Country Report - United Nations ESCAP
advertisement

Singapore Country Report
for The 5 Asian And Pacific Population Conference
th
SECTION 1 – Overview of the Population and Development Situation and
Prospects, with Special Attention to Poverty
The key Singapore demographic indicators are given in the table below.
Key Singapore Demographic Indicators, 1970-2001
1970
1980
1990
2000
2001
Population Structure
Total Population ('000)
2,074.5
2,413.9
3,047.1
4,017.7
4,131.2
Resident Population ('000)
2,013.6
2,282.1
2,735.9
3,263.2
3,319.1
Resident Average Annual Growth1
n.a.
1.3
2.2
1.3
1.7
Median Age (Yrs)2
19.5
24.4
29.8
34.2
34.6
0-14 years
39.1
27.6
23.0
21.5
21.4
15-24 years
21.6
23.8
16.9
13.0
12.8
25-64 years
35.9
43.7
54.1
58.3
58.4
3.4
4.9
6.0
7.3
7.4
Age Dependency Ratio (%)2
73.9
48.2
40.8
40.4
40.4
Child (under 15 years)
68.1
41.0
32.3
30.1
30.0
5.9
7.3
8.5
10.2
10.4
Total Live Births
45,934
41,217
51,142
46,997
41,451
Crude Birth Rate
22.1
17.6
18.2
13.7
11.8
3,065
1,818
1,827
1,598
1,406
10,717
12,505
13,891
15,693
15,367
5.2
4.9
4.7
4.5
4.4
20.5
8.0
6.6
2.5
2.2
65.8
72.1
75.3
78.1
78.4
Age Composition (%)2
65 years & over
Old Age (65 years & over)
Fertility
(Per 1,000 Population)
Total Fertility Rate (per 1000 resident females 15-44 yrs)
Mortality
Total Deaths ('000)
Crude Death Rate
(Per 1,000 residents)
Infant Mortality Rate
(Per 1,000 resident live-births)
Life Expectancy (Yrs)
Note: Data prior to 1980 refer to total population unless otherwise stated. From 1990 onwards, population refers to de jure counts.
1
Refer to growth over the previous year. For 1980, refers to average annual growth of resident population during 1970-1980.
For 1990, rate is based on 1989 and 1990 de facto counts.
2
For 1970, refers to resident population.
SECTION 2 – Fertility Levels and Trends, and their Implications for
Reproductive Health, Including Family Planning Programmes
Singapore, like many developed countries, is experiencing sub-replacement
population growth. The Total Fertility Rate (TFR) was 1.60 in 2000. The government
appointed a Working Committee on Marriage and Procreation to study the
demographic trends and their implications, and propose solutions. A package of
measures was introduced in Aug 2000 to supplement those introduced under the
New Population Policy in 1987.
1
P
Recent Demographic Trends
The measures introduced under the New Population Policy in 1987 seemed to work
in the beginning, with the Total Fertility Rate (TFR) rising from 1.62 in 1987 to 1.96 in
1988. It was 1.75 in 1989 and 1.86 in 1990, after which it started to decline. Recent
key demographic trends are as follows:
(a) Rising Singlehood – The resident single population has increased from
747,200 in 1990 to 760,400 in 2000.
(b) Delay in Marriages – The median age has increased 1.6 years for grooms
and 2.0 years for brides since 1985. In 2000, the median age at first
marriage for resident grooms and brides was 28.6 years and 26.2
years respectively.
(c) Delay in Family Formation - The median age of mothers at the birth of their
first child has increased from about 26 years in 1985 to almost 29
years in 2000.
(d) Sub Replacement TFR – Consequent to the above factors, TFR for 2000
was 1.60.
There was a need to supplement the measures introduced in 1987 to help remove
some of the obstacles couples faced in having (more) children. In Feb 2000, the
Government formed a Working Committee on Marriage and Procreation to study the
demographic trends and their implications, and propose solutions.
Current Obstacles to Marriage and Procreation
Based on public feedback, the main challenges young Singaporeans face in getting
married could be summarised as follows:
(a) Changing attitudes towards marriage - Although survey data continues to
indicate that the vast majority of Singaporeans still desired to marry and have
children, it is not a top priority. Because education, career and home
ownership goals take precedence, the search for a suitable marriage partner
is frequently left too late.
(b) Lack of opportunities to socialise and lack of social skills - Surveys and
feedback showed that this was a key obstacle for many young people.
(c) Financial Cost - The high cost of a wedding and the need to save for a house
of their own are often cited as reasons for delay in marriage.
The key challenges in couples having (more) children are as follows:
(a) Financial cost of raising children - This is the topmost concern for
Singaporeans wanting to have more children.
(b) Inability to balance between work and child rearing - This is a critical concern,
especially in a 24x7 global economy.
(c) Lack of suitable childcare arrangements - Availability of childcare at
convenient locations is an important issue of concern for many.
Supplementary Measures of Aug 2000
Singapore has adopted the following guiding principle to underpin measures to raise
the TFR:
2
Creating a total social environment conducive to family formation and well
being - No one measure by itself might work. However, taken together, a
package of measures might have a reasonable chance of arresting the
decline in TFR.
In line with the above philosophy, the Working Committee introduced a host of
measures in Aug 2000 to supplement those introduced in 1987. The measures were
aimed at removing the main obstacles couples faced in marriage and procreation.
The success of the package of measures is unclear as its implementation coincided
with the onset of an economic recession. Past evidence shows that there is a close
positive correlation between economic performance and number of marriages and
births. Thus, the full impact of the package of measures will not be known for some
time.
SECTION 3 – Mortality and Morbidity Trends and Poverty
Singapore has undergone tremendous socioeconomic changes in the last three
decades. Economic progress, improved housing and sanitation, clean drinking water
and good public health services have contributed to the markedly reduced incidence
of communicable diseases such as tuberculosis, diphtheria, poliomyelitis and enteric
fever. Over the same period, our health care services have also improved
dramatically. Today, Singaporeans are better informed about health issues, expect
and receive good, affordable medical care and generally enjoy good health with high
life expectancy.
The rate of natural increase, increased from 8.3 per 1,000 resident population in
1999 to 9.2 per 1,000 resident population in 2000. There were 46,997 births in 2000,
which was an increase of 8.4% from 43,336 births in 1999. The Crude Death Rate
remained at 4.5 deaths per 1,000 resident population in 2000.
