Dr.Kaan Yücel http://yeditepeanatomy1.org Bones of the upper limb
advertisement

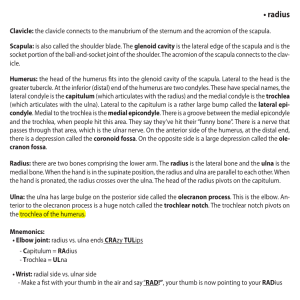
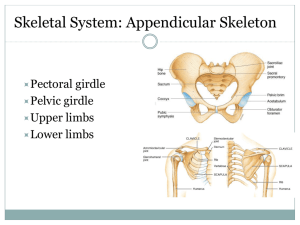
BONES OF THE UPPER LIMB 03 01. 2014 Kaan Yücel M.D., Ph.D. http://yeditepeanatomy1.org Dr.Kaan Yücel http://yeditepeanatomy1.org Bones of the upper limb The upper limb is characterized by its mobility and ability to conduct fine motor skills (manipulation). These characteristics are especially marked in the hand. One of the major functions of the hand is to grip and manipulate objects. Based on the position of its major joints and component bones, the upper limb is divided into shoulder, arm, forearm, and hand for precise description. The superior appendicular skeleton articulates with the axial skeleton only at the sternoclavicular joint, allowing great mobility. The clavicles and scapulae of the pectoral girdle are supported, stabilized, and moved by axioappendicular muscles that attach to the relatively fixed ribs, sternum, and vertebrae of the axial skeleton. The clavicle is the only bony attachment between the trunk and the upper limb. The medial end is called “sternal end". The lateral end is called “acromial” end”. The scapula lies on the posterolateral aspect of the thorax. It has medial, lateral, and superior borders and superior, lateral, and inferior angles. The posterior surface of the scapula is unevenly divided by spine of the scapula, into a small supraspinous fossa and a much larger infraspinous fossa. The spine continues laterally as the flat expanded acromion, which forms the subcutaneous point of the shoulder and articulates with the acromial end of the clavicle. The concave costal surface of most of the scapula forms a large subscapular fossa. The skeletal support for the arm is the humerus. The humerus (arm bone) articulates with the scapula at the glenohumeral joint and the radius and ulna at the elbow joint. The proximal end of the humerus has a head, surgical and anatomical necks, and greater and lesser tubercles. The distal end of the humerus has a condyle, two epicondyles, and three fossae. Ulna is the medial and longer of the two forearm bones.It is the stabilizing bone of the forearm. Radius is the lateral and shorter of the two forearm bones. The hand is the region of the upper limb distal to the wrist joint. It is subdivided into three parts: wrist, (carpus); metacarpus; digits (five fingers including the thumb). 2 http://www.youtube.com/yeditepeanatomy Dr.Kaan Yücel http://yeditepeanatomy1.org Bones of the upper limb 1. UPPER LIMB The upper limb is characterized by its mobility and ability to conduct fine motor skills (manipulation). These characteristics are especially marked in the hand. One of the major functions of the hand is to grip and manipulate objects. Efficiency of hand function results in large part from the ability to place it in the proper position by movements at the scapulothoracic, glenohumeral, elbow, radio-ulnar, and wrist joints. Unlike the lower limb, which is used for support, stability, and locomotion, the upper limb is highly mobile for positioning the hand in space. The upper limb is associated with the lateral aspect of the lower portion of the neck and with the thoracic wall. It is suspended from the trunk by muscles and a small skeletal articulation between the clavicle and the sternum: the sternoclavicular joint. Based on the position of its major joints and component bones, the upper limb is divided into shoulder, arm, forearm, and hand for precise description: • Shoulder: is the proximal segment of the limb and the area of upper limb attachment to the trunk. The pectoral (shoulder) girdle is a bony ring, incomplete posteriorly, formed by the scapulae and clavicles and completed anteriorly by the manubrium of the sternum (part of the axial skeleton). • Arm (L. brachium): first segment of the free upper limb (more mobile part of the upper limb independent of the trunk) and the longest segment of the limb. The arm is the part of the upper limb between the shoulder and the elbow joint. It extends between and connects the shoulder and the elbow and consists of anterior and posterior regions of the arm, centered around the humerus. • Forearm (L. antebrachium): second longest segment of the limb. The forearm is between the elbow joint and the wrist joint. The forearm includes anterior and posterior regions of the forearm overlying the radius and ulna. • Hand (L. manus): is the part of the upper limb distal to the forearm. The hand is formed around the carpus, metacarpus, and phalanges. It is composed of the wrist, palm, dorsum of hand, and digits (fingers, including an opposable thumb). 