Testimony Regarding Consumer Medical Debt and Fair Debt
advertisement

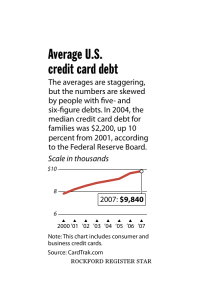
30 Winter Street, Suite 1004 Boston, MA 02108 Telephone: 617-338-5241 Fax: 617-338-5242 www.healthlawadvocates.org HealthLawAdvocates Fighting for Health Care Justice s PUBLIC HEARING RELATIVE TO 114.6 CMR 13.00: HEALTH SAFETY NET ELIGIBLE SERVICES BOARD OF DIRECTORS Wendy E. Parmet Ellen A. Bruce Jeffrey N. Catalano Michael S. Dukakis Paul W. Finnegan Ruth Ellen Fitch Daniel J. Jackson Diane Bissonette-Moes John E. McDonough S. Stephen Rosenfeld Thomas P. Sellers Eleanor H. Soeffing EXECUTIVE DIRECTOR Barbara Anthony VOLUNTEER LEGAL DIRECTOR S. Stephen Rosenfeld STAFF ATTORNEYS Matt Selig Lorianne Sainsbury-Wong Rebecca Rodman Rebecca Brink Mary Cyriac Georgia Maheras PARALEGAL Elaine Griffin Chris Haner OFFICE MANAGER Irene Nicolaides ADMINISTRATIVE ASSISTANT Laura Healey Before the Division of Health Care Finance and Policy August 22, 2007 Testimony of Health Law Health Advocates, Inc. Regarding Consumer Medical Debt and Fair Debt Collection Practices by Providers Presented by Barbara Anthony, Esq. Executive Director, Health Law Advocates Testimony before the Division of Health Care Finance and Policy regarding proposed regulation 114.6 CMR 13.00 August 22, 2007 Page 2 Introduction Good morning Commissioner Iselin and members of the Division. My name is Barbara Anthony, Executive Director of Health Law Advocates. We appreciate the opportunity to appear before you today to offer our comments on the Division’s proposed changes to regulations governing Health Safety Net Services. Health Law Advocates, Inc. (HLA) is a non-profit law firm affiliated with Health Care for All, a statewide consumer advocacy organization. Our clients are typically very low income people seeking access to health care. We represent clients for whom medical debt is a harsh reality. They may be uninsured, underinsured or facing coverage denials from aggressive payers. Medical debt is not discretionary. It is not the result of a spending spree for high end plasma TVs, computers or cameras. Medical debt incurred by consumer patients is the result of oftentimes unavoidable spending on necessary health care services. In this regard, medical debt is unlike other debt and as such consumers incurring medical debt should be accorded certain protections. These regulations present a unique opportunity for the Division to protect low-income consumers from the crush of medical debt. This testimony will address the need for regulatory safeguards to protect consumers who incur medical debt. There are a number of provisions in the proposed regulations that will add to the level of debt carried by consumer patients: 1. The proposed regulations exclude certain consumers categorically and these consumers must pay for all services out-of-pocket. 2. The proposed regulations impose premium like fees, deductibles and co-payments that taken together are unaffordable for low-income and even moderate-income consumers. 3. The expenses above would be in addition to lab fees, physician services, and followup care. While these additional expenses relate to changes in the Safety Net regulations, the Division should not overlook the debt that deductibles under health reform may cause a number of other consumers, who in some circumstances may use Safety Net resources as well. The Division, which has jurisdiction over hospitals and the way these providers treat consumers who incur medical debt, should take a broad look at this issue. The Division has regulations which regulate the way that hospitals treat low-income consumers who incur medical debt. Thus, in connection with these changes in the Safety Net, the Division is well within its jurisdiction to consider how these changes affect consumer debt and indeed, is within its jurisdiction to consider how the Massachusetts Health Reform Law will impact the way in which hospitals deal with consumers who incur medical debt. HLA urges the Division to strengthen these regulations to afford greater protections to consumers. Testimony before the Division of Health Care Finance and Policy regarding proposed regulation 114.6 CMR 13.00 August 22, 2007 Page 3 Commending the Division HLA commends the Division for strengthening the consumer protections in 13.08 (f)(4) by adding the language “interest free.” This change will make sure that consumers will have the best chance to pay off their medical debt. Compounding interest can make it impossible for a consumer to pay off an otherwise reasonable medical debt. We also appreciate the inclusion of “description of any program by which the hospital offers discounts from charges for the uninsured” in section 13.08(c)(2)(f). It is important to give consumers notice of the discount options available to them. This information should be available to the consumers themselves as well as in the Credit and Collection policies on file at the Division. Further, we feel the Division should consider expanding this to include discounts offered to the underinsured as well. Medical Debt is Based in Necessity Medical debt is a debt based in necessity and it is a hardship for the uninsured and underinsured. Not discretionary spending Medical debt is not discretionary; it is incurred for necessary health care treatments, payments and deductibles. Medical Debt is not usually