonological disorders involve a difficulty in
learning and organising all the sounds needed for
clear speech, reading and spelling.
They are disorders that tend to run in families.
Developmental phonological disorders may occur in
conjunction with other communication disorders such
as stuttering, specific language impairment, or
childhood apraxia of speech.
Synonyms
There is a little note here about the prevalent use of
the confusing and inappropriate term "phonological
processing disorder" and a list of some of the other
names that Developmental Phonological Disorders go
by!
What is involved in learning to
speak clearly?
The emergence in children of a properly organised
speech sound system is called phonological
development. Phonological development involves
three aspects:
the way the sound is stored in the child’s mind;
the way the sound is actually said by the child; and,
the rules or processes that map between the two
above.
Are these three aspects important
in therapy?
They are very important. Phonological therapy
always takes into account these three aspects, and the
fact that phonological development is a gradual
process for all children, whether they have
phonological problems or not. There is a range of
evidence based ("scientific") approaches to
phonological therapy.
Do all children with phonological
disorders need therapy?
No, some children simply need a little extra time to
catch up with their peers.
Most children with phonological disorders need more
time and speech-language pathology intervention
(speech therapy).
Assessment by a speech-language pathologist helps
determine what the particular needs of an individual
child are.
What are the characteristics of
phonological disorders?
Some children with developmental phonological
disorders have other speech and language difficulties
such as immature grammar and syntax, stuttering or
word-retrieval difficulties. However, many of them
just have a 'pure' developmental phonological
disorder, involving:
a problem with speech clarity in the preschool years,
with no subsequent reading and spelling problems, or
a problem with speech clarity in the pre-school years,
and, in the early school years, difficulty learning to
read, and difficulties with reading comprehension, or
speech and reading problems as described above,
plus difficulty with spelling, or
speech and spelling problems (i.e., no reading
difficulties), or
speech clarity problems in the pre-school years, and
difficulties with written expression in primary school.
Can the problems be treated?
Certainly! No matter what combination of difficulties
a child with a developmental phonological disorder
has, appropriate speech-language pathology treatment
is usually successful in eliminating or at the very
least, reducing the problem.
Why are reading and spelling
problematic?
Speech-Language Pathologists are constantly asked
the following two questions:
(1) "Why do some children, who have apparently
overcome their developmental phonological disorder,
in that their speech now sounds quite all right, have
reading and spelling problems?"
(2) "Why do they have difficulty with, or slowness in,
acquiring the pre-literacy skills that are a necessary
foundation for learning to read fluently with
understanding, spell, and produce written work?"
As parents and professionals we are finally beginning
to get some answers to these important questions.
Current research is showing that it is because these
children have poor phonological awareness in
particular, and poor metalinguistic ability generally.
Phonological awareness is the ability to recognise
and manipulate the sounds and syllables used to
compose words. Metalinguistic ability is the capacity
to think about and talk about language.
This is important!
Children with phonological impairments do not
necessarily go on to experience literacy problems, but
children who still have phonological disability in the
form of speech errors (especially those at the severe
end of the scale) when they start school, are very
much at risk for difficulties learning to read and spell.
This is one reason for wanting to treat them early, at
three or four years of age.
The other main reasons for treating children with
phonological disorders early are that it can be
frustrating, socially isolating, detrimental to selfesteem and confidence, and unpleasant generally, to
have speech that is difficult to understand compared
with the majority of children of similar age.
More information
If you have more questions and concerns about
developmental phonological disorders, or you would
like more information about children's speech sound
disorders, including childhood apraxia of speech
(CAS), go to this article. If you would like to read
about language development go to this article, and if
you would like to know more about how speech
develops, go here.
Are there other names for 'developmental phonological disorders'?
Developmental phonological disorders are known by many names including
'phonological disorder' and 'phonological dealay', and 'phonological impairment'.
Synonyms
FOR DEVELOPMENTAL
PHONOLOGICAL DISORDERS
Copyright © 1998 Caroline Bowen
Probably the best known synonym for
developmental phonological disorders
(Bowen, 1998) is 'phonological disability'
found in the early work of Ingram (1976),
and Grunwell (1981a, b). They are also
called phonological impairments.
As well, in the literature they are referred to
as: phonomotor disability (Folkins & Bleile,
1990), syntactic phonological syndrome
(Howell & Dean, 1991), phonological
disorder (Dean, Howell, Hill & Waters, 1990;
Fey, 1992; Kamhi, 1992; Stackhouse,
1993), and expressive phonological
impairment (Bird, Bishop & Freeman, 1995).
Dodd (1995) distinguished three distinct
types of phonological disorder (excluding
articulation disorders): delayed phonological
acquisition, inconsistent deviant disorder,
and consistent deviant disorder. Grunwell
and Russell (1990) also posited at least
three types, related to (1) form: the
inventory and contrastive system, (2)
function: the variability in the realisation of
adult contrasts, and (3) phonotactics (the
latter type discussed in detail in Grunwell &
Yavas, 1988).
There are references in the recent literature
to developmental phonological disorders as
other adjective-adjective-noun labels,
including permutations of the following, with
or without the word "learning", for instance,
developmental phonological learning
disorder (Gibbon & Grunwell, 1990):
functional
articulation
disorder
non-organic
phonologic(al)
disability
(ies)
developmental intelligibility
impairment(s)
child(hood)
phonetic
delay(s)
paediatric
speech
deviations
Misleading names!
Despite the fact that they are mentioned a
lot "phonological processing disorder",
"phonological process disorder" and
"phonological processes disorder" are not
synonyms for developmental phonological
disorder. They are inaccurate and
misleading terms and not proper SpeechLanguage Pathology diagnostic categories.
Somehow they have crept into the
vernacular - particularly in listservs, chat
and newsgroups. As an SLP and Clinical
Phonologist - I wish they would creep out
again!
References
Bird, J., Bishop, D.V.M., & Freeman, N.H.
(1995). Phonological awareness and literacy
development in children with expressive
phonological impairments. Journal of Speech
and Hearing Research, 38, 446-462.
Bowen, C. (1998). Developmental
phonological disorders: A practical guide for
families and teachers. Melbourne: The
Australian Council for Educational Research
Ltd.
Dean, E., Howell, J., Hill, A., & Waters, D.
(1990). Metaphon Resource Pack. Windsor,
Berks: NFER Nelson.
Dodd, B. (1995). Differential diagnosis and
treatment of children with speech disorder.
London: Whurr Publishers.
Fey, M.E. (1992). Clinical forum:
Phonological assessment and treatment.
Articulation and phonology: An introduction.
Language Speech and Hearing Services in
Schools, 23, 224.
Folkins, J., & Beale. K. (1990). Taxonomies
in biology, phonetics, phonology and speech
motor control. Journal of Speech and
Hearing Disorders, 55, 596-612.
Gibbon, F., & Grunwell, P. (1990). Specific
developmental language learning disabilities.
In P. Grunwell (Ed.). Developmental speech
disorders. Edinburgh, Churchill Livingstone.
Grunwell, P. (1981a). The nature of
phonological disability in children. New York:
Academic Press.
Grunwell, P. (1981b). The development of
phonology: A descriptive profile. First
Language, iii, 161-191.
Grunwell, P., & Russell, J. (1990). A
phonological disorder in an English-speaking
child: A case study. Clinical Linguistics and
Phonetics, 4, 29-38.
Grunwell, P., & Yavas, M. (1988).
Phonotactic restrictions in disordered child
phonology: A case study. Clinical Linguistics
and Phonetics 2, 1-16.
Howell, J., & Dean, E. (1991). Treating
phonological disorders in children: Metaphon
- theory to practice. San Diego: Singular
Publishing Group, Inc.
Ingram, D. (1976). Phonological disability in
children. London: Edward Arnold.
Kamhi, A.G. (1992). Clinical forum:
Phonological assessment and treatment. The
need for a broad-based model of
phonological disorders. Language Speech
and Hearing Services in Schools, 23, 261268.
Stackhouse, J. (1993). Phonological disorder
and lexical development: Two case studies.
Child Language Teaching and Therapy, 9, 2,
230-241.
Why do SLPs call the same thing by different names?
Good question!
Phonological processing disorder??!
There are two terms that are not included in the list of synonyms. They are
"phonological processing disorder" and "phonological processes disorder". Despite
their wide usage, these incorrect (and misleading) terms are not synonyms for
developmental phonological disorder. Neither are they names for closely related
speech sound disorders. They are "made up" terms that have somehow crept into
listservs and discussions. Even SLPs sometimes use them!
Synonyms
FOR DEVELOPMENTAL
PHONOLOGICAL DISORDERS
Copyright © 1998 Caroline Bowen
Probably the best known synonym for
developmental phonological disorders
(Bowen, 1998) is 'phonological disability'
found in the early work of Ingram (1976),
and Grunwell (1981a, b). They are also
called phonological impairments.
As well, in the literature they are referred to
as: phonomotor disability (Folkins & Bleile,
1990), syntactic phonological syndrome
(Howell & Dean, 1991), phonological
disorder (Dean, Howell, Hill & Waters, 1990;
Fey, 1992; Kamhi, 1992; Stackhouse,
1993), and expressive phonological
impairment (Bird, Bishop & Freeman, 1995).
Dodd (1995) distinguished three distinct
types of phonological disorder (excluding
articulation disorders): delayed phonological
acquisition, inconsistent deviant disorder,
and consistent deviant disorder. Grunwell
and Russell (1990) also posited at least
three types, related to (1) form: the
inventory and contrastive system, (2)
function: the variability in the realisation of
adult contrasts, and (3) phonotactics (the
latter type discussed in detail in Grunwell &
Yavas, 1988).
There are references in the recent literature
to developmental phonological disorders as
other adjective-adjective-noun labels,
including permutations of the following, with
or without the word "learning", for instance,
developmental phonological learning
disorder (Gibbon & Grunwell, 1990):
functional
articulation
disorder
non-organic
phonologic(al)
disability
(ies)
developmental intelligibility
impairment(s)
child(hood)
phonetic
delay(s)
paediatric
speech
deviations
Misleading names!
