Manual For Interpreting in Medical Setting
advertisement

I discovered this “Wikispace” for us to reference online! It has some good resources and articles that we can use during the course: Go to: www.interpreter.wikispaces.com Assignment: ……………………………………………………………… ……………………………………………………………… INTRODUCTION Becoming and Being an Interpreter One of the most common misconceptions about interpreting is that anyone who speaks two languages with relative fluency is automatically equipped with the skills they need to convert rapidly a message with both accuracy and appropriateness in such a way that the response of the listener is identical to what it would have been were there no language interference/barrier. This misconception, coupled with ever-increasing demand for interpretation in the medical setting has unfortunately led to a great variance in the quality and degree of professionalism encountered in clinical settings where nonEnglish speaking patients meet with healthcare professionals in the presence of an interpreter. There are several reasons for the often undetected or overlooked weaknesses of an untrained native speaker when s/he is thrust into a situation in which interpretation is needed. The primary cause for concern is unfamiliarity with the specialized vocabulary encountered in the field of medicine. Often the speaker uses a term that presents particular difficulty because of the lack of a term that corresponds exactly with that term in the other language, or simply the understandable lack of knowledge of that term. The untrained interpreter then senses the inadequacy of her/his vocabulary or background in healthcare and feels pressured to invent terminology that may or may not accurately express the exact impact/meaning of the words spoken by either party. Simply stated, the interpreters own experience and education may be severely or partially lacking if they were speakers of a language that was primarily spoken at home but were not educated in schools and/or countries where that language is predominant. These so-called “heritage speakers” are able to communicate easily in the language during basic social encounters (e.g. “Go there” “Sign here” “Do this” “Bring this”), but they are not generally prepared for the more complex linguistic skills required to “manage the flow of communication” in the more formal speech of medical care (e.g. “We need to assess your son’s prothrombin time in order to determine if he needs further evaluations and perhaps additional anticoagulants”). ©2009 Atlanta Academy of Languages, Atlanta GA 2 A second reason for concern is the lack of familiarity with Standards of Practice which serve to guide the interpreter through situations that s/he may experience in the encounter. Indeed, Standards of Practice for Medical Interpreters are now currently available in the field. These standards function as a practical guide to those with little previous experience in faceto-face interpreting and as a reminder of the ethical behaviors required of all professional interpreters who have completed a formal course of study in the field of interpretation. Additionally, in order to be most effective, interpreters must have a least a rudimentary knowledge of linguistics, taking into consideration register, context, content, connotative versus denotative meaning, implicit and explicit message, common idioms, etc. This understanding of the complexity of human language (i.e., that often the words being spoken have much deeper cultural, figurative, derogative, or other emotional connotations) draws the attention of the experienced interpreter and animates her/him to find “just the right” words to use in each and every situation. And this must be accomplished almost instantaneously! In summary, the tasks of the medical interpreter are demanding and amazingly complex! A great deal of information is transmitted in a small amount of time, without sufficient corrective reflection available. It is indeed a professional challenge! – e s king ©2009 Atlanta Academy of Languages, Atlanta GA 3 Working in groups, please discuss the following questions, being sure to assign someone to take notes in order to report back to the class about your group’s answers and observations. Be candid and frank! Discussion Questions: (1) What are other misconceptions? Do you agree with them? How did/do they develop? (2) Can responses really be expected to be identical? (3) What are the causes of variances among us? Is this necessarily a problem? What are the strengths and weaknesses we perceive? (4) What is the concept of “heritage speaker” all about? How do you feel about being labeled in that way? Can one overcome it? Does one need to do so? (5) What Standards would you create? How will they be organized? What are the most important to least important aspects of Standards of any kind? Are they intended to be rules or guidelines, or laws? (6) How does familiarity with linguistics help? Is it necessary? Define words you don’t know. Give your own examples. Tell us how people use words. (7) What are the implications of oral (interpretation) versus written (translation) projects? (8) How is our job complex/complicated? What areas are beyond our control? How do we develop professionally? ©2009 Atlanta Academy of Languages, Atlanta GA 4 Slide 1 Medical Interpreting It’s an meaningful art! ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 5 Slide 2 Beginning the Conversation! Para empezar… ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 6 Slide 3 What does it mean to be a PROFESSIONAL ? • • • • • • • • • Skills / Training ? Experience(s) ? Credentials ? Work Ethic ? “Craftmanship” ? Uniqueness ? Dependability / Consistency ? Self-realization / Self-proclaimed ? Recognition ? ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 7 Slide 4 WELL THEN, … What is “amateur” ? ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 8 Slide 5 Complete this sentence: An interpreter … ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 9 Slide 6 What does an interpreter really do? • Are you a noun or a verb ? – Is understanding the difference important to you ? ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 10 Slide 7 What are some of the things that an interpreter should BE ? What are some of the things that an interpreter should DO ? ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 11 Slide 8 So, what are some of the things that an interpreter should NOT BE ? And, what are some of the things that an interpreter should NOT DO ? ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 12 Slide 9 In small groups: Create three (3) RULES Create three (3) GUIDELINES Create three (3) SUGGESTIONS ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 13 Slide 10 What skill areas will we need to examine in this course? • Cultural Issues and Sensitivity when working with Hispanic/Latino patients • Linguistic Expertise (fluidity/grammar/syntax) • Medical Terminology (fluency/vocabulary) • Anatomy • Standards of Practice (MMIA) • Resources for Continuing Education and Professional Development ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 14 Slide 11 What are YOUR EXPECTATIONS ? ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 15 Slide 12 WHAT CHALLENGES WILL YOU FACE? ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 16 Slide 13 The Challenge • You need to be able to provide a complete and convincing argument for the use of professional interpreters in the medical field as opposed to non-trained speakers of SPANISH! – – – – HERITAGE BILINGUAL (ACTFL – SUPERIOR) NATIVE - N/L ED (1-9+) NATIVE - H ED (9-12+) ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 17 Slide 14 Group Work • Work within you group to answer the following question: • (1) What defines a professional interpreter? • (2) What reasons would you give to someone to try to convince them to use a professional interpreter in the medical field as opposed to a non-trained speaker of a language? ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 18 Slide 15 Skills List Assumptions • Cultural Expertise / Knowledge / Awareness / Sensitivity • Linguistic Expertise in two languages such that a message delivered in one language ilicits exactly the response it would have ilicited had it been delivered in the other language. • Medical Terminology – being increasingly familiar with medical terms, conditions, and treatments will facilitate effective medical interpreting • Standards of Practice – knowledge, familiarity, and compliance with Standards are a sign of a true professional in any field. ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 19 Slide 16 What is involved in interpreting for the patient and the healthcare professional? • A keen and real recognition that yours is also a profession, not just a skill! • A calm attitude that responds to stress in helpful ways, using practiced, learned skills. • A good sense of each situation…i.e., “sizing up the situation” ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 20 Slide 17 Skills-Based • Becoming an Effective Interpreter in the Medical Field is a learned, lifelong, skillsbased process. ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 21 Slide 18 Skill Areas Required to be a Professional Medical Interpreter: • Linguistic Expertise – Spanish and English and “Spanglish” – Grammar and Common Usage – Colloquialisms/Slang/Some Jargon – Ever-Increasing Knowledge of Regional Differences – Circumlocution – Awareness of Contextual Clues – Awareness of Some Limitations ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 22 Slide 19 Colloquialisms • • • • A colloquialism is an expression not used in formal speech or writing. Colloquialisms can include words (such as "gonna" or “fixin’ to"), phrases (such as "ain't nothin'" and "dead as a doornail"), or sometimes even an entire aphorism ("There's more than one way to skin a cat"). Dictionaries often display colloquial words and phrases with the abbreviation colloq. Colloquialisms are often used primarily within a limited geographical area. In some areas, overuse of colloquialisms by native speakers is regarded as a sign of substandard ability with the language. However, in the mouth of a non-native speaker, they are sometimes taken as signaling unusual facility with the language as they may be more difficult for non-native speakers to understand. A colloquialism can sometimes make its way into otherwise formal speech, as a sign that the speaker is comfortable with his or her audience, in contrast to slang, which if used in formal speech is more likely done so consciously for humorous effect. Words that have a formal meaning may also have a colloquial meaning that, while technically incorrect, is recognizable due to common usage. ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 23 Slide 20 Slang • • • • • • Slang is the non-standard or non-dialectal use of words in a language of a particular social group, and sometimes the creation of new words or importation of words from another language. It is a type of neologism. Slang can be described as way of deviating from standard language use, and is very popular with teenagers. Slang functions in two ways; the creation of new language and new usage by a process of creative informal use and adaptation, and the creation of a secret language understood only by those within a group intended to understand it. As such, slang is a type of sociolect aimed at excluding certain people from the conversation. Slang initially functions as encryption, so that the non-initiate cannot understand the conversation, or as a further way to communicate with those who understand it. Slang functions as a way to recognize members of the same group, and to differentiate that group from the society at large. Slang terms are often particular to a certain subculture, such as musicians, skateboarders, and drug users. Slang generally implies playful, informal speech. Slang is distinguished from jargon, the technical vocabulary of a particular profession, as jargon is (in theory) not used to exclude non-group members from the conversation, but rather deals with technical peculiarities of a given field which require a specialized vocabulary. Four now widely accepted characteristics of slang were identified in the paper "Is Slang a Word for Linguists," 53 American Speech 5, 14-15 (1978), by Bethany K. Dumas and Jonathan Lighter. Slang usually shares at least two of the following traits. First, it is markedly lower in dignity than Standard English. Second, it tends to first appear in the language of groups with low status, meaning they may have little power or little responsibility. Third, it is often taboo and would be unlikely to be used by people of high status. Fourth, it tends to displace a conventional term, either as a shorthand or as a defense against perceptions associated with the conventional term. ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 24 Slide 21 • • • Jargon Jargon is terminology, much like slang, that relates to a specific activity, profession, or group. It develops as a kind of shorthand, to express ideas that are frequently discussed between members of a group, and can also have the effect of distinguishing those belonging to a group from those who are not. Newcomers or those unfamiliar with a subject can often be characterized by their incorrect use of jargon, which can lead to amusing malapropisms. The use of jargon by outsiders is considered by insiders to be socially inappropriate, since it constitutes a claim to be a member of the insider group. Jargon can be distinguished from terminology in that it is informal and essentially part of the oral culture of a profession, with only limited expression in the profession's publications. Many jargon terms have non-jargon equivalents which would be used in print or when addressing non-specialists; other jargon terms, particularly those which are used to characterize or even ridicule non-specialists, have no such equivalents. The everyday use of the word jargon to describe any technical terminology incomprehensible to the lay person ignores this distinction between jargon and terminology. Oftentimes, people will use jargon derisively, meant to indicate disapproval with the use of words whose meaning is esoteric, and thus exclusionary of people who do not understand their meaning and background, for example in The Jargon of Authenticity by Theodore Wiesengrund Adorno. To describe an idea as jargon accomplishes in Bourdieu's terms several tasks. It maintains the speaker's "distinction" and social role as critic and judge, while at time excusing the speaker from listening or reading with attention, and it also expresses a safe, egalitarian attitude. ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 25 Slide 22 Idioms • • • An idiom is an expression (i.e. term or phrase) whose meaning cannot be deduced from the literal definitions and the arrangement of its parts, but refers instead to a figurative meaning that is known only through conventional use. In linguistics, idioms are figures of speech that contradict the principle of compositionality. Take the English expression to kick the bucket. A listener knowing only the meaning of kick and bucket would be unable to deduce the expression's actual meaning, to die. Although kick the bucket can refer literally to the act of striking a bucket with a foot, native speakers rarely use it that way. Idioms hence tend to confuse those not already familiar with them; students of a new language must learn its idiomatic expressions the way they learn its other vocabulary. In fact many natural language words have idiomatic origins, but have been sufficiently assimilated so that their figurative senses have been lost. ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 26 Slide 23 Skill Areas Required to be a Professional Medical Interpreter: • Cultural Competency • many cultures within a broader linguistic culture • diverse “mini” cultures within one culture • attitudes toward healthcare issues may vary from attitudes the interpreter is exposed to in other areas of life • etiological and epidemiological facts ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 27 Slide 24 Skill Areas Required to be a Professional Medical Interpreter: • Medical Terminology • Root Words; Prefixes; Suffixes • • • • • • • • The Body and The Diseases The Systems and Their Function The Symptoms and The Assessments The Typical Actions in Examination Process The Procedures The Treatments The Follow-up The Medications ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 28 Slide 25 Skill Areas Required to Be a Professional Medical Interpreter: • Awareness and Knowledge of Standards of Practice for Medical Interpreting • Demonstration of Compliance with the Standards of Practice for Medical Interpreting ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 29 Slide 26 You’re a Professional! • It is with this knowledge base that you will not only improve your personal career options, but also that of all medical interpreters! • “Make" them want us! ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 30 Slide 1 Transcultural Competency in the Treatment of Hispanic / Latino Patients E. Scott King, MA Spanish for Professionals Division of Atlanta Academy of Language Learning Inc. ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 31 Slide 2 “Hispanic” versus “Latino” • Hispanic is defined as Spanish-speaking – Definitely NOT a racial term! • Latino is defined as being related to or from the Spanish-speaking countries of North America, or from Central, Latin, or South America ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 32 Slide 3 “Transcultural” • The relatively new word “transcultural” implies reaching across cultural boundaries with one “foot” planted in the familiar ground of one’s own life experiences…reaching across the sometimes explicit but often implicit space between ourselves and another human being. It validates both a deeper awareness of and a growing appreciation for one’s own culture, as well as a willingness to learn about another’s culture in the process of seeking true communication! - E. Scott King ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 33 Slide 4 What is Culture? • The word culture implies an integrated pattern of human thoughts, communications, actions, customs, beliefs, values and institutions of a racial, ethnic, religious or socioeconomic group. • It’s tempting to think of culture only in terms of what experts refer to as “Culture with a Capital C” – in other words, art, music, & literature! • But culture with a “little c” includes the daily routines and expectations in a society, and might include how to order food from a drivethrough, use an ATM machine, order a meal, appear to an interview, drive a car, or act in a hospital! These things are often the more implicit behaviors of a group of individuals, and therefore are frequently viewed as the most mysterious barriers between us! ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 34 Slide 5 What is “transcultural competence” in dealing with Hispanic/Latino healthcare issues? • Transcultural competency implies effective communication ! • Not just Spanish words ! • Cultural knowledge/awareness is crucial ! • These knowledge-based skills can be learned ! ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 35 Slide 6 Barriers to Transcultural Competency • Barriers may be expected to exist, therefore, in all three areas of communication: • Language Barriers – “A different language is a different view of the world!” –Federico Fellini • Shades of meaning in words even when we have learned the language of the patient • Body Posture and Gestures may mean one thing in one culture and something entirely different in another (or nothing at all!) ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 36 Slide 7 Suggestions • Ask about words (whether in English or Spanish) whose meaning or implications are not quite clear to you… • What exactly do you mean by “--------” ? is a great question to ask the patient • Observe consciously and carefully the body language (eye contact and gestures, as well as personal space allowed) that the patient exhibits…these are clues to their thoughts! • Distance may indicate either distrust or respect in other cultures! ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 37 Slide 8 Cultural Sensitivity Cultural sensitivity is knowing that cultural differences as well as similarities exist without automatically assigning values to those differences, i.e., better /worse, right /wrong. (National Maternal & Child Health Center on Cultural Competency, 1997) ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 38 Slide 9 Hot versus Cold Climate Cultures • Sarah Lanier’s theory of Hot and Cold climate cultures (Lanier, 2002) offers easy to understand frames of reference when working or living with others. The generalizations found in this explanation of cultural differences can serve as a solid basis for “first-impression” insights into the behavior of others. ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 39 Slide 10 My Own Concept of Hot/Cold Climate Cultures C OLD C LIMATE C ULTURES HOT C LIMATE C ULTURES Lanier points out that there are exceptions found to solely a geographical interpretation of the Hot/Cold-Climate Cultures. ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 40 Slide 11 Hot Climate Cultures • People in and from hot climate cultures tend to be: • relationship oriented rather than task oriented • indirect communicators rather than direct communicators • group-identity seekers rather than individual-identity seekers • inclusive of many others rather than highly regarding of individual privacy • high-context members of their society (everything matters) rather than low-context members of their society (not much matters; anything goes-within reason) • not highly oriented to the clock rather than time oriented. ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 41 Slide 12 Cold Climate Cultures • People in and from cold climate cultures tend to be: • task oriented rather than relationship oriented • direct communicators rather than indirect communicators • individual-identity seekers rather than group-identity seekers • have high regard of individual privacy over the inclusive of many others in affairs • low-context members of their society (not much matters; anything goes-within reason) rather than low-context members of their society (everything matters) • time oriented to the clock rather than flexible in their concept of time ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 42 Slide 13 Our Patients • Patients from Cold-Climate Cultures seem to appreciate logic, efficiency, and informationloaded atmospheres. Respect for others is best expressed by respect for another’s time and privacy. • Patients from Hot-Climate Cultures seem to thrive on being relationship based where a “feel good” atmosphere is created. People take priority over efficiency and time, and “small talk” is an well-developed and highly valued art! ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 43 Slide 14 Our Patients • Patients from Cold-Climate Cultures seem to use short and direct questions and answers, and a “yes” is usually a “yes”, and a “no” a “no”. If they say nicely what they really think, you won’t be expected to take it too personally! • Patients from Hot-Climate Cultures seem to value being friendly above being honest, and even avoid taking any chance of offending or embarrassing others. Their “yes” or “no” may simply be an indication that they will consider further the situation, not that they will comply, act upon, or are answering honestly your request or question. ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 44 Slide 15 Our Patients • Patients from Cold-Climate Cultures seem to cherish their own right to an opinion and to independence, and take initiative within a group, making decisions on their own. Their “own space” is important. • Patients from Hot-Climate Cultures seem to seek their identity within a group, avoid appearing “pushy” by taking too much initiative, seek the support and protection of many others, and expect clear direction from the provider. One’s possessions should be shared, and one rarely desires solitude. ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 45 Slide 16 Our Patients • Patients from Cold-Climate Cultures seem to appreciate planning and advanced notice. Spontaneity must be brought under control. Hospitality is a special event and a serious matter. • Patients from Hot-Climate Cultures seem to believe that hospitality is a spontaneous gift, and is the context for all relationships. Gifts are usually expected. Food and drink play a major role in kindness and appreciation. ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 46 Slide 17 • In a Cold-Climate culture, who you know matters, but not nearly so much as what you know. Cold-Climate cultures usually do not expect Hot-Climate Cultures to know their rules of behavior, nor are they that interested in knowing the rules of the other culture. • In a Hot-Climate culture, honor and respect often outweigh freedom and casualness. Manners are of the utmost importance for success! ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 47 Slide 18 Identity / Nationalism • Of extreme importance and significance to almost every Spanish-speaker is the country from which they or their family have immigrated ! • Both country and region are important because the culture and expectations of each may differ significantly from one area to another. » Example : MEXICO has three (3) distinct regions and 31 states! Northern, Central (City), and Southern states vary in history, ethnic background, and culture. • There are many cultures represented in the broad terms “Hispanic” and “Latino” !!! ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 48 Slide 19 How well do we really communicate with each other? • Communication is more than simply words. In fact, words do “often get in the way”! • Communication is often non-verbal! • What are some examples of Latin nonverbal communication that might convey unspoken messages of discomfort or fear? ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 49 Slide 20 Gestures and Body Language • Hand signs – these differ so be careful » “OK” gesture » “Come here” gesture • Personal Space – extremely different! » Latin versus Anglo “personal space” • Other Body Language Signals » The so called “Latin nod” – don’t make presumptions! » Eye contact ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 50 Slide 21 Potential Areas of Misunderstanding • • • • • • • • Epidemiological and Etiological Understanding Directive versus Options-oriented healthcare Family Involvement Perception of symptoms and expression of pain Standards of modesty and Personal Space Linguistic challenges and barriers Diets and food issues Folkloric Medicines ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 51 Slide 22 Did you know? Mexican Americans have a higher incidence of diabetes, heart disease, hypertension, pernicious anemia and tuberculosis exposure. ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 52 Slide 23 Did you also know? • ‘Small talk’ before serious discussion may ease tension and increase comfort level with Spanish-speakers. • Courtesy is valued; arguments are considered rude. One does not openly question authority without fear of offending. Question: What implications are there for the physician? ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 53 Slide 24 What do you know about Latins/Hispanics and… • • • • • Directive care versus “options”? Attitudes towards Physicians? Attitudes toward diseases? Gender expectations? The implications of the gender of the interpreters? • Their formal educational level ? ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 54 Slide 25 …about Latinos/Hispanics and… • Their true knowledge of English? • The cultural “baggage” they bring with them that might affect healthcare? • The folklore medicine and home remedies that they have seen used or have experienced themselves? • Their general tastes in clothing, styles, foods, and cosmetics/appearance? • Their “polychronic” versus our “monochronic” view of events and time? ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 55 Slide 26 • As a “polychronic” culture, many Latins expect for many people to be involved in an activity all at one time! They won’t mind interrupting simply to announce their presence. Lines are not generally automatically formed (of course there are many exceptions among ‘high society”). ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 56 Slide 27 And What’s More… • Many Spanish-speakers consider it either rude or humiliating to indicate that they do not completely understand you (in both Spanish and in English). Be sure to always clarify and get a positive response from a Spanish-speaker before you assume that they understood you completely! • This will accomplish the very effective but blunt, non-Latino style discourse among Americans expressed aptly by the word “Huh???”! ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 57 Slide 28 Illness and Disease • Good health may be seen as good luck, a reward from God or a universal equilibrium with balanced forces of hot/cold, wet/dry, etc. • When family member is ill, may practice religious rituals, i.e., lighting candles, praying. • When in pain, many are stoic and exhibit great self-control; perceived as having high pain tolerance. • Prefer company of others, especially family, when in pain. • Folk medicine is practiced by some. “Curanderos”, and home remedies are frequently used (ear-wicking, copper bracelets, garlic, teas, rituals to cure “el susto” (post-traumatic stress), etc. • Illnesses /Death / grief are considered “God’s will;” saying the rosary with family is common for several evenings after a death. ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 58 Slide 29 It’s all in learning about the details! • Touch is very important, especially in caring for children. • Have narrowed ‘personal space’ & may see one’s distancing as aloof and unfriendly. • Smiling & handshakes are important, trustestablishing interactions. • Modesty is valued. ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 59 Slide 30 • Many Latins would perceive a nurse or doctor giving them treatment options as a sign that they are not well-trained! They prefer directive healthcare! • Many Latins want others in the examining area, fearing being alone. • Many Latins won’t give you clear signs that they do not completely understand you. • Many Latins respond well to just a small amount of Spanish to relax them! ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 60 Slide 31 Family life • Mexican and Latin American culture is mainly a nuclear family culture. 73% of families are married-couple families. • Matriarchal /matriafocal society with oldest female responsible for family cohesiveness, most health matters and family names. • Father, however, is often the decision-maker. ut Mother most approve or there will be little enforcement of decisions. ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 61 Slide 32 ….more about the family • The elderly are highly respected and live with their children. • Extended family also plays visible role in health and illness situations. • People of this culture may be hesitant to seek help / support outside of the family. ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 62 Slide 33 Other issues… • Working with Interpreters • • • • • • Family member versus professional Seasoned professional versus “convenience” Issues of accuracy Issues of sharing and discussing Unauthorized recommendations/guidance Standards do exist!!! » Refer to the Massachusetts Medical Interpreter Association (MMIA) ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 63 Slide 34 Now let’s practice what we’ve learned or need to learn! Situation 1: You’re interviewing a patient and reminding them of how important it is to “stick with” the diet you prescribed for them during their last visit. The patient will most likely think that……………………… ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 64 Slide 35 More fun! • Situation 2 You struggle to communicate that a patient needs to be sure to advise you immediately should their symptoms return or worsen. The patient smiles and nods their head indicating…………………………………… …….. ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 65 Slide 36 Even more! • Situation 3 Your interpreter, Pablo, is assisting you with Mrs. Rodríguez, who is in her third trimester of pregnancy and experiencing some bleeding and pain. Pablo will ………………………………………… ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 66 Slide 37 More situations… • Situation 4: You notice that a child patient has what appear to be ashes in his/her ears. Most likely………………………….. ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 67 Slide 38 Another… • Situation 5: You are visiting a Hispanic/Latino patient for Home Healthcare. S/he offers you something to drink. You do not want anything because you just had a large drink before arriving. You should explain that…………………………… ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 68 Slide 39 More situations • Your patient walks into the lobby and/or waiting/reception area. You are busy taking information or explaining how to complete forms to another patient. The Hispanic/Latino will/may…………………………………………… • Your nurses notice that all the Latino children seem to be running “wild” in the waiting room/reception area. The best way to correct this is by…………………………………………………….. ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 69 Slide 40 • Linguistic Expertise – Spanish and English and “Spanglish” – Grammar and Common Usage – Colloquialisms/Slang/Some Jargon • “Did you throw your back out?” – Ever-Increasing Knowledge of Regional Differences – Circumlocution – Awareness of Contextual Clues – Awareness of Some Limitations ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ____________________________________________________________________ ©2009 Atlanta Academy of Languages, Atlanta GA 70 Originally published in the Western Journal of Medicine. Reprinted by permission. West J Med 1992;157:255-259 Copyright © wjm. Translation Is Not Enough Interpreting in a Medical Setting Linda Haffner, Community and Patient Relations, Stanford University Medical Center, Stanford, California Correspondence to: Ms Haffner, 343 Lunada Ct, Los Altos, CA 94022 This article is based on speeches given in January and September 1991 at conferences sponsored by the Mid-Coastal California Perinatal Outreach Program. Unique obstacles must be overcome when providing medical care to patients who have an incomplete command of the English language. Serious barriers to effective communication may arise at the exact point where our health care system must succeed or fail. Miscommunication, differences in attitudes about health care, and various other misunderstandings interfere with or frustrate good health care for these patients and their families. Such difficulties are best overcome by the use of a professional interpreter who can ensure good communication between patients and health care professionals. My daily experiences as a professional medical interpreter and translator in Spanish provide insights into the complexities of bilingual and bicultural communication in the hospital setting. Although the examples given relate to Hispanic patients, the lessons learned can be extended to other foreign language patients as well. (Haffner L: Translation is not enough: Interpreting in a medical setting. West J Med 1992;157:255-259) Health care professionals often experience communication difficulties with Spanishspeaking patients; some also have various misconceptions about these patients. As a professional Spanish-language interpreter and translator* at Stanford (California) University Medical Center and being from Nicaragua, I know the problems these patients have in the clinics and the hospital wards. In this article I invite readers to accompany me on a typical day and to share some of these experiences. Some of them are sad, some are amusing, and all are interesting. If they counter a misconception or provide some small insight, I will have been successful. *Although these terms are often used interchangeably, technically interpretation involves oral communication and translation involves written communication. ©2009 Atlanta Academy of Languages, Atlanta GA 71 Before I describe a typical day in my profession, I must point out that not all Spanishspeaking patients are the same. They come from different cultural backgrounds, cultural influences, and educational levels.1 Highly educated and affluent Latinos have attitudes and beliefs about health care reasonably comparable to those of similarly educated and wealthy Americans. The challenge, and the subject of this article, are the Hispanic patients who are poor, come from rural areas, have little or no schooling, and have little or marginal fluency in English. These patients frequently but not necessarily are migrants or recent immigrants. In this article the terms "Hispanic" and "Latino" are used interchangeably to refer to persons who are Spanish speakers and whose principal cultural identity is Latin American. CULTURAL ISSUES My day begins at 8:30 AM. When I arrive at the hospital, three messages are already waiting for me on my beeper. The first is from an anesthesiologist in the Delivery Room who needs me to translate his explanation of the epidural procedure. An 18-year-old Mexican patient is having regular contractions, but she is only 4 cm dilated. The patient is becoming tense and exhausted from the pain, which is interfering with the childbirth process. The nurse has suggested some pain relief medication or an epidural block, but the patient refuses. As I clarify the nurse's offer to the patient, I learn the patient's real concern. She thought that she was being offered a raquea. Raquea or raquidea, a term frequently encountered in patients from rural Mexico, refers to the anesthesia procedure commonly known in the United States as a spinal block. Mexican patients associate raquea with a high incidence of serious complications. This patient is afraid that she would have chronic back problems or be paralyzed for life if given the raquea, problems she believes are caused by that procedure. To make it worse, at this moment her husband reminds her that if she does not have pain, she will not be a real mother, a common belief among Mexican patients. We explain to the patient that the epidural block is not like the raquea, that she would be awake and able to push and actively participate in her baby's birth. Finally, the husband and the patient agree to the epidural, and the baby is born without complications. The problem here is the patient's expectation that medical practices in the United States are the same as in Mexico and her fear (justified or not) about those medical practices, all complicated by basic cultural differences and beliefs. By creating in the patient a better understanding of the epidural procedure, we are able to bridge the language, cultural, and knowledge gaps. By around 9 AM the Obstetrical Diabetic Clinic is active. Each patient is seen by a physician, the hospital's dietitian, a social worker, and the nurse in charge of drawing blood. An interpreter is needed for almost every interaction. One patient, Ramona, is being seen for the first time in this clinic. She is 34 years old, Central American, and poor. She is a first-generation immigrant and, as is typical, believes herself to be a transient by choice. She has the idea that she will return to her country someday and has not committed herself to becoming part of the Anglo culture. "I would learn English if I ©2009 Atlanta Academy of Languages, Atlanta GA 72 planned to stay," is a common comment. Her command of English is exhausted after a few simple words and smiles. As I go into the room, I recognize her from another clinic in the hospital, and we greet each other by name. As part of her medical history, she is asked how many pregnancies she has had. She responds, "two." I continue to interpret for the physician as he asks all the different questions connected with her history. Ramona and I talk a little in Spanish while the physician makes some notes. Latino women, once they get to know you, tend to be talkative. She tells me how worried she is about her diabetes, which she believes she probably caused herself by "doing something wrong." She tells me about a third pregnancy that miscarried due, in her mind, to susto. Susto means "a terrible fright," and she holds the common belief that a terrible fright during pregnancy is bad for both mother and baby and can even kill an unborn child. She explains that, while pregnant, she was taking care of a 15-year-old niece. Suddenly the young girl felt sick to her stomach, went to bed, and died on the spot. Our patient had been terrified and had felt responsible. To make matters worse, the girl's family blamed our patient for the girl's death. The patient was about four months' pregnant at the time and miscarried four days after the incident. On hearing her story, I realize that she actually has had three pregnancies, not the two she had stated in response to the physician's question. For many Hispanic women, having a miscarriage or a stillborn child does not equate with a pregnancy; only the successful pregnancies count. In this example, the patient answered the physician correctly in the context of her cultural views, but, through no fault of his own, the medical history he obtained from this patient was incomplete. Her different cultural attitudes and beliefs are discovered and better understood through our conversation, and a more accurate and complete history results after those beliefs and attitudes are taken into account. At 9:25 AM there is a knock at the door as I finish up with Ramona, this time from the dietitian. The dietitian explains that a patient needs to be put on a special diet for diabetic pregnant mothers, to see if her diabetes could be controlled without insulin. This is a major task of persuasion. There is a saying in Spanish, "Dame gordura y te daré hermosura" ("Give me plumpness and I'll give you beauty"). This idea applies to babies, too. The belief is that a pregnant mother has to eat for two, that a thin baby is undesirable because a thin baby is unhealthy. In addition, many of these patients come from poor rural areas where most of their food is scarce and expensive, where meat is a luxury, and where anything American-made is beyond reach. When these patients come to this country, where food is abundant and comparatively cheap, they naturally tend to indulge. They have difficulty understanding that they should voluntarily go on a diet of restricted foods in the land of plenty. This patient believes in having a big baby, and she enjoys being able to eat anything she wants. We finally convince her that she cannot do this any longer and that, for the sake of her health, she has to diet to have a smaller baby. ©2009 Atlanta Academy of Languages, Atlanta GA 73 Often there is another complication if the family has little money to buy food. The diet we recommend, lots of vegetables and less tortillas and beans, typically is more expensive than what these patients otherwise would eat. It is also less popular because it omits the foods they like the best. The surprising result is that there are fewer compliance problems than would be expected, even with all these frustrations. Having a baby is important to Hispanic women, so most of them overcome their reluctance and comply with the recommended diet or at least try their best with their limited resources. In the Latino culture, women are supposed to sacrifice for the family, even to the point of eating a lot of vegetables.1,2 My next summons is from the Internal Medicine Clinic. The patient, a 50-year-old female peasant from Mexico, is accompanied by her 35-year-old son. Although the patient has been coming to the clinic for some time, she is new to me. Her son usually interprets, as he is reasonably fluent in both languages. This time I am called because the son has to leave to go to work. Before going into the room, the physician expresses to me his concern about whether the health problems claimed by this woman are real or imagined. She has been in the clinic three times before, each time with different vague and diffuse