Common Chart of Accounts - Nationwide Service Framework Library
advertisement

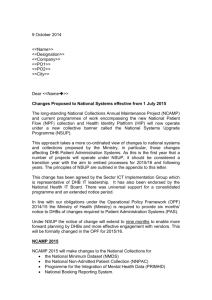
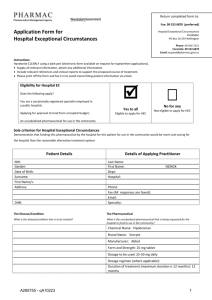
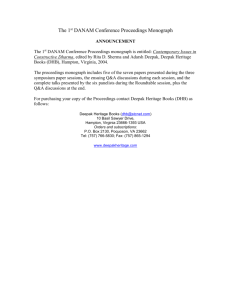
DHB/MoH Common Chart of Accounts Version 7.0 Issued December 2011 Valid for reporting from 1 July 2012 Contents 1. STATEMENT OF PURPOSE ............................................................................................................3 2. APPLICATION ..................................................................................................................................3 3. CHART MAINTENANCE AND CHANGE REQUESTS....................................................................3 4. GENERALLY ACCEPTED ACCOUNTING PRACTICE ..................................................................3 5. RELATIONSHIP OF THE CCoA TO THE COMMON COSTING STANDARDS .............................4 6. STRUCTURE AND DEFINITIONS ...................................................................................................4 6.1. GENERAL LEDGER STRUCTURE: ..........................................................................................4 6.2. SCOPE OF THE DHB/MoH CCoA ............................................................................................5 6.3. MANDATORY LEVELS .............................................................................................................5 6.4. STRUCTURE HIERARCHY .......................................................................................................7 6.5. NUMBERING SCHEME .............................................................................................................8 6.6. DEFINITIONS: MAJOR CATEGORY, SUB CATEGORY & GROUP ........................................8 7. DHB/MoH FINANCIAL REPORTING FRAMEWORK ...................................................................11 7.1. INTRODUCTION......................................................................................................................11 7.2. DHB FRAMEWORK .................................................................................................................11 7.3. PRINCIPLES ............................................................................................................................12 7.4. REPORTING REQUIREMENTS..............................................................................................12 7.5. MONTHLY FINANCIAL REPORTING TEMPLATE .................................................................13 7.6. MONTHLY FINANCIAL REPORTING TEMPLATE CODES ...................................................15 8. CONSOLIDATED CROWN FINANCIAL STATEMENTS ..............................................................16 8.1. REQUIREMENT .......................................................................................................................16 8.2. ELIMINATING INTER-CROWN ENTITY TRANSACTIONS ....................................................16 APPENDICIES APPENDIX A: DETAILED COMMON CHART OF ACCOUNTS (refer separate Excel Workbook) APPENDIX B: SUFFIX NUMBERING FRAMEWORK APPENDIX C: PERSONNEL / COMMON COSTING POOLS DHB/MoH Common Chart of Accounts 1. STATEMENT OF PURPOSE 1.1 The purpose of the DHB/MoH Common Chart of Accounts (CCoA) is to provide a nationally consistent coding system for the recording of transactions by District Health Boards (DHBs) and the Ministry of Health (MoH). 1.2 The CCoA will allow common presentation, interpretation and use of financial information produced by DHBs. 1.3 The CCoA supports and provides a stable platform for the Common Costing Standards and all cost reporting, comparative analysis and benchmarking. 2. APPLICATION 2.1 The CCoA is a mandatory accountability document under the Nationwide Service Framework. 2.2 The entire CCoA applies to all District Health Boards, their subsidiaries and other 100% Crown-owned health related entities, including shared services agencies from 1 July 2002. 