Despite the fact that they are mentioned a
lot "phonological processing disorder",
"phonological process disorder" and
"phonological processes disorder" are not
synonyms for developmental phonological
disorder. They are inaccurate and
misleading terms and not proper SpeechLanguage Pathology diagnostic categories.
Somehow they have crept into the
vernacular - particularly in listservs, chat
and newsgroups. As an SLP and Clinical
Phonologist - I wish they would creep out
again!
References
Bird, J., Bishop, D.V.M., & Freeman, N.H.
(1995). Phonological awareness and literacy
development in children with expressive
phonological impairments. Journal of Speech
and Hearing Research, 38, 446-462.
Bowen, C. (1998). Developmental
phonological disorders: A practical guide for
families and teachers. Melbourne: The
Australian Council for Educational Research
Ltd.
Dean, E., Howell, J., Hill, A., & Waters, D.
(1990). Metaphon Resource Pack. Windsor,
Berks: NFER Nelson.
Dodd, B. (1995). Differential diagnosis and
treatment of children with speech disorder.
London: Whurr Publishers.
Fey, M.E. (1992). Clinical forum:
Phonological assessment and treatment.
Articulation and phonology: An introduction.
Language Speech and Hearing Services in
Schools, 23, 224.
Folkins, J., & Beale. K. (1990). Taxonomies
in biology, phonetics, phonology and speech
motor control. Journal of Speech and
Hearing Disorders, 55, 596-612.
Gibbon, F., & Grunwell, P. (1990). Specific
developmental language learning disabilities.
In P. Grunwell (Ed.). Developmental speech
disorders. Edinburgh, Churchill Livingstone.
Grunwell, P. (1981a). The nature of
phonological disability in children. New York:
Academic Press.
Grunwell, P. (1981b). The development of
phonology: A descriptive profile. First
Language, iii, 161-191.
Grunwell, P., & Russell, J. (1990). A
phonological disorder in an English-speaking
child: A case study. Clinical Linguistics and
Phonetics, 4, 29-38.
Grunwell, P., & Yavas, M. (1988).
Phonotactic restrictions in disordered child
phonology: A case study. Clinical Linguistics
and Phonetics 2, 1-16.
Howell, J., & Dean, E. (1991). Treating
phonological disorders in children: Metaphon
- theory to practice. San Diego: Singular
Publishing Group, Inc.
Ingram, D. (1976). Phonological disability in
children. London: Edward Arnold.
Kamhi, A.G. (1992). Clinical forum:
Phonological assessment and treatment. The
need for a broad-based model of
phonological disorders. Language Speech
and Hearing Services in Schools, 23, 261268.
Stackhouse, J. (1993). Phonological disorder
and lexical development: Two case studies.
Child Language Teaching and Therapy, 9, 2,
230-241.
Are developmental phonological disorders something new?
No. In the past, a phonological disorder was termed a 'functional articulation
disorder', and the relationship between it and learning basic school work (like
reading and spelling) was not well recognised. Children were just thought to have
difficulty in articulating the sounds of speech. Traditional articulation therapy was
used to rectify the problem.
Is 'developmental phonological disorder' a 'functional articulation
disorder' under a different name?
'Developmental phonological disorder' is not simply a new name for an old problem.
The term reflects the influence of psycholinguistic theory on the way speechlanguage pathologists now understand phonological disorders. Nowadays, the
traditional diagnostic classification of 'functional articulation disorder' is falling into
disuse.
Children with phonological disability are usually able to use, or can be quickly taught
to use, all the sounds needed for clear speech - thus demonstrating that they do not
have a problem with articulation as such. In other words, we now know that the
problem is not a motor speech disorder. more here
Just to complicate matters, however, some children with developmental phonological
disorders also have difficulties with fine motor control and/or motor planning for
speech.
The difference between an
articulation disorder and a
phonological disorder
Copyright 2002 Caroline
Bowen
Citing this article
This page contains an article about
speech disorders. Cite it as:
Bowen, C. (2002). The difference between an
articulation disorder and a phonological disorder.
Retrieved from www.speech-languagetherapy.com/phonetic_phonemic.htm on (date).
Familiar questions
A question from the parent of a four
year old with difficult-to-understand
speech:
What is the difference between an
articulation disorder and a phonological
disorder? How can you tell the difference?
Are they treated differently?
A question from a colleague:
Although I have been a school-based SLP
for over 20 years I have to say I am
confused about the distinction between
phonetic speech sound disorders, and
phonemic speech sound disorders. In
simple terms, what exactly is the
difference?
Speech
Speech is the spoken medium of
language. Speech has a phonetic level and
a phonological (or phonemic) level.
Phonetic (articulation) level
The phonetic level takes care of the motor
act of producing the vowels and
consonants, so that we have a repertoire
all the sounds we need in order to speak
our language.
Phonological (phonemic) level
The phonological or phonemic level is in
charge of the brainwork that goes into
organising the speech sounds into
patterns of sound contrasts so that we can
make sense when we talk.
Articulation (phonetic) disorder
In essence, an articulation disorder is a
SPEECH disorder that affects the
PHONETIC level. The child has difficulty
saying particular consonants and vowels.
The reason for this may be unknown (e.g.,
children with functional speech
disorders who do NOT have serious
problems with muscle function); or the
reason may be known (e.g., children with
dysarthria who DO have serious problems
with muscle function).
Typical speech development
Speech-Language Pathologists make a
detailed study of all aspects of normal
human communication and its
development in the areas of voice,
speech, language, fluency and
pragmatics. A thorough knowledge and
understanding of what science reveals
about typical speech development is
critical to our understanding of children's
speech sound disorders.
Language
Language has been called the
symbolisation of thought. It is a learned
code, or system of rules that enables us to
communicate ideas and express wants
and needs. Reading, writing, gesturing
and speaking are all forms of language.
Language falls into two main divisions:
receptive language (understanding what is
said, written or signed); and, expressive
language (speaking, writing or signing).
Phonological disorder
A phonological disorder is a LANGUAGE
disorder that affects the PHONOLOGICAL
(phonemic) level. The child has difficulty
organising their speech sounds into a
system of sound contrasts (phonemic
contrasts).
What is the difference
between an articulation
disorder and a
phonological disorder?
In an articulation disorder the child's
difficulty is at a phonetic level. That is,
they have trouble making the individual
speech sounds.
In a phonological disorder the child's
difficulty is at a phonemic level (in the
mind). This "phonemic level" is sometimes
referred to as "the linguistic level" or "a
cognitive level".
Co-occurrence
An articulation disorder and a phonological
disorder can co-occur. That is, the same
child can have BOTH.
Assessment and diagnosis
Because of their knowledge-base, SpeechLanguage Pathologists (SLPs) are able to
distinguish between the many speech and
language disorders they have to assess
(or "differentially diagnose") in the course
of their work.
The assessment process typically involve
screening the child's communication skills
in a general way, and then forming an
hypothesis about the nature of any
apparent difficulties.
If speech clarity is a problem the SLP will
examine both the PHONETIC and the
PHONOLOGICAL aspects of the child's
speech. The tests chosen will depend on
the child's presentation and the theoretical
beliefs of the clinician.
Use of terminology
Some SLPs use the term "articulation
disorder" very loosely, especially when
they are explaining these complex ideas
to people who do not have a background
in linguistics or speech pathology. Indeed,
they may refer to a "phonological
disorder" as an "articulation disorder".
It can often be quite helpful for parents to
ask their SLP what they mean by the
particular terms they use.
"Functional"?
The term "functional" speech disorder' is
usually equated with the concept of
"cause unknown" and these disorders are
often referred to as speech disorders of
unknown origin.
Although we cannot "prove" or
"demonstrate" what has "caused" a
speech sound disorder in a particular
child, we can often form justifiable
hypotheses regarding the likely cause,
given a child's history (Flipsen, 2002).
Factors such as family history, frequent
otitis media, developmental apraxia of
speech, and psychosocial factors
(Shriberg, 1993) may be considered.
Developmental?
The word "developmental" in
"developmental phonological disorders",
"developmental dysarthria", and
"developmental apraxia of speech" (the
preferred term is "childhood apraxia of
speech") simply denotes that the
disorders occur in children. The word
"developmental" is not appended to
functional speech disorders, which occur
in both children and adults.
Intervention
There is information about the treatment
of children's speech sound disorders here.
Discussion
The phonological therapy discussion
group provides communication disorders
professionals with an opportunity to ask
and answer questions and explore
theoretical and research issues related to
young children's speech sound disorders
in general, and developmental
phonological disorders, articulation
disorders, and developmental apraxia of
speech in particular. The emphasis is on
theoretically sound, evidence-based
clinical assessment and intervention.
What is traditional articulation therapy?
There is no single definition of traditional articulation therapy. It is a term that is
applied to a number of therapy approaches that focus on the motor aspects of
speech production, with or without auditory discrimination training.
In essence, traditional articulation therapy involves behavioural techniques, focused
on teaching children new sounds in place of error-sounds or omitted sounds, one at a
time, and then gradually introducing them (new sounds that is) into longer and
longer utterances, and eventually into normal conversational speech.
Traditional Articulation
Therapy
Copyright © 1999 Caroline
Bowen
This page contains an article about
articulation therapy. Cite it as:
Bowen, C. (1999). Traditional articulation therapy.
Retrieved from http://www.speech-languagetherapy.com/TraditionalTherapy.htm on (date).
What constitutes the so-called
"traditional" approach to "articulation
therapy"? There is no single definition, for
indeed a number of beliefs and practices
may be involved, and the term clearly
means different things to different people,
depending on what they thought was
generally done.
Some of the procedures which have
characterised speech-language pathology
assessment and intervention for functional
speech disorders (articulation disorders),
and which may be considered by many
speech-language pathologists to embrace
"traditional" approaches, were described
by Powers (1971). She maintained that
the "stimulus methods" developed and
described by Travis (1931), had remained
the core of the majority of treatment
methodologies used by speech-language
pathologists.