complaints, none of which make medical sense. As we learn, the poor woman has a fistula in her rectum. In her previous visits, she could not bring herself to reveal her symptoms in the presence of, and therefore to, her son as he interprets for her. She tells me that she has been so embarrassed about her condition that she has invented other symptoms to justify her visits to the physician. She confesses that she has been eager to have a hospital staff interpreter from the first visit, but her hope had not materialized until now. This story illustrates two things: first, the modesty of many Latino women can be a serious problem; second, Latino women are often reluctant to reveal personal or private problems if their children are used to interpret. I have seen many Hispanic women who are reluctant to tell their physicians about vaginal problems or to have a Papanicolaou smear done because they are afraid of a pelvic examination.1 Their fear is partly caused by their expectation of discomfort, but to a large degree it is the result of a higher cultural standard of modesty. In addition, traditional Hispanic women often have an amazingly limited knowledge of female sexual anatomy. These attitudes may puzzle Anglo professionals but must be dealt with for medical care to be effective. USING CHILDREN AS INTERPRETERS My day is becoming hectic, and I am needed in several places at once. A common and unfortunate practice when an interpreter is temporarily unavailable is to use family members to interpret. It is easy to forget that the person in the middle is affected by what is happening and must assume a normal family role when the interpreting duties are over. The next page I answer involves this difficult and disturbing problem. The call is to help with a pregnant woman who may have a stillbirth. As I enter the patient's room, the first thing I see is a beautiful little girl with haunting big brown eyes--the patient's 7-year-old daughter. I introduce myself with the proper Spanish salutation. The mother seems upset, ©2009 Atlanta Academy of Languages, Atlanta GA 74 but the daughter looks very distressed and frightened. The child is shaking and with a quiet voice says to me, "No podía explicarle a mi mamá todo lo que los doctores me decían" ("I couldn't explain to my mom everything the doctors were telling me"). I quickly discover that this little girl was used as the interpreter during the ultrasound examination and was told to tell her mother that the baby (her little brother-to-be) is dead. This revelation stuns me. I sit and hold the little girl on my lap, trying to comfort her as she hugs me tightly. I softly talk to her about what has happened, and she starts to weep with big, slow tears. To me, one of the saddest moments is when she says to me, in a pleading voice, "Maybe my little brother's heart will work when he comes out of my mother's stomach." I am reminded of the time when I was required for a family conference for a patient about to be discharged. When I arrive at the conference, present are a physician, a nurse, a physical therapist, a social worker, and several family members. The patient, the father, is absent. Everyone is sitting around a table except one. Standing by the physician is the patient's 9-year-old son, who is acting as the interpreter. The child looks frightened. The physician rather abruptly says to me, "We don't need you, the boy is doing fine." The boy, however, pleads with me to stay and take over, saying, "Please, Señora, can you help me? I don't know if I am doing it right." Having to rely on interpreters certainly can be frustrating at times. The communication is inevitably slower, more awkward, and less precise, even if the interpreter is excellent. Another source of frustration is that the health care professional has less control when having to use an interpreter (professional or otherwise), and some, understandably, have a hard time with this fact. There is a simple explanation: The physician and the patient cannot speak to each other directly. Also, there may be a wait before the interpreter arrives. Because of budgetary constraints, there never are enough interpreters on staff for there to be on-call interpretation available for every need. Medical interpretation often involves unexpected matters of life and death. Being an interpreter is a heavy burden for a child, whose English is frequently marginal and certainly is not sophisticated. Disregard for these factors is hurtful to both the child and the family and threatens the effectiveness of the communication. The trauma to the unfortunate little girl (whose mother has a stillborn) is easily seen. I doubt anyone would consider using a child in this way if there were no language barrier. The situation in which the boy was used as an interpreter is similarly difficult, but the difficulty is perhaps a little more subtle. In rural Hispanic culture, the hierarchy is strict, with authority running from older to younger and from male to female. These relationships are for life, with parents in control of adult children and older adults in control of their younger adult siblings. Traditionally in Latino culture, the head of the family is expected to make the decisions regarding any family member. The whole family looks to this person for support and advice.3 By using a young family member as an interpreter, the physician puts the child in control, with a much higher status than the child would otherwise have. This disrupts the family's social order. ©2009 Atlanta Academy of Languages, Atlanta GA 75 In both of these cases, there was no emergency and no reason not to wait a few minutes for a professional interpreter to arrive. When foreign language gets in the way, however, otherwise sensitive and caring people occasionally become oblivious, and unintended harm can result. INFORMED CONSENT I am getting tired; it is nearly lunchtime, and the pages are relentless. This time I am called to the Well-Baby Nursery, where a woman needs to be asked about some routine matters: the family constellation, safety in the home, safety in the car, breast or bottle feeding, and follow-up care for her baby. Interpreting for the physician, I ask her whether she wants her baby boy circumcised. She nods, but then pauses and very seriously adds, "But my friend had a baby circumcised here, and they did it too much. I don't like how he looks. Can they just cut off a little bit?" To me, the woman clearly wants to decline the procedure but is having difficulty refusing what she considers an instruction from the physician. In general, Latinos feel they should agree with physicians out of politeness and respect, even when they really disagree or do not understand the issues involved. They expect physicians to make the decisions for them and do not understand why they are asked to make choices. They are used to, and seem to prefer, deferring to experts. These patients do not understand the American medical system and its notion of informed consent. Only when more acculturated do they start taking the level of responsibility for their own health that Americans routinely assume. Language and cultural issues once again are intermixed. The next interpreting request, which comes from the Gynecology Ward, involves a different issue of informed consent. The patient, a seriously ill 71-year-old Nicaraguan woman, has been in this country only a few years. Her children have been with her day and night, never leaving her side. When I arrive, the patient's family is distraught. They request a conference with the physician out of the patient's presence. The physician tells the family that the mother is dying and needs radical surgery, but he emphasizes that the surgery would prolong her life only a little. The physician wants to tell the patient and to ask for her consent to the operation. The daughters are very upset and against saying anything to their mother. They beg me to explain that their mother has the right to have hopes, that she should not be told that she is going to die, and that a painful and difficult operation that may buy her only a little more time is cruel. The result is an impasse that looks to go on for several days. The daughters vigilantly watch their mother, guarding her from physicians, and hiding the truth from her. Eventually a compromise is reached, with the patient receiving an accurate but moderated version of the bad news. Here the problem is partly language barriers, but mostly it is conflicting cultural attitudes about how (or whether) bad news should be conveyed to patients. I am convinced that the daughters would have lied to their mother about her condition (and tell the physician they did the opposite) if they were relied on to interpret. Hispanic families often try to hide the seriousness of the situation from ill relatives, especially if the patient may be dying. Instead, the patient is always given encouragement by the family with words like, "It is going to be OK," "You'll be out of here soon," and "The ©2009 Atlanta Academy of Languages, Atlanta GA 76 doctor said that you'll be fine and on your feet again." These desires and cultural practices are directly opposed to the Western notion of informed consent and our practice of describing medical situations in frank, sometimes brutal, detail. Next I am called to the Maternity Ward. A woman had previously signed a consent for an elective tubal ligation after her delivery and is scheduled to have the procedure in half an hour. The nurses noted that she seemed uncertain about the operation and wisely chose to call in an interpreter. It is quickly obvious that the patient has not fully understood that the sterilization is essentially permanent. A tubal ligation has been described to her as having her tubes "tied." She has consented, but with the idea that she can later change her mind-thinking the procedure is easily reversible. If her tubes can be "tied," she reasons, they can be "untied." She began to worry after asking a few questions to confirm her belief. She does not fully understand the answers in English but was having doubts. After I interpret the answers to her questions, she declines the procedure. Many Latinos believe that the main purpose in life is to reproduce, to people the land. This idea is strong and deeply rooted in their religious beliefs, which must be acknowledged, respected, and understood if we want to comprehend their attitudes toward family planning. Another family planning complication in Latinos is that men can feel threatened by the sterilization of the women. They often believe that a woman who is sterilized or uses birth control is going to be unfaithful. Besides, in their eyes, maleness is proved by paternity, and their attitude is that a wife is no longer a complete woman if she cannot bear children. LANGUAGE BARRIERS A patient in another room, a 30-year-old spunky but illiterate poor woman from Mexico, is hard working and proud. She is seven months' pregnant and has diabetes. Her diabetes is under control, and she is generally in good health, but she has complained of swelling and pain in her hands on previous visits. Sitz baths were