Arthritis_Lab_joint count_STL
advertisement

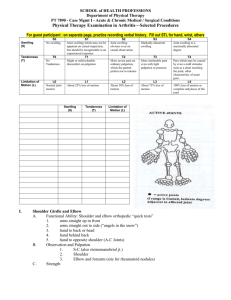
SCHOOL of HEALTH PROFESSIONS Department of Physical Therapy PT 7890 - Case Mgmt I - Acute & Chronic Medical / Surgical Conditions Physical Therapy Examination in Arthritis—Selected Procedures I. II. Shoulder Girdle and Elbow A. Functional Ability: Shoulder and elbow orthopedic “quick tests” 1. arms straight up in front 2. arms straight out to side (“angels in the snow”) 3. hand to back or head 4. hand behind back 5. hand to opposite shoulder (A-C Joints) B. Observation and Palpation 1. S-C (also sternomanubrial jt.) 2. Shoulder 3. Elbow and forearm (site for rheumatoid nodules) C. Strength Wrist and Hand A. Functional Ability 1. buttoning and unbuttoning 2. OT or CHT have tools for thorough exam B. Observation and Palpation (the hand often is key to preliminary medical diagnosis: skin, fingernails, deformity) 1. Distal radioulnar (piano key deformity) 2. Wrist (synovitis, subluxation, rheumatoid nodules, Tinel test) 3. MCP (synovitis, subluxation and ulnar drift) 4. PIP (synovitis vs. Bouchard’s nodes) 5. DIP (synovitis vs. Heberden’s nodes) C. Special Tests 1. Finkelstein’s 2. Bunnell-Littler (PIP intrinsic mm. vs. capsular tightness) 3. Retinacular (DIP retinacular ligs. vs. capsular tightness) D. Strength 1. Grip: sphygmomanometer inflated to 30 mm Hg 2. Standard dynamometer -1- III. 3. Pinch dynamometer Head A. TMJ 1. should admit minimum of two vertically held fingers 2. micrognatha (JRA) B. Temporal artery dilation, head pain, and polymyalgia rheumatica C. Laryngeal arthritis III. Spine and Ribs (Thorax) A. Cervical spine 1. Risky in possible RA: Active movements only 2. “Clunk” with forward flexion – atlanto-axial instability B. Chest expansion IV. Hip and Knee A. Functional ability: rise from chair without arms, squat B. Observation and palpation (knee): 1. alignment 2. atrophy accentuated by effusion 3. palpation of suprapatellar synovial pouch 4. knee joint effusion – bulge sign and Ballottement 5. Baker’s cyst C. Joint stability (medial-lateral stress in full knee extension) D. Special tests for screening 1. Thomas test 2. Patrick test (fabere) E. Elements of usual orthopedic examination as indicated V. Ankle and Foot A. Functional ability: tiptoes, heels, squat B. Observation: similarities to the hand 1. skin (rheumatoid vasculitis similar to arterial insufficiency) 2. deformities: subtalar joint collapse hallux valgus cock-up or overlapping toes C. Palpation 1. ankle joint effusion 2. tarsal joints 3. MTP joints 4. PIP and DIP joints Swelling (S) S0 No swelling Tenderness (T) T0 No Tenderness Limitation of Motion (L) L0 Normal joint motion S1 Joint swelling which may not be apparent on casual inspection, but should be recognizable to an experienced examiner T1 Slight or mild tolerable discomfort on palpation S2 Joint swelling obvious even on casual observation S3 Markedly abnormal swelling S4 Joint swelling to a maximally abnormal degree T2 More severe pain on ordinary palpation, which the patient prefers not to tolerate T3 More intolerable pain even with light palpation or pressure. L1 About 25% loss of motion L2 About 50% loss of motion L3 About 75% loss of motion T4 Pain which may be caused by even a mild stimulus such as a sheet touching the joint; often characteristic of acute gout. L4 100% loss of motion or complete ankyloses of the joint -2-