Powers began her therapy with auditory
discrimination training. A sound was
identified, named, discriminated from
other speech sounds, and then
discriminated in contexts of increasing
complexity.
Permutations of the traditional approach,
always putting discrimination of sounds
produced by others first, are to be found
in Berry and Eisenson (1956), Carrell
(1968), Garrett (1973), Sloane and
Macaulay (1968) and and of course, Van
Riper (1978), who wrote:
"The hallmark of traditional therapy lies in
its sequence
of activities for: (1) identifying the
standard sound,
(2) discriminating it from its error through
scanning
and comparing, (3) varying and correcting
the various
productions until it is produced correctly,
and finally,
(4) strengthening and stabilizing it in all
contexts and
speaking situations." Van Riper, 1978 p.
179
Therapy resources designed for the
administration of traditional approaches to
speech therapy for children's speech
sound disorders continue to be published,
some incorporating aspects of other
programs and methodologies, and some
with evidence of internal development.
Adopting the role of teacher, the therapist
guides the child through a series of
carefully sequenced and graded steps,
usually one phoneme at a time. The
procedure starts with ear training, and
goes on through increasingly complex
production contexts. Finally the phoneme
is used in spontaneous conversational
speech, and the emphasis moves to selfmonitoring.
The child takes a passive learning role,
with active exploration and processing of
the sound system not specifically
encouraged. The approach, rather than
being communication centred, is "therapy"
centred, with the child learning what the
therapist sets out to teach.
Following the example of the medical
profession, published evidence of the
success of traditional approaches has
been mainly in the form of case
illustrations and clinical descriptions (for
example, Powers, 1971; Travis, 1931;
Van Riper & Irwin, 1959).
Is traditional therapy still an acceptable form of treatment?
Traditional therapy techniques, using the format outlined above, have withstood the
test of time, and can still be very suitable for children with functional speech
disorders.
What is a functional speech disorder?
A functional speech disorder is a difficulty learning to make specific speech
sounds. The index page for a series of articles about functional speech disorders is
here.
Children with just a few speech-sound difficulties such as lisping (saying 'th' in place
of 's' and 'z'), or problems saying 'r', 'l' or 'th' are usually described as having
functional speech disorders. But, you guessed it! There are synonyms for this too.
Functional speech disorders are often referred to as 'mild articulation disorders' or
'functional articulation disorders'. Examples include:
The
The
The
The
The
The
word
word
word
word
word
word
super pronounced as thooper.
zebra pronounced as thebra.
rivers pronounced as wivvers.
leave pronounced as weave.
thing pronounced as fing.
those pronounced as vose.
NOTE:
Some of these sound changes are acceptable in a number of English dialects.
FUNCTIONAL SPEECH
DISORDERS
What are
they?
Copyright 2004 Caroline
Bowen
Functional Speech Disorders INDEX
Difficulty with one, or just a
few sounds
Functional speech disorder is one of
several speech sound disorders that can
occur in children. A child with a functional
speech disorder has difficulty learning to
make a specific speech sound (e.g., /r/),
or a few specific speech sounds, which
may include some or all of these: /s/, /z/,
/r/, /l/ and 'th'.
Synonyms
Functional speech disorders are
sometimes referred to as "articulation
disorders", "functional articulation
disorders" or "articulation problems".
Functional speech disorders are not the
same thing as developmental phonological
disorders, developmental apraxia of
speech, or developmental dysarthria. The
similarities and differences between these
disorders are discussed in this article
about speech sound disorders.
The precise cause is unknown
By definition, the precise cause (or
causes) of functional speech disorders is
(or are) usually unknown. Even so, we do
know that structural (anatomical),
linguistic and environmental factors,
persistent ear infections associated with
intermittent hearing problems, and other
significant interruptions to a young child's
health and well-being, can impact
negatively on speech acquisition.
Assessment
All speech-language pathology
intervention is based upon individual,
ongoing assessment of a client's
communication skills. The therapist first
"screens" all areas of communicative
function, including voices, speech,
language, fluency and pragmatics, and
then does an in-depth assessment of
particular areas that may be problematic.
The assessment may include clinical
observations and standardised and nonstandardised tests.
Diagnosis
Informed assessment provides the basis
for diagnosis. The speech-language
pathologist is able to tell the young
client's carers, or the older client, what
the problem is, discuss the extent and
severity of the problem, and explore
treatment options.
Therapy (Treatment) Planning
Ideally, the Speech-Language Pathologist
will be able to propose a treatment plan
that he or she believes is both evidencebased (or theoretically sound) and optimal
for a particular client.
For example, a child of 5 who substitutes
/w/ for /r/ ("wabbit" for "rabbit") may be
offered 10 once-weekly therapy
appointments augmented by daily
homework (practice), then a break of
about four weeks, with a plan to review
progress at that time.
Parents would be given an expectation
that, with appropriate intervention and
good co-operation between clinician,
family and child, it would be reasonable to
expect the problem to resolve within 14
weeks or so. It would be explained that
some children require more or less
therapy than others.
Prognosis
A prognosis is a prediction about the likely
outcome of therapy. In general the
prognosis for the successful treatment of
functional speech disorders in children is
good.
However, the therapist may not feel ready
to talk about prognosis immediately after
assessment and diagnosis, preferring to
wait until the child has had a few
treatment sessions and until he or she and
his or her family is into a routine of doing
the necessary supervised home practice.
Prognosis may not be as positive if the
child does not comply with homework, or
does not receive appropriate
encouragement at home. There is more
information about homework below.
Therapy (Treatment) for
children
For many years Speech-Language
Pathologists have been remarkably
successful in treating individuals with
functional speech disorders using
evidence-based (scientific) traditional
and innovative approaches. There is an
intersting article on the ASHA web site
about former White House press secretary
Ari Fleischer who was successfully
treated for a functional speech disorder
when he was a child. Looking back on this
positive experience, Fleischer is quoted as
saying:
"I hope I can inspire children who have
lisps and others with speech disorders to
realize that it can be a phase in your life
that you deal with and go through, and it’s
over and you can still have a wonderful
future ahead.
And I also would say to all the speechlanguage pathologists and other health
care workers that you never know what
impact you are having on the children you
are treating today. In first grade, Dr.
Shulman made a difference in my life that
I’m sure he never anticipated at the time."
Therapy (Treatment) for adults
If they are not successfully treated in the
early years, functional speech disorders
can persist into adulthood, often causing
considerable distress. These adults may
have difficulty pronouncing just one or
two sounds, like /s/ and/z/, or just /r/, or
just /l/. On this page adults talk about
their experience of lisping.
With speech-language pathology
intervention and a monitored (by the SLP)
practice schedule, motivated adults often
overcome these disorders, achieving
"standard" speech sound production of
any of the sounds that were previously in
error.
Homework for children
There is research evidence to show that
supervised, appropriate homework
expedites therapy gains. "Supervised" in
this context means that homework tasks
have been devised by the clinician on a
case-by-case basis, in response to the
progress (or sometimes lack of progress)
made by the child.
Homework typically "builds" on previous
therapy sessions and previous homework.
Usually, the homework for week 1 is no
longer necessary in week 2, and so forth.
Because every child is different, progress
varies for each child. That is why the
therapist, in ideal circumstances, does not
want to hand out an intervention plan for
non-SLPs to administer without
supervision.
Unsupervised, or minimally
supervised home programs
Of course, "ideal" management is not
always possible, and the only intervention
option for some clients is a well-explained
home program, administered by parents
or significant others. With such home
programs it is highly desirable for the SLP
to review progress and provide ongoing
guidance at regular intervals.
"Please send me some
exercises!"
Many people email me requesting
exercises, or do-it-yourself programs to
correct their lisps and other speech sound
problems. The answer to these requests
has to be, sorry, but no.
Do-it-yourself therapy for
children
Understandably, parents often wonder
whether they can avoid the need,
inconvenience and costs of professional
intervention and help their children by
"treating" their lisps themselves using doit-yourself (DIY) approaches.
Even for very mild functional speech
disorders, appropriate intervention is best
administered by Speech-Language
Pathologists. SLPs are highly trained
professionals who have very specialized
knowledge and skills in relation to treating
speech difficulties.
"Do-it-yourself" therapy is inadvisable.
With the best will in the world parents and
others simply do not have the diagnostic
and intervention skills to accurately
diagnose and treat communication
impairments.
Do-it-yourself therapy for
adults
Similarly, resourceful adults frequently
search for self-help materials and
exercises.
But "do-it-yourself" therapy is inadvisable
for adults too, as is self-diagnosis.
If you are an adult with a speech
impairment that has persisted from
childhood, and you are keen to eliminate
it (not everyone is, mind!) do yourself a
favour and seek the professional
assessment and expert advice of a
Speech-Language Pathologist.
FUNCTIONAL SPEECH
DISORDERS
INDEX
A child with a functional speech disorder
has difficulty learning to make a specific
speech sound, or a few specific speech
sounds, particularly r, l, s, z and th.
Functional Speech Disorders: What
are they?
The web page "Functional speech
disorders: What are they?" provides brief,
plain English information about the
definition, characteristics, assessment and
treatment of functional speech disorders
in children and adults. Your questions
about do-it-yourself assessment and
therapy for children and adults are
answered.
What does 'functional' mean?
The way this term is used by SpeechLanguage Pathologists is briefly explained.
Normal expectations and atypical
production of /s/ and /z/
Typical speech development in children is
a gradual process and many children go
through a NORMAL stage of producing /s/
and /z/ with the tongue between the
teeth. In the article "Normal expectations
and typical production of /s/ and /z/"
typical phonetic ("articulation")
development is discussed, with particular
reference to /s/ and /z/.
Lisping: when /s/ and /z/ are hard to
say
This is the "original" article about lisping
on this site and as well as describing the
four types of lisp it includes links to
related information for professionals and
consumers.
