D- Project Protocol APR13
advertisement

WHO-HPH Recognition Project
WHO-HPH PROJECT:
EFFECT OF A RECOGNITION PROCESS – A MULTI-CENTRE RCT
PROJECT PROTOCOL
Principal Investigator
Professor Hanne Tonnesen, WHO-CC Copenhagen
PHD Student
Jeff Kirk Svane
Scientific Supervisors
Professor Hanne Tonnesen, WHO-CC Copenhagen
Associated Professor Shu-Ti Chiou, National Yan-Ming University, Taipei
Participants
Clinical Hospital Departments from Taiwan, the Czech Republic, Thailand, Slovenia,
Canada, Indonesia, Estonia, Malaysia, Norway, South Korea (and more to come).
1
WHO-HPH Recognition Project
Aim
The aim for this research project is to evaluate whether a Recognition Process (that
supports implementation of health promotion in hospitals) generates better health gains
for patients and staff
Background
Clinical health promotion is a patient-centred approach in healthcare services, where
adding health promotion to the traditional clinical pathway would improves the effect of
treatment results and contributes to improved patient safety.(1;2) For example,
introducing health promotion interventions such as an intensive smoking cessation
intervention before surgery reduces the postoperative complications.(3-5)
According to the World Health Organization (WHO), health promotion represents key
dimension of quality in hospitals, along with clinical effectiveness and patient safety.(6)
Conventionally, activities on quality management in hospitals are involving planning,
implementation, evaluation, and continuous improvement of all clinical and non-clinical
activities. The WHO clinical health promotion standards would fit into these activities by
helping hospital management and staff members to assess and improve the quality of
health care and thereby again better health for patients, staff, and community.(7;8)
In essence, health promotion is considered as part of nearly all quality standards on
hospitals, however still mainly in implicit way. Moreover, assessing hospitals
departments’ performance in relation to the implementation of health promotion
activities and standards is still a novel area. For these reasons, a new recognition
process has been proposed, where this process would utilize set of WHO-HPH tools
and standards that tackle clinical health promotion activities in explicit forms.
Additionally, this process would be useful in documenting hospital departments’ quality
of care and evaluating their policies in relation to clinical health promotion activities,
while providing the best platform for making strategies on implementation of HP in
hospitals for better patients and staff health gains.
2
WHO-HPH Recognition Project
Nevertheless, the literature on Randomised Clinical Trials (RCT) studies concerning
accreditation and quality improvement recognition processes is limited. Example on the
rare literature concerning accreditation by using a RCT design is one important study
that had done to evaluate impact of hospital accreditation on the quality of care at the
national level in South Africa. (9) So, this study would be an additive value into the
existing literature.
The study would be randomised clinical trial concerned with effectiveness of the
proposed recognition process.
Main hypotheses:
The aim for this WHO-HPH research project is to evaluate whether A Recognition
Process to support implementation of healthcare promotion in hospitals and health
services generates better health gains for patients and staff.
The study hypothesis is
I.
Hospitals departments that are allocated to the WHO-HPH Recognition Process
would after one year:
a. Improve health gains for their patients and staff
b. Deliver more health promotion services
compared to the departments allocated to the control group and continue with
their routine clinical practice.
Study outcome measurements
Frequency of health promotion services delivered on smoking, excessive alcohol use,
overweight, mal-nutrition, and physical activity to smoking, excessive drinking,
overweight, malnourished, and physical inactive patients. These services concern
clinical health promotion activities, like motivational counselling and brief interventions,
as well as intervention, rehabilitation and after treatment.
Physical, mental, and social health status among patients and staff will be measured by
short form (SF36). (10)
3
WHO-HPH Recognition Project
Design
An RCT with hospital departments allocated to one of the two groups
Undergo the Recognition Process immediately = Intervention group
Continue their usual routine = Control group
Then, after one year, the Control group begins the recognition process (= delayed start),
while the Intervention group (=immediate-start) continues with the recognition process.
