Spieth et al. Online Supplement Online Supplement Pressure

Spieth et al. Online Supplement
Online Supplement
Pressure support improves oxygenation and lung protection compared to pressure controlled ventilation and is further improved by random variation of pressure support
Peter M. Spieth, MD 1,2 ; Alysson R. Carvalho, DSc 1,3 ; Andreas Güldner, MD 1 ; Michael
Kasper, PhD 4 ; René Schubert Cand. Med.
1 ; Nadja C. Carvalho, MSc 1 ; Alessandro Beda,
PhD
1
; Constanze Dassow, PhD
5
; Stefan Uhlig, MD, PhD
5
; Thea Koch, MD, PhD
1
,
Paolo Pelosi, MD, PhD 6 ; Marcelo Gama de Abreu, MD, PhD 1
1
Pulmonary Engineering Group, Department of Anesthesiology and Intensive Care Therapy,
University Hospital Carl Gustav Carus, Dresden, Germany;
2
Departments of Anesthesia,
Medicine and Physiology, Interdepartmental Division of Critical Care Medicine, University of Toronto, Keenan Research Center in the Li Ka Shing Knowledge Institute of St. Michael´s
Hospital, Toronto, Canada;
3
Laboratory of Respiration Physiology, Biophysics Institute
Carlos Chagas Filho, Federal University of Rio de Janeiro, Brazil;
4
Institute of Anatomy,
Dresden University of Technology, Germany;
5
Institute of Pharmacology and Toxicology,
University Hospital Aachen, Germany;
6
Department of Environment, Health and Safety,
University of Insubria, Varese, Italy.
Address reprints requests to Dr. M. Gama de Abreu: Pulmonary Engineering Group
Department of Anesthesiology and Intensive Care Therapy, University Hospital Carl Gustav
Carus, Dresden University of Technology, Fetscherstr. 74, 01307 Dresden, Germany.
Address electronic mail to: mgabreu@uniklinikum-dresden.de
or mgabreu@aol.com
.
1
Spieth et al. Online Supplement
Detailed Methods
Detailed experimental protocol
The study protocol was approved by the Institutional Animal Care Committee and the
Government of the State of Saxony, Germany, and performed in accordance to federal laws and the NIH Guidelines for the care and use of laboratory animals.
The study was designed as prospective, three-armed experimental trial. Twenty-four female pigs (27.2–37.0 kg) were premedicated by intramuscular injection of 10 mg/kg ketamine (Ratiopharm, Ulm, Germany) and 1 mg/kg midazolam (Ratiopharm). After orotracheal intubation with a cuffed 8.0 ID endotracheal tube (Malinckrodt, Athlone, Ireland) anesthesia was deepened and maintained via an intravenous line placed in an auricular vein by means of the continuous infusion of midazolam (1-2 mg.kg
-1
.h
-1
) and ketamine (15-20 mg.kg
-
1
.h
-1
). Muscle paralysis was achieved by continuous administration of atracurium
(Ratiopharm) (0.5-2.5 mg.kg
-1
.h
-1
). Animals were ventilated in a volume controlled ventilation (VCV) mode using the mechanical ventilator EVITA XL 4 Lab (Dräger Medical,
Lübeck, Germany) with the following settings: Tidal volume (V
T
) = 10 mL/kg, F
I
O
2
= 1.0, inspiratory/expiratory ratio (I:E) = 1:1, PEEP = 5 cmH
2
O and respiratory rate (RR) to achieve
PaCO
2
in the range 35-45 mmHg. Volume status was maintained by infusion of crystalloid solution (E153, Serumwerk Bernburg) at a rate of 5-10 mL.kg
-1 .h
-1 in order to keep pulmonary capillary wedge pressure (PCWP) approximately constant.
The right anterior surface of the neck was infiltrated with 10 mL xylocaine 2% (Astra
Zeneca, Wedel, Germany), and a paramedian skin incision was performed. After the preparation of the internal carotid artery, the external jugular vein and the trachea, an indwelling catheter was inserted in the carotid artery. A 7.5 Fr. pulmonary artery catheter
(Opticath, Abbott Laboratories, Abbott Park, IL) was advanced through an 8.5 Fr. Sheath placed in the external jugular vein until typical pulmonary arterial pressure waveforms could be observed on the compound monitor system (CMS, Agilent, Böblingen, Germany).
Thereafter, animals were tracheotomized using an 8.0 ID tracheal tube (Malinckrodt).