What do the terms "lisp" and
"lisping" mean?
Some individuals, including some speechlanguage pathologists, do not like the
term lisp, perceiving it to carry a lot of
baggage, and would prefer it not to be
used in professional contexts. Specifically,
people in the gay community may object
to the term lisp, especially when it is used
in a pejorative, disparaging or belittling
way. Some of these issues are briefly
outlined in this article.
Letters to an SLP about lisping
I have been reading the information on
your site and have finally gotten up the
courage to write to you to ask your advice
about a lisping problem. I am 33 years
old...
SLPs talk about Lisping - Therapy for
Children
Opinions vary with regard to how difficult
or easy it is to help a child to overcome a
lisp, and how long it will take. My own
perception (this is about me if you are a
first-time visitor to this site and you would
like to know who is writing this!) is that
the treatment of lisps in motivated young
children is usually short-term and
successful...
Imagery and the Butterfly Position
The client is encouraged to think of the
tongue assuming the shape of a
butterfly...
Lateral /s/ Palatal /s/ - The Butterfly
Procedure
Allow the child time to master each step
before proceeding to the next. Slow and
steady (usually) wins the race!
What is the difference between an
articulation disorder and a
phonological disorder?
A simple explanation.
Related pages
Speech and language development in
infants and young children
Whether they speak early or late, are
learning one language or more, are
learning to talk along typical lines or are
experiencing difficulties, the language
acquisition of all children occurs gradually
through interaction with people and the
environment...Children's speech does not
sound like adult speech because they
make typical child-like "sound
replacements"...
Normal speech development / Typical
acquisition
Anyone who has been around children
who are under 5 years of age will know
that their speech sounds are not
pronounced correctly all the time. In fact
small children's speech can be quite
difficult to understand because their sound
system is not yet organised like adult
speech...
Q&A: Phonological Disorders,
Functional Speech Disorders, Apraxia,
Dysarthria
In this article the key similarities and
differences between typically developing
speech, functional speech disorders,
developmental phonological disorders and
childhood apraxia of speech (DVD/DAS)
are explained and discussed in a question
and answer format.
Bear in mind that there is considerable
individual variation between children. If
you are in doubt about your own child's
speech sound development an assessment
by a speech-language pathologist will
quickly tell you if your child is 'on track'
and making the right combination of
correct sounds and 'errors' for their age...
Developmental Phonological
Disorders / Caroline Bowen
Developmental Phonological Disorders
(also called "phonological disability" or
"phonological disorders", etc) are a group
of language disorders that affect children’s
ability to develop easily understood
speech by the time they are four years
old, and, in some cases, their ability to
learn to read and spell. Phonological
disorders involve a difficulty in learning
and organising all the sounds needed for
clear speech, reading and spelling. They
are disorders that tend to run in families...
Oral Motor Therapy: Exercises, Tools
and Toys
There is no need for oral motor exercises
(e.g., sucking and blowing exercises,
drinking thick-shakes through straws,
etc), oral motor tools (e.g., horns, straws,
etc) or oral motor toys (e.g., toy whistles,
trumpets, etc) in treating functional
speech disorders, developmental
phonological disorders or developmental
apraxia of speech.
Citing this article
This page contains an article about
lisping. Cite it as:
Bowen, C. (1999). Lisping: When /s/ and /z/ are
hard to say. Retrieved from http://www.speechlanguage-therapy.com/lisping.htm on (date).
There are several related articles on this
site:
1. Functional Speech Disorders INDEX
2. Letters to an SLP about lisping
3. SLPs talk about Lisping - Therapy
for Children
4. Functional Speech Disorders: What
are they?
5. Butterfly Procedure for Lateral /s/
and /z/
6. Beyond Lisping: Gay speech styles
and code switching
7. Typical speech development
8. What do the terms "lisp" and
"lisping" mean?
LISPING
When /s/ and /z/ are hard to say
Copyright 1999 Caroline Bowen
What is a lisp?
A lisp is a Functional Speech Disorder
(FSD). A functional speech disorder is a
difficulty learning to make a specific
speech sound, or a few specific speech
sounds.
The word 'functional' means that the
cause of the disorder is not
known. Indeed, in some (recent)
literature FSDs are referred to as "speech
delay of unknown origin" or "speech
disorder of unknown origin".
Functional speech disorders, or speech
delays of unknown origin, may persist into
adulthood. They can be treated
successfully in motivated children and
adults.
Historically, FSDs were referred to as
"dyslalia" and within that category,
difficulty saying /s/ and /z/ was called
"sigmatism".
Where does the problem lie?
The speech difficulty in a child with a
functional speech disorder is probably at a
phonetic level: that is, the child has a
particular difficulty producing certain
sounds correctly. Alternatively, the child
has learned to say a sound, or sounds, the
wrong way, and the incorrect
pronunciation has become a habit.
This is different from the situation of
children with developmental
phonological disorders who can usually
make the individual speech sounds, or be
taught to reasonably easily, but have
difficulties organising their speech sounds
into patterns. In these children
phonological processes persist beyond
typical age expectations.
Functional speech disorders are speech
disorders, while developmental
phonological disorders are linguistic
(language) disorders.
Co-occurrence
Functional speech disorders and
developmental phonological disorders can
co-exist, so you might find a child with a
developmental phonological disorder who
also lisps. In other words, and rather
more technically, phonetic and phonemic
speech sound deviations can occur in the
same individual.
A 'lay' term
Problems saying 's', 'z, 'r', 'l' and 'th' are
common in functional speech disorders. If
they use it at all, speech-language
pathologists usually use the lay term "lisp"
to refer to a difficulty achieving the
correct tongue position when pronouncing
the /s/ and /z/ sounds.
Characteristics of lisping
Typically, when a person lisps their tongue
either protrudes between, or touches,
their front teeth and the sound they make
is more like a 'th' than a /s/ or /z/.
Protruding the tongue between the front
teeth while attempting /s/ or /z/ is
referred to as 'interdental' production, and
touching the front teeth with the tongue
while attempting to produce /s/ or /z/ is
called 'dentalised' production.
There are two other types of lisp: the
lateral lisp, and the palatal lisp. In a
lateral lisp the person produces the 's' and
'z' sounds with the air escaping over the
sides of the tongue, while in a palatal lisp
they attempt to make the sounds with the
tongue in contact with the palate.
The four types of lisp are described in
more detail below.
Is a lisp ever 'normal'?
It is a perfectly normal developmental
phase for some (not all) children to
produce interdental or dentalised /s/ and
/z/ sounds until they are about 4½ years
of age. There are age norms here.
On the other hand, neither lateral or
palatal lisps are part of the normal
developmental progression. The speech of
a child with a lateral or palatal lisp should
be assessed, by a speech-language
pathologist, without delay.
Intelligibility
Lisping, as an isolated speech
characteristic, does not usually reduce the
person's intelligibility unduly. Most
people can easily understand what the
person with a lisp is saying.
Image
While there is usually little impact on
intelligibility, the impact of a lisp on a
child's "image" can be quite powerful. Of
course, some children grow up in an
environment where their lisp goes
unnoticed, or where it is not regarded as
cause for concern. Other children gain
positive recognition because they lisp,
particularly when the lisp is regarded as
sweet, funny, or endearing. By contrast,
others face criticism, ridicule, nagging and
teasing.
Grow up now
Sometimes children's lisps are regarded
as cute until they reach a certain age at
which time the same adults who have
almost been encouraging them to lisp
decide abruptly that it is high time they
"grew out of it". I have often wondered
what it can be like for four and five year
olds in this situation.
Four types of lisp
1. Interdental (frontal) lisp
In an interdental lisp (or frontal lisp) the
tongue protrudes between the front teeth
and the air-flow is directed forwards. The
/s/ and /z/ sound like 'th'.
Children developing speech along typical
lines may have interdental lisps until they
are about 4½ - after which they
disappear. If they don't 'disappear' an SLP
assessment is indicated.
Interdental /s/
Words such as 'soup', 'missing' and 'pass',
which all contain the voiceless alveolar
fricative consonant /s/ are pronounced
'thoop', 'mithing' and 'path'. The voiceless
'th' sound that occurs in a word like 'thing'
(or a sound very much like it) replaces the
/s/.
Interdental /z/
Words like 'zoo', 'easy' and 'buzz' which all
contain the voiced alveolar fricative
consonant /z/ are pronounced 'thoo',
'eethee' and 'buth'. The voiced 'th' sound
that occurs in a word like 'them' (or a
sound very much like it) replaces the /z/.
2. 'Dentalised lisp'
'Dentalised lisp' is not an 'official'
diagnostic term. It is an expression (like
'dentalised production') that SLPs use to
describe the way an individual is
producing certain sounds. The tongue
rests on, or pushes against, the front
teeth, the air-flow is directed forwards,
producing a slightly muffled sound.
Typically developing children (in terms of
their speech) may produce dentalised
variants of /s/ and /z/ until around 4½
years - and then grow out of it. If they
don't grow out of it, an SLP assessment is
indicated.
3. Lateral lisp
Lateral lisps are not found in typical
speech development. The tongue position
for a lateral lisp is very close to the
normal position for /l/ and the sound is
made with the air-flow directed over the
sides of the tongue. Because of the way it
sounds, this sort of lisp is sometimes
referred to as a 'slushy ess' or a 'slushy
lisp'. A lateral lisp often sounds 'wet' or
'spitty'.
Unlike interdental and dentalised lisps,
lateral lisps are not characteristic of
normal development. An SLP assessment
is indicated for anyone with a lateral lisp.
4. Palatal lisp
Palatal lisps are not found in typical
speech development. Here, the midsection of the tongue comes in contact
with the soft palate, quite far back. If you
try to produce a /ç/ - or a 'h' closely
followed by a 'y', and prolong it, you more
or less have the sound.
Unlike interdental and dentalised lisps,
palatal lisps are not characteristic of
normal development. An SLP assessment
is indicated for anyone with a palatal lisp.