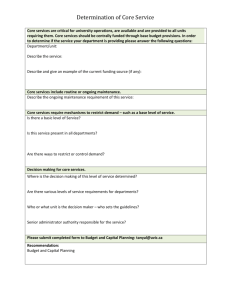
Trial Profile
(RP) = Recognition Process
Clin Dept
n = 2x44
RP
R
Intervention
Data collect
Control
TAU
RP
Intervention
Data collect
1y
Control
Data collect
Site Visit & Data Val
2y
Control
Data collect
Site Visit & Data Val
4
WHO-HPH Recognition Project
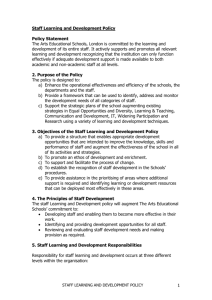
Whole Project Time Line
Settings
The study aim is to recruit hospitals in Taiwan, the Czech Republic, Thailand, Slovenia,
Canada, Indonesia, Estonia, Malaysia, Norway, South Korea (and more to come).
Randomisation and allocation of intervention (WHO-HPH recognition process)
1. The randomisation process is computerised using blocks of unknown sizes, and
stratification for each participating country. The randomisation process is
performed by an independent researcher who is not otherwise involved with the
research project.
2. Blinding: the statistical analyses would be done by an independent researcher.
Materials
88 clinical hospital departments (2 X 44) are recruited from national/regional the HPH
networks. The number is based on the power calculation below.
5
WHO-HPH Recognition Project
Inclusion criteria: All kinds of clinical hospital departments are eligible; from university as
well as non-university clinical hospital departments
Exclusion criteria: palliative care departments, paediatric departments, nursing homes,
non-hospital departments, and primary care facilities would be excluded, as the WHOHPH standards and tools are not validated for these clinical activities.
Sample size
We assume that the minimum relevant differences in deliveries of health
promotion services is 30 % (δ=0.3) between the intervention and control groups.
Additionally, we assumed that frequency of health promotion deliveries is 40%
(control departments π2=0.4) based on the literature, thereby the expected outcome
is 70 % (intervention departments π1= 0.7).
Accordingly, we would need around 40 departments in each arm considering
80% power, and 5% two-sided significance. Considering the possible drop outs of
10% over the whole study, the required sample size in each study arm is 44
departments.
Formula for calculating the sample size:
n > {(1(1- 1) + 2(1- 2))(Z + Z)2} /2
1 2
Methods
WHO-CC, Bispebjerg University Hospital will be responsible for running the Recognition
Project in collaboration with the participating National / Regional HPH Coordinators,
Hospital/HS Management, Heads of Department and local HPH Coordinators. It is
understood that the project administration should be simple, transparent and smooth.
Moreover, the project would be under the oversight of WHO Europe Regional Office in
Copenhagen.
The manual for the Recognition Process is based on the WHO Standards for HP in
Hospitals, the indicators from the HPH DATA Model, the Documentation Model for HPH
Activities and the indicators given in the SAT Tooli. The manual includes forms for the
internal audit of medical records, for the surveys aimed at staff and patients. In addition
6
WHO-HPH Recognition Project
a standardised index score (%) of fulfilment of WHO-HPH standards and related
measurable elements is included in the manual. These scores are categorised
according to the table below:
1-25%
26-50% 51-70% 71-80% 81-90%
91-100%
Basic
light
level
green
green
bronze
silver
gold
ooooo
ooooo
ooooo
ooooo
ooooo
ooooo
Inclusion, Agreement & Allocation
H/HS Management, Head of Dept, N/R and H/HS Coordinators sign the agreement for
participation. Then the randomisation takes place, and the participants are allocated to
either
The intervention group with immediate start of the Recognition Process or
The control group, which continues the routines as usual, and start the
Recognition Process only after one year.
The baseline package
This is sent to start the Recognition Process; i.e. immediately to the Intervention Group
and delayed one year for the control group. It includes a printed copy of the signed
agreement and contact information as well as:
A CD Rom with the project description, Action plan and Time schedule tailored
for the participating department. Also included is the Manual (a written form and
a video) and material for collection of data,
o Case report files (CRF) to collect the documentation to be delivered in
copies, Forms to be used for the internal Medical Records Audit, and the
Patient and Staff Surveys.