2.3 The Ministry of Health is required to use the CCoA for recording Provider payments categorised in the 6000 series of codes. This is the shared part of the CCoA. 3. CHART MAINTENANCE AND CHANGE REQUESTS 3.1 The CCoA is maintained under the authority of the CFO Technical Accounting Group (TAG). 3.2 The secretariat function for the chart is provided by the NHB, DHB Performance section. 3.3 TAG manages a CCoA working group that is intended to be representative of the sector with an appropriate skill mix to cover all aspects of the chart. The structure and personnel will be reviewed annually as part of the CCoA review process. 3.4 The CCoA will be dynamic so it can support the varying financial reporting needs of DHBs and MoH. Change requests and issues are to be directed to the Chair or Secretary of the working group. Requests must be submitted by 31 July of each year. The CCoA will be updated annually each October. 4. GENERALLY ACCEPTED ACCOUNTING PRACTICE 4.1. The CCoA is intended to comply (or support compliance) with Generally Accepted Accounting Practice (GAAP) as described in accounting standards promulgated by the New Zealand Institute of Chartered Accountants. CCoA Version 7.0 3 5. RELATIONSHIP OF THE CCoA TO THE COMMON COSTING STANDARDS 5.1. The conceptual framework of the DHB/MoH CCoA, and their relationship to the Common Costing Standards is depicted below. FIGURE 1 – Conceptual Framework of DHB/MoH CCoA with the Common Costing Standards Purchase Units Patients Intermediate Products Fully Costed Direct R/C’s Direct R/C’s DHB COMMON CHART of ACCOUNTS Indirect R/C’s General Ledger DHB Common Chart of Accounts COMMON COSTING STANDARDS 6. STRUCTURE AND DEFINITIONS 6.1 GENERAL LEDGER STRUCTURE The Chart of Accounts: The Multi-segment General Ledger coding number, which describes some, or all of the following elements: Entity (Organisation) Service (or Division) Responsibility Centre Account Number Any Suffixes CCoA Version 7.0 4 Example (structure for use at Waitemata DHB): 02 – 70 – 740 – 2468 – 00000 Segment 1 Organisation Segment 2 Service Waitemata DHB Clinical Support Segment 3 RC Segment 4 Account Number General Laboratory Phlebotomist Segment 5 Suffix Accident Leave This example explains: Waitemata DHB (Organisation) Clinical Support (Service) General Laboratory (RC) Phlebotomist Payroll (Account) Accident Leave (Suffix) 6.2 SCOPE OF THE DHB/MoH CCoA The Scope of this Standard is to define a consistent structure and methodology for the account number segment of the multi segment general ledger coding number (segment 4 as circled in the above example). The definition and use of organisational unit segments (segments 1, 2 and 3 in the above example) is at the discretion of individual DHB. The use of the account suffix segment (segment 5 in the above example) is optional. Account suffixes may be implemented and used to breakdown costs to a more detailed level. The account number segment consists of up to 4 mandatory levels. These are described below: 6.3 MANDATORY LEVELS The following mandatory levels apply to DHBs. Level 1 – Major Category: 1000’s Revenue 2000’s 2001 2002-2199 2200-2399 2400-2599 2600-2799 2800-2999 3000’s 4000’s 5000’s 6000’s 8000’s 9000’s Expenditure Personnel Medical Personnel Nursing Personnel Allied Health Personnel Support Personnel Management/Administration Personnel Outsourced Services Clinical Supplies Infrastructure & Non-Clinical Supplies Provider Payments (joint DHB/MoH use) Internal Allocations Balance Sheet CCoA Version 7.0 5 Level 2 – Sub Category: A significant subdivision inside a Level 1 Major Category. Example: Within Level 1 Major Category ‘Revenue’, Level 2 identifies the following divisions: Government and Crown Agency Sourced, Patient/Consumer Sourced and Other Income. NOTE: Not all categories (Level 1) have Sub Categories (Level 2). Level 3 – Group: Defines significant subdivisions inside a Level 2 Sub-Category. Example: Within Level 1 Sub Category ‘Allied Health’ Level 3 identifies the following divisions: Therapies, Psychologists, Social & Community, Laboratory, Payroll, Pharmacy, Radiology & Radiotherapy, Ambulance & Paramedical, Other Allied Health & Allied Health-Other Costs. Level 4 – Posting Level Account: Defines