'sh', 'zh', 'ch', 'j'
Sometimes children and adults who lisp
when they attempt to say /s/ and /z/ also
have tongue placement problems when
they try to say 'sh' as in 'shoe', 'zh' as in
measure, 'ch' as in 'chair', and 'j' as in
'jump'.
They may dentalise these sounds, or
produce them interdentally, or produce
them with lateral air escape, or with
excessive palate to tongue contact.
"...everything seems
interdental"
Some children produce many sounds
interdentally. Tongue protrusion, or very
'forward' or 'anterior' tongue placement
may be observed when they say not only
/s/, /z/, 'sh', 'zh', 'ch' and 'j', but also /n/,
/l/ and other sounds.
In some children "everything" seems
interdental. This may sometimes be an
indication that the nose is constantly
obstructed, due for instance, to allergy,
infection, large adenoids or craniofacial
anomalies, or may be associated with
habitual mouth breathing, tongue thrust,
or sucking habits.
Waiting
Studies to confirm it are unavailable as far
as I know, but I think most SLPs would
agree that in their clinical experience
there is a greater likelihood that children
will "grow out of" interdental or dentalised
lisps than lateral or palatal lisps.
I did a quick Web search and found a lot
of advice about lisping on the web - some
of it very accurate and sensible. It worried
me though, that many sites included the
advice to WAIT until a child is 7 or 8 years
of age before becoming concerned about
lisping.
Waiting well past 4½ is not good advice.
The longer the child waits the stronger
any "habit factor" will be. It is true that
some children are not ready for therapy at
4½, but it is advisable to let a properly
qualified professional (SLP / SALT) provide
guidance in relation to the individual child,
working on the results of face-to-face
assessment.
The "right" age for therapy for one child
may be different from the "right" age for
another, even within the same family.
Referral and assessment
Young children are usually referred for
assessment of lisps by their parents or
caregivers, often on the advice of preschool teachers.
It is, of course, uncommon for SLPs to
attempt to treat an interdental lisp, or
dentalised production of /s/ and /z/, in
children under 4½ years of age, because
it is regarded as normal for them to
produce the sounds that way. They may,
however, be interested in assessing
children under 4½ who are reported to be
lisping, in order to see whether it is a lisp,
and, if so, what type of lisp it is.
Treatment for a lateral or palatal lisp may
be appropriate in children under 4½.
The assessment process
Assessment involves screening all areas of
communicative function. The SLP takes a
detailed history, examines the anatomy of
the mouth and the movements it can
make (checking for tongue tie, palate
structure and function, swallowing
patterns and so on), takes a speech and
language sample for analysis, and
observes voice quality, fluency, and
semantic and pragmatic skills skills.
Sometimes it may emerge that although a
child is having difficulty saying /s/ and /z/,
he or she is not actually lisping. These
children may have some other speech
sound disorder.
Omitting /s/ and /z/ (sun = un, tease =
tee) or replacing them with consonants
like /w/ or /d/ (sun = wun, so = doe) are
not forms of lisping. Children with these
sound replacements may be having
phonological difficulties.
Therapy
In my own experience, and that of my
immediate colleagues, therapy for lisps in
young children is usually short-term and
successful. Opinions vary among speech
and language professionals with regard to
how difficult or easy it is to help a child to
overcome a lisp, and how long it will
usually take.
Most speech-language pathologists will
use a "Traditional Articulation
Therapy" approach, or variations of it
(see Judith Duchan's site for an
interesting history of its development).
Let's say that the client in the following
example has an interdental lisp. In
essence, her therapy will be like this:
1. We will determine that the client
2.
3.
can hear the difference between
/s/ and 'th' as individual sounds,
and in words (e.g., sink / think).
We will do some auditory
bombardment or focused auditory
input. There are word lists and
word contrasts here that could be
used at this stage.
Using tactile, auditory and motoric
cues we will teach the client to
make the new /s/ sound.
4. We will choose a word-position
(let's say, for the sake of the
example, that we choose the initial
position).
5. Using motor cues we teach the
client to imitate and the produce
independently /s/ in isolation
6. ... in broken syllables
(s-oo s-ee s-or s-ie s-oh...)
7. …in syllables
(soo see sor sie soh...)
8. …in words
(Sue see saw sigh sew...sun sip
soap...)
9. …in phrases
(so silly, send sam, seven seals)
10.
…in sentences
(I see a sock...)
11.
…in controlled
conversational contexts
(e.g., during dinner)
12.
…in conversation
13.
…phasing out modelling and
reinforcement
14.
...and working towards selfmonitoring and self-correction.
At each step in the process the client will
practice under the supervision of an adult.
Brief, frequent practice periods work best.
There is a good description of various
approaches and techniques in this book:
Bernthal, J.E., & Bankson, N.W. (1998).
Articulation and phonological
disorders.(4th ed.) Boston: Allyn and
Bacon.
The Butterfly Procedure
Imagery and the Butterfly Position
Adults who lisp
Functional speech disorders, such as lisps,
or difficulties saying /r/, /l/ or 'th' can
persist into adulthood, especially in people
who "dropped out" of therapy as children,
or who did not receive treatment.
No prrroblem!
Some adults who lisp have no desire to
seek therapy and are happy to accept
their speech the way it is. There are many
well known people (and and a few cats) in
public life, and some colourful characters
who have 'trade-mark' lisps as part of
their image or persona.
Frustration
But there are also adults who lisp who are
extremely unhappy about it. Some send
email (here are just a few examples)
expressing frustration, embarrassment,
and feelings of low self esteem and
defeat. They often fear that it may be 'too
late' to change their speech, and many of
them say that their lisp colours the way
other people regard them. It is quite
common, for example, for teenage boys
and young men to tell me that people
(incorrectly) assume that they are gay
because they lisp. Does that suggest that
to you that gay men who don't lisp are
actually straight? I don't think so.
Me Talk Pretty One Day by David
Sedaris provides an astonishing insight
into one person's experience of being
dragooned into "therapy" (for a lisp) in
the fifth grade. Essential reading for SLPs
who work with children.
The assessment process
Adults who lisp, and who do want help
generally seek the help of a speechlanguage pathologist on their own behalf,
often with the encouragement of a friend,
family member, colleague or partner.
Therapy
Therapy for adults is along the same lines
as therapy for children. Adults are usually
very motivated to practice, but they
sometimes find it difficult to find someone
to help them with their "homework". It is
vital to have someone to "supervise" your
practice, giving you accurate feedback,
and encouragement, just as a parent
would working with their own child.
Who can help?
The most effective way of managing a lisp
is to seek the professional services of a
speech-language pathologist. Some adults
like the idea of a do-it-yourself program,
but I have never actually heard of success
with one of these.
How do I find an SLP?
There are links to help you find services
here.
Page updated
http://www.speech-languagetherapy.com/lisping.htm
Is traditional articulation therapy an appropriate approach to treating
developmental phonological disorders?
The traditional approach is unsuitable for children with developmental phonological
disorders. SLP's who include phonological principles in their theory of intervention
believe that a 'phonological approach' should be used with children with phonological
disorders.
Phonological approaches to intervention, of which there are several, are called
'phonological therapy'.
Phonological
Principles
Copyright © 1999 Caroline
Bowen
"The defining characteristic of
phonological therapy is
that it is ‘in the mind’" Grunwell, 1988
The terms phonological therapy and
phonological remediation permeate the
current speech-language pathology
literature. They are often used
ambiguously, and it is not always clear
whether they refer to intervention for
developmental phonological disorders, or
intervention that is, by nature, somehow
'phonological'.
Phonological Therapy
The term 'phonological therapy' is used
throughout this web site to mean the
application of phonological principles to
the treatment of children with
developmental phonological disorders
(also called 'phonological impairment',
etc!). Stoel-Gammon and Dunn (1985,
page 168) provided a neat summation of
the principles of phonological therapy.
They believed that it:
(1) is based on the systematic nature of
phonology;
(2) is characterised by conceptual, rather
than motoric, activities; and,
(3) has generalisation as its ultimate goal
In general agreement, Grunwell (1985)
said that the aim of the therapy was:
"...to facilitate cognitive reorganisation of
the child’s phonological system and his
phonologically-oriented processing
strategies" (p. 99).
Similarly, Fey (1992) stated that:
"phonological therapy approaches are
designed to nurture the child’s system
rather than simply to teach new sounds"
(p.277).
PACT: A broad-based
approach
PACT (Bowen and Cupples, 1998a,
1998b) is a broad-based approach to
phonological therapy. Kamhi (1992) used
the term ‘broad-based’ when he argued
the need for a treatment methodology
that had some explanatory value, stating
that: "Such models are consistent with
assessment procedures that are
comprehensive in nature and treatment
procedures that focus on linguistic, as well
as motoric, aspects of speech" (p. 261).
What is phonological therapy?
The term phonological therapy refers to the application of phonological principles
to the treatment of children with phonological disability. Phonological therapy:
1. is based on the systematic nature of phonology;
2. is characterised by conceptual, rather than motoric, activities;
3. aims to facilitate age-appropriate phonological patterns through activities that
4.
encourage and nurture the development of the appropriate cognitive
organisation of the child’s underlying phonological system; and,
has generalisation as its ultimate goal.
Phonological
Principles
Copyright © 1999 Caroline
Bowen
"The defining characteristic of
phonological therapy is
that it is ‘in the mind’" Grunwell, 1988
The terms phonological therapy and
phonological remediation permeate the
current speech-language pathology
literature. They are often used
ambiguously, and it is not always clear
whether they refer to intervention for
developmental phonological disorders, or
intervention that is, by nature, somehow
'phonological'.
Phonological Therapy
The term 'phonological therapy' is used
throughout this web site to mean the
application of phonological principles to
the treatment of children with
developmental phonological disorders
(also called 'phonological impairment',
etc!). Stoel-Gammon and Dunn (1985,
page 168) provided a neat summation of
the principles of phonological therapy.