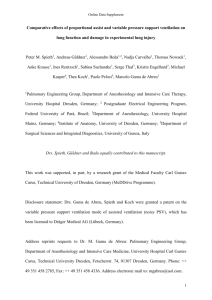
A heated pneumotachograph (Fleisch No. 2, Fleisch Inc., Lausanne, Switzerland) connected to a differential pressure transducer (PXL12X5DN; Sensortechnics, Troy, NY) was placed between the Y-piece of the ventilator and the tracheal tube to determine airway flow
( V
). Airway pressure (Paw) was monitored with by a second pressure transducer
(SCX01DNC; SenSym ICT, Milpitas, CA), which tip was placed at the distal part of the pneumotachograph next to the tracheal tube. An esophageal catheter (Erich Jaeger, Höchberg,
2
Spieth et al. Online Supplement
Germany) was placed and advanced into the mid chest. Correct position was confirmed according to a maneuver described by Baydur et al. (1). The signals of Paw, esophageal pressure (Pes) and V
were digitized at 150 Hz and acquired by the Data Acquisition System
(DAS), which is a main platform written for the LabView environment (National Instruments,
Austin, TX) and also used in our previous studies (2). The volume was calculated as the numerical integration of the V
signal. Figure OS-1 illustrates the experimental setting.
Figure OS-1: Experimental setting.
Urine was collected by means of an 8 Fr. catheter placed in the urinary bladder by means of a mini-laparotomy.
For the calibration of the pneumotachograph, the flow signal was recorded by the
DAS during two minutes and the inspiratory flow was increased by 50 % in the last 30 seconds of acquisition without changing V
T
. Increase of flow was necessary in order to obtain a wider flow range where the calibration procedure should be performed. Signals were processed offline by a subroutine written for MatLab (MathWorks, Natick, MA) to calculate the coefficients of a third order polynomial which best fitted to the flow data. Calibration was accepted if the error of inspiratory and expiratory V
T
in each respiratory cycle was less than
3%.
3
Spieth et al. Online Supplement
Following instrumentation, the lungs were gently recruited by means of a 30/30 maneuver (Paw of 30 cmH
2
O for 30 sec) and the animals were allowed to stabilize for 15 minutes. Baseline 1 measurements were then obtained and injury was performed by means of repetitive saline lung lavages (see Induction of Lung Injury ). After injury, animals were ventilated in the pressure controlled ventilation (PCV) mode with PEEP = 8 cmH
2
O, F
I
O
2
=
0.5, the RR to maintain the arterial pH > 7.30 and driving pressure titrated to a V
T
of approximately 6 mL/kg. After 30 min, baseline 2 measurements were obtained and animals randomly assigned to mechanical ventilation with PCV, pressure support ventilation (PSV) or noisy PSV (see Assisted Mechanical Ventilation for detailed settings). Animal weights and number of lavages to achieve lung injury are shown in Table OS-1.
Table OS-1 – Bodyweight and no. of lavages to achieve lung injury in protocol A
Bodyweight [kg] Lavages [no.]
PCV
31.6 ± 2.3
31.1 ± 3.8
13 ± 8
14 ± 4
PSV noisy PSV
31.1 ± 2.9 14 ± 7
PCV = pressure controlled ventilation, PSV = pressure support ventilation, noisy PSV = noisy pressure support ventilation. Values are given as mean and standard deviation. Statistical analysis was performed using one-way ANOVA and yielded no differences among groups.
Animals were then ventilated for additional 6 h in the respective modes, with hemodynamic and gas exchange measurements, as well as recording of respiratory parameters being performed hourly (see Measurements ). Finally, animals were sacrificed with boluses of thiopental 2g and KCl 1M 50 ml, and lung tissue probes taken from defined regions for processing and analysis (see Histology ). Figure OS-2 illustrates the time course of interventions.
5h 6h
4
Spieth et al. Online Supplement
Figure OS-2 - Time course of interventions. PCV = Pressure Controlled Ventilation. During induction of spontaneous breathing in the conventional and variable pressure support ventilation groups, animals in the PCV groups were ventilated for 30 minutes to compensate for the average time needed to induce and stabilize spontaneous breathing.
Induction of Lung Injury
Following baseline measurements, lung injury was induced by repetitive lung lavages with 0.9% saline solution (37-39°C) as described by Lachmann et al. (3). Injury was considered stable if PaO
2
/F
I
O
2
< 200 mmHg for at least 30 minutes.
