RecInMichChap15 - Michigan State University
advertisement

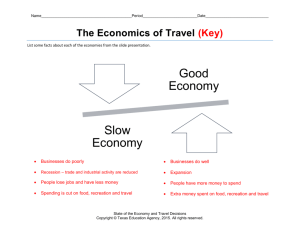
15 Therapeutic Recreation Jean Folkerth Richard Paulsen Robert Frost Handicapper fishing site with “balconies” for wheelchairs, St. Clair County. (Photo courtesy of Theodore Haskell.) Therapeutic Recreation is considered an emerging profession in health care settings. Because of the Americans with Disabilities Act (ADA), the need for persons with degrees in therapeutic recreation to provide recreation or recreation consultation for persons with disabilities is growing. The two national professional membership organizations offer similar, but different definitions of therapeutic recreation (TR). According to the National Therapeutic Recreation Society (NTRS) therapeutic recreation is: 143 Practiced in clinical, residential, and community settings, the profession of therapeutic recreation uses treatment, education, and recreation services to help people with illnesses, disabilities, and other conditions to develop and use their leisure in ways that enhance their health, independence, and well-being (National Therapeutic Recreation Society, 1994). The American Therapeutic Recreation Association (ATRA) offers the following definition of therapeutic recreation: Therapeutic Recreation is the provision of Treatment Services and the provision of Recreation Services to persons with illness or disabling conditions. The primary purpose of Treatment Services, which are often referred to as Recreation Therapy, is to restore, remediate or rehabilitate to improve functioning and independence as well as reduce or eliminate the effects of illness or disability. The primary purpose of Recreation Services is to provide recreation resources and opportunities in order to improve health and well-being. Therapeutic Recreation is provided by professionals who are trained and certified, registered or licensed to provide Therapeutic Recreation (American Therapeutic Recreation Association, 1987). Within the field, therapeutic recreation is practiced differently dependent on the population, setting, philosophy of the agency and reimbursement. It is expected that therapeutic recreation services are delivered by persons whose minimal qualifications are that the person has a degree in therapeutic recreation and/or is certified by the National Council for Therapeutic Recreation Certification. The person so certified is a Certified Therapeutic Recreation Specialist (CTRS). How the Field Developed in Michigan The history of therapeutic recreation in the State of Michigan does not reach as far back as most of the other areas of recreation service, but in it’s comparatively short lifeline, therapeutic recreation has taken a “fast-track” in emerging as a reputable health service provider. Therapeutic recreation’s early roots can be traced to our state institutions for persons with emotional and mental impairments. In the late 1940s, state facilities, like Traverse City, Oak-dale, and Kalamazoo Hospitals, began to shift services from custodial to more active forms of care, including activity programs. After World War II, the Veterans Administration Hospitals also introduced “medical recreation~~ services aimed at improving the social and emotional adjustment of their new resident clients. In the 1950s, recreation services people appeared in large private psychiatric facilities, like University of Michigan Hospital and Pine Rest Hospital in Grand Rapids. These early forerunners of therapeutic recreation were called Activity Therapists. During this decade, the value of recreation services was also recognized in expanded programs within prison settings and community centers. The growth of recreation for persons with special needs resulted in the first state conference in 1957, the Michigan Activity Therapy Conference. The 1960s and 1970s were a boom era for therapeutic recreation. The creation of enabling legislation, the “deinstitutionalization” of state facilities, the advent of professional curricula and the foundations of professional organizations all paved the way for the profession of therapeutic recreation to blossom. In 1963, federal legislation created Community Mental Health services. This led directly to the shifting of services from Michigan’s state hospitals to the providing of community-based services for persons with emotional or mental impairments. These outpatient or day treatment programs featured recreation as a key component of their services. Programs and facilities emerged with recreation for special populations as their main focus, including specialty camps like Indian Trails (physical impairments) and Teushmaheta (visual impairments) in West Michigan, being prime examples. In 1968, the Michigan Special Olympics was inaugurated. Accessibility and “least restrictive environment” were legislative concepts that pushed recreation into community settings. In the mid-1970s, the Tri-City Therapeutic Recreation Program was launched. This program focused on serving the special population community of Wayne, Westland, and Garden City. This was the first of many Michigan communities to provide special recreation programs within the traditional parks and recreation departments. In 1974, under a federal grant from the Bureau of Education for the Handicapped, the first Michigan professional therapeutic recreation curriculum was established at Michigan State University. It was around this time that the body of knowledge in therapeutic recreation began to take form in textbooks and professional journals, like the Therapeutic Recreation Journal. By the late 1970s, therapeutic recreation had become an established branch of the main state recreation organization, Michigan