prescribed so that the patient could have immersion therapy for her hands and arms. Because the physician knew some Spanish and the patient knew a little English, no interpreters were used on previous visits. On this visit, the physician and the dietitian are concerned about the patient's unexpected weight loss during the previous week, and they decide to call for an interpreter to help find the cause. As we try to figure out what is going on, the patient asks me to tell the physician that her hands are still hurting, but she proudly adds that she has been very good about doing her sitz baths. She says, "They are very tiring, but I have been doing them for 20 minutes twice a day." I ask her to tell me what she was doing because I wonder how a bath could be so tiring. Very seriously, she explains she would fill the bathtub with water and get in and sit down. Then she would stand up, sit down, stand up, sit down, stand up, sit down-for 20 minutes at a time. No wonder she was tired! I want to both laugh and cry. The image of this very pregnant woman intently doing deep-knee bends in the bathtub is comical, but her pride and sincerity are touching. If she ©2009 Atlanta Academy of Languages, Atlanta GA 77 had fallen, she could have suffered serious injury. Once again I realize how important good communication is and how risks can be increased by faulty communication. Next I am called to the Emergency Department. When I arrive, the room is full of physicians and nurses. Among them is an x-ray technician busily taking an x-ray film of a man's leg. The patient, a 38-year-old Mexican gardener, had fallen out of a 10-ft high tree. After I introduce myself, the physicians and I ask the patient routine questions. The man keeps repeating, "Mi canilla, mi canilla." Somebody else in the room knew a little Spanish, which explains to me why the technician is taking x-ray films of the man's leg. I tell them that he means his wrist, which turns out to be broken. In most Spanish-speaking countries, canilla means shinbone and the use of canilla for the wrist is a little unusualexcept in certain parts of Mexico where the word means wrist. Spanish technically is not divided into dialects, but the meaning of a word can vary by context or the region of the speaker. I sometimes observe physicians and nurses who know a little of the language trying to converse in Spanish with their Hispanic patients. I always encourage this practice. Among other benefits, it helps make a patient feel more comfortable and builds rapport.4 It is important when making this effort not to overestimate language abilities and to remember that a much lower skill level of communication is required for "chatting." It is also important to remember that even if a question appears to be more or less understood by the patient, the answer may not be understood by the health care professional well enough to be the basis for a medical decision. Learning a foreign language to the point of the true bilingualism of a professional interpreter takes a lot of time and practice, and the subtleties involved-and the potentially disastrous consequences of an error in interpretation-are even more telling in the medical context. Proper medical interpretation requires a firm grasp of two different and complex languages to achieve immediate, highly functional, and accurate translation, often at times of high stress and in critical circumstances, plus an ability to communicate effectively in each language at many different educational levels. A modest course of study in Spanish is not enough to interpret reliably in a medical situation. An inexperienced Spanish speaker usually does not know the right Spanish word or may know the right word but not how to pronounce it properly. The results can be confusing, insulting, or comic. One physician who was trying to be friendly with a female patient, asked her, "¿Cuántos anos tiene usted?" He intended, "¿Cuántos años tiene usted?" ("How old are you?"), but, by mispronouncing the word años as anos, what he really asked was, "How many anuses do you have?" In another case, a 70-year-old Cuban woman was being discharged from the hospital into the care of her daughter, also a non-English-speaking resident of Cuba. The woman's granddaughter was doing the interpreting, as she had throughout the hospital stay with reasonable success. The young girl thought she did a good job of clearly explaining the discharge instructions, but her aunt, the person for whom she was interpreting, did not understand that the grandmother's medication was to be tapered off. Instead, after release ©2009 Atlanta Academy of Languages, Atlanta GA 78 from the hospital, the aunt cut back the dosage suddenly. This error was discovered only when the patient returned to the hospital very ill with other complications. The granddaughter, although fully bilingual, was not trained to make certain her aunt fully understood the instructions. In these instances, "back-interpretation" should be usedask that the interpreted instructions be repeated back so that any miscommunication can be detected and corrected and questions can be cleared up. I am asked many times, "How do you say this or that in Spanish?" In most cases several words or expressions need to be tried until the interpreter is certain that the patient truly understands what the interpreter is trying to say. Few Spanish-speaking patients or families ask a lot of questions. Most of the time they just nod and go home, wondering what they were told in the hospital or the clinic. Using a professional interpreter who is aware of this tendency helps to avoid misunderstandings. So goes a typical day in a large university medical center. This account of my daily experiences shows why it is important to always use professional interpreters in medical settings. This may not always be possible, of course, because of limited staffing or in emergencies. It is tempting, when rushed for time, to forge ahead and "make do," relying on dimly remembered high school Spanish plus the patient's or a family member's broken English. However tempting it may be, this choice should be avoided. A little Spanish and broken English typically are inadequate for the level of communication required for good medical care. Using family members, friends of the patient, or Latino cleaning staff rarely is sufficient and can have bizarre consequences.5,6 Cleaning staff are untrained and inexperienced in medical interpretation, among other problems. Family members-and patients, for that matter-similarly are untrained and inexperienced and may suffer a dramatic decline in English proficiency when confronted with the stresses inherent in the context of illness. It has been observed that the "language of our childhood remains the language used during times of intimacy and stress."1 Professional interpreters are the conduit for effective, efficient, and reliable communication between a health care professional and a patient or family member not fluent in English. Health care professionals must recognize that the situation always is bicultural and not merely bilingual. Successful communication between a health care professional and a patient, if a non-English speaker is involved, requires more than mechanical translation between English and the foreign language. The use of a professional interpreter can help achieve this objective. REFERENCES 1. Poma PA: Pregnancy in Hispanic women. J Natl Med Assoc 1987;79:929-935 2. Hall TA: Designing culturally relevant educational materials for Mexican American clients. Diabetes Educat 1987;13:281-285 3. Poma PA: Impact of culture on health care: Hispanos. Illinois Med J 1979;156:451-458 4. Swartz MH: Textbook of Physical Diagnosis. New York, NY, WB Saunders/Harcourt Brace Jovanovich, 1989 ©2009 Atlanta Academy of Languages, Atlanta GA 79 5. Rader G: Management decisions: Do we really need interpreters? Nurs Manage 1988;19:46-48 6. Carol E: Use of interpreters in medical care. Sonoma Co Physician 1991;42:28-31 ©2009 Atlanta Academy of Languages, Atlanta GA 80 STANDARDS OF PRACTICE FOR MEDICAL INTERPRETERS Atlanta Academy of Languages ACCURACY OBJECTIVE: To interpret with the highest degree of accuracy achievable. Related Ethical Principle: Interpreters strive to render the message accurately, conveying the content and spirit of the original message, taking into consideration the cultural context. 1. The interpreter renders all messages accurately and completely, without adding, omitting, or substituting. For example, an interpreter repeats all that is said, even if it seems redundant or irrelevant. This information may be more important than the interpreter realizes. 2. The interpreter replicates the register, style, and tone of the speaker. For example, unless there is no equivalent in the patient/provider 's language, an interpreter does not substitute simpler explanations for medical terms a speaker uses, but may ask the speaker to re-express themselves in language more easily understood by the other party. 3. The interpreter advises parties that everything said will be interpreted. For example, an interpreter may explain the interpreting process to a provider by saying "everything you say will be repeated to the patient/provider" 4. The interpreter manages the flow of communication. ©2009 Atlanta Academy of Languages, Atlanta GA 81 For example, an interpreter may ask a speaker to pause or slow down. 5. The interpreter corrects errors in interpretation. For example, an interpreter who has omitted an important word corrects the mistake as soon as possible. 6. The interpreter maintains transparency. For example, when asking for clarification, an interpreter says to all parties, "I, the interpreter, did not understand, so I am going to ask for an explanation." CONFIDENTIALITY OBJECTIVE: To honor the private and personal nature of the educational interaction and maintain trust among all parties. To be in constant compliance with the Health Insurance Portability and Accountability Act (HIPAA). Related Ethical Principle: Interpreters treat as confidential, within the direct clinical team, all information learned in the performance of their professional duties, while observing relevant requirements regarding disclosure. 7. The interpreter maintains confidentiality and does not disclose information outside the treating team, except if required by law. For example, an interpreter does not discuss a patient’s case with his/her own family or with community members. ©2009 Atlanta Academy of Languages, Atlanta GA 82 8. The interpreter protects written patient information in his or her possession. For example, an interpreter does not leave notes on an interpreting session in public view. IMPARTIALITY OBJECTIVE: To eliminate the effect of interpreter bias or preference. Related Ethical Principle: Interpreters strive to maintain impartiality and refrain from counseling, advising, or projecting personal biases or beliefs. 9. The interpreter does not allow his/her own personal judgments or cultural values to influence objectivity. For example, an interpreter does not reveal personal feelings through words, tone of voice, or body language. 