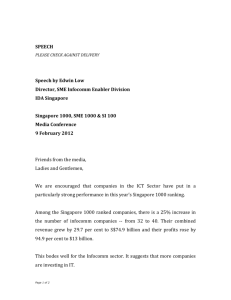
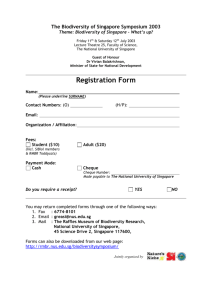
Infant Mortality
Singapore’s infant mortality rate continued to remain low at 2.2 per 1,000 resident
live births in 2001. This was lower than the rate of 3.3 per 1,000 resident live births
reported in 1999. The neonatal mortality rate and the perinatal mortality rate were
1.8 per 1,000 live births and 4.3 per 1,000 live and stillbirths, respectively.
FIGURE 1: INFANT MORTALITY, 1957 – 2000
Rate per 1,000
Resident Live-Births
50
40
30
20
10
0
1957 1960
1965
1970
1975
1980
3
1985
1990
1995
2000
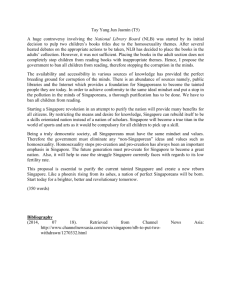
Maternal Mortality
There was an increase from four maternal deaths in 1999 to eight in 2000. The
maternal mortality has maintained at low rates of 0.07 1,000 live and stillbirths in
2001. Singapore’s maternal mortality rate is comparable with that of the developed
countries.
FIGURE 2: MATERNAL MORTALITY, 1957 –2000
Number of Deaths
60
50
40
30
20
10
0
1957 1960
1965
1970
1975
1980
1985
1990
1995
2000
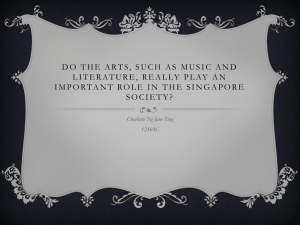
Life Expectancy
The average life expectancy at birth of Singapore residents was 78.4 in 2001
compared to 77.6 years in 1999. Expectancy of life at birth for males was 76.4 years
and that for females was 80.4 years.
FIGURE 3: LIFE EXPECTANCY AT BIRTH, 1957 – 2000
Expected
Years
85
Female
Total
Male
80
75
70
65
60
Year
55
1957
1960
1965
1970
1975
1980
1985
1990
1995
2000
Major Causes of Mortality and Morbidity
Since 1960, death rates have fallen for all age groups. The total number of deaths
increased marginally, from 15,516 in 1999 to 15,692 in 2000. The crude death rate
maintained at 4.5 deaths per 1,000 resident population. The leading causes of death
in Singapore continued to be cancer and heart disease. In 2000-2001, these
diseases constituted more than 50% of all causes of deaths in Singapore.
4
TABLE 1: 10 LEADING CAUSES OF DEATH, 1999 and 2000
Percentage of
Total Deaths
1999
2000
(15,516)
(15,693)
Cause
Cancer
26.6
27.0
Ischaemic & other heart diseases
25.7
25.1
Pneumonia
10.6
11.4
Cerebrovascular disease
10.5
10.4
Injuries
6.9
7.2
Diabetes mellitus
2.3
2.3
Nephritis, nephrotic syndrome &
nephrosis
1.2
1.3
Bronchitis, emphysema & asthma
0.9
0.7
Chronic liver disease & cirrhosis
1.0
0.7
Septicaemia
0.8
0.6
Non-communicable Diseases
Chronic non-communicable and degenerative diseases are the most important public
health problems in Singapore today. Cancer, coronary heart disease, and stroke are
the leading causes of mortality, accounting for over 60% of all deaths and a high
burden of disability. Most of these conditions can be prevented or their impact
ameliorated through the adoption of healthy life styles, optimal long-term control of
major risk factors such as diabetes and hypertension, and screening and early
treatment. Successful containment of these chronic non-communicable diseases at a
national level requires a comprehensive and coordinated approach involving various
agencies, healthcare facilities, and teams.
The Ministry of Health initiates and coordinates the development and implementation
of National Disease Management plans for stroke, coronary heart disease, common
cancers, myopia and renal failure. These plans set out strategies for each disease,
spanning the continuum from primary, secondary and tertiary prevention, to early
disease detection, effective treatment and rehabilitation. Health promotion activities
are conducted to educate the public on the prevention of chronic diseases through
the reduction of behavioral risk factors such as smoking, a sedentary lifestyle,
unhealthy diets, obesity and stress.
Cancer
Cancer has been the leading cause of death in Singapore since 1991. In 2000, it
accounted for 26.9% of all deaths. The main cancers causing death among men
during the year were cancers of the lung, colo-rectum, liver and stomach. For
women, these were cancers of the breast, lung, liver and colo-rectum. Pap smears
for cervical cancer and mammography for breast cancer are screening tests offered
at polyclinics and hospitals.
5
Cardiovascular Diseases
In 2000, cardiovascular diseases, including coronary heart disease and stroke
accounted for about one third (34.8%) of all deaths. Coronary heart disease is the
major cardiovascular disease. People with a high risk of developing cardiovascular
disease are encouraged to undergo tests to screen for risk factors. The three-year
community health screening initiative “Check Your Health” programme was launched
last year to provide people aged 55 years and older with a chance to be tested for
risk factors and counselled on the disease, at subsidised rates.
Diabetes Mellitus
Diabetes was the sixth most common cause of death in 2000. It is also the leading
cause of end-stage renal disease and blindness in adults. The Comprehensive
Chronic Care Programme (CCCP) was launched in 2001, with the aim to improve
the management of these three common cardiovascular risk factors, namely
diabetes, hypertension and high blood cholesterol. The benefit for patients in the
CCCP is the personalised care given by a case manager who tracks and
encourages each patient. This will facilitate patients’ compliance to treatment and
follow-up, thus ensuring good control and management of their medical conditions.
Myopia
Myopia is a major public health problem in Singapore. About one-third of primaryone (6-7 years old) students had myopia. A National Myopia Prevention Programme,
targeted to screen children at a young age, has been developed so that preventive
actions can be taken to arrest the progression of myopia among them. The Ministry
is working closely with the Ministry of Education on a special programme for school
children.