3 Dr.Kaan Yücel http://yeditepeanatomy1.org Bones of the upper limb Figure 1. Regions of the body and the upper limb http://psychology.wikia.com/wiki/Mouth_(human) 2. BONES OF THE UPPER LIMB The pectoral girdle and bones of the free part of the upper limb form the superior appendicular skeleton; the pelvic girdle and bones of the free part of the lower limb form the inferior appendicular skeleton. The superior appendicular skeleton articulates with the axial skeleton only at the sternoclavicular joint, allowing great mobility. The clavicles and scapulae of the pectoral girdle are supported, stabilized, and moved by axioappendicular muscles that attach to the relatively fixed ribs, sternum, and vertebrae of the axial skeleton. Figure 2. Bones of the upper limb https://encrypted-tbn2.gstatic.com/images?q=tbn:ANd9GcSW8LslcjBie9q3v6c-iF5_yVmA8HzibdIxevO5SvdpHeTI8MDa 4 http://www.youtube.com/yeditepeanatomy Dr.Kaan Yücel http://yeditepeanatomy1.org Bones of the upper limb 3. BONES OF THE PECTORAL GIRDLE 3.1. CLAVICLE (COLLAR BONE) The clavicle is the only bony attachment between the trunk and the upper limb. It is palpable along its entire length and has a gentle S-shaped contour, with the forward-facing convex part medial and the forward-facing concave part lateral. The medial end is called “sternal end". The sternal end is enlarged and triangular where it articulates with the manubrium of the sternum at the sternoclavicular joint. The lateral end is called “acromial” end”. The acromial end is flat where it articulates with the acromion of the scapula at the acromioclavicular joint. Figure 3. The location of the clavicle http://www.daviddarling.info/images/clavicle.gif The medial two thirds of the shaft of the clavicle are convex anteriorly, whereas the lateral third is flattened and concave anteriorly. These curvatures increase the resilience of the clavicle and give it the appearance of an elongated capital S. Although designated as a long bone, the clavicle has no medullary (marrow) cavity. It consists of spongy (trabecular) bone with a shell of compact bone. The inferior surface of the clavicle is rough because strong ligaments bind it to the 1st rib near its sternal end and suspend the scapula from its acromial end. The conoid tubercle, near the acromial end of the clavicle, gives attachment to the conoid ligament, the medial part of the coracoclavicular ligament. Also, near the acromial end of the clavicle is the trapezoid line, to which the trapezoid ligament attaches; it is the lateral part of the coracoclavicular ligament. The subclavian groove (groove for the subclavius) in the medial third of the shaft of the clavicle is the site of attachment of the subclavius muscle. More medially is the impression for the costoclavicular ligament, a rough, often depressed, oval area that gives attachment to the ligament binding the 1st rib (L. costa) to the clavicle, limiting elevation of the shoulder. 5 Dr.Kaan Yücel http://yeditepeanatomy1.org Bones of the upper limb Functions of the clavicle: • Serves as a moveable, rigid support from which the scapula and free limb are suspended, keeping them away from the trunk so that the limb has maximum freedom of motion. The support formed by the clavicle is movable and allows the scapula to move on the thoracic wall at the “scapulothoracic joint,” increasing the range of motion of the limb. Fixing the point of the support in position, especially after its elevation, enables elevation of the ribs for deep inspiration. • Forms one of the bony boundaries of the cervico-axillary canal (passageway between the neck and the arm), affording protection to the neurovascular bundle supplying the upper limb. • Transmits shocks (traumatic impacts) from the upper limb to the axial skeleton. Figure 4. Clavicle http://medchrome.com/basic-science/anatomy/clavicle 