They believed that it:
(1) is based on the systematic nature of
phonology;
(2) is characterised by conceptual, rather
than motoric, activities; and,
(3) has generalisation as its ultimate goal
In general agreement, Grunwell (1985)
said that the aim of the therapy was:
"...to facilitate cognitive reorganisation of
the child’s phonological system and his
phonologically-oriented processing
strategies" (p. 99).
Similarly, Fey (1992) stated that:
"phonological therapy approaches are
designed to nurture the child’s system
rather than simply to teach new sounds"
(p.277).
PACT: A broad-based
approach
PACT (Bowen and Cupples, 1998a,
1998b) is a broad-based approach to
phonological therapy. Kamhi (1992) used
the term ‘broad-based’ when he argued
the need for a treatment methodology
that had some explanatory value, stating
that: "Such models are consistent with
assessment procedures that are
comprehensive in nature and treatment
procedures that focus on linguistic, as well
as motoric, aspects of speech" (p. 261).
References
Bowen, C. & Cupples, L. (1999a). Parents
and children together (PACT): a
collaborative approach to phonological
therapy. International Journal of Language
and Communication Disorders. Vol 34 No
1, 35-55.
Bowen, C. & Cupples, L. (1999b).A
phonological therapy in depth: a reply to
commentaries. International Journal of
Language and Communication Disorders.
Vol 34 No 1, 65-83.
Fey, M.E. (1992). Clinical Forum:
Phonological assessment and treatment.
Articulation and phonology: An
addendum. Language Speech and Hearing
Services in Schools, 23, 277 - 282.
Kamhi, A.G. (1992). Clinical forum:
Phonological assessment and treatment.
The need for a broad-based model of
phonological disorders. Language Speech
and Hearing Services in Schools, 23, 261268.
0
Grunwell, P. (1988). Comment on ‘Helping
the development of consonant contrasts’.
Child Language Teaching and Therapy, 4,
57-59.
Grunwell, P. (1985). Phonological
Assessment of Child Speech (PACS).
Windsor: NFER-Nelson.
0
Stoel-Gammon, C., & Dunn, C. (1985).
Normal and abnormal phonology in
children. Austin Texas: Pro-Ed. Inc.
Page updated
http://www.speech-language-
therapy.com/PhonologicalPrinciples.htm
Where does the problem (of phonological disorder) lie?
In essence, the child with a developmental phonological disorder has a language
difficulty affecting their ability to learn and organise their speech sounds into a
system of 'sound patterns' or 'sound contrasts'. The problem is at a linguistic level,
and there is no impairment to the child's larynx, lips, tongue, palate or jaw.
Does that mean there is no such thing as an articulation disorder?
Unfortunately, no. Children with "dyspraxia" (Childhood Apraxia of Speech) or a
dysarthria have articulation disorders (or motor speech disorders). Children with
anatomical (structural) differences such as cleft lip and palate, tongue-tie or other
cranio-facial anomalies may also have articulation disorders.
Tongue-tie
ANKYLOGLOSSIA or SHORT LINGUAL
FRAENUM
Copyright © 2000 Caroline Bowen
Citing this article
This page contains an article about
ankyloglossia. Cite it as: Bowen, C. (2000).
Tongue-tie, ankyloglossia or short fraenum.
Retrieved from http://www.speech-languagetherapy.com/tonguetie.html on (date).
The tongue
The most important articulator for speech
production is undoubtedly the tongue.
During speech, the amazing range of
movements the tongue can make include
tip-elevation, grooving, and protrusion.
Relatively short at birth, the tongue grows
longer, and thinner at the tip, as we get
older.
As well as having a speech function, the
tongue is needed for sucking, chewing,
swallowing, eating, drinking, tooth and
gum health, kissing, sweeping the mouth
for food debris and other particles (such
as hairs), warming the air during mouthbreathing, and oral play (for instance,
poking the tongue out and waggling it
about for fun).
More Pictures
Tongue-tie
In anatomy, a fraenum (or fraenulum) is a
small fold of tissue that checks or limits
the movements of an organ part.
Everyone has a lingual fraenum (lingual
fraenulum) under the tongue. It is a thin,
vertical fold of tissue with attachments to
the under-surface of the tongue and to
the floor of the mouth.
The terms 'ankyloglossia', 'short fraenum',
'short fraenulum', or 'tongue tie', refer to
a restricted lingual fraenum due to a
consolidation of tissue, usually leading to
reduced mobility of the tongue.
It is commonly observed that a person
with tongue tie cannot protrude the
tongue tip beyond the edges of the lower
incisors, or to the maxillary alveolar ridge
(behind the upper incisors). Sometimes
when a person with tongue tie attempts to
protrude the tongue it forms a
characteristic 'W' shape.
Parents of infants and toddlers with
tongue tie are sometimes advised that the
tie will "stretch", or "break" permitting a
free range of movement, as the child
grows. These stretching and breaking
phenomena have not been formally
studied or documented in the medical or
speech-language pathology literature.
Potential effects of tongue tie
1. Speech development
It is important to note that tongue tie
does not necessarily impair speech, in
fact, it rarely appears to do so. Many
individuals compensate well and have
normal sounding speech, even those with
the fraenum attached very close to the
tongue tip under the tongue. Some
individuals with tongue tie may have
imprecise articulation, especially at
speed.
2. Dental health
Cavities ('dental caries') can occur due to
food debris not being removed by the
tongue’s action of sweeping the teeth and
spreading saliva.
3. Periodontic health
Gingivitis (gum disease) can develop, for
the reason stated above.
4. Oral hygiene
Halitosis (bad breath) may be present,
due to caries and food debris.
5. Eating and digestion
Some children with tongue tie are messy
eaters due to a restricted ability to tidy up
inside and outside of their mouths while
they are having a meal. Some are unable
to circle their lips with their tongues in
order to fully lick their lips. In extreme
cases poor oral hygiene can lead to
digestive complaints.
6. Sexual function
Restricted tongue movements may affect
sexual expression.
7. Appearance
The tongue can be unduly obvious or
unusual looking in some individuals,
particularly when they are close up, or
appear on video, film or TV.
8. Oral play
Children in particular may not be able to
participate in play routines involving
tongue movements and gestures.
9. Self esteem
It has been noted clinically that occasionally an older
child or adult will be self-conscious, embarrassed or
resentful about their tongue tie.
Assessment
When asked by parents or dental or
medical colleagues to assess the need for
tongue tie surgery (frenectomy), a
speech-language pathologist takes into
account the above factors. They look at
the range of tongue movements, the two
points of attachment of the fraenum, and
speech development. As Purcell (2000)
cautions, not every tongue-tie requires
surgery:
"Tongue tie or ankyloglossia may impact
on accurate speech production, early
feeding and the ability to clean the teeth
with the tongue after meals or snacks.
However, these problems are usually
observed in only the more severe
instances of ankyloglossia. Thus, it is
important to note that each individual with
ankyloglossia requires a thorough
individual assessment and evaluation in
order for the most appropriate
management strategies to be selected."
Primary concerns for the speech-language
pathologist are the effects of the
ankyloglossia on the particular child’s
speech, dental and periodontic health and
oral hygiene. Subjective factors, such as
concerns about self-esteem, cosmetic
appearance, sexual function and oral play
tend to be the domain of the child’s
parents, with the speech-language
pathologist fulfilling an informationsharing role, if required.
Examining for tongue tie
In a typical initial consultation the speechlanguage pathologist conducts a case
history interview and assessment,
recording the following information:
Date
Name
Date of Birth
Age
Parents
Address
Telephone
History including family history and
language development
Presentation
Early feeding
Feeding now
Teeth
Tongue Movements
Appearance
Oral Hygiene
Saliva control (swallowing)
Phonological development (organisation of
the speech-sound-system),
Speech sound (phonetic) development
Speech clarity
Tongue tie surgery
Tongue tie surgery (lingual frenectomy)
involves more than just a simple clipping
or a quick snip, but more involved tissue
resection under general anaesthetic. It is
therefore not recommended unless there
is a good (speech, dental or other)
justification for doing it.
Lingual frenectomy and lingual
frenotomy are different procedures.
Lingual frenotomy is often performed on
newborns and neonates with tongue-tie to
enable them to latch and suckle. Lingual
frenotomy is sometimes referred to as
"tongue clipping". It is done with a local
anaesthetic. This is about frenotomy.
The potential for complications and
discomfort need to be discussed with the
surgeon and anaesthetist.
Some parents/caregivers like to seek two
speech-language pathology opinions to
help them make their decision whether to
not to proceed with tongue tie surgery.
Children should be assessed by a speechlanguage pathologist prior to tongue tie
surgery. Some require pre-operative
exercises, and most require postoperative exercises under a speechlanguage pathologist's supervision.
The purpose of post-operative
exercises
Post-operative exercises following tonguetie surgery are not intended to increase
muscle-strength, but to:
1. Develop new muscle movements,
2.
3.
particularly those involving tonguetip elevation and protrusion, inside
and outside of the mouth.
Increase kinaesthetic awareness of
the full range of movements the
tongue and lips can perform. In
this context, kinaesthetic
awareness refers to knowing where
a part of the mouth is, what it is
doing, and what it feels like.
Encourage tongue movements
related to cleaning the oral cavity,
including sweeping the insides of
the cheeks, fronts and backs of the
teeth, and licking right around both
lips.
Will the exercises improve
speech?
The exercises will not improve speech.
The article What is the evidence for
oral motor therapy? and the web page
Oral Motor Therapy: Exercises-ToolsToys explain that if you want to improve
speech, you have to work on speech.
Exercises
Discuss these suggested exercises with
YOUR child's speech-language pathologist
before commencing them. The SLP will
modify them according to your child's age
and requirements. Encourage oral play
generally, and do a selection of the
following exercises, in any order, in 3 to 5
minute bursts, once or twice daily for 3 or
4 weeks post-operatively. Have a torch
and hand-mirror handy. Make it fun.
1. Stretch your tongue up towards
2.
3.