Mental Health
The major mental health disorders seen in Singapore are depression, anxiety
disorders, and schizophrenia. About one in ten persons have anxiety disorder. The
national plan for the prevention and control of major mental health disorders aims to
increase mental health awareness and promote good mental health. The Early
Psychosis Intervention Programme which is a comprehensive and integrated
treatment programme targets to reduce chronic disability among schizophrenic
patients.
End-stage Renal Disease
Renal disease has been among the top 10 leading causes of death in Singapore
since 1960. The number of new patients on dialysis has been continuously
increasing in the past decade. A national renal disease control plan is currently
under development. It involves strategies to reduce prevalence of risk factors like
diabetes and hypertension; detect renal disease at its early stages; and ensure good
clinical management of patients with chronic renal disease to prevent the
progression to end-stage renal disease (ESRD).
6
Communicable Disease
Legislation
The Infectious Diseases (ID) Act was enacted in 1976 to prevent the introduction and
spread of infectious diseases into Singapore. The Ministry of Health and the Ministry
of the Environment jointly administer this act. For the control of infectious disease in
Singapore, the ID Act provides for the notification of specified infectious diseases.
For the list of notifiable diseases, see Annex A.
Childhood Diseases
The Childhood Immunisation Programme offers our children protection against nine
important childhood diseases namely, tuberculosis, diphtheria, pertussis, tetanus,
poliomyelitis (Sabin), measles, mumps, rubella (MMR) and Hepatitis B. Diphtheria
and measles immunisation are compulsory by law. All immunisations except
Hepatitis B, are given free at the polyclinics and schools.
Poliomyelitis
The Western Pacific Region, of which Singapore is a member, was certified by the
World Health Organisation (WHO) to be free of poliomyelitis (or polio) on 29 Oct
2000. After the Americas, this is the second region in the world to have achieved
polio-free status.
Tuberculosis
Since 1987, after more than a decade of stagnation, the rate of new tuberculosis
cases is started a declining trend since 1999. This could be attributed to improved
surveillance and treatment strategies adopted since 1997 under the Singapore TB
Elimination Programme (STEP). STEP was implemented in Apr 1997 to strengthen
the existing TB Control Programme with the aim of eliminating the disease in fifteen
years’ time. Strategies include treatment of infectious TB cases, early detection,
chemoprophylaxis for infected contacts, and prevention (BCG vaccination). The
STEP Surveillance System was enhanced in 2000 to facilitate surveillance and
monitoring of TB cases.
Hepatitis B
Reported cases of Hepatitis B infection in Singapore has deceased over the past few
years. The overall Hepatitis B immunity rate is 40%, with the young age group of 1829 years having the lowest immunity rates. Prevention through immunisation is a key
strategy in the Hepatitis B control programme in Singapore to prevent liver cancer.
Over the last six years the coverage of infants who completed the full course of
Hepatitis B immunisation has been about 90%.
HIV
See section 8.
SECTION 4 – Migration, Urbanisation and Poverty
CIRD to fill in based on inputs from relevant agencies ……...
7
SECTION 5 – Population Ageing
Current Situation of the Elderly Population
In Singapore, the number of residents aged 65 years and over has increased
significantly .In 1990, there were 164,000 elderly and they constituted 6% of the
resident population. In 2000, their size increased to 238,000 or 7.3%
Overall, there were fewer men than women among the elderly population. This is
largely contributed by the longer female life expectancy as compared with the male
is a major contributing factor.
With increased longevity, the old-old population (aged 85 years and over) increased
at a faster pace than the overall elderly population. From 1990 to 2000, the old-old
increased by 6.1% as compared with 3.7% for the elderly. Male had a slightly higher
growth rate than females in both the elderly and old-old populations.
Policies and Programmes to Provide Support to the Elderly Population
Policies and programmes that need to be developed to provide support to the elderly
population are wide ranging. We will consider those in the areas of healthcare,
housing, income security, caregiving facilities and living arrangements.
Healthcare
In the area of healthcare Singapore adopts a multi-prong approach to address the
needs of the elderly and to support the elderly.
Health Promotion and Prevention of Disability
We emphasize health promotion and prevention of disability. Public education is
conducted through public forums and workshops. We have set up an exhibition
zone on healthy living, where exhibits and fun models are placed and open to
visitors. A Committee on Health Screening was set up to work out guidelines on the
types and frequency of screening for the adult population. Health screening
programmes are conducted for early detection of problems and early treatment
through a national community health screening programme. which screens for
hypertension, diabetes and blood cholesterol levels.
Health Services for the Elderly
A range of health services is in place to cater to the needs of the elderly. This
includes acute hospital services, specialty services, outpatient services, community
hospitals, nursing homes and home care services.
Licensing and auditing standards are set for the healthcare institutions to ensure that
care standards are of an acceptable level.
Training courses for caregivers are available at many healthcare institutions and also
at the grassroot organisations. This courses serve to teach caregivers basic skills in
caring for the elderly
8
Housing and Living Arrangements
Project to Improve the Living Conditions of the Elderly
This project was introduced in 1993 jointly by Ministry of National Development
(MND), HDB, and the Ministry of Community Development and Sports (MCDS) to
improve the living conditions of 1-room rental blocks with a high concentration of the
elderly. Improvements include:
i.
installing support handlebars in toilets, common corridors and lifts
ii.
alert alarm systems
iii.
non-slip tiles
iv.
having lift landings on every floor.
These improvements are fully paid for by the government. MCDS also arranges for
VWOs to provide care and support services and organise activities for the elderly
residents. To facilitate the provision of care and support services, HDB provides
space for the VWO to set up and operate a Seniors Activity Centre (the
Neighbourhood Link now replaces the Seniors Activity Centre) within the block. The
provision of both hardware and software (assistance from MCDS) has allowed the
elderly to live independently while being assured of help when they need it.
Studio Apartment
Studio Apartments was launched in 1998 to meet the needs of a growing number of
senior citizens. These customised apartments with 30-year leases will better meet
the elderly citizens' housing needs as well as allow them to live near their children
and other elderly people in HDB estates where public amenities are easily
accessible. Elderly-friendly features such as brightly lit corridors and lever tap
handles are complemented with safety features like pull cords linked to an alert
system, as well as heat detectors linked to the central fire alarm system to create a
hospitable living environment. There are also Voluntary Welfare Organisations
(VWO) providing care and support services to the elderly in these apartment blocks.