the account into which transactions are posted and accumulated. Example: Within Level 3 Group ‘Laboratory’, Level 4 identifies the following divisions: Laboratory Technologists, Laboratory Assistants and Phlebotomists. NOTE: There are a number of level 4 accounts (particularly in the Payroll Expenditure Major Categories) which can be omitted, if a level 5 account (i.e. suffix) is used. Level 5 – Suffix Account: Defines the sub accounts within the posting account, which in turn are used for posting transactions. This level is optional, as different DHB G/L systems may not be able to cope with Suffixes. The suffix allows individual DHBs to track specific items, as per individual organisational need. Payroll Example: Within Level 4 Account ‘2471 - Senior Pharmacist’, Level 5 includes the following divisions in addition to Regular time payment: Accident Leave, Annual & Long Service Leave, Other Leave, Sick Leave, Statutory, Training/Study Leave, Allowances, etc. See Appendix A: Chart of Account Detail. Non-Payroll Example: Within the Level 4 Account ‘3404 – Central Nervous System Pharmaceuticals’, suffix accounts 01 and 02 could be used to refer to Clozapine and Olanzapine respectively (Schizophrenia drugs – tracked due to their high costs). 6.4 STRUCTURE HIERARCHY The hierarchical framework for determining an account number is illustrated in the flow diagram below for a Registered Nurse Long Service Leave accrual. CCoA Version 7.0 6 Framework for Determining Account Number - Statement of Financial Performance Revenue Revenue or Expense? Similar logic tree Expense Payroll Outsourced Services Clinical Supplies Infrastructure & NonClinical Supplies Provider Payments Internal Allocations Account Number ‘Build’ Occupational Group? Medical Account Number: 2_ _ _ Nursing Allied Health Support Management / Administration Account Number: 22 _ _ (with suffix) or 23 _ _ (non-’regular’ pay without suffix) Professional Group? Senior Nurse Registered Nurse Enrolled Nurse Senior Midwife Registered Midwife Health Service Assistant Account Number: 2210 (with suffix) 2210 or a 2300 if not ‘regular’ pay type Pay Type ? Ordinary Annual & LSL Sick Leave Overtime Account Determined Penal Account Number: with Suffix: without Suffix: Etc 2210xx 2347 6.5 NUMBERING SCHEME Specific 4 digit account numbers have been prescribed in the DHB/MoH CCoA. Where it has been necessary for DHB’s to have further flexibility of data capture and reporting then 2 options exist: CCoA Version 7.0 7 1. Use of Suffix Accounts (both Statement of Comprehensive Income and Statement of Financial Position) 2. Use of Ranges. For specific account codes (i.e. bank accounts), a range of accounts has been specified for usage. This is the only situation for using accounts other than prescribed in this standard. 3. The numbering of the accounts has been done to accommodate different general ledger systems, and their technical specifications: Parent (or Summary) accounts at major categories, and grouping levels, are required by some G/L systems. Thus, the parent account number (i.e. 4th digit = 0, 1, or even 2) has been reserved from use by a (level 4) posting level account. Parent accounts may also use the account number ending in ‘99’. Hence this account number has also been reserved. 6.6 DEFINITIONS: MAJOR CATEGORY, SUB CATEGORY & GROUP Refer to New Zealand Institute of Chartered Accountants Financial Reporting Standards for generic definitions. STATEMENT OF FINANCIAL PERFORMANCE Revenue External sources of revenue or cost recovery to the DHB. Excludes internal charging or billings at a consolidated level. Government and Crown Agency Sourced Revenue This consists of revenue sourced from central government and its agencies. following revenue streams: MoH – Vote Health MoH – Personal Health MoH – Mental Health MoH – Public Health MoH – Disability Support MoH – Maori Health Inter District Flows Other DHB’s Government (non DHB’s) It includes the Patient / Consumer Sourced Revenue Other Income CCoA Version 7.0 8 Expenditure Personnel Direct costs for those staff directly employed (i.e. those people with a