Induction of spontaneous breathing
After induction of acute lung injury, mechanical ventilation was switched in all animals to PCV according to the recommendations of the ARDS Network (4). PCV was performed in the airway pressure release ventilation mode (APRV) with a F
I
O
2
of 0.5; PEEP of 8 cmH
2
O; I:E ratio of 1:1 and inspiratory pressures yielded to receive tidal volumes of 6 ml/kg. After baseline 2, animals were randomly assigned to the three treatment groups. If animals were randomized to the PSV or noisy PSV groups, muscle paralysis was stopped, and the infusions of ketamine and midazolam reduced to 10-15 mg.kg
-1 .h
-1 and 0.5-1 mg.kg
-1 .h
-1 , respectively. Respiratory rate was reduced to 15 breaths per minute in order to enforce respiratory drive until negative excursions could be visualized in the esophageal pressure curve. Both, noisy PSV and PSV animals were than ventilated in the PSV mode and a stabilization period of 15 minutes was allowed. Following that, the respective assisted mechanical ventilation mode was initiated. If animals were assigned to PCV, mechanical ventilation and anesthesia regimens were kept unchanged, but a period of 30 min was allowed to approximately match the times of controlled and assisted mechanical ventilation.
Assisted Mechanical Ventilation
The assisted ventilation modes were performed as follows:
PSV : The driving pressure level (P asb
= Ppeak-PEEP) was set to achieve a mean V
T
of approximately 6 mL/kg. The inspiratory V trigger was 2.0 L/min and the expiratory cyclingoff criterion was 25% of peak V .
Noisy PSV : The EVITA XL 4 Lab was controlled by a laptop through a serial port type
RS 232 using the MEDIBUS
®
protocol (Dräger Medical AG) to perform noisy PSV. A set of
600 randomly generated, normally distributed values with mean ± SD = 1 ± 0.3, which corresponded to a coefficient of variation of 30%, was multiplied by P asb
, yielding the pressure support values to be used. We decided to use the degree of variability of 30% in P asb
5
Spieth et al. Online Supplement because it has been shown that this level allows to achieve the best compromise between oxygenation and respiratory mechanics (5). Each pressure support value was sent to the
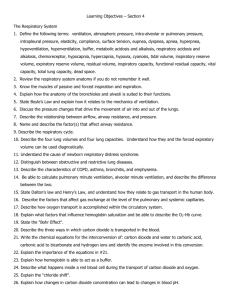
EVITA XL 4 Lab breath-by-breath. After completion of a cycle of 600 breaths, which, depending on the respiratory rate, corresponded to approximately 20 min of assisted ventilation with this mode, the system looped itself. Other settings were identical to those from PSV. Figure OS-3 shows the front panel of the software used to control the mechanical ventilator and perform noisy PSV.
Figure OS-3. Front panel of the controller for noisy pressure support ventilation. P asb
target = pressure support to achieve a mean tidal volume of approximately 6 mL/kg; done (%) = percentage of the sequence of P asb
values (n=600) that has been already sent to the ventilator.
After completion of the sequence, the system looped itself.
Detailed descriptions of measurements
Gas Exchange and Hemodynamics
Arterial and mixed venous blood samples were analyzed for respiratory gases and pH using an ABL 505 blood gas analyzer (Radiometer, Copenhagen, Denmark), and for oxygen saturation and hemoglobin concentration with an OSM 3 Hemoximeter (Radiometer) calibrated for swine blood. Gas tension measurements were performed at 37 o
C and corrected for core body temperature measured by the pulmonary arterial catheter. The oxygen content in
6
Spieth et al. Online Supplement arterial and mixed venous blood, as well as venous admixture, oxygen delivery, oxygen consumption and oxygen extraction rate were calculated using standard formulae. Arterial and pulmonary artery pressure were measured continuously, whereas central venous pressure and
PCWP were measured at each measurement point using the CMS. Systemic and pulmonary vascular resistance were calculated using standard formulae. Cardiac output was measured with the pulmonal artery catheter by means of the conventional thermodilution method. Three measurements with 10 mL 0.9% iced saline solution equally spread over the respiratory cycle were obtained and averaged.