10. The interpreter discloses potential conflicts of interest, withdrawing from assignments where such a conflict of interest may in reality exist or appear to exist. For example, an interpreter avoids interpreting for a family member or close friend, or for neighbors. ©2009 Atlanta Academy of Languages, Atlanta GA 83 RESPECT OBJECTIVE: To acknowledge the inherent dignity of all parties in the interpreted encounter. Related Ethical Principle: Interpreters treat all parties with respect. 11. The interpreter uses professional, culturally appropriate ways of showing respect. For example, in greetings, an interpreter uses appropriate titles for both parents and providers. Interpreters use the polite form of address (in languages where such distinctions are customary) appropriately. 12. The interpreter promotes direct communication among all parties in the encounter. For example, an interpreter may tell the patient and the speaker to address each other directly, rather than addressing the interpreter. 13. The interpreter promotes patient/provider autonomy. For example, an interpreter directs a patient who asks him or her for a ride home to appropriate resources within the institution. ©2009 Atlanta Academy of Languages, Atlanta GA 84 CULTURAL AWARENESS OBJECTIVE: To facilitate communication across cultural differences. Related Ethical Principle: Interpreters strive to develop awareness of the cultures encountered in the performance of interpreting duties. 14. The interpreter strives to understand the cultures associated with the languages he or she interprets, including the culture(s) in regard to health care, and represents the non-speaker of that language in the most culturally-appropriate manner possible. For example, an interpreter learns about the health care system and customs, etc. of countries where the patient’s language is spoken. When interpreting, s/he may also suggest appropriate ways to approach a variety of topics and create a higher degree of trust among the parties involved. 15. The interpreter alerts all parties to any significant cultural misunderstanding that arises. For example, if a speaker recommends that a patient who is fasting for religious reasons eat a good breakfast, an interpreter may call attention to the potential conflict. ©2009 Atlanta Academy of Languages, Atlanta GA 85 ROLE BOUNDARIES OBJECTIVE: To clarify the scope and limits of the interpreting role, in order to avoid conflicts of interest. Related Ethical Principle: The interpreter maintains the boundaries of the professional role, refraining from personal involvement. 16. The interpreter limits personal involvement with all parties during the interpreting assignment. For example, an interpreter does not share or elicit overly personal information in conversations with a patient. 17. The interpreter limits his or her professional activity to interpreting within an encounter. For example, an interpreter never advises a patient in regards to medical or health care questions or decisions, but redirects the patient to ask the provider. 18. The interpreter with an additional role adheres to all interpreting standards of practice while interpreting. For example, an interpreter who is also a patient representative/chaplain/nurse does not confer with another provider in the patient’s presence, without reporting what is said. ©2009 Atlanta Academy of Languages, Atlanta GA 86 PROFESSIONALISM OBJECTIVE: To uphold the public’s trust in the interpreting profession. Related Ethical Principle: Interpreters at all times act in a professional and ethical manner. 19. The interpreter is honest and ethical in all business practices. For example, an interpreter accurately represents his or her credentials and therefore does not claim to have expertise in the field of education other than those reflected by his/her specific experience, job position, and/or professional degrees. 20. The interpreter is prepared for all assignments. For example, an interpreter asks about the nature of the assignment and reviews relevant terminology prior to an assignment. 21. The interpreter discloses skill limitations with respect to particular assignments. For example, an interpreter who is unfamiliar with a medical term or acronym (such as MI or TIA) asks for an explanation before continuing to interpret. ©2009 Atlanta Academy of Languages, Atlanta GA 87 22. The interpreter avoids sight translation (reading a text silently and then rapidly translating it orally), especially of complex or critical documents, if he or she lacks sight translation skills. For example, when asked to sight translate a consent form, an interpreter instead asks the speaker to explain its content and then interprets the explanation. 23. The interpreter is accountable for professional performance. For example, an interpreter does not blame others for his or her interpreting errors. 24 The interpreter advocates for working conditions that support quality interpreting. For example, an interpreter on a lengthy assignment indicates when fatigue might compromise interpreting accuracy. 25. The interpreter shows respect for professionals with whom he or she works. For example, an interpreter does not spread rumors that would discredit another interpreter. 26. The interpreter acts in a manner befitting the dignity of the profession and appropriate to the setting. For example, an interpreter dresses appropriately and arrives on time for appointments. ©2009 Atlanta Academy of Languages, Atlanta GA 88 PROFESSIONAL DEVELOPMENT OBJECTIVE: To attain the highest possible level of competence and service. Related Ethical Principle: Interpreters strive to further their knowledge and skills, through independent study, continuing education, and actual interpreting practice. 27. The interpreter continues to develop language and cultural knowledge, as well as interpreting skills. For example, an interpreter stays up to date on changes in medical terminology, health care trends or practices, current health care concerns, and/or regional slang. 28. The interpreter seeks feedback to improve his or her performance. For example, an interpreter consults with colleagues about a challenging assignment and on occasion asks that another qualified interpreter observe an encounter in order to provide honest and useful feedback. 29. The interpreter supports the professional development of fellow interpreters. ©2009 Atlanta Academy of Languages, Atlanta GA 89 For example, an experienced interpreter mentors novice interpreters. 30. The interpreter participates in organizations and activities that contribute to the development of the profession. For example, an interpreter attends professional workshops and conferences. ADVOCACY OBJECTIVE: To prevent harm to parties that the interpreter serves. Related Ethical Principle: When the patient’s health, well-being or dignity is at risk, an interpreter may be justified in acting as an advocate. 31. The interpreter may speak out to protect an individual from serious harm. For example, an interpreter may intervene on behalf of a patient with a life-threatening allergy or a severe fear/phobia, if the condition has been overlooked. 32. The interpreter may advocate on behalf of a party or group to correct discrimination, mistreatment or abuse. For example, an interpreter may alert his or her supervisor to patterns of disrespect towards patients. ©2009 Atlanta Academy of Languages, Atlanta GA 90 The competent interpreter: 1. Introduces self and explains role. Ideally, the interpreter consults first with the provider to learn the goals of the medical encounter, and with the patient to assess language requirements. Then, if this is their first meeting, the interpreter explains his role to both the patient and provider. The interpreter must emphasize the professional obligation to transmit everything that is said in the encounter to the other party and to maintain confidentiality. 2. Positions self to facilitate communication. The interpreter should be seen and heard by both parties, but should position herself in the place that is least disruptive to direct communication between provider and patient, and most respectful of the patient's physical privacy. 3. Accurately and completely relays the message between patient and provider. The interpreter converts oral messages expressed in one language into their equivalent in the other, so that the interpreted message can elicit the same response as the original. The interpreter does not alter or edit statements from either party, or comment on their content. The goal is for the patient and the provider to feel as if they are communicating directly with one another. 4. Uses the interpretation mode that best enhances comprehension. The interpreter encourages direct communication between patient and provider using whatever modes are appropriate. Usually the best mode will be to use "I..." in reference to the speaker rather than "he said that..." or "she said that..." and to interpreter for the patient and the provider alternately. 5. Reflects the style and vocabulary of the speaker. The interpreter attempts to preserve the register (special vocabulary and level of formality) as well as the emphasis and degree of emotion expressed by the speaker. 6. Ensures that the interpreter understands the message to be transmitted. The interpreter asks for clarification or repetition if the message from either party is unclear. 7. Remains neutral. In situations where there is conflict between patient and provider, the interpreter remains outwardly calm, continues interpreting completely, lets the parties speak for themselves and does not take sides. 8. Identifies and separates personal beliefs from those of other parties. The interpreter does not project his own values into the discussion. 9. Identifies and corrects own mistakes. The interpreter checks the accuracy of her own interpretation. 10. Addresses culturally based miscommunication when necessary. The interpreter identifies instances in which cultural differences between provider and patient have the potential to seriously impair their communication. In those instances, the interpreter shares cultural information with both ©2009 Atlanta Academy of Languages, Atlanta GA 91 parties that may be relevant, or assists the speaker in developing an explanation that can be understood by the listener. Professional Standards: Ethics Professional ethics are rules that help you maintain a professional relationship with the people you work with and for. A medical interpreter must maintain a professional relationship with both the patient and the provider in a health care encounter. The Working Group recommends the following set of professional ethics standards. An ethical interpreter: 1. Maintains confidentiality. Information exchanged in any interpreter exchange--for example, between a patient and a health care provider--is private. The interpreter does not intentionally reveal confidential information. 2. Interprets accurately and completely. The interpreter is committed to transmitting the content and spirit of the original message into the other language without omitting, modifying, condensing or adding. 