legal employment relationship) by the DHB. This category therefore excludes contractors. Medical Personnel All staff employed primarily as practicing physicians and/or surgeons. This does not include medical staff employed solely in a management role. Nursing Personnel All qualified nursing staff, registered and enrolled, and nursing aides. This does not include nursing staff employed solely in a management role. The CCoA has categorised Nursing by professional occupation group, rather than by location/health specialty. Allied Health Personnel All professional health occupations (excluding medical or nursing staff) employed to provide patient care, either directly or indirectly. Support Personnel All staff employed to maintain the infrastructure and facilities of the DHB. Management/Administration Personnel All management, clerical and corporate staff. Includes any clinical staff employed solely in a management role. Outsourced Services Purchase of external staff through bureau or other employment organisation (i.e. contractors, where a legal employment relationship does not exist). Services provided here are input-based (i.e. inputs into the process of delivering patient care) rather than output based. Medical Personnel Nursing Personnel Allied Health Personnel Support Personnel Management/Administration Personnel Outsourced Clinical Services Provision of entire diagnostic or treatments to the DHB, as an outsourced service (i.e. more than just the pure labour). Examples include laboratory tests, MRIs, CTs, etc. Services provided here are input-based (inputs into the process of delivering patient care i.e. inputs into a larger health output/purchase unit) rather than outputs based (these are coded to the Provider payments section). Outsourced Corporate Services Provision of entire (or mostly entire) Corporate services to the DHB, as an outsourced service (i.e. more than just the pure labour). Examples include Finance, Human Resources, Information Technology, and supply chain (including procurement). (Note that partial IT Bureau and Outsourcing Fees are coded under a/c 5305). Outsourced Services – Funder Services To be utilised for outsourced costs of Provider Audit & Monitoring and Service Monitoring & CCoA Version 7.0 9 Assessment as well as the funding of the DHB Shared Services funding agencies. Clinical Supplies Materials or suppliers used or consumed either directly or indirectly, in the treatment of patients. Treatment Disposables Diagnostic Supplies & Other Clinical Supplies Instruments and Equipment Patient Appliances Implants and Prostheses Pharmaceuticals Drug expenditures, classified into individual accounts as categorised by the British National Formulary. Other Clinical & Client Costs Infrastructure & Non-Clinical Supplies All non-payroll expenses related to the operation or maintenance of the organisational infrastructure rather than the direct treatment of patients. Hotel Services, Laundry & Cleaning Facilities Transport IT Systems & Telecommunications Interest & Finance Charges Professional Fees & Expenses Other Operating Expenses Democracy Subsidiaries and Joint Ventures Provider Payments Payments & disbursements made to providers by the Fund within the DHB. These are outputbased payments (in contrast to input based payments as identified in the Outsourced Clinical Services section). Payments are made for an output-based service (e.g. IPA & GP consultations, Community pharmacy drugs dispensed). Personal Health Mental Health Public Health Disability Support Maori Health Internal Allocations Internal charges or Billings between Responsibility Centres (RC’s) within the DHB eliminate at a consolidated level. STATEMENT OF FINANCIAL POSITION Current Assets Non-Current Assets Current Liabilities Non-Current Liabilities Crown Equity CCoA Version 7.0 10 7. DHB/MoH FINANCIAL REPORTING FRAMEWORK 7.1. INTRODUCTION All DHBs acknowledge their financial reporting obligations to the Ministry and other central Government entities. The Ministry will maintain a DHB Financial Reporting Template consistent with the DHB CCoA, in consultation with the DHBs for their completion. The Ministry will act as a single central repository for sector financial information receiving completed monthly templates from each DHB and serving the financial information needs of the Ministry, Statistics New Zealand and The Treasury (for Consolidated Crown Financial Statement information). The 6000 range of the chart is jointly shared by the DHBs/MoH in terms of its structure and use for reporting purposes. 