Lift Upgrading Programme (LUP) and the Main Upgrading Programme (MUP)
LUP provides easy access and mobility for the elderly who may find staircases an
obstacle to their movements. In MUP, standardised elderly-friendly features such as
non-slip bathroom tiles have also been included as an optional item.
Cash Grants
Other schemes that complement the elderly projects are incentives in the form of
cash grants or priority allocation of new flats. These encourage married children to
live together with their parents or near their parents for mutual care and support.
Examples of such schemes include the Multi-Tier Family Housing Scheme, and the
Joint-Selection Scheme.
Income Security
Older workers are more vulnerable because of seniority-based pay system pushes
wages up beyond what their skills and productivity can justify. When older workers
lose their jobs, they tend to have higher wage expectations, which makes it more
difficult for them to find re-employment. The 40% CPF contribution rate exacerbates
9
these problems, because it discourages employers from taking on older workers,
and also discourages older workers from working for lower take-home pay.
To address the problem of older workers being less skilled, there is a need to
continue pushing for skills upgrading. Last year, the Government introduced a
comprehensive set of programmes to upgrade the skills of older workers. These
included enhanced support for the Skill Redevelopment Programme (SRP), and the
People-for-Job Traineeship Programme (PJTP) which incentivises employers to hire
older workers by defraying part of the associated training costs. These programmes
were originally intended to last for 12 months, to tide older workers over immediate
difficulties in the economic downturn. The Government will now extend the enhanced
support to the SRP, as well as the PJTP, for an additional year until November 2003.
The government will also improve the PJTP for older workers. Under the PJTP,
workers receive wage support for 6 months, amounting to 50% of their wages. For
workers who are more than 50 years old, the government will extend this period of
wage support to 9 months, but at a lower support rate of 25% for the additional 3
months.
To address the problem of the seniority-based wage system, there is a need to inject
greater flexibility in the wage system. The effort to promote flexi-wages has yielded
results, but it will take many years to complete. There is a need to complement it by
lowering the burden of statutory charges on wages for this vulnerable group of older
workers.
The Government therefore agrees with the recommendations of the ERC to keep the
employer’s CPF contribution rate for workers aged 50-55 at the current 16%. We will
also progressively lower the employee CPF contribution rate for workers aged 50-55
from 20% to 16%, as we restore the CPF contribution rate. This will increase the
take home pay for these workers and help them to meet their financial commitments.
With this structural change, the total CPF contribution rate for workers aged 50-55
will be 32% - 16% from employers and 16% from employees. This is a meaningful
step-down from the 40% full rate for those aged below 50, to 32% for those aged 50
- 55, to 20% for those aged 55 - 60. It will encourage employers to keep their older
workers.
Some older workers have also expressed concern that the non-restoration will affect
their ability to service their mortgages. To help workers facing mortgage shortfalls
due to the non-restoration, the Government will allow these CPF members to
continue to draw on their Special Account to pay their mortgages for a longer period
of time. The government had already introduced such a scheme when the CPF rate
was cut in 1998. The government will extend its duration.
Programmes at the Grassroots Level
Grassroots organisations are very active in programmes and initiatives to support the
elderly. Programmes at the grassroots levels include:-
10
(i)
(ii)
(iii)
(iv)
(v)
(VI)
Partnership with Ministry’s to provider subsidised primary care services
to the needy elderly
collaboration with hospitals and healthcare providers to conduct
training programmes for caregivers
community outreach programmes to identify and address the needs of
elderly in the community through volunteer groups
organisation of health fairs
provision of neighbourhood meals to needy elderly
set up of IT centre to encourage senior citizens to learn new skills
SECTION 6 – Reproductive Health
The infant mortality rate and maternal mortality rates in Singapore are comparable to
most developed countries. The government, as part of its national development
programme, embarked on a family planning programme immediately after Singapore
achieved independence in 1965. Besides the comprehensive provision of clinic
services, the programme included a wide range of social and fiscal incentives to
achieve a "two child" family norm. After a decade stabilisation of population growth,
the government has replaced the policy in 1987 with a selectively pro-natalist "three
or more if you can afford it" policy.
TABLE 3: NUMBER OF LIVE-BIRTHS, CRUDE DEATH RATES (CBR), TOTAL FERTILITY RATES
(TFR) AND CRUDE DEATH RATES (CDR), 1957 – 2000
1957
1970
1980
1990
1999
2000
61,757
45,934
41,217
51,142
43,336
46,631
1,000
42.7
22.1
17.6
18.4
12.8
13.6
TFR (per woman 15-44
yrs)
6.41
3.07
1.82
1.87
1.47
1.59
CDR
(per
population)
7.4
5.2
4.9
4.8
4.5
4.5
Total Live Births
CBR
(per
population)
1,000
Family Planning Services
Family planning services are readily available to the whole population through
services provided by the Ministry of Health, public and private doctors. The service is
available both at a tertiary level (KK Women's and Children's Hospital) as well as at
primary care level through government polyclinics. These provide the people with
informed choice on various type of contraception. IUCD (Intra Uterine Contraceptive
Device) and Hormonal Contraception is available on a prescription-basis, after
proper medical evaluation. Emergency contraception is also available at the tertiary
centers.
11
Termination of Pregnancy
Abortion was legalised in 1970, and is readily available and accessible to all
Singaporeans and residents. This Act ensures that women who have unwanted
pregnancies, who have exhausted all existing options, undergo a safe treatment of
termination of pregnancy performed by suitably trained doctors.
The Termination of Pregnancy (TOP) Act currently allows authorized doctors to
provide treatment to terminate a pregnancy which is less than 24 weeks gestation in
approved institutions. TOP can only be performed by authorized medical
practitioners and in approved institutions. The Ministry of Health approves the list of
institutions or medical practitioners who can perform TOP. Under the TOP Act, preabortion counselling is required before the treatment of termination of pregnancy is
done. For women under 16 years of age, who under go abortion, special counselling
with emphasis on adolescent health education, is conducted at a special center by
trained staff.
Adult Reproductive Health
Singapore provides a comprehensive tertiary to primary level adult gynaecological
health services. At tertiary level, this also includes gynaecological oncology and
urology. Singapore has achieved some major milestones for treatment of infertility in
the past decade, including high IVF (in vitro fertilization) success rates.