3.2. SCAPULA (SHOULDER BLADE) The scapula is a large, flat triangular bone which lies on the posterolateral aspect of the thorax, overlying the 2nd-7th ribs with: three angles (lateral, superior, and inferior) three borders (superior, lateral, and medial) two surfaces (costal and posterior) three processes (acromion, spine, and coracoid process) The scapula has medial, lateral, and superior borders and superior, lateral, and inferior angles. Borders (margins) of the scapula Medial border: When the scapular body is in the anatomical position, the thin medial border of the scapula runs parallel to and approximately 5 cm lateral to the spinous processes of the thoracic vertebrae; hence it is often called the vertebral border. 6 http://www.youtube.com/yeditepeanatomy Dr.Kaan Yücel http://yeditepeanatomy1.org Bones of the upper limb Lateral border: From the inferior angle, the lateral border of the scapula runs superolaterally toward the apex of the axilla; hence it is often called the axillary border. The lateral border is made up of a thick bar of bone that prevents buckling of this stressbearing region of the scapula.The lateral border terminates in the truncated lateral angle of the scapula, the thickest part of the bone that bears the broadened head of the scapula. The glenoid cavity is the primary feature of the head. The shallow constriction between the head and the body defines the neck of the scapula. Superior border: is marked near the junction of its medial two thirds and lateral third by the suprascapular notch. The suprascapular notch is located where the superior border joins the base of the coracoid process. The superior border is the thinnest and shortest of the three borders. The scapula is capable of considerable movement on the thoracic wall at the physiological scapulothoracic joint, providing the base from which the upper limb operates. Posterior surface of the scapula Acromion Deltoid tubercle of the scapular spine Spine of the scapula Supraspinous and infraspinous fossae The convex posterior surface of the scapula is unevenly divided by a thick projecting ridge of bone; spine of the scapula, into a small supraspinous fossa and a much larger infraspinous fossa. The spine continues laterally as the flat expanded acromion (G. akros, point), which forms the subcutaneous point of the shoulder and articulates with the acromial end of the clavicle. The deltoid tubercle of the scapular spine is the prominence indicating the medial point of attachment of the deltoid. The spine and acromion serve as levers for the attached muscles, particularly the trapezius. Anterior (Costal) surface of the scapula Subscapular fossa The concave costal surface of most of the scapula forms a large subscapular fossa. The broad bony surfaces of the three fossae provide attachments for fleshy muscles. Lateral surface of the scapula Coracoid process Fossa ovalis Glenoid cavity Superolaterally, the lateral surface of the scapula has a glenoid cavity (G. socket), which receives and articulates with the head of the humerus at the glenohumeral joint. The glenoid cavity is a shallow, concave, oval fossa (L. fossa ovalis), directed anterolaterally and slightly superiorly—that is considerably smaller than 7 Dr.Kaan Yücel http://yeditepeanatomy1.org Bones of the upper limb the ball (head of the humerus) for which it serves as a socket. The beak-like coracoid process (G. korakōdés, like a crow's beak) is superior to the glenoid cavity and projects anterolaterally. This process also resembles in size, shape, and direction a bent finger pointing to the shoulder. Figure 5. Scapula and the shoulder joint http://therapyworksltd.files.wordpress.com/2012/07/shoulder.jpg Figure 6. Scapula- costal surface, lateral view, and posterior surface http://conornordengren.com/2011/10/14/the-shoulder-girdle-part-1-bones-and-joints-2 CLINICAL ANATOMY Fractures of the Clavicle The clavicle is one of the most frequently fractured bones. Clavicular fractures are especially common in children and are often caused by an indirect force transmitted from an outstretched hand through the bones of the forearm and arm to the shoulder during a fall. A fracture may also result from a fall directly on the shoulder. The weakest part of the clavicle is the junction of its middle and lateral thirds. Fractures of the Scapula Fracture of the scapula is usually the result of severe trauma, as occurs in pedestrian-vehicle accidents. Usually there are also fractured ribs. Most fractures require little treatment because the scapula is covered on both sides by muscles. 