planned in advance; accordingly, it is not predictive of a consumer’s creditworthiness. And while no hardship may be intended by the proposed changes and even by the Health Reform Law itself, all would agree that refinements in terms of affordability are still evolving and it is likely that costs will be imposed on those who cannot readily pay. Who is affected? Increasing numbers of individuals are unable to pay their bills for medical treatment and are accumulating significant amounts of medical debt. In one Massachusetts study, 40 percent of people questioned reported having some medical debt.1 Although many of those reporting medical debt are uninsured, having health insurance is not a guarantee against medical debt because health insurance coverage is not always sufficient to cover the entire cost of treatment. However, for those without insurance, any type of treatment can generate large medical bills as these individuals are charged the full cost of care and do not benefit from the reduced rates insurance companies generally pay. Consequences Medical debt can be a deterrent to seeking medical treatment for current health conditions. People already burdened by medical debt are hesitant to generate more bills.2 Medical debt can stretch an already tight budget even tighter and make it difficult to pay for other necessities. 1 Carol Pryor, Getting Care But Paying the Price: How Medical Debt Leaves Many in Massachusetts Facing Tough Choices, The Access Project, February 2004. 2 The Consequences of Medical Debt: Evidence from Three Communities, February 2003. Testimony before the Division of Health Care Finance and Policy regarding proposed regulation 114.6 CMR 13.00 August 22, 2007 Page 4 For some, overwhelming medical debt eventually leads to personal bankruptcy. In a recent bankruptcy study, one-third of debtors reported they had substantial medical debt.3 Medical debt reported to a Credit Reporting Agency will have a negative impact on consumers’ credit for at least seven years. For all of these reasons and more, the Division has sounds policy and legal reasons for addressing these issues. Certain uninsured consumers are excluded from the Safety Net and compelled to either incur medical debt or forego medical treatment Certain consumers are categorically excluded from the Safety Net and will be subject to paying for medical services out-of-pocket. Under the proposed regulations, the Health Safety Net Trust Fund establishes Health Safety Net – Primary, which provides MassHealth Standard type benefits to individuals with household incomes less than 200% of the federal poverty level (FPL). 114.6 CMR 13.04(6)(c)(2). This expansion of medical services available to consumers encourages a transition from emergency care to preventive care treatment and supports continued public health benefits. Eligible individuals, however, must be ineligible for MassHealth or Commonwealth Care. Those individuals eligible for MassHealth or Commonwealth Care but not enrolled are likewise exempt from the Health Safety Net – Primary benefits. 114.6 CMR 13.04(1)(2). However, not all consumers who are eligible for either state subsidized insurance program can afford the monthly premiums and co-payments. In addition, 114.6 CMR 13.04(1)(b)(5) provides that individuals who have access to affordable employer sponsored insurance under the affordability standards of the Commonwealth Health Insurance Connector Authority (“Connector”) are exempt from Health Safety Net - Primary. This puts the burden on consumers to seek Certificates of Exemption from the Connector and prove that their employer offered insurance plan is not affordable to them. The procedures and forms for applying for Certificates of Exemption are not yet ready, and there has been a lack of consumer education as to Certificates of Exemption. Moreover, no safety net exists for consumers when Certificates of Exemption are sought from the Connector because these consumers are categorically excluded from the Health Safety Net – Primary. As a result, consumers will be compelled to forgo medical treatment, pay out-of-pocket for services, or incur medical debt. Health Safety Net – Primary: Deductibles are unaffordable, and the Division provides no guidance on how consumers should track their deductibles Monthly deductible accumulations and the proposed consumer tracking of deductibles is impractical and will result in consumer aversion to use of Safety Net. Health Safety Net – Primary patients with income at 150-200% FPL must meet a $35.00 monthly deductible. 114.6 CMR 13.04(6)(c)(2). These deductibles accumulate monthly, regardless of whether or not services are used, from the date of the patient’s eligibility determination as identified by MassHealth. The 3 Melissa Jacoby, Teresa A. Sullivan & Elizabeth Warren, Rethinking the Debates over Health Care Financing: Evidence from the Bankruptcy Courts, New York University Law Review, May 2001. Testimony before the Division of Health Care Finance and Policy regarding proposed regulation 114.6 CMR 13.00 August 22, 2007 Page 5 maximum deductible of $420.00 yearly could well exceed the cost of services. Moreover, the fact that no deductibles apply to medical services received at Community Health Centers (“CHC”) that are exempt from the Critical Access provision under 114.6 CMR 13.03 is absolutely meaningless to consumers. Consumers