Respiratory Variables
Respiratory variables were calculated offline from continuous recordings (2 min during controlled ventilation and 5 min during spontaneous breathing) of airway pressure
(Paw), esophageal pressure and airway flow ( V ). The product of esophageal pressure over time (PTP) was calculated during inspiration taking the first value at the beginning of the respiratory cycle as offset. PTP values were averaged throughout the whole acquisition periods. Mean and peak airway pressure (Paw,m and Paw,p, respectively) were calculated as the area under the airway pressure curve divided by time, and as the mean peak airway pressure detected in all respiratory cycles during the acquisition time, respectively. Mean transpulmonary pressure (P
L
,m) was calculated as the difference between mean airway pressure and mean esophageal pressure over the whole respiratory cycle during the acquisition time, while peak transpulmonary pressure (P
L
,p) was determined as the mean peak value of the transpulmonary pressure detected in all respiratory cycles during the acquisition time.
Histology
Heart and lungs were extracted en bloc while applying a continuous positive airway pressure (CPAP) that corresponded to the level of PEEP used. Right lung lobes were fixed by perfusion with 4% buffered formaldehyde solution and CPAP maintained during fixation.
Perfusion pressure was held constant and corresponded to the mean pulmonary arterial blood pressure measured at Time 6 . Lung tissue probes of app. 8 cm
3
were taken from gravitational dependent (dorsal – lung segmentum 2 - posterius) and non-dependent zones (ventral - segmentum 3 - anterius) of the right upper lobe. Following perfusion fixation and immersion in 4% buffered formaldehyde solution for seven days, tissue samples were embedded in
7
Spieth et al. Online Supplement paraffin, cutted in slices of 5 µm thickness and stained with hematoxylin-eosin for histological analysis.
Photomicrographs at magnifications of x40, x100 and x400 were obtained from four non-overlapping fields of view per section using a light microscope. Diffuse alveolar damage
(DAD) was quantified by an expert in lung pathology (MK) blinded to the experimental protocol and groups using a weighted scoring system similar to that proposed in our previous study (6). Values from 0 to 5 were used to represent the severity of alveolar edema, interstitial edema, hemorrhage, inflammatory infiltration, epithelial destruction, microatelectasis and overdistension, with 0 standing for no effect and 5 for maximum severity. Additionally, the extent of each score characteristic per field of view was determined with values of 0 to 5, with
0 standing for no appearance and 5 for complete involvement. Scores were calculated as the product of severity and extent of each feature, being situated in the range 0-175.
Pulmonary Mechanical Stress Markers and Inflammatory Response
Lung tissue probes were taken from dependent and non-dependent zones of the right lower lobe, snap frozen and kept at -80°C until processing as described in our previous work (7).
Briefly, tissue probes for quantitative real-time (qRT)-PCR were ground in a mortar under liquid nitrogen to a homogenous powder. Total RNA was isolated from the equivalent of mg homogenous lung tissue with NucloeSpin RNA II Kit according to the manufacturer's instructions
(Machery Nagel, Düren, Germany). A total of 8 µl RNA was mixed with 2µl Oligo-(dt)-primer
(Invitrogen), centrifuged and subsequently incubated at 65°C for 10 min to linearize RNA. Then,
2 µl of this RNA-primer-mix were added to 1 µl Superscript II Reverse Transcriptase (200U/µl)
(Invitrogen, Karlsruhe, Germany), 4 µl 5x strand buffer (250 mM Tris-HCL, ph 8.3; 375 mM
KCL,15mM MgCl
2
) (Invitrogen), 2 µl DTT (0,1M) (Invitrogen), 2 µl dNTP-Mix (10mM)
(peqLAB, Erlangen, Germany), 1 µl RNAseOut (40 U/µl) (Invitrogen) and incubated for 90 min at 37 °C. Following that, the mixture was diluted with 30 µl H
2
O (Aqua B.braun; Braun,
Melsungen, Germany). The qRT-PCR product accumulation was monitored with a
LightCycler480 (Roche-Diagnostics) using 1 µl of total cDNA, 200nM forward , 200 nM reverse primer and SYBR-Green I Mastermix (Roche-Diagnostics) according to manufacturer's instructions. Primers shown in Table OS-2 were used.