8 http://www.youtube.com/yeditepeanatomy Dr.Kaan Yücel http://yeditepeanatomy1.org Bones of the upper limb 4. BONE OF THE ARM . 4.1. HUMERUS (ARM BONE) the largest bone in the upper limb The skeletal support for the arm is the humerus. The humerus (arm bone) articulates with the scapula at the glenohumeral joint and the radius and ulna at the elbow joint. In cross-section, the shaft of the humerus is somewhat triangular with: anterior, lateral, and medial borders anterolateral, anteromedial, and posterior surfaces Intermuscular septa, which separate the anterior compartment from the posterior compartment, attach to the medial and lateral borders. Proximal end of the humerus Anatomical neck of the humerus Greater & lesser tubercles Head of the humerus Intertubercular (bicipital) groove Surgical neck of the humerus The proximal end of the humerus has a head, surgical and anatomical necks, and greater and lesser tubercles. The spherical head of the humerus articulates with the glenoid cavity of the scapula. The anatomical neck of the humerus is formed by the groove circumscribing the head and separating it from the greater and lesser tubercles. It indicates the line of attachment of the glenohumeral joint capsule. The surgical neck of the humerus, a common site of fracture, is the narrow part distal to the head and tubercles. The junction of the head and neck with the shaft of the humerus is indicated by the greater and lesser tubercles, which provide attachment and leverage to some scapulohumeral muscles. The greater tubercle is at the lateral margin of the humerus, whereas the lesser tubercle projects anteriorly from the bone. The intertubercular (bicipital) groove separates the tubercles. Shaft of the humerus Deltoid tuberosity Medial and lateral supraepicondylar (supracondylar) ridges Radial groove The shaft of the humerus has two prominent features: the deltoid tuberosity laterally, for attachment of the deltoid muscle, and the oblique radial groove (groove for radial nerve, spiral groove) posteriorly. 9 Dr.Kaan Yücel http://yeditepeanatomy1.org Bones of the upper limb Distally, the bone becomes flattened, and the medial and lateral borders expand inferiorly as the lateral supraepicondylar ridge (lateral supracondylar ridge) and the medial supraepicondylar ridge (medial supracondylar ridge). The lateral supraepicondylar ridge is more pronounced than the medial and is roughened for the attachment of muscles found in the posterior compartment of the forearm. Distal end of the humerus Condyle of the humerus; Trochlea+Capitulum Coronoid fossa Medial and lateral epicondyles Olecranon fossa The distal end of the humerus has a condyle, two epicondyles, and three fossae: Condyle The two articular parts of the condyle, the capitulum and the trochlea, articulate with the two bones of the forearm. Capitulum (L. little head) articulates with the radius of the forearm. Lateral in position and hemispherical in shape, is not visible when the humerus is viewed from the posterior aspect. Trochlea (L. pulley) articulates with the ulna of the forearm. It is pulley shaped and lies medial to the capitulum. Its medial edge is more pronounced than its lateral edge and, unlike the capitulum, it extends onto the posterior surface of the bone. Epicondyles The two epicondyles lie adjacent, and somewhat superior, to the trochlea and capitulum. The medial epicondyle, a large bony protuberance, is the major palpable landmark on the medial side of the elbow, and projects medially from the distal end of the humerus. It is the attachment site for the muscles of the anterior (flexor) compartment of the forearm. The lateral epicondyle is much less pronounced than the medial epicondyle. It is lateral to the capitulum and the attachment site for the muscles of the posterior (extensor) compartment of the forearm. Fossae Coronoid fossa adjacent to the radial fossa superior to the trochlea. It receives the coronoid process of the ulna during full flexion of the elbow. Olecranon fossa largest fossa, immediately superior to the trochlea on the posterior surface of the distal end of the humerus. It accommodates the olecranon of the ulna during full extension of the elbow. Radial fossa a shallow fossa immediately superior to the capitulum on the anterior surface of the humerus. It accommodates the edge of the head of the radius when the forearm is fully flexed. 