4.
your nose, then down towards your
chin. Repeat.
You can vary the exercise above
and make it more interesting by
putting a dab of food in various
positions above the top lip, to be
retrieved with the tongue tip (You
could call this game "Elephant
Tongue" and read books about
elephants (e.g. "Babar") to
stimulate your child's interest in
playing the "tongue games"
spontaneously at other times - not
just when you are there.
Open your mouth widely. Touch
your big front teeth with your
tongue with your mouth still open.
Can you FEEL how tough your
teeth are?
Look in the mirror. Still with your
mouth open wide, say dar-dar-dar,
now say nar-nar-nar, now say tar-
tar. Look in the mirror to see what
your tongue is doing. Can you FEEL
where it is?
5. Lick your whole top lip from one
side to the other.
6. Now go back the other way.
7. Lick your whole bottom lip from
one side to the other.
8. Go back the other way.
9. See how many times you can lick
your lips right around.
10.
Poke your tongue out as far
as it will go.
11.
Shut your mouth and poke
it into your left cheek to make a
lump.
12.
Do the same on the other
side.
13.
Now see if you can make
your top lip fat without opening
your mouth.
14.
Can you go in-out-in-out-inout with your tongue?
(demonstrate)
15.
Put your tongue behind
your teeth and shut your mouth.
Can you find your big top teeth
with your tongue while your mouth
is still shut? FEEL how tough your
teeth are.
16.
Play your own version of
copy cats, Simon Says or Follow
the Leader incorporating the
preceding movements.
PLEASE - discuss these
suggested exercises with your
child's speech-language
pathologist before
implementing them. They may
not be necessary or appropriate
for your child.
Adolescents and adults with
tongue tie
This article
http://www.speech-language-
generates copious
correspondence! Having read it, numerous
young people and adults with tongue-tie
write to ask if it is "too late" for them to
have a lingual frenectomy.
therapy.com/tonguetie.html
Since all speech-language pathology
intervention is based on face-to face
assessment it would be impossible, as
well as unethical, for me to offer individual
advice (see DISCLAIMER). My
suggestion to these correspondents is for
them to start by seeking an opinion from
a speech-language pathologist.
SLPs as well as members of the
community and medical practitioners vary
in their views on the advisability of, and
the necessity for, tongue-tie surgery for
adults and children.
When frenectomy is performed, the
operation is likely to be done by a general
surgeon, an ENT surgeon, a cosmetic
("plastic") surgeon, or an oral surgeon.
The decision for an adolescent or adult to
proceed with frenectomy is arrived at
through consultation between the client,
the SLP and, of course, the surgeon.
Many people report that they have found
it difficult to access a surgical remedy
when they ask for a referral from their
own doctor, or approach a surgeon
directly (without an SLP opinion).
Links
Ankyloglossia: To clip or not to clip?
That's the question - an article by Ann
W. Kummer writing in the ASHA Leader,
10 (17), 6-7, 30. (Dec 27, 2005) See
also:
Perspectives on Tongue Tie
References
Oral Motor Therapy: Exercises - Tools
- Toys
This is an article about oral motor
exercises. The bottom line is, if you want
to improve speech, work on speech.
Tongue-tie: Impact on Breast Feeding
Complete Management Including
Frenotomy
This video, produced by a Canadian
doctor, Evelyn Jain, MD, CCFP, IBCLC is
intended to aid the physician in identifying
tongue-tie and performing frenotomy. It
demonstrates a comprehensive method of
assessment of the impact of tongue-tie on
breastfeeding, as well as a follow up
management plan for the lactation
consultant.
WEBWORDS 5- Craniofacial Web
Resources
ACQ Internet Column June 2000
What is the evidence for oral motor therapy?
This is another article about oral motor
exercises, driving the message home: if
you want to improve speech, work on
speech.
Page updated 7 November 2007
http://www.speech-languagetherapy.com/tonguetie.html
Webwords Index
Webwords 5
FACING THE WORLD
Craniofacial web resources
The ACQ Internet Column: June 2000
Caroline Bowen
How basic is this!
Thoughts about the fundamental
importance of having an intact anatomy
for speech production have been running
around my head for weeks. For the
themes of this edition of the ACQ (the
face, teeth, tongue and palate) take us
directly to our speech therapy roots,
making us think in the most
uncomplicated of ways about the organs
of speech: how they look and what they
do. How basic it is when we meet new
clients to start the assessment process by
taking a covert but informed squiz at their
faces. With a quick flash of the oral torch
we invite ourselves to an inside tour of
what they keep behind closed lips: you
know, the teeth the fairy hasn't claimed
yet, the tongue: thrusting, tied, or just
plain big, and the palate (I'll get to that
shortly)...all that sort of thing.
But sometimes the oral musculature
examination is deferred when we
encounter for the first time a client whose
facial features, in themselves, tell us
much of what we need to know, and
prompt us to reach for the journals to see
if there is anything helpful or new for the
client and clinician regarding Treacher
Collins Syndrome, Velo-Cardio Facial
(Shprintzen) Syndrome (here),
Craniosynostosis, or one of the myriad of
other conditions and diseases listed in the
NORD databases. NORD is the only
organization of its kind; a unique
federation of more than 140 not-for-profit
voluntary health organizations serving
people with rare disabilities. Its web site
receives more than 5 million hits each
year and over 1 million searches of its
databases are made annually.
I recognise your face from
somewhere...
With faintly satisfied smirks on their
famously photogenic faces, veteran BBC
interviewer Michael Parkinson and singer
and song writer Paul McCartney touched
upon the topic of being instantly
recognisable. Emphasising his
connectedness with a Liverpool working
class population, Paul told a well-seasoned
story against himself - and a funny one at
that! But it is hard to think of a funny
anecdote for a person to tell about the
times their face has been instantly
identified with a special "craniofacial"
population. Funny stories, no...but
poignant stories, inspirational stories,
brave stories...NOW you're talking. Take,
for example, the story of Kristi
Branstetter, an expert on arhinia.
Kristi writes: "I was born with congenital
total arhinia (complete absence of the
nose). I look at life like this: Things could
be worse...I feel good about myself most
of the time... I prefer to be around people
with positive attitudes so I can maintain
my own positive attitude... some people
are intimidated by my appearance...most
people are accepting. Those who reject
me just don't become a part of my life and
do not to get to know me as a person".
Read more about Kristi here.
Searches
Web searches
uncover a variety of
useful resources
including
www.cleftline.org,
and Peter Flipsen Jr's
Cranio-Facial
Anomalies links.
Tongue in cheek
With several copy deadlines looming the
temptation to drift off into (irrelevant)
cyberspace was easy to resist while
assembling these links. However, my
attention deficit did click in for a second
when I spotted The Tooth Fairy: A
Sceptical Analysis by Adrian Barnett. I
mean, who could resist Adrian's bio that
included the news that he is not only an
atheist, sceptic, and owner of three cats
and a thousand fleas, but also the world's
two-billionth greatest lover?
Tongue-tie
Someone else with a fascinating profile
that I've met on my Internet travels is
Evelyn Jain, a family physician and
lactation specialist in Calgary,
Canada. Evelyn was already the mother of
three daughters when she started medical
school "later in life", to use her
expression. She has been in Family
Practice for a decade and has a very busy
breastfeeding clinic. Finding that there
were babies who could not latch well even
with the best of maternal and professional
efforts she started clipping tight frenula in
1990, documenting excellent results. Dr
Jain describes the surgery as a simple and
safe procedure that is necessary when the
tongue movements in, out, and upwards
are limited. As a Clinical Assistant
Professor at the Faculty of Medicine she
was instrumental in getting lactation
established as part of the regular
academic and clinical curriculum at the
University of Calgary. In 1998 she won a
National Award of Excellence in Family
Practice for her innovative work in
breastfeeding, particularly regarding
infant tongue-tie.
Family ties
Evelyn is looking forward to addressing
the Australian lactation Consultants
Conference in Melbourne in October 2000
on the topics of Tongue-Tie and Breast
Reduction Surgery and their management
in the breastfeeding period. She is also
eagerly anticipating seeing her daughter
Kamini Jain compete in the kayak races at
the Sydney Olympics as a member of the
Canadian National Team.
Guess what?
Finally, here's a challenge that stumped
everyone, including me. In 12 words or
less: what are the most obvious unifying
characteristics of the tongue, salivary
glands and diaphragm? The answer can be
found on page 72 of the June 2000 ACQ.
Velo-Cardio-Facial
Syndrome Links
22q deletion, chromosome 22q11.2 deletion, Shprintzen
syndrome, DiGeorge syndrome
22q11 deletion syndrome
Development and Neurobiology
VCFS FAQ
Health Report
VCFS Information
VCFS Support
Home Page Webwords
Index
Page updated
http://www.speech-languagetherapy.com/webwords5.htm
Childhood Apraxia of Speech
What is dyspraxia?
Let's start with a reminder about what it is not! Childhood Apraxia of Speech is a
childhood speech disorder. It is NOT the same as "Apraxia" or "Dyspraxia" in adults
who have had strokes or head injuries.
Children with dyspraxia (or apraxia - both terms are as "correct" as any of the others
listed below) have the capacity to say speech sounds but have a problem with motor
planning. They have difficulty making the movements needed for speech,
voluntarily.
Dyspraxia can be mild, moderate or severe. It can apparently resolve with
appropriate therapy, in that the person's speech sounds acceptable, though the
underlying deficit probably remains forever. Alternatively, it can persist for a lifetime,
in the form of very little speech and / or very difficult to understand speech, despite
a great deal of appropriate therapy.
Is dyspraxia in children called by different names?
Dyspraxia in children is known by various names:
apraxia
apraxia of speech
developmental apraxia of speech [DAS]
childhood apraxia of speech [CAS]
suspected childhood apraxia of speech [sCAS]
developmental verbal dyspraxia [DVD]
developmental articulatory dyspraxia [DAD]
Why is dyspraxia in children called by different names?