7.2. DHB FRAMEWORK The Cabinet Minutes of 18 May 2000 state that the DHBs shall produce financial statements detailing the performance of three dimensions (arms) of DHBs, as set out below. The rational behind this policy is to maintain the transparency and accountability in the allocation of funds towards DHB Provider and non-hospital service providers. DHB Funder – responsible for the funding of health and disability services. In this arm DHBs report on the receipt of funds from the Crown and the allocation of funds to providers, including to their own hospitals. This excludes governance, management and administration activities relating to allocation of funds. DHB Provider – responsible for governance and management of crown owned hospital and associated health services. Reports on the provision of health and disability services and associated fringe activities such as renting surplus properties etc. DHB Governance & Funding Administration - refers to the governance, management and administration activities relating to the allocation of funds. This includes: DHB Board costs, such as payments to Board members, meeting expenses, etc. all costs relating to the advisory committees to the Board, such as the Community and Public Health Advisory Committee, Disability Support Advisory Committee and Hospital Advisory Committee. The Hospital Advisory Committee could fit in DHB Provider, but the funding for the committee is included in the overall funding for DHB Governance and Funding Administration the corporate costs of servicing the Board (Board secretariat function) the share of the CEO costs relating to DHB Funder the corporate costs of working on DHB accountability requirements specific costs of managing DHB Funder, such as needs assessment, contracting with providers and monitoring the providers the share of corporate costs in managing DHB Funder, such as share of Finance, IT, etc. costs relating to shared services agencies the cost of internal audit which works at the Board's behest. CCoA Version 7.0 11 This excludes: the share of CEO costs relating to DHB Provider the share of corporate costs relating to DHB Provider. 7.3. PRINCIPLES The reporting requirements are based on the following principles: 1) A DHB is one organisation. The overall benefit of a DHB should take precedence to the benefit of a particular dimension of the DHB. However, Government wants transparency between the three dimensions of Funds, Governance & Funding Administration and Provision. 2) DHBs must report on the performance of DHB Funder. DHBs must report on the allocation of funds to the providers. Reporting on DHB Funder should clearly identify how funds are spent in each of the five service areas: (i) Personal Health (ii) Mental Health (iii) Disability Support Services (iv) Public Health and (v) Maori Health. 3) DHB Funder will undertake all funding activities. DHB Funder will hold all the risk relating to funding activities and shall not transfer it to DHB Provider. 4) DHBs must report on the use of funds allocated to DHB Governance & Funding Administration. 5) DHBs must report on the performance of the DHB Provider. DHBs must report on use of funds allocated to the providing arm of the DHB, assets employed and liabilities or risk entered into in the provision of services. 6) Retained earnings of separate arms of DHBs should be recorded separately and should be reinvested or used to manage the risk of respective arms. 7) DHBs should provide sufficient information to produce consolidated reports on the performance of a given DHB, the sector and the government. 