10 http://www.youtube.com/yeditepeanatomy Dr.Kaan Yücel http://yeditepeanatomy1.org Bones of the upper limb CLINICAL ANATOMY Fractures of the humerus Most injuries of the proximal end of the humerus are fractures of the surgical neck. These injuries are especially common in elderly people with osteoporosis. The injuries usually result from a minor fall on the hand, with the force being transmitted up the forearm bones of the extended limb. Figure 7. Humerus Figure 8. Distal end of the humerus http://www.edoctoronline.com/medical-atlas.asp?c=4&id=22082 http://www.medpreponline.com/2009/06/supracondylar-fractures-of-humerus-in.html 5. BONES OF THE FOREARM The two forearm bones serve together to form the second unit of an articulated mobile strut (the first unit being the humerus), with a mobile base formed by the shoulder, that positions the hand. However, because this unit is formed by two parallel bones, one of which (the radius) can pivot about the other (the ulna), supination and pronation are possible. This makes it possible to rotate the hand when the elbow is flexed. 5.1. ULNA medial and longer of the two forearm bones The ulna is the stabilizing bone of the forearm. Proximal end of the ulna Coronoid process Olecranon 11 Dr.Kaan Yücel http://yeditepeanatomy1.org Bones of the upper limb Radial notch Trochlear notch (Semilunar notch) Tuberosity of the ulna The proximal end of the ulna is larger than the proximal end of the radius. This end is specialized for articulation with the humerus proximally and the head of the radius laterally. For articulation with the humerus, the ulna has two prominent projections: 1) Olecranon projects proximally from its posterior aspect (forming the tip of the elbow) and serves as a short lever for extension of the elbow. 2) Coronoid process projects anteriorly. Its superolateral surface is articular and participates, with the olecranon, in forming the trochlear notch. The lateral surface is marked by a smooth rounded cavity; radial notch for articulation with the head of the radius. Inferior to the coronoid process is the tuberosity of the ulna. The olecranon and coronoid processes form the walls of the trochlear notch (semilunar notch). The trochlear in profile resembles the jaws of a Crescent wrench as it “grips” (articulates with) the trochlea of the humerus. Shaft of the ulna Supinator crest Supinator fossa The shaft of the ulna is broad superiorly where it is continuous with the large proximal end and narrow distally to form a small distal head. The shaft of the ulna is triangular in cross-section and has: three borders (anterior, posterior, and interosseous) three surfaces (anterior, posterior, and medial). The anterior border is smooth and rounded. The posterior border is sharp and palpable along its entire length. The interosseous border is also sharp and is the attachment site for the interosseous membrane, which joins the ulna to the radius. Inferior to the radial notch on the lateral surface of the ulnar shaft is a prominent ridge, the supinator crest. On the lateral surface of proximal end of ulna, just below the radial notch is a concavity, the supinator fossa. Distal end of the ulna Head of the ulna Ulnar styloid process At the narrow distal end of the ulna is a small but abrupt enlargement, the disc-like head of the ulna with a small, conical ulnar styloid process. The ulna does not reach—and therefore does not participate in—the wrist (radiocarpal) joint. 