3. Maintains impartiality. The interpreter withdraws from assignments where personal ties or beliefs may affect impartiality and refrains from interjecting personal opinions or biases into the interview. 4. Maintains professional distance. The interpreter understands the boundaries of the professional role and monitors her own personal agenda, refraining from becoming personally involved in a patient's life. 5. Knows own limits. The interpreter refrains from interpreting beyond his training, level of experience and skills. In addition, he avoids situations that may represent a conflict of interest or may lead to personal or professional gain. 6. Demonstrates professionalism. The interpreter clearly understands her role and refrains from delivering services that are not part of that role. The interpreter conducts herself in dress, posture and speech in a manner appropriate to the situation, and is respectful, courteous and honest. ©2009 Atlanta Academy of Languages, Atlanta GA 92 OTHER SUGGESTIONS: BODY POSTURING: HANDS FEET SHOULDERS LOCATION Remember: The goal of all body positioning and body language should be enhancing effective and direct communication between the healthcare provider and the patient. ©2009 Atlanta Academy of Languages, Atlanta GA 93 APUNTES SOBRE TERMINOLOGÍA MÉDICA (A PROPÓSITO DEL TALLER EN LAS TUNAS) 1- ACENTUACIÓN DE LETRAS MAYÚSCULAS Recordar que todas las letras mayúsculas deben llevar tilde al igual que las minúsculas cuando así lo recomienden las normas ortográficas. 2- USO EXCESIVO DE LETRAS MAYÚSCULAS EN TEXTOS Las letras mayúsculas en los textos deben limitarse en lo posible a nombres propios, de países, de ciudades, de instituciones y como primera letra de cualquier párrafo o de ciertas abreviaturas. 3- USO DEL GERUNDIO EN MEDICINA Tratar de evitar el uso del gerundio (terminaciones en –ando, -iendo) cuando no expresen acciones simultáneas con el verbo principal. 4- USO DE ABREVIATURAS Siempre que se utilice una abreviatura en un texto por primera vez debe escribirse al lado entre paréntesis su significado. 5- EXPRESIONES INADECUADAS a) PALABRAS TOMADAS DIRECTAMENTE DE OTRO IDIOMA INCORRECTAS CORRECTAS shock choque stress estrés tractus, tracto vía, tubo ductus conducto déficit deficiencia, insuficiencia shunt derivación, cortocircuito testis, testes testículo canal conducto diabetes mellitus diabetes sacarina septum, septo tabique b) PALABRAS PARECIDAS A LAS DEL INGLÉS INCORRECTAS canalículo transplante imagenología reasumir malrotación droga ostomía sonda de Levine ©2009 Atlanta Academy of Languages, Atlanta GA CORRECTAS conductillo trasplante imaginología reiniciar rotación anómala fármaco, medicamento estoma sonda de tipo Levin 94 amoxicillina ampicillina salvataje remover consentimiento informado INCORRECTAS patología severo scintigrafía manejo amoxicilina ampicilina preservación extirpar, extraer autorización verbal o escrita CORRECTAS enfermedad, afección grave, intenso, extenso ganmagrafía conocimiento (enfermedades) tratamiento (enfermos) exstrofia asistencia (en determinado contexto) proquinéticos citoquinas desorden fallo cardiaco división de un órgano precoz proceder (como sustantivo) usualmente extrofia ayuda procinéticos citocinas enfermedad, alteración insuficiencia cardiaca sección o incisión temprano, preclínico procedimiento con frecuencia, frecuentemente, generalmente efusión derrame ultrasonido (examen complementario) ecografía invasivo cruento no invasivo incruento resucitación reanimación o reposición de volumen sanguíneo desorden enfermedad, alteración infante niño pacientes en edad pediátrica niño, niñez 5- ERRORES DE GÉNERO O DE ACENTUACIÓN INCORRECTAS CORRECTAS el éxtasis la estasis la hipospadia el hipospadias la epispadia el epispadias -scopía -scopia epístaxis epistaxis anastómosis anastomosis quémosis quemosis equímosis equimosis ©2009 Atlanta Academy of Languages, Atlanta GA 95 6- PALABRAS QUE NO EXISTEN EN LOS DICCIONARIOS INCORRECTA CORRECTA sangramiento sangrado, hemorragia lisar seccionar, separar íctero ictericia endopleural pleural minitoracotomía toracotomía pequeña transabdominal intra(a)bdominal transoperatorio intraoperatorio, perioperatorio protocolizar siclemia siclémico hacer un protocolo, incluir en un protocolo drepanocitemia, anemia drepanocítica paciente con drepanocitemia 7- INCORRECCIONES EN LA GRAFÍA DE PALABRAS Y ACRÓNIMOS INCORRECTAS CORRECTAS la TAC el tac SIDA sida delección deleción meningococcemia meningococemia desición decisión autoingerto autoinjerto debridar desbridar decamación descamación 8- EXPRESIONES INADECUADAS INCORRECTA CORRECTA de acuerdo a de acuerdo con asociado a asociado con relacionado a relacionado con respecto con respecto a mortalidad (con respecto a una enferm.) letalidad cirugía (como procedimiento) operación, intervención quirúrgica sepsis (limitada) infección sepsis generalizada sepsis ©2009 Atlanta Academy of Languages, Atlanta GA 96 hematoma infestado hematoma infectado 9- UNIDADES DE MEDIDA Siempre se debe tratar de utilizar las unidades internacionales, y emplear abreviaturas escritas con minúsculas y sin punto (m, cm, kg, ml, etc.). 10- TAXONOMÍA DE LOS GÉRMENES: Deben escribirse en palabras procedentes del latín con letras cursivas, o en español, pero utilizando la grafía correcta. INCORRECTO CORRECTO Streptococus Pyogenes Streptococcus pyogenes, estreptococo piógeno Prescription Terms & Abbreviations Prescription abbreviation a ac ad lib AM ASAP BID c d h hs mo p pc PM PRN q qAM QD q4h QID QOD qPM rep Prescription term before before meals as desired morning as soon as possible twice a day with day hour bedtime (hour of sleep) month after after meals evening as needed every every morning every day every four hours four times a day every other day every evening repeat ©2009 Atlanta Academy of Languages, Atlanta GA 97 STAT TID UD wk i ii iii iv v vi vii viii ix x xii xv xvi xx xxx L C D M ss cc g, G, GM gal gr L lb mEq mcg mg mL no. oz pt qt tsp tbsp BP NOW-immediately three times a day as directed week 1 2 3 4 5 6 7 8 9 10 12 15 16 20 30 50 100 500 1000 1/2 cubic centimeter gram gallon grain liter pound milliEquivalent microgram milligram milliliter number ounce pint quart teaspoon one tablespoon blood pressure ©2009 Atlanta Academy of Languages, Atlanta GA 98 c D/C Disp HA non rep N/V qs, qsad Rx s Sig sx T, temp < > with discontinue dispense headache no refill nausea and vomiting fill up to prescription; take without signatura; directions for the patient symptoms temperature less than more than ©2009 Atlanta Academy of Languages, Atlanta GA 99 Medical Terminology Quiz Matching exercise acro ??? chir-, chiro- ??? pod-, poda- ??? thorac-, thoraco- ??? broch-, broncho- ??? pneu-, pneumo- ??? pulmo-, pulmono- ??? angi-, angio- ??? vas-, vaso-, vasculo- ??? cardi-, cardio- ??? phleb-, phlebo- ??? vene-, veno- ??? throm-, thrombo- ??? viscero- ??? col-, colo- ??? cyst-, cysto- ??? enter-, entero- ??? mast-, masto- ??? metra-, metro- ??? gastr-, gastro- ??? Top of Form ©2009 Atlanta Academy of Languages, Atlanta GA 100 ANSWER KEY TO PREVIOUS PAGE QUIZ acrochir-, chiropod-, podathorac-, thoracobroch-, bronchopneu-, pneumopulmo-, pulmonoangi-, angiovas-, vaso-, vasculocardi-, cardiophleb-, phlebovene-, venothrom-, thromboviscerocol-, colocyst-, cystoenter-, enteromast-, mastometra-, metrogastr-, gastro- usually refers to extremities relationship to the hand relationship to the foot relationship to the chest relationship to the bronchi relationship to the lungs relationship to the lungs relationship to the blood vessels relationship to the blood vessels relationship to the heart relationship to the veins relationship to the veins relationship to a clot relationship to the body organs relationship to the large intestine association with the urinary bladder association with the intestine association with the breast uterus association with the stomach ©2009 Atlanta Academy of Languages, Atlanta GA :-) :-) :-) :-) :-) :-) :-) :-) :-) :-) :-) :-) :-) :-) :-) :-) :-) :-) :-) :-) 101 PRACTICE QUIZ 1. -emia means: Blood Condition. NEPHRO = HEPATO = Deficiency. Excess of. MYEL = Death of 2. -pnea means : LITHO = Break. Breathing. GLOSS0 = Swallowing. Circulation. OTO = 3. -stenosis means: Hardening. RHINO = Constriction. Expanding. ENCEPHO = Malignancy. 4. -ostomy means: OSTEO = Cut into or incision. Ablation. STOMATO = Enlargement. Create an artificial opening. ©2009 Atlanta Academy of Languages, Atlanta GA GASTRO = 102 5. -otomy means: Cut into or incision. ENTERO = Ablation. Enlargement. Create an artificial opening. ORCHIDO = POD = 6. -megaly means: -ALGIA Multiply. Ablation. - HISTERO Enlargement. Diseased. - ARTRO 7. -plasia means: Formation, development or growth. MASTO Repairing of, suturing. Metastisizing of a tumor. Condition. 8. -cele means: Cell. Chest. Cavity. Swelling, protrusion. ©2009 Atlanta Academy of Languages, Atlanta GA 103 9. -itis means: Itching. Burning. Scaly. Inflammation. 10. The Suffix "pepsia" refers to: Chest muscles The nervous system Digestion Hearing 11. onc/o means: old cancer tumor deadly 12. iatr/o means: hirsute iodine physician, medicine cold 13. lip/o: white fat rough soft ©2009 Atlanta Academy of Languages, Atlanta GA 104 14. xantho means: yellow brown anti reversed 15. eti/o (as in etiology): system science of cause history 16. dys- means: two difficult easy forked 17. hypo- means: below, incomplete over, outside through inside, within 18. chrom/o means: silver color brittle shiny ©2009 Atlanta Academy of Languages, Atlanta GA 105 19. rhabd/o means: rod-shaped science of rapid history 20. sarco means: flesh, connective tissue solid opaque forked 21. Endo means: Above. Below. Within. Fat. 22. Thromb/o means: To throb. To divide. To clot. To dry out. 23. Brady- means: Fast. Irregular. Prolonged. Slow. ©2009 Atlanta Academy of Languages, Atlanta GA 106 24. Salping/o means . Fallopian tube. Pus. Polyp. Flesh, connective tissue. 25. Onych/o means Testicle. The same as Orchi/o. Single, one. Nail. 26. Tachy- (as in tachycardia) means: A slowing down Irregular Fast or rapid Malignant 27. andro means: above, over human through male 28. viscer/o means: cut open internal organs exoskeleton relate to ©2009 Atlanta Academy of Languages, Atlanta GA 107 29. cyano blue white cyanide large 30. gno/o means: small knowledge science of branch 31. cyto means fat smooth blue cell 32. myo- refers to your: brain myoptic nerve feet muscle 33. neuro means: nerve new digestive system endocrine system ©2009 Atlanta Academy of Languages, Atlanta GA 108 34. kary / o means cell karaoke nucleus illness 35. leuk/o means: white limpid black sickle-shaped 36. erythro/o means: membrane heart-shaped red brown 37. histo/o means: film time tissue yellow 38. melano means: black diseased malignant cancer ©2009 Atlanta Academy of Languages, Atlanta GA 109 39. path/o means: within purple excised disease 40. somat/o means: extremity body tissue nerve ©2009 Atlanta Academy of Languages, Atlanta GA 110
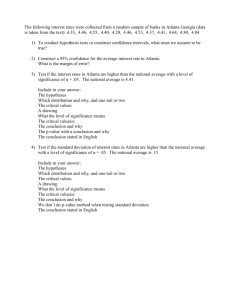
![[Your Name] Skills Profile Work History](http://s3.studylib.net/store/data/008337404_1-3d242ce7f6b5e92a9d69c7d0772f4a68-300x300.png)