8) The reporting system shall be effective and efficient and build on what already exists in the sector including the CCoA. 9) Sector Services will act as paying agents for the DHBs and will process all provider contracts and payments including those with other DHBs. 10) DHBs will maintain the Service Level Agreement (SLA) between DHB Funder and DHB Provider (and can provide proforma journals to account for SLA). The nationwide service framework and national pricing will be relevant to DHBs in setting the SLA. 7.4. REPORTING REQUIREMENTS DHBs are required to produce separate financial statements for the three dimensions or arms and other financial information as set out below: CCoA Version 7.0 12 DHB Funder - Statement of Comprehensive Income. DHB Governance & Funding Administration - Statement of Comprehensive Income. DHB Provider - Statement of Comprehensive Income for DHB Provider. A set of adjustments that will enable the production of consolidated statements for the whole of the DHB. Consolidated Statements of Comprehensive Income, Position, Changes in Equity and Cash Flow for the DHB as a whole. Information on inter-DHB and inter-Crown Entity transactions and balances. Statement DHB Funder DHB Provider DHB Governance & Funding Admin Consolidation Eliminations Consolidated Statements Statement of Comprehensive Income Statement of Financial Position Combined Statement Statement of Changes in Equity Combined Statement Cashflow Statement Combined Statement Supplementary information Inter-DHB and inter-Crown Entity transactions 7.5 MONTHLY FINANCIAL REPORTING TEMPLATE The Monthly Financial Reporting Template is constructed consistent with the CCoA with some supplementary information requirements. The conceptual framework of the Monthly Financial Reporting Template is depicted below. CCoA Version 7.0 13 STATEMENT OF COMPREHENSIVE INCOME DHB Funder Personal Health DHB Governance & Funding Administration DHB Funder Mental Health Level 3 reporting Includes net cost allocation to/from DHB Provider DHB Funder Public Health DHB Funder Disability Support DHB Funder Maori Health DHB Provider Eliminations Level 3 reporting Includes net cost allocation to/from DHB Provider As DHB (internal) Provision is classified in the DHB Funder Financial Statements as Level 4 Provider Payments these amounts need to be eliminated to produce Consolidated Financial Statements DHB Consolidated Either Elimination information or Consolidated information need to be provided Supplementary financial statement disclosure information: Depreciation Interest Costs Etc Supplementary Sector & Crown consolidation information: (Additional L3 or L4 information showing amounts to eliminate) For each ring fence Revenue Level 3 reporting Provider Payments Level 4 reporting STATEMENTS OF CASHFLOW & FINANCIAL POSITION DHB Consolidated Provide consolidated information for all arms. Sector & Crown Consolidation Information: (Additional L3 information showing amounts to eliminate) CCoA Version 7.0 14 7.6 MONTHLY FINANCIAL REPORTING TEMPLATE CODES The following coding system shall be used in financial reporting to the Ministry. The first segment of the code identifies the service area and the dimension of the DHB. The second segment relates to account code, based on the Common Chart of Accounts. The third segment of code identifies inter-DHB and inter-crowns Entity transactions. The CCoA (Appendix C) suggests using suffix numbers to identify the area service code. Any DHBs whose systems cannot use five-digit suffixes should capture the information another way, e.g. the responsibility centre codes could be used to identify the ring fence (the first two digits of the suffix). This would reduce the suffix to three digits. Then the data needs to be mapped to report to the Ministry. XX – XXXX - XXXXX As per DHB CCoA Suffix to identify InterDHB/Crown Entity Arm/Service Area DHB Funder, DHB Provider, Personal Health, etc. Account Code as per CCoA (generally Level 3) Arm/Service Area Code 00 01 05 10 20 Description Consolidated Accounts Intra-DHB Consolidation Eliminations DHB Governance & Funding Administration DHB Provider DHB Funder 30 40 60 70 80 90 Maori Health Personal