Reproductive Health Screening Programmes are offered at the primary and
secondary care level and include breast and cervical cancer screening. The
screening is offered at subsidised rates, at multiple centers across the island. There
is a well-established referral system of positive cases to specialised centers for
further evaluation and treatment. A screening registry to support tracking and recall
of patients for screening is being developed at the national level.
SECTION 7 - Adolescent Reproductive Health
School Curriculum
The teaching of growth and development is included in the health education syllabus
at all levels in primary school. This includes teaching children about habits that
promote healthy growth, changes at puberty and ways to cope with these changes.
AIDS/sexually transmitted diseases (STD) are mentioned as transmissible diseases.
For secondary schools, the teaching of human reproduction, STD and AIDS is
included in the lower secondary science and biology syllabi.
The Ministry of Education (MOE) has a sexuality education programme, “The
Growing Years” which aims to provide knowledge about human sexuality and the
consequences of sexual activity to enable students to make informed decisions.
Different educational packages are developed for the various educational levels.
Training sessions are conducted to enable teachers to conduct the activities on
sexuality with confidence.
12
AIDS Education Programme
In addition to the teaching in the school curriculum, the Ministry of Health's statutory
division, Health Promotion Board, conducts an ongoing AIDS education programme
at schools. The objectives of the AIDS education programme are to:
(i)
(ii)
(iii)
raise awareness of AIDS/STD among school students
inform students about ways to prevent STD/AIDS infection
discourage promiscuous sexual behaviour
The AIDS Education Programme is targeted at all secondary schools, vocational
training centres, polytechnics and other pre-university centres. The programme
comprises talks, video shows, exhibitions and distribution of educational print
materials. The content includes discussion on STD and AIDS, the importance of
abstinence, effects of pre-marital sex and ways to prevent STD infection.
Non Government Organizations
Various NGOs are involved in family planning and population work. These
organizations concentrate on enhancing quality of life through the promotion of
reproductive health and the knowledge of human sexuality, through formal sex
education programmes. A voluntary organisation, Action for AIDS, Singapore, was
formed in 1988. Its activities complement the government's efforts in controlling AIDS.
Its objectives are to promote educational activities relating to AIDS and HIV infection,
support welfare activities for and prevent discrimination against patients and families.
SECTION 8 – Demographic, Economic and Social Impact of HIV/AIDS
Human Immunodeficiency Virus &Acquired Immunodeficiency Syndrome
Since the first reported cases of Human Immunodeficiency Virus (HIV) infection in
1985, by 31 December 2001, 1599 Singaporeans were reported to be HIV infected.
Among them, there were 628 asymptomatic carriers, 381 with full-blown AIDS and 590
have died. Most of these were single males in the 20 – 49 age group. Sexual
transmission was the main mode of transmission among Singaporeans. Up to the end
of December 2001, 96.4% of all HIV infected Singaporeans contracted their infection
through sexual transmission. Very much smaller proportions contracted the infection
through intravenous drug use (2%), through the perinatal route, 0.3% and through renal
transplant overseas and 0.2% through blood transfusion.
Although homosexual transmission was the more common mode of HIV transmission
in the early years of the epidemic in Singapore, heterosexual transmission has become
the most common mode of HIV transmission among Singaporeans since 1991. In
2001, it accounted for 81% of HIV transmission among Singaporeans. Most of these
cases contracted the infection through casual sex with commercial sex workers in
Singapore and overseas. The male-to-female sex ratio among the known cases was
7:1. Almost 60% of cases were between the ages of 20 - 39 years at the time of
diagnosis.
13
National AIDS Control Programme in Singapore
The control and prevention of AIDS comes under the central control of the Ministry of
Health, with the active involvement of all relevant government agencies and community
groups to combat and control AIDS in Singapore. The National AIDS Control
Programme was drawn up in 1985.
The programme comprises:
•
public education and education of high risk groups;
•
legislation;
•
immigration and labour policies;
•
protection of the national blood supply through routine screening of blood
and blood products;
•
management of the infected;
•
counselling those with high risk of infection;
•
monitoring the disease;
•
training of personnel; and
•
conducting research and studies.
The main focus of Singapore's programme against AIDS is on health education. The
health education is targeted at the general population as well as those at risk of the
infection. To further enhance AIDS education for persons at high risk of infection, AIDS
education programmes are carried out for high-risk groups and the adolescent.
Individuals who perceive themselves to be at risk of infection are encouraged to
undergo HIV screening. Since early detection of the infection allows early treatment
and care, facilities for anonymous screening are widely available. Counselling also
provided at screening centres, as an opportunity for a change in lifestyle and risk
behaviour.
In Singapore, subsidised inpatient and outpatient care is accessible to HIV/AIDS
patients. Patients are allowed to draw from their Medisave account for anti-HIV drugs
that are registered in Singapore. HIV/AIDS patients who require additional financial or
social assistance can approach NGOs or other charitable organisations for help.
SECTION 9 – Gender Equity and Development
Approach by Government
Singapore is committed to women's empowerment and their full participation on the
basis of equality. The basic rights of women are ensured through legislation, namely
the Singapore Constitution, the Women's Charter, the Employment Act and the
Penal Code. Meritocracy based on equal opportunities has been a key principle
guiding gender equality in Singapore.
Men and women are treated as equal partners in society and women are not
marginalised or disadvantaged. Equal opportunities based on the principle of
meritocracy has resulted in women naturally occupying important leadership
positions in various spheres, as trade union leaders, youth leaders, Ambassadors,
14
Members of Parliament, entrepreneurs, judges and more recently as Divisional
Police Commander, Permanent Secretaries in the Civil Service, Commanders of
army and air force units and President of the Association of Small and Medium
Entreprises (ASMEs).
Education and Skills Upgrading
The key to equalising opportunities is via education of females. From 2003, primary
school education in national schools will be made compulsory for both boys and girls
(6 years). The intake levels of females at our polytechnics and Universities have
been increasing steadily over the years, from 42.1% and 50.2% respectively in 1990
to 47.4% and 51.3% in 2000. This has helped to close the gender wage gap, from
21% in 1991 to 11% in 2000 for professionals, and from 39% to 19% for production
crafts-persons.
