CRP 3 test line WB
advertisement

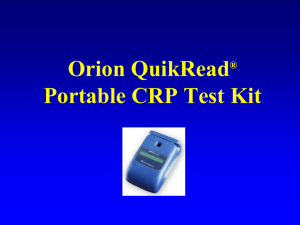
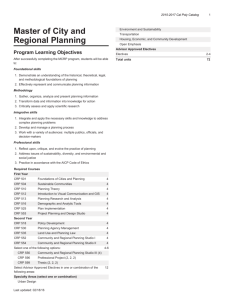
Rapid CRP Serum/Whole Blood Cassette Test INTRODUCTION The Rapid CRP Serum/Whole Blood Cassette Test is a colloidal gold/antibody complex based immunoassay designed for the semi-quantitative detection of human CRP in serum or whole blood. It is intended for professional use as indicator of inflammatory processes. Elevated levels of CRP are not specific to any one disease, but have been linked to a number of diseases, including: bacterial infections, rheumatoid arthritis, myocardial infarctions, and malignant tumors. Elevated levels of CRP are also a good indicator of future cardiac problems. During an inflammatory process the level of CRP rises dramatically. CRP concentration can rise from a basal level of 1 to 5 g/ml to 500 g/ml within hours of inflammation onset. Due to the large range over which CRP levels can vary, few semi-quantitative rapid CRP tests are currently available. PRINCIPLES OF THE PROCEDURE The Rapid CRP Serum/Whole Blood Cassette Test consists of a chromatographic absorbent device and a combination of polyclonal antibodies that selectively detect CRP in serum or whole blood samples and give semi-quantitative results. In ten minutes, levels of CRP in samples can be detected within the following ranges: <0.1 g/ml, 0.11.0 g/ml, 1.0-10 g/ml, and >10 g/ml. Serum or whole blood migrates through the absorbent area and along the test membrane. CRP present in the specimen is bound by antibody-dye conjugate forming antibodyantigen complex. The complex is captured by anti-CRP antibody immobilized in the three test zones (test line 1, test line 2, and test line 3) of the membrane forming pink-rose bands. The use of three test lines to yield semi-quantitative results is described further in the Result Interpretation section below. In the absence of CRP no lines will form in the three test zones. Dye conjugate is captured by the antibody immobilized in the control zone (control line) of the membrane, again producing a pink-rose band. A band at the control line shows that the test has worked correctly and results from the test lines should be considered valid. TEST STORAGE Store the test below 28C, do not freeze. Prior to use bring test and components to room temperature. WARNINGS AND PRECAUTIONS FOR USERS 1. Handling should preclude any pipetting by mouth. 2. Do not allow smoking or eating where specimens and reagents are being handled. 3. Wear disposable gloves while handling kit reagents or specimens. Wash hands thoroughly afterwards. 4. Avoid splashing or aerosol formation. 5. Clean up spills thoroughly using an appropriate intermediate-to-high level disinfectant. 6. Decontaminate and dispose of all specimens and potentially contaminated materials as if they were infectious. 7. Do not use reagents after the expiration date. 8 For in vitro diagnostic use only. Specimen Collection and Preparation Either whole blood, plasma or serum may be used as samples for this procedure. For the whole blood or plasma procedure, collect blood in a tube containing 5mM EDTA or 10mM citrate as the anticoagulant. If serum samples are to be used, collect blood in a tube without anticoagulant and allow to clot. Heat inactivation of samples may lead to hemolysis or protein denaturation and therefore should be avoided. MATERIALS PROVIDED 1. CRP Serum/Whole Blood cassettes MATERIALS REQUIRED BUT NOT SUPPLIED 1. Disposable droppers 2. Automatic pipettors 3. Microfuge tubes (or other similar tubes). ASSAY PROCEDURE 1. Bring all reagents and specimens to room temperature. 