12 http://www.youtube.com/yeditepeanatomy Dr.Kaan Yücel http://yeditepeanatomy1.org Bones of the upper limb 5.2.RADIUS lateral and shorter of the two forearm bones Proximal end of the radius A short head Neck Radial tuberosity Head of the radius Proximally, the smooth superior aspect of the discoid head of the radius is concave for articulation with the capitulum of the humerus during flexion and extension of the elbow joint. The head also articulates peripherally with the radial notch of the ulna; thus the head is covered with articular cartilage. Neck of the radius The neck of the radius is a constriction distal to the head. The oval radial tuberosity is distal to the medial part of the neck and demarcates the proximal end (head and neck) of the radius from the shaft. The radial tuberosity is medially directed. Shaft of the radius Oblique line of the radius The shaft of the radius, in contrast to that of the ulna, gradually enlarges as it passes distally. Throughout most of its length, like the ulna, the shaft of the radius is triangular in cross-section, with: three borders (anterior, posterior, and interosseous) three surfaces (anterior, posterior, and lateral). The anterior border begins on the medial side of the bone as a continuation of the radial tuberosity. In the superior third of the bone, it crosses the shaft diagonally, from medial to lateral, as the oblique line of the radius. The posterior border is distinct only in the middle third of the bone. The interosseous border is sharp and is the attachment site for the interosseous membrane, which links the radius to the ulna. Distal end of the radius Dorsal tubercle of the radius Radial styloid process Ulnar notch The medial aspect of the distal end of the radius forms a concavity, the ulnar notch, which accommodates the head of the ulna. Its lateral aspect becomes increasingly ridge-like, terminating distally in the radial styloid process. The radial styloid process is larger than the ulnar styloid process and extends farther distally. This relationship is of clinical importance when the ulna and/or the radius is fractured. 13 Dr.Kaan Yücel http://yeditepeanatomy1.org Bones of the upper limb Projecting dorsally, the dorsal tubercle of the radius lies between otherwise shallow grooves for the passage of the tendons of forearm muscles. The distal end of the bone is marked by two facets for articulation with two carpal bones (the scaphoid and lunate). Figures 9 & 10. Radius & Ulna http://www.bcnlp.ac.th/Anatomy/page/apichat/bone/page/ulna.html http://www.daviddarling.info/images/radius_and_ulna.jpg CLINICAL ANATOMY Fractures of the Radius and Ulna Fractures of both the radius and the ulna are usually the result of severe injury. A direct injury usually produces transverse fractures at the same level, usually in the middle third of the bones. Isolated fractures of the radius or ulna also occur. Because the shafts of these bones are firmly bound together by the interosseous membrane, a fracture of one bone is likely to be associated with dislocation of the nearest joint. Fracture of the distal end of the radius is a common fracture in adults > 50 years of age and occurs more frequently in women because their bones are more commonly weakened by osteoporosis. A complete transverse fracture of the distal 2 cm of the radius, called a Colles’ fracture, is the most common fracture of the forearm. The distal fragment is displaced dorsally and is often comminuted (broken into pieces). The fracture usually occurs as the result of trying to ease a fall by outstretching the upper limb. The force drives the distal fragment posteriorly and superiorly, and the distal articular surface is inclined posteriorly. This posterior displacement produces a posterior bump, sometimes referred to as the “dinner-fork deformity” because the forearm and wrist resemble the shape of a fork. Fractures of the olecranon process can result from a fall on the flexed elbow or from a direct blow. 14 http://www.youtube.com/yeditepeanatomy Dr.Kaan Yücel http://yeditepeanatomy1.org Bones of the upper limb Olecranon Bursitis A small subcutaneous bursa is present over the olecranon process of the ulna, and repeated trauma often produces chronic bursitis. 