Employment
At the work place, female employees are protected by existing labour legislation
against any form of discriminatory practices and exploitation. There is equality of
treatment in respect of employment terms and compensation for work-related injuries
in various occupations. The Employment Act, which stipulates the minimum terms
and conditions of employment, offers protection to employees regardless of gender,
age or religion. Employees who feel aggrieved by unfair employment practices may
seek the assistance of the Ministry of manpower or seek redress through the civil
court.
Our Female Labour Force Participation Rate continued to improve, from 52.7% in
1999 to 54.3% in 2001. With improved education, the proportion of women in the
Professional, Administrative, Technical and Managerial positions continued to
improve from 35.5% in 1999 to 37.3% in 2001. More females are also taking up
courses previously dominated by males, such as in engineering. In 2000, the ratio of
females to males of the first year engineering students at the University was 1: 2.4,
as compared to 1:5 in 1995.
Skills training and lifelong learning are given great emphasis by Government to
enable Singapore to compete in the global economy. Equal access to training is
given to workers of both sexes. Women took up about 61% of the training places of
the Skills Redevelopment Programme.1
The minimum statutory retirement age was raised from 60 to 62 from 1 January 1999
under the Retirement Age Act. This benefits both male and female employees who
are given the opportunity to continue working until the age of 62 years.
In May 2002, Singapore ratified a core ILO Convention- Convention 100 on Equal
Remuneration. The ratification of this Convention is an affirmation of our belief in
the fair and equal treatment of men and women at the workplace for work of equal
value.
1
April to Jun 2001
15
Health
Singapore has attained parity with the advanced industrialised countries in the health
status of its population including women. Female life expectancy at birth reached 80
years in 1999, infant mortality rate was 3.3 per 1,000 resident live births and
maternal mortality rate was almost zero, one of the lowest in the world.
Family and Work Life
With equal education and job opportunities for girls, dual income families are
becoming a norm in Singapore and currently 45% of our households are dualincome. The Married Female Labour force participation rate continued to increase,
from 43.9% in 1995 to 52.3% in 2001.
The National University of Singapore (NUS)2 Study in 2000 on “Family Ideology and
Practice: Implications for Marital Satisfaction” found that the majority of Singapore
women tended to be traditional in their perception of gender-specific domestic
responsibilities and ideals. However better-educated women3 were increasingly
likely to prefer a more egalitarian role sharing relationship with their spouse. As this
group of women is likely to increase in the work force, and more singles can be
expected to take on a larger care giving role as Singapore’s population ages, the
Singapore Government introduced work life strategies at the work place and other
measures such as family life education programmes to create a total environment
conducive to raising a family.
Since 1 October 2000, the Singapore Civil Service has implemented various work
practices that will allow its employees to have a better work-life balance. These
include granting a married male officer full pay unrecorded leave for 3 days each on
the occasions of the birth of his first three children. Ministries and departments are
also allowed to implement work-life strategies such as flexi-work arrangements and
telecommuting. More and better child care centres and family life programmes are
being provided.
There has been increasing awareness on the importance of fathers’ involvement in
the upbringing of the young. Fathers are beginning to realise and appreciate their
own involvement in the development of their children. The Centre for Fathering
(Singapore), a non-profit company, has been working with individuals, corporations
and community groups to create public awareness, equip fathers with parenting skills
through fathering seminars and emphasise the importance of strong marriages in
providing a nurturing environment for children.
The Singapore Government will continue to work closely with its partners including
women's groups to facilitate women's participation in various fields.
2
By Paulin Tay Straughan, Department of Sociology, Shirlena Huang and Brenda Yeoh of the Department of
Geography. The study consisted of 1,000 women.
3
About 20 % of the study group.
16
SECTION 10 – Behavioural Change Communication and Advocacy and
Information and Communications Technology as Tools for Population and
Development and Poverty Reduction
Infocomm21 is Singapore’s five-year strategic plan for harnessing Infocomm
technologies to boost national competitiveness and improve quality of life for its
people. One of the goals of Infocomm 21 is widespread use of technology by
Singaporeans. To achieve this, the Singapore Government firmly believes that the
use of Infocomm technology will empower its citizens to enjoy a better quality of life.
To ‘e-power’ the people of Singapore, the Government has adopted a three-prong
approach as follows:
Increase Infocomm literacy
Improve access to Infocomm technology
Encourage adoption of an e-lifestyle
Driving this movement is the Government’s vision of an e-inclusive society where
everyone, regardless of age, language, social background or ability, are able to reap
the benefits of Infocomm technology for a better quality of life.
To realise this vision, the Government created a tripartite partnership involving the
3Ps representing the People sector (community groups and voluntary welfare
organisations), the Private sector (commercial organisations) and the Public sector
(government agencies). Harnessing the power of partnership toward this common
goal of national e-inclusion, a three-year programme was launched in 2000 to
encourage Singaporeans to embrace an e-lifestyle.
What is an e-lifestyle?
To live an e-lifestyle, Singaporeans need to know how to leverage Infocomm
technology to enhance their quality of life, improve employment opportunities and
adopt lifelong learning. An e-lifestyle bridges lives and distance; individuals are able
to communicate online anytime, anywhere with friends and families. An e-lifestyle
also empowers individuals to discover their true potential through online learning and
education opportunities. By using the Internet to perform routine or time-intensive
tasks such as paying bills, filing tax returns or buying movie tickets, Singaporeans
enjoy convenience as well as time and cost savings.
Since year 2000, a comprehensive range of public education programmes has been
developed to encourage Singaporeans to embrace an e-lifestyle, especially in four
key areas (4Es) of e-Learning, e-Communications, e-Entertainment and eTransactions.
Audience profile
A profile-oriented strategy has been adopted to encourage adoption of an e-lifestyle
by identifying six distinct profiles among the population of Singapore:
Workers
Homemakers
Senior Citizens
Professionals/Managers/Executives/Businessmen (PMEBs)
Students
Disabled individuals
17
Such a profile-oriented strategy helps individuals relate to the benefits of an elifestyle according to their needs. This is achieved by promoting awareness and
usage of key online services and Infocomm appliances that are relevant to them.
It has been recognised that students and PMEBs are typically ahead of the other
groups in adopting aspects of the e-lifestyle. Because of their exposure to
technology in school or at work, they tend to be more savvy and receptive to
performing tasks or purchasing goods and services online. In this respect, PMEBs
and students are viewed as ‘influencers’ who can help other individuals appreciate
the benefits of an e-lifestyle.