2. Dispense three drops of each standard and serum/whole blood samples into specimen wells of cassettes (run at least two duplicates of each standard and sample). 3. Incubate 10 minutes for serum, or 15 minutes for whole blood samples 4. At the end of the test, read the test results by comparing samples to standards to determine bracketed concentration of CRP in the sample. RESULT INTERPRETATION Sample Results for CRP test: 0g/mL 0.1g/mL 1g/mL 10g/mL 100g/mL 1. At 0.1 g/ml or less, a weak signal should appear at test line 1 (T1). 2. At 1.0 g/ml, a strong signal should appear at test line 1 (T1). 3. At 10 g/ml, strong lines should appear at both T1, accompanied by a medium strength signal at test line 2 (T2). 4. At 100 g/ml, strong lines should appear at T1, accompanied by a medium strength signal at test line 2 (T2) and a weak signal at test line 3 (T3). 5. If no control (C ) signal is observed, the test result should be considered invalid and be run again. APPENDIX 1 Diagramatic Presentation of CRP 3 Test Line Whole Blood Cassette Test To Reveal Relative Signal Intensity As A Function of CRP Concentration (ug/ml) in Log Scale. CRP- 3Test Line Whole Blood Cassette Test Relative Intensity 3.5 3 2.5 2 Test Line 1 1.5 Test Line 2 1 Test Line 3 0.5 0 -2 -1 0 1 2 Log [CRP ug/ml] REFERENCES 1. Luhr, T. A., and Modi, J. Development of a high-sensitivity C-reactive protein assay. IVD Technology, 6(2): 27-35 (2000). 2. Ridker, P. M., Hennekens, C. H., Buring, J. E., and Rifai, N. C-Reactive Protein and other markers of inflammation in the prediction of cardiovascular disease in women. The New England Journal of Medicine, 342(12): 836-843 (2000). 3. Powell L, C-Reactive Protein A review, Am J Med Technol 87:138-142 (1979). 4. Kushner I, Rzewricki DL, “The acute phase response: General Aspects”, Ballicre’s Clinical Rheumatology 8:513-530 (1994). Ridker PM, Hennekens CH, Buring JE, Rifai N, C-Reactive Protein and other markers of inflammation in the protection of cardiovascular diseases in women. The New J Med 342:836-843 (2000). 5. 6. Ridker PM, Cushman M, Stampfer M, et al. Inflammation, aspirin, and the risk of cardiovascular disease in apparently healthy men. N Eng J Med 336:973-979 (1999). 7. Ridker PM, Cushman M, Stampfer M, et al. Pasmar concentration of CRP and risk of developing peripheral vascular disease. Circulation 97:425-428 (1998). 8. Koenig W, Sund M, Forlich M, et al. CRP; a sensitive marker for inflammation, predicts future risk of coronary heart disease in initially healthy middle-aged men. Results from the MONICA Augsburg Cohort Study 1984-1992. Circulation 99:237-242 (1999) 9. Katritsis D, Korovesis S, Giazitzoglou E, Parissis J, Kalivas P, Webb-Peploe MM, Ioannidis JPA and Halliassos A. Clin Chem 47:882-886 (2001). 10. Ridker PM, Glynn RJ, Hennekens CH: CRP adds to the predictive value of total and HDL cholesterol in determining risk of first myocardial infarction. Circulation 97:2007-2011 (1998). 11. Ridker PM, Buring JE, Shih H, et al. Prospective study of CRP and the risk of future cardiovascular events among apparently healthy women. Circulation 98:731-733 (1998). 12. Rifai N, Ridker PM. Proposed cardiovascular risk assessment algorithm using high sensitivity C-reactive protein and lipid screening. Clin Chem 47:28-30 (2001). 13. Chander J, Gurmin T, Robinson N. The place of gold in rapid tests IVD Technology 6:2 37-49 (2000). 14. Wilson NB, Nakane PK in “Immunofluorescence and related staining terchniques (knapp W, Holubar K, Wick G. Eds) pp 215-224, Elsvier/North-Holland Biochemical Press, Amsterdam (1978).