cannot be expected to have knowledge about which CHC services subject them to a monthly deductible. Consider, for example, the situation of a consumer whose income is 200% FPL or $20,424 for an individual. If this consumer became eligible for the Safety Net in January 2008 but receives no services until December 2008 at a CHC which is not free-standing, the consumer will be responsible for a $420 accumulated deductible. This deductible could exceed the cost of medical treatment. This consumer was unknowingly accumulating a $35.00 monthly deductible with no understanding whatsoever as to the basis for the debt owed until medical treatment is needed. A patient responsibility of $420.00 for the medical service results in consumer medical debt. Consumers will be ill-equipped to track and document the deductibles, especially if there is more than one family member or more than one hospital involved. In addition, there is no cap on cost sharing to consumers in households, especially larger families. Consumers at income levels of 150-200% FPL are extremely vulnerable and will be unable to pay the monthly accumulated deductible. Such deductible tracking is not generally imposed upon patients seeking medical care. At a minimum, the Division must provide simple and easy to understand protocols for consumers on to how to track deductibles. Consumers eligible for Partial Health Safety Net should not be subjected to additional cost sharing such as co-payments HLA recommends that the Division not impose additional cost sharing burdens on Partial Health Safety Net consumers who are already subject to meeting a yearly deductible. Individuals with incomes greater than 200% and not more than 400% FPL are eligible for Partial Health Safety Net coverage. These individuals must first meet a deductible that is computed by taking 40% of the difference between the household income and 200% FPL for the same household size.4 Adding cost sharing and co-payments in addition to the yearly deductible calculation is onerous and unaffordable for these consumers. Neither MassHealth nor Commonwealth Care imposes a deductible, except for nonworking members of MassHealth Commonhealth. The Safety Net should not burden these consumers by imposing additional cost sharing such as co-payments. HLA further recommends that the Division include a Section 13.06 in the proposed regulations to define the annual deductible formula. The Safety Net is not an insurance plan and should avoid mirroring insurance cost sharing The Health Safety Net is not an insurance plan for consumers, yet its cost sharing mirrors the premiums and co-payments under the state’s subsidized health insurance plan, Commonwealth Care. Consumers who access the Safety Net, unlike consumers who are members of a health plan, 4 Although 114.6 CMR 13.06 is inadvertently omitted from the proposed regulations, it appears that the Division of Health Care Finance and Policy’s intent was to establish a yearly deductible for Partial Health Safety Net consumers consistent with the existing regulations governing the Uncompensated Care Pool, 114.6 CMR 10.03 (2)(b). Testimony before the Division of Health Care Finance and Policy regarding proposed regulation 114.6 CMR 13.00 August 22, 2007 Page 6 are uninsured, receive no membership card and none of the protections and rights accorded to health plans members. There are no defined patient benefits under the Safety Net as found in health insurance plans. Imposing insurance-plan cost sharing on patients who access the Safety Net is inappropriate because Safety Net patients are uninsured. In addition, consumers could be misled into thinking that they are members of a health plan, and believe they are entitled to receive benefits that are not available. These consumers are subject to the Individual Mandate and will therefore already be responsible for tax penalties for noncompliance as of 12/31/07. In order to avoid confusion, HLA recommends that the Division outreach to consumers who are eligible for the Safety Net. Consumers should be informed that the Safety Net does not constitute a health insurance plan and, thereby, fails to satisfy the Individual Mandate. Consumer education must include notice and instructions to patients accessing the Safety Net. These consumers may be required to seek Connector approval via a Certificate of Exemption in order to avoid tax penalties for noncompliance with the Individual Mandate. Cost sharing increases consumer medical debt The fact that there is no cost sharing for medical services to consumers with incomes below 200% FPL5 who access services at free-standing CHC’s is meaningless. Consumers cannot be expected to know which CHC’s are exempt from the critical access provision. Those consumers who live closest to non-free standing CHC’s will be inadvertently penalized by paying more out-ofpocket. That may mean that Consumers residing in urban cities and towns will incur increased cost sharing for accessing medical care at hospital-licensed CHC’s. Low income consumers have limited income and cannot afford to pay cost sharing. The Safety Net should, therefore, continue to cover medically necessary services provided by hospitals and health centers without imposing additional costs on consumers. The cumulative effects of copayments of $5 for outpatient services, $50 for an emergency room visit (waived if admitted), $50 for an inpatient admission, $1 for a generic drug, and $3 for a single source drug are simply unaffordable to low income consumers. Cost sharing will increase consumer medical debt or force some consumers to avoid medical treatment due to expense. The Safety Net compels consumers to incur substantial medical debt due to cost sharing. It also compels consumers to incur medical debt for any services received from providers other than hospitals or community health centers. Even if consumers seek services at hospitals or CHC’s, there is no guarantee that additional medical debt will not incur. Reimbursable services under 114.6 CMR 13.03(2) et seq. relate to inhouse medical services. The proposed rules continue this practice. Reimbursable services fail to account for medical services rendered at hospitals or CHC’s that are billed by private physician organization groups, external laboratories, and/or other independent medical providers who do not bill directly through the site of treatment. Consumers will mistakenly believe they have complied with the Safety Net eligible services requirements of 114.6 CMR 1303 by seeking medical treatment hospitals or CHC’s. Independent providers will then bill the consumers separately 5 It appears that the Division intended to exempt children in with family incomes below 200% FPL from all cost sharing, including both co-payments and deductibles. The proposed regulations, however, only specifically exempt these children from co-payments. 114.6 CMR 13.04(6)(a)(1)(c) Testimony before the Division of Health Care Finance and Policy regarding proposed regulation 114.6 CMR 13.00 August 22, 2007 Page 7 because those services are not covered by the Safety Net. Consumers have no way of knowing this. Consumers cannot be expected to know whether a treating physician at a hospital or CHC is actually an independent provider. In addition, the scope of benefits is not defined under the Safety Net in part because consumers can only receive from the hospital or CHC those medical services that the facility already provides. Consequently, uninsured patients may fail to receive additional services not offered at the hospital or CHC, and it may be more difficult for physicians to arrange specialty or nonemergency care for uninsured patients. This burdens consumers with unanticipated and unavoidable medical bills and debt. In addition, HLA recommends that the Division clarify the proposed regulations so that children in household incomes of no more than 200% are exempt from all cost sharing, including co-payments under 114.6 CMR 13.04(6)(a)(1)(c) and monthly deductibles. The Safety Net should provide a Hardship Waiver process The Safety Net’s eligibility exclusions oust from covered medical services those consumers who, through not fault of their own, receive erroneous determinations by MassHealth in regard to their eligibility for MassHealth or Commonwealth Care or whose enrollment into state-subsidized insurance is otherwise delayed. These consumers receive neither six month retroactive coverage nor gap in coverage state-subsidized medical services from the Safety Net. In addition and as discussed above, some consumers who are eligible for MassHealth or Commonwealth Care are unable to afford the premium payments and applicable co-payments, if any. Because they are eligible for CommCare and cannot afford the premiums, they will be uninsured but ineligible for the Safety Net. Consumers may also be unable to afford employer offered insurance. Accessing medically necessary health care through the Safety Net is the only means by which these persons can obtain the services needed. Accordingly, HLA recommends that the Division allow consumers to demonstrate the severity of their hardship situations and to be waived into the Safety Net, even though otherwise excluded under the proposed regulations. Such wavier providers under the Safety Net ought to be more flexible, generous and robust than those of CommCare. HLA proposes that the Division establish a broad Hardship Waiver process and promulgate regulations consistent with the intent that the Safety Net serve as a last resort of state-subsidized medical care for disadvantaged consumers. HLA urges the Division to permit consumers an opportunity to be heard on their individual or family hardship factors through a Hardship Waiver process that is faire and responsive to the needs of the uninsured. Collecting bad debt Section 13.05 of the proposed regulations governs claims for emergency bad debt. Hospitals and CHC’s must first undertake collection actions before submitting claims for payment by the Fund. Such required collection action includes reasonable efforts to obtain the financial information necessary to determine responsibility for payment of the hospital bill from the patient or guarantor and reasonable efforts to verify patient supplied information. Moreover, the actions that the hospital must take before writing off an account to the Health Safety Net under 114.6 CMR 13.05(3) are substantially similar to existing Free Care requirements under 114.6 CMR 12.04(2). Hospitals are now, however, required to submit a claim for each inpatient bad debt, and CHC’s are Testimony before the Division of Health Care Finance and Policy regarding proposed regulation 114.6 CMR 13.00 August 22, 2007 Page 8 required to submit a claim for all urgent bad debt. Hospitals and CHC’s are required to provide the Health Safety Net Office with evidence of reasonable collection efforts. 