The journey so far
Supported by partners from the public, private and people sectors, an e-lifestyle
campaign called e-Celebrations Singapore was launched in 2000. Positioned as
Asia’s most extensive e-lifestyle campaign to shape Infocomm adoption for learning,
work and leisure, e-Celebrations Singapore features a vibrant mix of programmes
and activities to accelerate the adoption of an e-lifestyle among the public. Whether
you are seven or seventy, e-Celebrations Singapore promises something fun and
interesting for everyone. The activities are all designed to encourage online activity
through engaging the target audience in one or more of the 4Es. In 2001, eCelebrations reached out to over 300,000 homemakers, senior citizens, workers,
students and disabled individuals. e-Celebrations 2002 is a year-long series of elifestyle events with special themes each month, such as Broadband Month, eVolunteer Month, Infocomm Literacy Month, e-Society Month and Wireless Month.
Through collaborative efforts with community partners to build an e-inclusive society
these past two years, Singapore has scored especially well in the area of Infocomm
usage in Households. In year 2001, 64% of households have at least one computer.
Internet connectivity grew quickly with 57% of households having Internet access in
2001. The adoption level of Infocomm technology has also increased among
Singaporeans. Between 1996-2001, yearly surveys on Infocomm Usage in
Households show that Internet access has grown steadily across different ethnic
communities and income groups. More senior citizens and individuals with lower
education are also beginning to use the Internet. Singapore is successfully
narrowing the digital divide that exists between people of various ages, income
levels, ethnic background and educational qualifications. In June 2000, the World
Information Technology and Services Alliance or WITSA gave Singapore the Award
for Excellence in the Public Sector in recognition of its efforts to promote an elifestyle.4
Strategy: Improving Infocomm Literacy
National IT Literacy Programme (NITLP)
Targeted at workers, homemakers and senior citizens, NITLP equips trainees with
basic computing and Internet skills that will improve their quality of life and enhance
their employment opportunities. Since June 2001, more than 85,000 individuals been
trained under this programme, which is available at 35 training centers across the
island.
4
For more information www.ecelebrations.gov.sg
18
The NITLP also offers an e-learning module which allows trainees to practise what
they have learnt in the classroom. The biggest advantage is that they can do this at
their own pace, anytime, anywhere, as long as they have access to the Internet. eNITLP adds an experiential element to the classroom curriculum by providing
simulated lessons to guide learners, step-by-step, on how to use the Internet for
transactions, communication and entertainment. 5
Strategy: Improving Access to Infocomm Technology
PC Reuse Scheme
The PC Reuse Scheme provides needy families with refurbished personal
computers so that they can have the opportunity to learn IT skills. This scheme also
helps to minimise PC wastage as old computers are given a new lease of life. Old
computers are collected from government agencies, private sector companies and
members of the public. Community groups arrange for the old computers to be
refurbished and deployed to needy recipients through self-help groups. Some of the
self-help groups have even set up their own IT resource centres for their members to
be trained in basic IT skills. To date, about 9000 PCs have been deployed to needy
families and the self-help group’s IT Resource Centres. Each refurbished computer
comes with six months of toll-free Internet access and at least one year of technical
support. The recipients can also attend the National IT Literacy Programme (NITLP)
for free. 6
Special Programmes for the Disabled Community
To ensure that people living with disabilities are not neglected, the Government took
the lead in organising the Assistive Technology 2001 Exhibition to create awareness
of how technology can empower disabled individuals for daily living, work and play.
The exhibition showcased technologies designed to assist and empower the
disabled community. This inaugural event attracted more than 7000 participants. 7
Strategy: Encouraging Adoption
e-Ambassador
The e-Ambassador programme combines Infocomm technology with the spirit of
volunteerism. Early adopters of Infocomm technology are recruited as eAmbassadors and trained in IT and communication skills, then entrusted to coach 10
family members or friends in using Infocomm services and appliances. The eAmbassadors empower fellow Singaporeans to discover their potential and enjoy the
many benefits of Infocomm technology. Currently, there are 1,200 e-Ambassadors
in the community inducting their friends and family to the e-lifestyle. 8
Multi-lingual Internet Content
To cater to the needs of Singapore’s multi-racial society, focus groups were formed
to promote the development of Malay and Tamil Internet content, as well as
encourage Internet usage within these two communities. The Singapore Government
For more information www.nitlp.com.sg
For more information www.ecelebrations.gov.sg/eprog_pcreuse.html
7
For more information www.ecelebrations.gov.sg/www/assistivetech/index.htm
8
For more information www.ecelebrations.gov.sg/eambassador/about_the_programme.htm
5
6
19
assists in developing and aggregating compelling local content in Malay and Tamil.
An example is e-Pedoman, the first-of-its kind, bi-directional, English-to-Malay
translation portal launched in March 2001. The two focus groups reached out to
more than 780,000 individuals in the Malay community and 500,000 individuals in
the Tamil community to raise awareness and encourage adoption of an e-lifestyle. A
similar National Chinese Internet Programme has also been very successful in
helping the Chinese-speaking community embrace the Internet. 9
Most recently… The Great Singapore Surf
From 30 August – 1 September, 10,000 Singaporeans took a dive into the world
wide web at the Great Singapore Surf, the country’s largest ever mass IT training
event. Organised by a whole host of community, private and public sector partners,
this inaugural event taught participants basic computing and Internet skills required
to navigate the web. The Great Singapore Surf marks the start of the Infocomm
Literacy Month, which takes place between 30 August to 30 September 2002. This
month long event highlights the importance of infocomm literacy and lifelong
learning. The target is to train 15,000 people at the Great Singapore Surf and
through an island-wide promotion for NITLP at select Authorised Training Centres
during the Infocomm Literacy Month. 10
Singapore – the path to e-inclusion
The Government manages a variety of awareness and outreach programmes to
encourage Singaporeans to live the e-lifestyle, and will continue to drive the einclusion movement to empower individuals to discover their potential through
Infocomm technology. For those who are already ‘e-included’, the challenge is to
raise the level of sophistication in how they use Internet applications and services.
Through e-inclusion, every Singaporean will enjoy a better quality of life and
increased employment opportunities.
SECTION 11 – Data, Research and Training
The Singapore Government has the expertise within its various agencies to conduct
research, and collect and interpret data.