8
Spieth et al. Online Supplement
Table OS-2: Porcine primers
Gene Forward Primer Reverse Primer
ß-2Mg 5´-AGGTTCAGGTTTACTCACGC-3´ 5´-GCGTTCATCTTCTCCCCGT-3´
AREG 5´-ATTATGCTGCTGGACTGGAC-3´ 5´-TCGCTACCAGAAGGCATTT-3´
TNC
IL-6
IL-8
5´-ATCAGCCAGCGGGGACAAA-3´ 5´-GGATGTTGATGCGATGTGTG-3´
5´-AAGATGCCAAAGGTGATGCC-3´ 5´- TCTCACACATCTCCTCTCTC-3
5´-CCTTCTTGGCAGTTTTCCT-3´ 5´-GTGGAAAGGTGTGGAATGC 3 ´
TGF-ß 5´-GGACTACTACGCCAAGGA-3´ 5´-GCCCGAGAGAGCAATACA-3´
ß-2Mg = ß-2 Microglobulin; AREG = Amphiregulin; TNC = Tenascin c; IL-6 = Interleukin 6; IL-
8 = Interleukin 8; TGF-ß = Transforming growth factor ß.
Data obtained from a given lung area were normalized to the house keeping gene ß2 microglobulin and to the PCV group. Values are expressed as fold induction. Programs of amplification used in qRT-PCR are depicted in Table OS-3. Preincubation was performed at 95°C for 5 min. After amplification, melting curves were generated at 95°C for 5 min and acquisition points were continuously obtained at a rate of 5/s between temperatures of 65 to 97 °C.
Table OS-3: Amplification program
Gene T preinc.
(°C) t preinc.
(s) T ann.
(°C) t ann.
(s) T elon.
(°C) t elon.
(s) T aqu.
(°C) t aqu.
(s) Cycles T mc
(°C)
ß-2Mg 95 10 58 10 72 15 74 1 35 82
AREG 95 10 56 10 72 15 74 1 35 86
TNC
IL-6
95
95
10
10
58
57
10
7
72
72
15
10
80
74
1
1
45
45
88
81
IL-8 95 10 55 10 72 10 74 1 45 83
TGF-ß 95 10 56 7 72 15 74 1 45 85
ß-2Mg = ß-2 Microglobulin; AREG = Amphiregulin; TNC = Tenascin-c; IL-6 = Interleukin 6; IL-
8 = Interleukin 8; TGF-ß = Transforming growth factor ß. T preinc
. = preincubation temperature; t preinc.
= preeincubation time; T ann.
= annaling temperature; t ann
. = annaling time; T elong.
= elongation temperature; t elong.
= elongation time; T aqu.
= acquisition temperature; t aqu.
= acquisition time; T mc
= melting curve temperature.
To quantify cytokine levels in lung tissue, the frozen tissue samples were grounded with a pestle in mortar and re-suspended in cold PBS (pH 7.5) containing complete mini TM protease inhibitor mix (Roche Diagnostics, Mannheim, Germany). The suspension was homogenized, centrifuged (16,000 g) and the supernatant analyzed for IL-6 and IL-8 using commercially available ELISA kits (R&D Systems) according to manufacturer’s instructions.
Broncho-alveolar lavage sampling and processing
A lung broncho-alveolar lavage (BAL) with 50 ml 0.9% saline solution was performed in the extracted right middle lobe. Aliquots of the supernatant were obtained and kept frozen
9
Spieth et al. Online Supplement at -80°C until processing. Levels of IL-6 and IL-8 in BAL fluid were measured by commercially available ELISA kits (R&D Systems, Wiesbaden, Germany) according to manufacturer’s instructions.
Online Supplement References
1. Baydur A, Behrakis PK, Zin WA, et al. A simple method for assessing the validity of the esophageal balloon technique. Am Rev Respir Dis 1982;126(5):788-791.
2. Gama de Abreu M, Quelhas AD, Spieth P, et al. Comparative Effects of Vaporized
Perfluorohexane and Partial Liquid Ventilation in Oleic Acid- induced Lung Injury.
Anesthesiology 2006;104(2):278-289.
3. Lachmann B, Robertson B, Vogel J. In vivo lung lavage as an experimental model of the respiratory distress syndrome. Acta AnaesthesiolScand 1980;24(3):231-236.
4. The Acute Respiratory Distress Syndrome N. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med 2000;342(18):1301-1308.
5. Spieth PM, Carvalho AR, Guldner A, et al. Effects of different levels of pressure support variability in experimental lung injury. Anesthesiology 2009;110(2):342-350.
6. Spieth PM, Knels L, Kasper M, et al. Effects of vaporized perfluorohexane and partial liquid ventilation on regional distribution of alveolar damage in experimental lung injury. Intensive Care Med 2007;33(2):308-314.
7. Spieth PM, Carvalho AR, Pelosi P, et al. Variable tidal volumes improve lung protective ventilation strategies in experimental lung injury. Am J Respir Crit Care
Med 2009;179(8):684-693.
10