114.6 CMR 13.05(1)(d)(2)[sic.]6 Consumer protections regarding debt collections should be strengthened to protect consumers from medical debt and unfair collection practices HLA highlights below the proposed changes to the debt collection practices that fail to adequately protect consumers: There is no longer any protection for consumers who serve as guarantors of medical debt. The proposed regulations omit a prohibition on providers’ obtaining an execution against the personal residences or motor vehicles of guarantors. Consumer protection remains in place for low income patients, e.g., those patients with family incomes not greater than 400% FPL. 114.6 CMR 13.04(1)(a) The proposed regulations, however, are silent with respect to use of lawsuits, wage garnishments, and other collection efforts. The proposed regulations force a medical distinction between emergency services and urgent care. That means that if a doctor determines a patient’s medical need was not an emergency but was an urgent care need, then the provider receives no reimbursement for services except for screening services. Consumers will be billed in full for the services. 114.6 CMR 13.05(2)(b). While the proposals above weaken protections for consumers, this is occurring against a backdrop of hospitals and CHCs imposing so-called “charges” on patients who are uninsured or sometimes on those who are underinsured. Hospitals and CHC’s should be precluded from charging low-income consumers the highest rates. Consumers’ bills for non covered services should be limited to the Medicare/MassHealth rate as the maximum rate charged. Charging the highest rates to uninsured consumers who are most vulnerable and least able to pay – the poor people’s premium-- will result in increased medical debt. It is fundamentally unfair that uninsured consumers accessing necessary medical care are billed more than the Medicaid/MassHealth rate. For these reasons, HLA recommends that the Division ensure that the rates charged to uninsured patients are capped at the MassHealth rate. Moreover, uninsured patients should receive information about financial assistance programs when they receive and again when they are billed for services. The negative impact of “bad debt" creates a stigma for consumers. Even if a hospital or CHC has written off the bad debt, consumers may still be responsible. For example, collection agents on behalf of the hospital or CHC may continue to seek recovery from the uninsured consumer, sometimes, many, many years after the debt was incurred and written off by the hospital. Medical debt can destroy the consumer’s credit report for up to seven years, thereby affecting the consumer’s ability to obtain loans, utilities, housing, or even employment. Providers and their 6 HLA notes that this section was improperly labeled. The reporting requirements should be cited as 114.6 CMR 13.05(1)(b), not 114.6 CMR 13.05(1)(d). Testimony before the Division of Health Care Finance and Policy regarding proposed regulation 114.6 CMR 13.00 August 22, 2007 Page 9 agents must refrain from unscrupulous and aggressive collection practices against uninsured consumers. Uninsured consumers should be treated with respect, dignity and fairness. Recommendations Medical providers in Massachusetts, including hospitals and CHCs, are covered by the Attorney General’s Debt Collection Regulations, 94 CMR 7.00 et seq. All hospitals and CHCs should incorporate these regulations into their debt collection practices. However, the Division can go further than these regulations and provide for even greater consumer safeguards. We are all familiar with the scandalous practices used by collection agencies and others in connection with mortgage and home improvement debt. There is no question that medical debt is about to rise due to a variety of factors. This is an opportunity for Massachusetts regulators to get ahead of the curve and impose fair debt collection practices for medical debt and to avoid the specter of consumers losing homes, wages, automobiles or simply being forced into bankruptcy because of unanticipated and unplanned for medical debt. Health Law Advocates proposes strengthening consumer protections in the following ways: 1.Expansion of payment plan options a. Lowering this minimum payment to $15 per month. Under the proposed regulations, a consumer is required to pay a minimum $25 monthly payment. For many low income consumers, even a $25 monthly payment is an enormous strain on resources. HLA recommends that Division require that hospitals and community health centers work with consumers to provide comfortable payment plans including the flexibility to adjust the monthly payment as necessary providing a ceiling of $15 per month. b. Payment plans for less than $1000 should be for a minimum of one year, with flexibility for a longer repayment term. Under the proposed regulations, a consumer with less than $1000 in medical debt must be “offered a one year payment plan.” 13.08 (f)(4). This translates to $83.25 per month if a person owes $999. This amount is significantly higher than the $25 per month payment plan that is in the current regulations. 