Recreation and Park Association (MRPA). As much as the time frame of the 1960s through the 1970s was that of foundation building, the time frame of the 1980s to the mid-1990s can be characterized as that of creating professional depth and definition for therapeutic recreation. Early in the 1980s the National Council for Therapeutic Recreation Certification (NCTRC) assumed responsibility for the certification and recertification of therapeutic recreation professionals. The research and development of this organization led to the first national certifying exam being administered in 1990. In 1984 numerous therapeutic recreation practitioners created a second organization to service the profession, the American Therapeutic Recreation Association (ATRA). A Michigan chapter of ATRA was created in the early 1990s. The professional organizations in this time frame worked to legitimize the role of therapeutic recreation in health care services. They created standards of practice, codes of ethics, and an enhanced body of knowledge via research and publications. The practice of therapeutic recreation responded to shifts in health service delivery by programming for shorter hospital stays in clinical settings. The shift away from hospitals also created the need for therapeutic recreation services to assist in the transition back to life in the community for special populations. Therapeutic recreation programs in the areas of return to work, community reintegration, and partial hospitalization are examples of this trend. The last decade (1980s) has seen the number of certified therapeutic recreation specialists double to almost 700 in the mid-1990s in the State of Michigan. The expansion of the field in the 1980s is also seen by the creation of seven colleges or universities providing academic preparation in therapeutic recreation. The professional organizations representing therapeutic recreation in the State of Michigan now number seven and annually offer over 70 different workshops or conferences. The history of therapeutic recreation in the State of Michigan is really rather remarkable given its late inception. Therapeutic recreation has emerged from a diversionary service within custodial care to a frontrunner in today’s changing health services. With a projected growth rate of 20% through the year 2000, therapeutic recreation will need to continue its rapid development for years to come. 144 Recreation in Michigan: Great Professional Opportunities Therapeutic Recreation in Clinical Health Care Due to the changing nature of the health care system in this country, the field of therapeutic recreation also has been going through changes. Agency accrediting bodies, such as the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) and the Commission on Accreditation of Rehabilitation Facilities (CARF), third party reimbursement companies and managed care providers, are demanding that the profession become more accountable for their outcomes. This will change the way therapeutic recreation professionals think about their responsibilities to their patients and how they perceive themselves. The profession has long believed that there is a process in the delivery of therapeutic recreation services. This process is what all recreation therapists do, regardless of the patient population. The process consists of assessment, planning, implementation and evaluation. Assessment is the first step in the process. It is, therefore a very crucial step. It is assessment that tells the recreational therapist7 (RT) how and at what level the patient is functioning. To do this effectively, the RT must assess the client in at least four behavioral domains: physical, social, emotional and cognitive. Since an RT’s expertise is in the area of recreation and leisure, it is generally accepted that the client also must be assessed in the areas of leisure attitudes, skills and knowledge. In many clinical settings the recreational therapy program is not being reimbursed by third party payers, thus some programs are not determining specific functional skills in relation to the four behavioral domains, but are using recreation and leisure assessments only. To assess a client, the RT may use a variety of assessment instruments or just one. Most agencies try to use a “commercial” assessment instrument that has had validity and reliability tests completed on it. These assessment instruments measure functional abilities, e.g., Leisure Competence Measure (LCM) or the Comprehensive Evaluation in Recreation Therapy (CERT), or they measure leisure attitudes and knowledge, e.g., Leisure Diagnostic Battery (LDB). To determine a person’s leisure interests and skill level, most agencies design their own assessment tool. While using the assessment instruments, the RT must utilize observation and communication skills to ensure that clients not only understand what is being asked of them but also begin to form a trusting relationship with the RT. At the completion of the assessment, the RT summarizes the assessment findings in relation to the client’s strengths, weaknesses and functional abilities. Planning is the second step in the therapeutic recreation process. Following the completion of a client’s assessment, the RT must write an individual treatment plan. According to ATRA’s Standards of Practice (1994) and NTRS’s Administrative Guidelines (1990), the treatment plan must include long and short term goals, behavioral objectives, intervention strategies, outcome evaluation procedures and discharge or transition plans (Carter, Van Andel & Robb, 1995). Within the planning phase, the RT is also considering all the information received from the treatment team and making treatment and program adjustments