Health Disability Support Services Public Health Mental Health Other 95 97 98 Inter-DHB elimination 130 140 Mental Health supplementary Inter-Crown eliminations CFIS CCoA Version 7.0 Maori Health Personal Health 15 160 170 180 190 Disability Support Services Public Health Mental Health Other 8. CONSOLIDATED CROWN FINANCIAL STATEMENTS 8.1. REQUIREMENT The Public Finance Act 1989 and the Fiscal Responsibility Act 1994 require the government to produce actual and forecast financial statements in accordance with Generally Accepted Accounting Practice (GAAP). GAAP requires full line-by-line consolidation of State Owned Enterprises (SOE’s) and Crown Entities (CEs). The Ministry will act as intermediary to collect information for Treasury on the DHB sector. This eliminates the need for the DHBs to report to Treasury directly. The information for the Crown financial statements incorporates the DHB consolidated financial statements supplemented by further information requirements as detailed in the reporting template. Some of this information will be available from the DHB General Ledger whilst some will need to be sourced from sub-ledgers of the General Ledger and other sources. 8.2. ELIMINATING INTER-CROWN ENTITY TRANSACTIONS Treasury requires information on all material inter-Crown Entity transactions to produce consolidated Crown financial statements in accordance with the Crown accounting procedure. Some inter-Crown Entity transactions may not be material to individual organisations, but in aggregate they may be material to the Crown accounts as a whole. (For example, transactions with NZ Post.) The eliminations required for the Crown financial statements are set out in the Intercrown worksheet of the reporting template. This details all the Government Departments, Crown Entities and State-Owned Enterprises for which transactions and balances need to be identified. Please refer to the document “Requirements and Guidelines for Using Templates” for detailed guidance on reporting Inter-Crown transactions. CCoA Version 7.0 16 APPENDIX B: SUFFIX NUMBERING FRAMEWORK Suffix Numbering Framework (Optional) This appendix provides an optional (Level 5) Suffix Numbering Framework that may be adopted by individual DHBs for the following reasons: 1. The DHB CCoA provides this option for Payroll non-ordinary Time Payments in lieu of a Level 4 Account. 2. The recording of all financial information in the DHB CCoA at a Level 4 (Posting Account Level) is insufficient, without supplemental information, to capture the details required to record all transactions and balances with: a) b) c) 3. DHB and other Health Sector Entities – to facilitate consolidated Sector Financial Statements. Other Crown Entities – to facilitate consolidated Crown Financial Statements; and The five Health Fund service areas and MoH sub-groups for Provider Payments. Sector Services record the nature of Provider Payments i.e. whether they are fixed payment, demand driven (uncapped) or variable payment (capped). The numbering in this framework will parallel that used by the Monthly Financial Reporting Template to capture the detailed information they require, under 2 above. Suffix No’s 1-99 Used by: Payroll Suffix Accounts 41 Accident Leave 42 Annual Leave 43 Other Leave 44 Sick Leave 45 Statutory (including Time in Lieu) 46 Training/ Study Leave 47 Long Service Leave 52 54 56 Allowances Overtime Penal 61 63 65 ACC Levy Fringe Benefit Tax Meals 66 67 68 69 70 Government Kiwi Saver contributions Superannuation GSF Contribution Expense Defined Contribution Plan Defined Benefit Plans 71 72 74 Training – Clinical Training Agency Training – General External Clinical Supervision 76 Professional Membership Fees & Costs 87 89 Recruitment Expenses & Advertising Relocation Expenses 95 96 97 98 Gratuities Grievance Settlements Payment on return from Maternity Leave Redundancies 30200-88999 Service Area NB Digit number indicates which part of the 5-digit suffix code is being referred to. The Ministry Service Area 1st & 2nd digit: 30 Maori Health 31 By Maori for Maori (Services that have Maori governance & management structures) 32 Maori Specific (Services from a mainstream provider, but they are separately identified as being targeted specifically for Maori) 33 Maori Health Sector Development 34 MAPO 35 Treaty 40 41 42 43 44 45 46 47 48 49 51 53 55 Personal Health Child and Youth Maternity and Neo-natal Oral Health Pacific People’s Health Primary – General Practice Services Primary – Population-Based Services Primary – Referred Services Management Radiology Pharmac Medical Surgical High Cost / Case Management Inter Regional / Inter District Flows 60 61 63 65 66 67 Disability Support Age Related Intellectual Physical Children General 70 71 72 74 75 76 77 78 79 Public Health Projects Public Health Contracts – mainstream Maori Specific Contracts Pacific Island Specific Contracts Personal Contracts – Mainstream Personal Contracts – Maori Specific Personal Contracts – Pacific Island Specific Other 80 81 82 83 84 Mental Health Inpatient Services Community Services Community Residential New Anti-Psychotics 85 86 87 88 Workforce Development Other Mental Health Maori Mental Health Pacific Island Mental Health 3rd digit: Payment Type: 2 = Fixed Payment 3 = Demand Driven (Uncapped) 4 = Variable Payment (Capped) 4th & 5th digit: Entity: 00 = Non DHB 01 = Northland DHB 02 = Waitemata DHB 03 = Auckland DHB 04 = Counties Manukau DHB 05 = Waikato DHB 06 = Bay of Plenty DHB 07 = Lakes DHB 08 = Tairawhiti DHB 09 = Taranaki DHB 10 = Hawke’s Bay DHB 11 = MidCentral DHB 12 = Whanganui DHB 13 = Capital & Coast DHB 14 = Hutt DHB 15 = Wairarapa DHB 16 = Nelson Marlborough DHB 17 = West Coast DHB 18 = Canterbury DHB 20 = South Canterbury DHB 21 = Otago DHB 22 = Southland DHB 23 = NZ Blood 25 = Southern DHB 9. APPENDIX C: PERSONNEL / COMMON COSTING POOLS Personnel / Common Costing Pools Personnel account definitions (with corresponding common costing standard cost pool) MEDICAL (ABFAC Standard, Schedule 7.7.3, 7.7.3a, 7.7.6, 7.7.10, 7.7.11, 7.7.15) Specialist Medical Officer MOSS General Practitioners Registrars House Officers Probationers and Interns NURSING (ABFAC Standard, Schedule 7.7.2, 7.7.8, 7.7.10, 7.7.11, 7.7.12, 7.7.13, 7.7.14, 7.7.15, 7.7.16) Nurse Practitioners Senior Nurses - this includes Senior Nurses, Nurse Managers, and Nurse Educators Registered Nurses Enrolled Nurses Nurse Assistants Registered Midwives Internal Bureau Nurses Health Assistants ALLIED HEALTH (ABFAC Standard, Schedule 7.7.7) Audiologists Child Therapists Dental Therapists Occupational Therapists Physiotherapists Podiatrists Speech Therapists Therapist Aids/Assistants Therapist Interns/Trainees Other Therapists Case Managers Community Support Workers Cultural Workers Health Education Workers Health Promotion Officers Health Protection Officers Home Aides Psychologists Psychotherapists Recreation/Training/Welfare Officers Social Workers Trainee Psychologists Youth Workers LABORATORY (ABFAC Standard, Schedule 7.7.4) Laboratory Technologists Laboratory Assistants Phlebotomists PHARMACY (ABFAC Standard, Schedule 7.7.9) Pharmacists Pharmacist Interns Pharmacist Technicians & Assistants RADIOLOGY & RADIOTHERAPY (ABFAC Standard, Schedule 7.7.6) MRTs & Sonographers MRTs & Sonographer Students AMBULANCE & PARAMEDICAL Ambulance Officers Intermediate Care Ambulatory Officers Paramedics OTHER ALLIED HEALTH Technicians Dietitians Hearing/Vision Testers Scientific Officers & Researchers Other Allied Health Staff SUPPORT STAFF (No Cost Pool) Hotel Services Supervisors Cleaners Cooks Drivers Kitchen Assistants Orderlies Security Patrolmen Storemen Other Hotel Services Workers Laundry & Sterile Supply Supervisors Laundry Workers Sterile Supply Assistants Biomedical Technicians Carpenters Electricians Fitters Labourers & Groundsmen Maintenance Supervisors & Engineers Painters Plumbers/Boilermen Interpreters Civil Defence & Disaster Response Other Support Staff MANAGEMENT/ADMINISTRATION STAFF (No Cost Pool) Executive Managers Supervisors Professional staff Fixed Term Clinical Co-ordinators Administrative, Clerical & Secretarial staff – Clinical Administrative, Clerical & Secretarial staff – Non-Clinical