13.08(f)(4). A consumer should be afforded the opportunity to take advantage of the payment plan recommendations given in these regulations - $25 per month, even if that means that the payment period is longer than a year. c. Payment plans for greater than $1000 should be for a minimum of two years according to a schedule. Under the proposed regulations, a consumer with more than $1000 in medical debt is “offered at least a two year interest fee payment plan.” 13.08 (f)(4). This language can be construed to mean that a consumer is obligated to pay off their debt in two years regardless of the amount owed. We recommend that the Division create a payment schedule allowing for greater Testimony before the Division of Health Care Finance and Policy regarding proposed regulation 114.6 CMR 13.00 August 22, 2007 Page 10 flexibility. Hospitals and CHCs should be given explicit leave to extend payment plans and encouraged to create a policy that is more generous. Low-income consumers should be encouraged to work with the hospital to pay off the debt in a reasonable manner. 2. Protect consumers in collection a. Hospitals should be prohibited from selling debt in bulk Hospitals and CHCs should be prohibited from selling old medical debt in bulk to credit collection companies. In these transactions, the title to the debt is sold to the bulk buyer who then proceeds to go after the consumer. Such debt is usually very old, cannot be verified, and in many cases, may be a mistake. Consumers, however, do not understand their rights to contest the validity of such claims and to demand that the debt be verified. Consumer are then hounded by the collector, typically a variety of threats are made to the consumer and the consumer ends up settling with the collector to avoid threatened consequences. b. Clearly warn consumers about hospital collection actions Under 13.08 (d), the Division requires that providers post signs notifying patients of the availability of financial assistance. We recommend that this requirement be extended. Providers should clearly warn consumers that if they do not qualify for any public programs, they will be responsible for costs of the medical services. This includes explaining the provider’s collection and budgeting policies and when a consumer is referred to an outside agency for collection. Consumers should clearly know what to anticipate after they receive services at a hospital or CHC. c. Protect consumer credit ratings The Division should prohibit providers and through contract, their collection agencies, from reporting medical debt to consumer rating agencies. Unplanned for medical debt is not a predictor of creditworthiness. Bad debt reported to a credit rating agency lasts seven years and a consumer should not be penalized for a medical emergency. d. Reduce and limit the opportunities to refer medical debt to collection agencies Providers should make all attempts to work with consumers to settle the debt prior to referring it to collection agencies. A provider is in the best position to provide payment counseling to consumers with medical debt. For example, HLA recently had a client A.A. with medical debt at a local hospital. A.A. was sent to a collection agency that refused to allow her to pay less than $50 per month on her medical debt. A.A. was willing to pay for the services, but could only afford $30 per month. $50 per month is an enormous portion of her salary. However, the hospital was willing to negotiate a lower payment plan and told the collection agency to accept this. e. Prohibit wage garnishment and liens on motor vehicles and personal residences Testimony before the Division of Health Care Finance and Policy regarding proposed regulation 114.6 CMR 13.00 August 22, 2007 Page 11 The proposed regulations disallow a lien against motor vehicles and personal residences without the express approval of the Provider’s Board of Trustees. 13.08(b). We recommend that providers not be allowed to attach motor vehicles or personal residences at all. A consumer should not face the loss of his or her home or means of transportation because they had the misfortune to have a medical emergency. Further, there is no provision regarding the garnishment of wages. We recommend that the Division prohibit such action. Wage garnishment is particularly punitive form of attachment and has not place in the Massachusetts health care system. Conclusion In sum, HLA is very concerned about the economic impact of the proposed regulations on low income Massachusetts consumers. The cumulative impact of new and myriad deductibles and co-payments will produce a significant hardship on those who are in most need of the Free Care Safety Net. Moreover, the appearance of new and sizable deductibles for some insurance products will also add to the cost of necessary medical care for other low and moderate income consumers. Because of this, there is no question that medical debt among consumer patients will spiral. The Division needs to be proactive and set a course for fair dealing and humane debt collection and credit counseling practices among providers. The time for laying the groundwork for a level playing field among all providers is now. Thank you for he opportunity to present the views of Health Law Advocates. Testimony prepared by: Barbara Anthony, Esq. Executive Director Lorianne Sainsbury-Wong, Esq. Senior Staff Attorney Georgia Maheras, Esq. Staff Attorney