The CD ROM also contents inspiration material for making a Quality Plan related
to the results of the data collection
7
WHO-HPH Recognition Project
Data collection and Quality Plan
The participating department collects the data based on:
A) Copies of Policies, Guidelines, and Programs etc (translated into English) signed
by Head of Dept, H/HS Coordinator and N/R Coordinator - according to the “Data
Form”
B) Internal Audit of 50 consecutive medical records (from the month prior to
inclusion) – according to the “MR Audit Form”
C) Survey for patients and staff – according to the “SF-36 + Additional forms”
Using the baseline results a Quality Plan including clear Milestones, Action plan and
Time line is developed for implementation during the following period of 12 months. The
Hospital/HS Management, the Head of Department as well as the N/R and H/HS
Coordinators sign the plan – according to the “Manual”.
Returning Baseline Package
All collected data and the Quality Plan are sent to WHO-CC in Copenhagen.
Implementation of Quality Plan
The participating department implements the Quality Plan over the next 12 months
according to the Milestones, Action plan and Time line. Minor adjustments are often
necessary according to changes in hospital structure, patient groups, staff etc in order
to reach the Milestones.
Follow-up Package for Data collection
This is sent to follow-up 1 year after the start of the Recognition Process. It includes a
CD ROM with similar data collection material as the Baseline package.
Data collection: Internal MR Audit and Revised Quality Plan
The data collection procedures are also similar to the procedures at the baseline.
Using the follow-up results a Revised Quality Plan including new clear Milestones,
Action plan and Time line is developed for implementation in the next 12 months period.
8
WHO-HPH Recognition Project
The Hospital/HS Management, the Head of Department as well as the N/R and H/HS
Coordinators sign the plan – according to the “Manual”.
All collected data and the Revised Quality Plan are sent to WHO-CC in Copenhagen.
Data Validation: Site visit
The Recognition Process ends with a site visit that takes place only after receiving all
materials at the WHO-CC in Copenhagen. The visit is expected to confirm the data from
internal MR audit and surveys results collected at the follow-up after one year.
Interviews of staff and patients, and an external audit of 50 randomly selected medical
records are included in the site visit.
Certificate with results
Delivery of Recognition Process Certificate showing the results of the participating
department
Recruitment
Each hospital can recruit only one clinical department to participate in this WHO-HPH
research project.
However, a major hospital or health service that consists of different geographic sites
(e.g. hospitals or clinics) that are clearly separated regarding management of
department, other staff, patients groups, scope of activities, and provided treatment can
recruit more than one department after agreement with the WHO-CC in Copenhagen.
Data and Statistical Methods
Frequency of health promotion services delivered is compared between the two groups
by Fischers’ Exact Test.
Physical, mental, and social health status are scored using the SF-36 and compared
with the Mann-Whitney Test between the two groups.
All analyses would be done on an intention to treat principle. An external researcher
blinded for group allocation would do the analyses on anonymourised data using
9
WHO-HPH Recognition Project
relevant statistical software such as SAS and STATA 11.
Hospital department data would be anonymourised, entered and stored in a predesigned database dedicated for this project proposal. A list of codes for the individual
department will be kept separated from the database (and under lock). Only the
research team would use the database in connection with the collection of the baseline,
follow-up and external survey data from the participating departments.
Ethical considerations
Ethical evaluation would be obtained from the Scientific Ethical Committee in the Danish
Capital Region (International Studies) before the study implementation.
The WHO-HPH Standards and tools as well as the SF-36 Questionnaire to be used in
the Recognition Process project are scientifically validated in previous research projects
and the results are published.
Participation in the study will be approved before inclusion by the involved Hospital
Management, Head of Department, National/Regional HPH Coordinator, and the local
Hospital/HS Coordinator. Department data will be anonymourised and stored in secured
files with limited access and released to the research team only, in terms to guarantee
confidentiality and security. Data confidentiality procedures would be according to the
Danish Data protection agency guidelines.