6. BONES OF THE HAND The hand is the region of the upper limb distal to the wrist joint. It is subdivided into three parts: wrist (carpus); metacarpus; digits (five fingers including the thumb). Carpal bones The wrist, or carpus, is composed of eight carpal bones (carpals) arranged in proximal and distal rows of four. These small bones give flexibility to the wrist. The carpus is markedly convex from side to side posteriorly and concave anteriorly. Augmenting movement at the wrist joint, the two rows of carpals glide on each other; in addition, each bone glides on those adjacent to it. From lateral to medial, the four bones in the proximal row of carpals • Scaphoid (G. skaphé, skiff, boat): a boat-shaped bone that articulates proximally with the radius and has a prominent scaphoid tubercle; it is the largest bone in the proximal row of carpals. • Lunate (L. luna, moon): a crescent (or moon) -shaped bone between the scaphoid and the triquetral bones; it articulates proximally with the radius and is broader anteriorly than posteriorly. • Triquetrum (L. triquetrus, three-cornered): a pyramidal bone on the medial side of the carpus; it articulates proximally with the articular disc of the distal radio-ulnar joint. • Pisiform (L. pisum, pea): a small, pea-shaped bone that lies on the palmar surface of the triquetrum. From lateral to medial, the four bones in the distal row of carpals • Trapezium (G. trapeze, table): a four-sided bone on the lateral side of the carpus; it articulates with the 1st and 2nd metacarpals, scaphoid, and trapezoid bones. • Trapezoid: a wedge-shaped bone that resembles the trapezium; it articulates with the 2nd metacarpal, trapezium, capitate, and scaphoid bones. • Capitate (L. caput, head): a head-shaped bone with a rounded extremity and the largest bone in the carpus; it articulates primarily with the 3rd metacarpal distally and with the trapezoid, scaphoid, lunate, and hamate. • Hamate (L. hamulus, a little hook): a wedge-shaped bone on the medial side of the hand; it articulates with the 4th and 5th metacarpal, capitate, and triquetral bones; it has a distinctive hooked process, the hook 15 Dr.Kaan Yücel http://yeditepeanatomy1.org Bones of the upper limb of the hamate, that extends anteriorly. Carpal arch The carpal bones do not lie in a flat plane; rather, they form an arch, whose base is directed anteriorly. The lateral side of this base is formed by the tubercles of the scaphoid and trapezium. The medial side is formed by the pisiform and the hook of hamate. Figure 11. Carpal bones http://www.daviddarling.info/encyclopedia/C/carpal.html The proximal surfaces of the distal row of carpals articulate with the proximal row of carpals, and their distal surfaces articulate with the metacarpals. Metacarpus The metacarpus forms the skeleton of the palm of the hand between the carpus and the phalanges. It is composed of five metacarpal bones (metacarpals). Each metacarpal consists of a base, shaft, and head. The proximal bases of the metacarpals articulate with the carpal bones, and the distal heads of the metacarpals articulate with the proximal phalanges and form the knuckles. The 1st metacarpal (of the thumb) is the thickest and shortest of these bones. Phalanges Each digit has three phalanges except for the first (the thumb), which has only two; however, the phalanges of the first digit are stouter than those in the other fingers. Each phalanx has a base proximally, a shaft (body), and a head distally. The proximal phalanges are the largest, the middle ones are intermediate in size, and the distal ones are the smallest. 16 http://www.youtube.com/yeditepeanatomy Dr.Kaan Yücel http://yeditepeanatomy1.org Figure 12. Anatomy of the hand Figure http://www.yalemedicalgroup.org/stw/images/125411.jpg Bones of the upper limb Figure 13. Bones of the hand http://www.daviddarling.info/encyclopedia/P/phalange.html CLINICAL ANATOMY Injuries to the Bones of the Hand The scaphoid is the most frequently fractured carpal bone. It often results from a fall on the palm when the hand is abducted, the fracture occurring across the narrow part of the scaphoid. Dislocation of the lunate bone occasionally occurs in young adults who fall on the outstretched hand in a way that causes hyperextension of the wrist joint. Fractures of the metacarpal bones can occur as a result of direct violence, such as the clenched fist striking a hard object. The fracture always angulates dorsally. The “boxer’s fracture” commonly produces an oblique fracture of the neck of the fifth and sometimes the fourth metacarpal bones. Fractures of the phalanges are common and usually follow direct injury. 17