In particular, the Singapore Department of Statistics conducts demographic research
into a variety of topics, from household living arrangement to changing marriage
patterns. In recent years, research focuses on the implications of changing age
structure. The Department also maintains a comprehensive system of demographic
indicators on a routine basis. These include population estimates, marriage and
divorce indicators, life expectancy at birth, fertility and mortality indicators. The
pertinent data are published in the Department's Monthly Digest of Statistics,
Yearbook of Statistics and Statistical Highlights, as well as other occasional
publications.
In addition, its three universities are well positioned to provide academic expertise
where necessary.
9
For more information www.epedoman.com.sg
For more information http://www.ecelebrations.gov.sg/great_spore.html
10
20
SECTION 12 – Partnership and Resources
The Singapore Government has an established network of private and community
partners on whom it leverages on for its policy and programme formulation and
implementation, such as the healthcare system.
The Singapore Healthcare Financing System
The Government ensures that good and affordable basic medical services are made
available to all Singaporeans through the provision of heavily subsidised medical
services at the public hospitals and polyclinics. All private hospitals, medical clinics,
clinical laboratories and nursing homes are required to maintain a good standard of
medical services through licensing by the Ministry. The Singapore healthcare
financing system is based on individual responsibility, coupled with government
subsidies to keep basic healthcare affordable. Patients are expected to pay part of
the cost of medical services that they use, and pay more when they demand a higher
level of services. In the public hospitals, the hospitalisation expenses are subsidised
up to 80% by the government. Individuals are encouraged to take responsibility for
their own health by saving for medical expenses.
Government Healthcare Finance Schemes
The Government has put in place three major financing schemes to help
Singaporeans pay for their share of healthcare expenses – Medisave, MediShield
and Medifund.
Medisave is a compulsory savings scheme, introduced in 1984, to help
Singaporeans save and pay for their hospitalisation expenses, especially for their
retirement. Under the Medisave scheme, every working person is required by law to
set aside 6-8% of his income into his personal Medisave account which can be used
to pay for the hospitalisation expenses incurred by himself or his immediate family
members.
To supplement Medisave, an affordable basic catastrophic illness insurance scheme
called MediShield was introduced in 1990. MediShield, is a catastrophic illness
insurance scheme, is designed to help individuals meet the medical expenses from
major or prolonged illnesses. To avoid the problems associated with pre-paid
insurance, MediShield operates on a system of deductibles and co-payment. In
1994, the MediShield Plus schemes were introduced to cater to those using private
hospitals or higher class or wards in the public sector hospitals.
While the co-payment principle helps to avoid the pitfalls of a completely free
medical system. Community and state help are made available to those in need, so
that no Singaporean would be denied of essential medical treatment because of
inability to pay. In 1993, the Government established Medifund to help needy
Singaporeans pay their medical bills. It provides a safety net for those who, despite
help from government subsidies, Medisave and MediShield, are still unable to afford
their medical expenses.
21
Government Subvention
The Ministry of Health provides funding to the public hospitals, and VWOs (voluntary
welfare organisations) which offer a range of community and home-based medical
and nursing care.
The subsidy accorded to each inpatient depends on the class of ward that the patient
chooses to stay in, ranging from 20% to 80%. Financial counselling is provided by
the hospitals to allow patients make informed choices between the different types of
ward accommodation on admission. The primary care services provided at the public
sector polyclinics are subsidised at 50% of costs for the elderly/child and 50% for
adult. Subsidies are also given to VWOs that provide healthcare services such as
renal dialysis, nursing home care and hospice are. The Ministry funds 50% of the
operating expenditure of these VWOs and 90% of their capital expenditure.
In Apr 2000, the Government established the ElderCare Fund to secure the future
affordability of step-down care for households of low-and lower-middle income. The
interest income the ElderCare Fund derives would be used to finance operating
subsidies to community hospitals, hospices, nursing homes, day rehabilitation, home
medical
SECTION 13 – Other Issues
Helping disadvantaged families
While Singapore has put in place affordable health care, housing and education for
the general population, there is always a segment of the society who may fall into
greater need. These disadvantaged families generally lack resources and family
support and may need assistance to access basic services to support them through
difficult times. A range of relief schemes/measures have been put in place to provide
disadvantaged families help with basic subsistence needs, housing costs, health
costs, child care services and schooling expenses.
Under its "Many Helping Hands" approach, the government works together with
voluntary, community and religious organisations to develop a network of social
services to assist individuals and families in need. The overall emphasis is to help
families falling into need to recover and become self-reliant over time. The bulk of
help given is through subsidies for education, health and housing; direct financial
assistance is given for targeted programmes such as rental housing, childcare and
student care. Financial assistance for general living expenses is given after
casework assessment. The government waives school fees for deserving cases. The
3 Ms approach (Medisave, Medishield and Medifund) for financing healthcare
ensures that the most needy are provided for. Low cost rental housing and
generous housing schemes are also provided to ensure that low-income families are
able to access public housing.
The government builds the social safety net by acting as a provider and catalyst. It
supports infrastructure and social service development by voluntary welfare
organisations through its policies, allocation of land and matching funds for approved
22
programmes. The government also assists in capability building of the social service
agencies, namely in staff training, systems improvement and the use of information
technology.
Employment assistance and skills upgrading are key measures for eradicating
poverty,as they help build capacity so that they can remain productive and gainfully
employed in the new economy. Large scale grant programmes have been set in
place to encourage skills upgrading, ranging from providing affordable training for
low-skilled workers to incentivising employers to send their workers for training.
These will help families get back to or remain in the workforce and improve their
household incomes with time. The importance of helping the children of
disadvantaged families to break out of the poverty cycle is recognised. Early
intervention to foster childhood development is crucial. Hence, the government is
exploring more early intervention models for children, such as Healthy Start.
23
Annex A
List of Notifiable Diseases in Singapore
1. Tuberculosis
2. Venereal diseases
(Chancroid, Gonorrhoea, Non-specific urethritis, Syphilis)
3. AIDS/HIV infection
4. Leprosy
5. Chickenpox
6. Cholera
7. Dengue
8. Dengue haemorrhagic fever
9. Diphtheria
10. Encephalitis
11. Viral hepatitis
12. Malaria
13. Poliomyelitis
14. Plague
15. Typhoid
16. Paratyphoid
17. Mumps
18. Hand, foot and mouth disease
19. Yellow fever
20. Measles
21. Rubella
22. Legionellosis
23. Nipah virus infection
24