The surveys among staff and patients will be carried out in accordance to the hospital
guidelines for this kind of surveys. Patient and staff data from are collected completely
anonymously.
Project Organisation and Economy
The project is organised with a research team from WHO-CC in Copenhagen,
International Supervisors, National/Regional and H/HS Coordinators from the HPH
Networks, Hospital Managements and Heads of participating departments.
10
WHO-HPH Recognition Project
The National/Regional Coordinators and the H/HS Coordinators are responsible for
supporting the project, while the Hospital Managements and Heads of Department are
responsible for driving the project processes, collecting the data and implementing the
quality plan. The participating clinical hospital departments and Networks secure their
own resources related to participating in the project.
The project is approved by the Copenhagen University as a part of the PHD study for
Jeff Kirk Svane, who is supervised by Professor Hanne Tønnesen and Professor Shu-Ti
Chiou.
The project is anchored in WHO-CC at Bispebjerg University Hospital and Health
Sciences under the Faculty of Medicine at Lund University, which also cover office
facilities etc. for the PHD student. The project is included in the Memorandum of
Understanding between WHO and HPH and explicitly included in the related Action
Plan.
Authorships and Dissemination of Results
The WHO-CC research team in Copenhagen informs the participating departments and
others involved in the project about the study results as soon as possible after ending it.
The main results will be included in the PHD of Jeff Kirk Svane, who will draft the main
paper(s) under supervision of Hanne Tønnesen and Shu-Ti Chiou.
Any authorship follows the Vancouver Criteria. While, maximum one active person from
each N/R Network would be co-author in the published paper/s on this research project,
the active others would be acknowledged.
The results will be disseminated in clinical, scientific and public forums and media
including the WHO and HPH Network websites, as well as in other relevant forums.
Publication of the research results in International scientific journals would be done
according to CONSORT guidelines for RCT.
11
WHO-HPH Recognition Project
Reference List
(1) Oppedal K, Nesvåg S, Pedersen B, Skjøtskift S, Aarstad AKH, Ullaland S, et al.
Health and the need for health promotion in hospital patients. Eur J of Pub Health
2010.
(2) Groene O, Jorgensen SJ. Health promotion in hospitals-a strategy to improve
quality in health care. The Eur J of Pub Health 2005;15:6-8.
(3) Møller AM, Villebro N, Pedersen T, Tønnesen H. Effect of preoperative smoking
intervention on postoperative complications: a randomised clinical trial. Lancet
2002;359:114-7.
(4) Tonnesen H, Nielsen PR, Lauritzen JB, Moller AM. Smoking and alcohol
intervention before surgery: evidence for best practice. B J of Anaesth
2009;102:297-306.
(5) Nasell H, Adami J, Samnegard E, Tønnesen H, Ponzer S. Effect of Smoking
Cessation Intervention on Results of Acute Fracture Surgery: A Randomized
Controlled Trial. J Bone and Joint Surg 2010;92:1335-42.
(6) Standards for health promotion in hospitals: development of indicators for a selfassessment tool, WHO/Europe 2004. World Health Organization Regional Office
for Europe 2004
(7) Groene O, Jorgensen SJ, Fugleholm AM, Garcia Barbero M. Standards for health
promotion in hospitals: development and pilot test in nine European countries. Int J
Health Care Qual Assur Inc Leadersh Health Serv 2005;18:300-7.
(8) øvretveit J, Gustafson D. Using research to inform quality programmes. BMJ
2003;326:759-61.
(9) Salmon JW, Heavens J, Lombard C, Tavrow P. The impact of accreditation on the
quality of hospital care: KwaZulu-Natal Province, Republic of South Africa.
Operations Research Results 2003;2:17.
(10) McHorney, Colleen A.; Ware, John E.; Raczek, Anastasia E. The MOS 36-Item
Short-Form Health Survey (SF-36): II. Psychometric and clinical tests of validity in
measuring physical and mental health constructs. Med Care 1993; 31: 247-263
12
WHO-HPH Recognition Project
13