accordingly. In addition to writing treatment plans, the RT is responsible to ensure that the resources are available for the client’s treatment. Implementation is the third step in the therapeutic recreation process. It is within this step that the RT draws upon his/her leadership skills and any special knowledge that will enhance the client’s treatment. The RT’s listening and understanding skills are brought once more into 7 Recreational Therapist (RT) will be used in this section only since most persons working in therapeutic recreation in the clinical area are referred to as Recreational Therapists. Therapeutic Recreation 145 action to form a clinical bond with the client and encourage recovery. It is within this step that a thorough understanding of activity analysis and the adaptation of both activities and equipment is necessary. When implementing the client’s individual treatment plan, the RT must be aware of the client’s goals, any behavioral interventions required and the client’s actual behaviors during all the sessions. Depending on the agency, the RT will document treatment sessions and client behavior within those treatment sessions on a daily or weekly basis. Evaluation is the last step in the therapeutic recreation process. It is at this step that the RT collects data and develops a discharge plan for the client. It is now that the RT must report to the treatment team on the effectiveness of the treatment and whether the client improved his/her functioning by achieving the established outcome measures. The treatment team as a whole determines whether to revise, continue or discontinue treatment. Settings Health Care Services The therapeutic recreation process (see preceding section) is applied in a variety of health care settings, such as Sinai Hospital (rehabilitation), Stepping Stones Pediatric Center (children, outpatient, TBI), St. Joseph TBI Community Re-entry Program (adult, outpatient, TBI), and Chelsea Community Hospital (all disabilities). An illustrative case study of Chelsea Community Hospital is presented. Chelsea Community Hospital. Chelsea Community Hospital is a community owned, not-for-profit, acute care hospital in the Village of Chelsea. It provides services for persons in the Washtenaw County area and is a 113-bed facility. Chelsea Hospital offers recreational therapy services to patients in the psychiatric, rehabilitation, older adult, chemically-dependent, and head pain inpatient units and brain injured day treatment programs through both individual and group treatment. The RT (Recreation Therapy) department consists of a director, three full-time and two part-time CTRSs. Each therapist is primarily responsible for a specific unit but is able to work with patients from other units through programs that combine unit activities. The Mission of the Recreation Therapy department is to renew and discover one’s passion for life. Through education and experience we will provide an environment where patients, families, and community members feel safe and respected as they take risks to realize their talents, interests, and abilities. We believe that therapeutic leisure activities empower people to enrich their quality of life, instill self-respect and discover their potential to contribute to the well-being of themselves and others. We are committed to people living lives that they love (Chelsea RT Departmental Mission, 1994). ... Each year the department services over 11,000 persons through its inpatient and some specialized outpatient programs. Each unit offers a variety of programs dependent upon the needs of the clients and the skills of the therapists. There are a variety of interdisciplinary groups co-led by Recreational Therapists, Occupational Therapists, Speech Therapists, Social Workers and Nurses. Functional Living Skills, Tuesday Lunch Special, Assertiveness, Distress Tolerance, and Family Day are examples of these groups. The department also provides 146 Recreation in Michigan: Great Professional Opportunities therapy programs in the areas of sports/fitness, leisure education, and arts and expressive activities. To participate in RT, patients on the medical units and adolescents from the head pain units must have a referral from their doctor. The RT department also offers “combined” activities open to patients from all units in the evenings and weekends, rotating around activity themes based on social games, leisure education, horticulture, entertainment, crafts and pet therapy. Since Chelsea is a community hospital, some of its most innovative and exciting programs are the outreach programs that are available for persons in the community who have special needs. “Partners in Golf” is a golf workshop for the physically impaired which receives much attention every year. “Playing Through” is a drop-in golf league, which has the physically impaired and the able-bodied playing together. A different type of program is REConnection Day which offers a sampling of leisure activities adapted to meet the needs of persons with physical, mental or social challenges. The Traumatic Brain Injured Camp is an annual event and includes 15 campers who are survivors of traumatic head injuries. An interdisciplinary team, including physical, occupational, speech and recreational therapists, social workers and nurses, accompany the clients. It is a week-long residential program which allows the participants to re-engage in leisure activities and be with others who have sustained similar injuries. Thus, it can be seen that the Recreational Therapy Department at Chelsea Community Hospital offers a comprehensive program, which serves a variety of populations and provides a variety of inpatient and outpatient treatment and