Nutritional Assessment - Trinity Valley Community College
advertisement

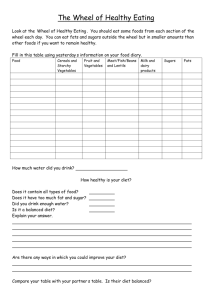
TRINITY VALLEY COMMUNITY COLLEGE ASSOCIATE DEGREE NURSING ASSESSMENT OF A CLIENT WITH A COMPLEX HEALTH CARE PROBLEM PART A: NUTRITIONAL ASSESSMENT Student’s name______________________________ Please answer in complete sentences as to what the client stated. DIET HISTORY 1. Are you currently on a diet prescribed by a physician? If so, what type? Why was this diet prescribed? Is anyone else in your household on this diet? If diet is not prescribed, why is this diet being recommended by student? 2. How would you describe your appetite? 3. Do you adhere to your recommended diet? If no, why not? If yes, explain how you adhere to your diet? 4. Have you discussed this diet with a registered dietician? If so, when? How many visits? Do you have any handouts or written information about your recommended diet? 5. Who does your grocery shopping? Where do you shop? How often do you go to the grocery store? 6. Do you have any financial problems when buying food for your recommended diet? How much food do you spend on food for one (1) week? 7. Who prepares your meals? Do you have any difficulties preparing your meals? 8. Do you have any difficulty eating/feeding yourself? Do you have any dental problems? 9. What are your usual meal times? How long are your meals? Do you regularly eat alone or with others? Where do you eat most of your meals? Do you watch TV while you are eating? 10. Do you eat snacks? When and what types of snacks do you eat? 11. What do you usually drink with meals? How much do you drink in a 24-hour period? What types of drinks do you usually have? 12. Describe ethnic/cultural spiritual beliefs and practices that affect what you eat. 13. What foods do you particularly like? 14. What foods do you dislike? 15. How do your eating habits change when you are emotionally upset? 16. Describe your usual exercise during a day. During the week? (Type, intensity, duration, frequency) 17. Are there any other facts about your lifestyle that you think might be related to your nutritional health? 18. Have you recently lost or gained more than 10 lbs. If yes, explain the surrounding circumstances (including associated illness, dietary habits, changes, and time frame). 19. Do you have available family members/significant others as a resource for you? If yes, please describe who and what type of support. 20. How often do you eat out? Where do you eat (restaurants, fast-food)? What do you typically order at the establishment? Does this adhere to your recommended diet? ASSESSMENT OF CLIENT’S KNOWLEDGE OF RECOMMENDED DIET (this is what your client stated) 1. What types of foods are allowed, not allowed, and what foods are restricted in your recommended diet? 2. How do you decide what you will eat at each meal? 3. Do you read food labels? How often? (Could have client demonstrate reading food labels). Identify which type of labels the client looks for in food products? Is this appropriate for recommended diet? DIETARY INTAKE ASSESSMENT 1. Instruct your client to keep a 3-day food diary. Complete a computer analysis of 3-day diary and analyze the results. Include the 3-day diary and the computer analysis. 2. Summarize amount, frequency of foods, and portions consumed during the three days (evaluate 3-day diary). Please note that combination foods should be listed under each specific category (i.e. pizza, casseroles). Milk (type): ______________________ Cheese: _______________________ Red meat: ________________________ Grains: ________________________ Poultry: __________________________ Eggs: _________________________ Pork: ____________________________ Margarine: _____________________ Fish: ____________________________ Cooking oil: ____________________ Protein substitute: __________________ Sugar: _________________________ Potatoes/rice/pasta (type): ____________ Butter: _________________________ Fruits (type): ______________________ Vegetables (type): ________________ Desserts (type): ____________________ Candy: _________________________ Beverages (type): __________________ Alcohol intake (type): _____________ Frequency of times not preparing/eating at home: __________________________________ 3. List any other foods pertinent to the client’s recommended diet that you identified after evaluation of the 3-day food diary. 4. Do you take any vitamins/herbs/iron/calcium on a daily basis? 5. Explain all medications that the client takes that affect the complex health problem for which the diet is recommended. Discuss the dietary implications of the medications. 6. List any food allergies the client has and any drug allergies. ANALYSIS OF FOOD DIARY On a separate sheet of paper(s) evaluate the food analysis of your client’s 3-day diary. Compare the client’s 3-day diary with the recommended diet. Identify what foods your client should continue to eat and what modifications your client should make to adhere to the recommended diet. Highlight the pertinent information on the 3-day diary. Discuss in detail what modifications the client needs to make including nutritional teaching. Provide an individualized 2-day meal plan reflecting the client’s 3-day food diary. n:soph/fall/nutritional assessment Revised 07/13