On close reading of the literature, all the dyspraxia 'names' seem to mean the same
thing when it comes to looking at the actual symptoms or features of the child's
speech production, mouth movements and slow progress acquiring speech. The most
commonly used names for it are probably: developmental apraxia of speech [DAS],
developmental articulatory dyspraxia [DAD], and developmental verbal dyspraxia
[DVD]. Childhood Apraxia of Speech [CAS] is an insurance friendly newcomer that
has rapidly currency in the United States in recent years, and in the contemporary
research literature where the terms CAS and sCAS are used.
In general each of these terms refer to children who have the capacity (the neuromuscular wherewithal, if you like) to say speech sounds but who have a problem
with motor planning. Messages from the brain, intended to tell the speech
mechanism (larynx, lips, tongue, palate and jaw) what movements to make to
produce speech, do not occur easily for children with dyspraxia. This difficulty
comprises both a motor planning problem AND a difficulty 'retrieving' speech sounds
and patterns when they are required.
The characteristic speech of such children includes differences in the rhythm and
timing (prosody or 'melody') of speech and inconsistent speech sound errors. The
distinguishing characteristic of apraxia of speech is that it is a problem with motor
speech planning and programming, with NO weakness, paralysis or poor coordination of the speech mechanism.
It is probably safe to say that that whether researchers or clinicians call the disorder
DAS/CAS/sCAS, DAD or DVD, they would ALL agree that the features outlined above
are characteristic of the speech problem they are studying, assessing or treating.
It is also probably true to say that whatever term is being used to name the
problem, experienced clinicians at the 'grass roots' level will be drawing on a very
similar range of therapy techniques and activities.
All of which begs the question: so why call the problem by different names? There
are at least five main THEORIES that attempt to explain the basis of developmental
apraxia.
(1) It is due to an auditory processing problem
(2) It is a very specific 'specific language impairment' affecting language acquisition
at the sound-syllable-prosody level
(3) It is due to an organisational problem with sequencing the movements required
for speech
(4) It is due to a difficulty with making volitional (pre-planned, if you like)
movements for speech production
(5) It is due to various combinations of these factors.
Importantly, these are THEORIES that are currently being formulated and tested by
speech scientists. The fact is, we do not yet have a watertight explanation for
dyspraxia.
Many clinicians and researchers actually working with children in the "apraxia
population" who use the terms DAS and DAD tend to be those who veer towards the
"motor based" explanation.
Those who use the term DVD tend towards a "language based" explanation. Some
clinicians use the terms DAS and DVD interchangeably. Some, who embrace the
probability that the problem might be "linguistic" and "motor" in origin use
DVD/DAS.
Then again, there are clinicians who use terms such as these because they have
dropped into their clinical vernacular, in which case the term used does not reflect a
particular theoretical orientation.
What are the characteristics of
Childhood Apraxia of Speech?
To recapitulate, the distinguishing
characteristic of childhood apraxia of
speech is that it is a problem with motor
speech planning and programming, with
NO weakness, paralysis or poor coordination of the speech mechanism.
Some authorities believe that the primary
difficulty children with dyspraxia have is
with volitional (voluntary) movements of
the speech production mechanism.
Children with CAS, if they are able to talk,
usually make very variable articulation
errors, their speech is slow, it seems very
effortful to an onlooker, and there is a lot
of 'trial and error' involved in trying to
make particular sounds. The rhythm of
speech usually seems wrong to the
listener, and the child seems to put the
emphasis in all the wrong spots (that is,
there is something obviously unusual
about their prosody).
The key features that alert a speechlanguage pathologist to the possibility of a
CAS diagnosis in a young child are these:
1. The child may have no words, very
2.
3.
4.
few words, or up to 100 to 200
words in their vocabulary. They are
unlikely to be attempting to make
more than a handful of 2-word
combinations.
Some give the impression of
struggling to talk, exhibiting trial
and error attempts to say words,
accompanied by great frustration.
Many use self-taught signs and
gestures to augment
communication, which may include
a lot of ingenious body language
and facial expression. They MAY
use a lot of mime and gesture to
communicate. Some augment
signs and gestures with a
repertoire of sound-effects (car
noises, and the like) to good effect.
Their speech has several of these
characteristics:
i.
Words, in general, are not
clearly spoken, though
there may be remarkable
exceptions such as a very
clear (and useful!) 'no'.
Examples of this lack of
clarity might include 'ball'
being pronounced as 'or'
and 'knee' being
pronounced as 'dee'.
ii.
Speech errors affect vowels
as well as consonants. For
instance, 'milk' might be
pronounced 'mih', 'muh' or
'meh'.
iii.
Inconsistency is evident,
with the same word being
pronounced in several
different ways (e.g., 'me'
pronounced as 'ee', 'dee',
'bee' 'nee', or 'mee'). This is
called token-to-token
variability.
iv.
Sounds that are used in
some words are omitted
from other words. I knew a
child who could say 'p'
TWICE in the word 'Poppi'
(her grandfather) but who
pronounced both 'happy'
and 'puppy' as 'huh-ee'.
v.
vi.
vii.
When asked to imitate
speech sounds, sound
effects (e.g., car noises:
brm-brm etc) or words, the
child does not seem to know
where to start.
They may have unusual
intonation, pausing and
stress patterns.
They may not seem to know
where to "put" nasal
resonance.
5. Many of these children can
6.
UNDERSTAND LANGUAGE at a
more advanced level than their
limited speech would suggest. This
is sometimes called the ReceptiveExpressive gap.
They MAY not be able to easily
copy mouth movements (i.e., nonspeech movements) as well as
their age-peers, and they may be
(understandably!) reluctant to
imitate speech movements and
words.
Why is it referred to as a
'controversial' diagnosis?
Having said that CAS or sCAS is a motor
speech disorder, it is important to note
that it is a somewhat controversial
diagnosis, with some authorities seeing it
as a purely motor speech disorder with no
'language' (linguistic) component; others
seeing it as a linguistically based disorder;
others seeing it as a combination of these
two; with yet another group doubting its
very existence as a diagnostic entity!
What do you think?
My own position is that childhood apraxia
of speech does exist, as a complex
disorder and that no two children with it
will be precisely the same. It can range
from mild to severe.
Some children with CAS appear to have a
motor planning / programming problem
with little or no accompanying language
component. In my clinical experience this
is a rarity. Most appear to have a motor
planning / programming difficulty
combined with associated linguistic
difficulties, particularly phonological
problems and difficulties with expressive
grammar and syntax. I do not see these
language difficulties as part of the CAS,
but as difficulties that commonly occur
alongside the CAS.
While the idea of a purely linguistic, or
phonological basis (that is, no motor
planning component) for DVD is
intriguing, to date there is no convincing
research data to support such a view.
When can a developmental
dyspraxia diagnosis be made?
There is no actual AGE at which CAS can
be diagnosed for sure. It is more to do
with STAGE than age.
SLP's often have CAS on their 'short-list'
of probable diagnoses for children who are
late talkers with difficult-to-understandspeech (especially if they have feeding
difficulties and sensory integration issues
too) but we cannot be really sure until the
child has plenty to say, or, at the very
least, is making many speech attempts.
Ideally, the SLP has to be in a position to
do a detailed speech and language
assessment that includes analysing
speech movements, speech sounds,
speech patterns and speech rhythms. To
be able to do this the child has to be
attempting to say lots of words.
SLP colleagues and I have made
diagnoses of CAS in children who had
vocabularies of between 100 and 200
words, and who ranged in age from 2;3 to
4;6. We also know of several children for
whom a clear diagnosis of DAS was not
possible until after the age of 7.
The Dysarthrias
What is dysarthria?
The question should really be 'What are
the dysarthrias?' as dysarthrias have
many causes and characteristics. Children
with the various types of dysarthria have
a neuromuscular impairment. That is, the
speech mechanism (larynx, lips, tongue,
palate and jaw) may be paralysed, weak
or poorly co-ordinated.
Dysarthrias can affect ALL motor speech
processes: breathing, producing sounds in
the larynx, articulation, resonance, and
the 'prosody' or rhythm of speech.
Can phonetic disorders,
phonological disorders, dyspraxia
and the dysarthrias co-occur?
The disorders can occur, in varying
degrees, in the same individual. For
example, a child might have a severe
developmental phonological disorder with
mild dyspraxic features. Another child
might have dyspraxia with mild
dysarthria.
Can speech sound disorders occur
with OTHER communication
disorders?
Specific language impairment (SLI),
semantic-pragmatic language
disorder (SPLD), stuttering, voice
disorders and other communication
disorders can occur in the same child,
alongside phonological disorders,
dyspraxia and dysarthria.
Internet Information about
CAS
There is a lot of information on the
Internet relating to CAS. Some of it, for
example the material on the ApraxiaKids site with its well moderated listserv,
is helpful, authoritative and factual.
Unfortunately, the same cannot be said
about some of the other sites that are
"out there". Be selective in what you take
the time to read or print out, and ask your
child's Speech-Language Pathologist (or a
SLP colleague if you are a professional
seeking information) which sites they
recommend. When you visit a site, check
for yourself that the author has reliable
credentials.
When seeking out information about
Childhood Apraxia of Speech in the
Internet, proceed with caution, because
not everyone who claims to be a speech
and language expert is!
Handout
INFORMATION FOR FAMILIES
Childhood Apraxia of Speech
If this is all new to you...
Above all, if you are the parent of a child
who is in the process of diagnosis, or who
has recently been diagnosed with CAS,
get on with the therapy and try not to
jump ahead in time, worrying about
symptoms and situations that may never
arise for your child! And please be guided
by the SLP who knows your child as he or
she is the person who is most likely to be
able to provide you with really relevant
(even if sometimes uncomfortable)
answers.
Electronic discussion
Participate in professional discussion of
the issues raised in this article on the
phonologicaltherapy list.
Books by Caroline Bowen
1998
2007
2009 ABOUT
Page updated
الموقع
http://members.tripod.com/Caroline_Bowen/phonol-and-artic.htm