recreation programs. Special Recreation Services Therapeutic recreation also provides programming through community recreation. It differs from the health care settings by its application of the TR process. According to the 1990 United States Census, approximately 485,000 Michigan citizens with disabilities live, work and, recreate in their communities. Since the early 1970s, specialized units within local recreation and park departments have provided services that specifically address the leisure needs of people with disabilities. Non-profit advocacy and support organizations providing a variety of services to persons with specific disabilities and their families have included recreational programming in their offerings, particularly at the local level, since their inception. Examples of such organizations include: Association for Retarded Citizens, United Cerebral Palsy, and Little People of America. Special recreation services differ from therapeutic recreation services in that the focus is not on medical treatment. Kennedy, Smith and Austin (1991) describe special recreation as a leisure service that modifies equipment, environment, and access to enable persons with disabilities to participate in community-based leisure experiences. The term “special recreation” often is used in reference to the specialized nature of the assistance provided to enable participation. Support and Advocacy Organizations. Michigan is unique because organizations that support the needs of persons with disabilities do not typically provide services directly to their membership. Organizations, such as United Cerebral Palsy of Michigan and the Association for Retarded Citizens, focus their resources on advocacy, education and referral. Services such as day care, vocational training and recreation are accessed through existing community-based programs offered by churches, schools, municipalities and human services organizations. 148 Recreation in Michigan: Great Professional Opportunities Therapeutic Recreation 147 Community Services In Michigan, special recreation services have been provided through municipal government, county government, and non-profit support organizations. Examples of each class of special recreation service highlight the role of recreation, program offerings, and management. Sterling Heights. The City of Sterling Heights’ Special Recreation Program was the 1994 Special Recreation Award winner for cities under 200,000 in population. During its award winning year, 650 persons with special needs were provided opportunities to participate in 35 different activities. Professional leadership was used to plan and implement 386 sessions which served 10,753 participants. Programs were developed to provide the citizens of Sterling Heights a variety of leisure opportunities. Programs included: Super Saturday for the Artistic, Sports Night, Early Childhood Learning Program, Day Camp, Recreation Plus Club & POHI Teen Club, Wheelchair Tennis and Basketball, Dinners Club, Dance, Choral Group/Music Lessons and Travel Club. As a result, persons with mental, physical, auditory, and emotional impairments were provided with opportunities to actively participate in the life of the community throughout the year. The Sterling Heights Special Recreation Program is a unit within the Parks and Recreation Division of the Department of Community Services. Staffing throughout the year varies from 13 to 30 part-time/seasonal employees. Professional full-time staff includes the Program Coordinator and the program assistant. They function as a team to plan, manage, and supervise staff and programs. Oakland County Parks and Recreation. Oakland County employs a certified therapeutic recreation specialist (CTRS) to serve primarily as a consultant to constituent communities and to coordinate large events for persons with disabilities. Efforts by constituent communities to provide “inclusive” (the new term under ADA) recreation services are supported by the county consultant educating recreation leaders in appropriate modification techniques for persons with disabilities enrolled in their programs. During 1994 the county directly served constituents through coordinated events, enabling nearly 9,000 recreation participations by persons with disabilities. Programs include activities such as: cerebral palsy state games, disabled aerobics, recreation and respite, and wheelchair basketball. While one county therapeutic recreation specialist facilitates a variety of recreation services in the county, as in other public agencies, it should be recognized that volunteers play a significant role in providing leadership and assistance in the many programs offered throughout the year. Professional Organizations There are two national professional membership organizations with Michigan affiliates, as described in “How the Field Developed in Michigan.” The National Therapeutic Recreation Society (NTRS), a branch of the National Recreation and Park Association (NRPA), was founded in 1965. Its focus is on the provision of services in both health care and community settings. The American Therapeutic Recreation Association (ATRA) was founded in 1984. It is an independent organization with its primary focus being the delivery of therapeutic recreation services in health care settings. The profession also has an independent certifying agency, not a part of either professional organization. The National Council for Therapeutic Recreation Certification (NCTRC) was Therapeutic Recreation 147 formed in 1981 and is responsible for the management and administration of certification and recertification standards for therapeutic recreation personnel. In the State of Michigan most therapeutic recreation positions require that the person be certified by NCTRC. Most students who graduate from a therapeutic recreation program at a Michigan college or university will be eligible to take the certification examination, given twice a year. A person who has been awarded the credential is called a “Certified Therapeutic Recreation Specialist” (CTRS). Michigan, itself, has two statewide professional membership organizations and several regional organizations. The statewide professional organizations parallel the national membership organizations. The Therapeutic Recreation Committee is a committee of the Michigan Recreation and Park Association (MRPA). It works within the state to ensure recreation services are available for persons with disabilities. It also provides a TR Institute every June. The Michigan Therapeutic Recreation Association is a state affiliate of the ATRA. Its focus is primarily on needs of persons who work in health care settings. It provides a oneday workshop in the fall. The Activity Therapy Conference is a group of professionals from a variety of health care settings who sponsor a workshop every fall in therapeutic recreation. Its only purpose is the conference and, thus, is not considered a professional membership organization. There are also a variety of active local and regional groups in Michigan, such as the Metro-Detroit TR Association. These groups focus on local problems and needs and serve as an excellent networking opportunity. It is desirable for professionals to participate in both a national organization and its Michigan affiliate and a local or regional organization, if one is in the vicinity. Career Opportunities Therapeutic recreation has been described as one of the “hottest” professions of this decade (the 1990s). In fact, recreational therapy is identified as the 14th fastest growing profession requiring a bachelor’s degree. Nearly 33,000 therapeutic recreation specialists were employed in 1990. There is an expected 39% increase in employment opportunities through the year 2005 (Occupational Outlook Quarterly, Spring 1992). Therapeutic recreation specialists are employed in a variety of health care settings, such as physical rehabilitation hospitals, psychiatric treatment facilities, substance abuse treatment programs, and geriatric care programs. These provide opportunities for the therapeutic recreation specialist to work as a member of a medical treatment team. In many of these settings a therapeutic recreation specialist may work with inpatient units or outpatient services. There also are some positions in the community services settings with local government recreation departments, and limited positions with support and advocacy organizations. (See comments in next section.) Therapeutic recreation specialists working in entry level positions can expect to earn between $18,000—$24,000 per year (1995). This range is affected by geographical location and by the type of organization. Clinical rehabilitation services positions are at the high end of the salary range with geriatric services (nursing homes) positions at the lower end of the range. Community setting positions usually are mid-range. Therapeutic Recreation 149 Future Changes in the funding of health care and health care delivery will have a direct effect on the provision of therapeutic recreation services. If the profession is able to demonstrate effectiveness of care through patient outcomes and documentation of treatment practices, the resulting demonstration should legitimatize including therapeutic recreation services in various health care delivery systems. Community-based organizations, primarily local park and recreation departments, also hire therapeutic recreation specialists to manage special recreation services for their constituents. As a result of expectations placed on local park and recreation departments by the Americans with Disabilities Act (ADA), therapeutic recreation specialists also may be sought to fill general recreation leadership positions. The ADA with its philosophy of “inclusive services” is presenting new challenges to the provision of recreation services in Michigan communities. Including persons with disabilities in the activities of the community has always been part of therapeutic recreation. Renewed emphasis has been placed on the increased participation of persons with disabilities in non-special recreation programs in the regular ongoing programs. As a result, general recreation leaders need to develop attitudes, knowledge, and skills that will enable them adequately to serve any citizen who participates in an activity they offer. Notwithstanding, it is expected that Special Recreation Services will continue to be provided to meet affiliation, social, and skill development needs of persons with disabilities. References American Therapeutic Recreation Association (1987). Definition Statement. Hattiesburg, MS: American Therapeutic Recreation Association. American Therapeutic Recreation Association (1993). Standards for the Practice of Therapeutic Recreation and Self Assessment Guide. Hattiesburg, MS: American Therapeutic Recreation Association. Carter, M.J., G. Van Andel, & G. Robb (1995). Therapeutic Recreation: a Practical Approach. (2nd ed.) Prospect Heights, IL: Waveland Press. National Therapeutic Recreation Society (1994). Definition of Therapeutic Recreation. Arlington, VA: National Recreation and Park Association. National Therapeutic Recreation Society (1990). Guidelines for the Administration of Therapeutic Recreation Service. Alexandria, VA: National Recreation and Park Association. Recreation Therapy (1992). Occupational Outlook Quarterly. 150 Recreation in Michigan: Great Professional Opportunities