physiology_lec26_22_3_2011
advertisement

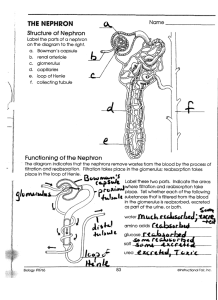
بسم هللا الرحمن الرحيم Lecture no.26 22-03-2011 Renal system 1st: we'll talk about the handling of substances in the nephron: 1) some substances are filtered & totally excreted such as Inulin. (the concentration of the substance in Bowman's space = it's concentration In blood plasma.) 2) some substances are filtered & totally reabsorbed such as Glucose. Note that the plasmic clearance of GLU=0.. Remember… Plasmic clearance of a solute: the amount of plasma cleared from X substance per minute time. & it can be measured by the equation: Cx =( Ux + V)/ Px Where Ux : conc. Of X in urine V : urine flow Px : conc. Of X in systemic blood flow 3) some substances are filtered & secreted (from the peritubular fluid in to the filtrate.) 4) Finally..some other substances are filtered, reabsorbed & secreted depending on the need of the body. 2nd:Glomerular filtration rate (GFR): -Glumerular filtration rate: volume of fluid filtrated in to the Bowman's space per unit time. - We can measure GFR by calculating Inulin clearance : Plasma entering the glumerulus =660 ml ≈ 700 ml Inulin injected = 6 mg / 100 ml so that in 660 ml of plasma,the total amount of Inulin injected =(40-50) now..the blood entering the glumerular filtrate =125 ml/min the amount of Inulin =50 mg /100 ml so that in 125 ml of plasma…inulin excreted =62.5 mg / min 1 Uin=62.5 mg / ml V= 1 ml/min Pin = 50 mg / 100 ml Inulin clearance = GFR = 62.5 *100 *1 = 125ml/min 50 ** THE characteristics of substances suitable for measuring GFR: 1.freely filterable (conc. in glumerular filtrate=conc. in plasma) unlike lipoproteins. 2.Not reabsorbed or secreted by renal tubules. 3. Not metabolized by the kidneys. 4. substances must be physiologically inert ( not toxic & have no effect on filtration rate ). Any substance that fits to these criteria could serve as a glumerular marker For measuring GFR..such as Inulin. Factors affecting the GFR: 1. Changes in the renal blood flow. 2. Changes in the Glumerular capillary hydrostatic pressure PGC(either effected by changes in the systemic blood flow pressur or afferent & efferent arteriolar pressure:-afferent a. constriction blood flow in the glumeruli decreases PGC decreases net filtration pressure decreases. -efferent a. constriction PGC increases net filtration pressure increases.) 3. Changes in the concentration of proteins which affect the colloidal osmotic pressure. 4. Changes in Bowman's space hydrostatic pressure PBS ( edema in the kidneys, & ureter obstruction.) 5. An increase in the permeability of blood vessels. 6. A decrease in the total area of glumerular capillaries due to( diseases or partial nephroctomy.) Remember: Basic renal processes: 1. Filtration. 2. Reabsorption. 3. Secretion. 2 - Any substances reabsorbed or secreted through the tubules have to pass either in between cells ( Paracellular pathway )(1) through tight junctions, Or through cells (Transcellular pathway) (2). - Na+ handling in nephrons: -Na+ reabsorption along the nephron: 1. The proximal tubule: reabsorbs the largest fraction of filtered Na+ ≈ 67%. 2. Henle's loop: Thick ascending limb reabsorbs ≈ 25% of filtered Na+, while little reabsorption occurs in thin ascending & descending limbs due to low permeability to electrolytes and water. 3. Distal tubules: reabsorbs a small fraction of filtered Na+ ≈ 5%. 4. The collecting tubules (cortical part & medullary collecting tubules) reabsorb approximately 3% of filtered Na+. **The most important functions of nephrons is the REABSORPTION of NA+(because water reabsorption depends on Na+ reabsorption). So…on daily basis kidneys must make sure that + The Na filtered = The Na+ excreted through a process called Na+ Balance, in order to keep the Na+ concentration in the molecules & in the blood almost constant. - Different nephron segments use different transporters or channels for transcellular Na+ reabsorption… 1. In proximal tubules : Firstly, active Na+ reabsorption is electrogenic. In the apical membranes of the proximal tubule Na enters to cell coupled to organic solute transport such as(glucose, aminoacids, phosphate , sulfate, or lactate…etc.) (3), Na+ entry is also coupled to the extrusion of H+ (through Na-H exchanger). (1).Paracellular transport is only passive and driven by the gradients secondary to transcellular transport mechanisms. (2).Transcellular route is both active and passive and based on the activity of transmembrane pumps, channels, and carriers. (3). Glucose, amino acids, inorganic phosphate, and some other solutes are reabsorbed via secondary active transport through cotransport channels driven by the sodium gradient out of the nephron. 3 Second, The most common drive for the reabsorption is the basolateral located Na-K-ATPase (sodium-potassium pump), which is responsible for the 2nd step of Na+ reabsorption moving three sodium atoms out of the cell in to peritubular capillaries( back to blood) and two potassium atoms into the cell, the energy derives from the hydrolysis of one ATP molecule. ** 2 Factors favor the entry of Na+; Electrochemical gradient ( the concentration of Na+ as well as the charge "electrical difference across the membrane"). When Na+ enters the cell under the effect of these 2 factors, Energy is produced (by the hydrolysis of ATP), & that energy is utilized to carry Glu, aminoacids,phosphate…etc. Or in opposite direction H+. ** Cells have to keep the electrochemical gradient constant ( Na+ should always be more outside, while K+ should be more inside the cell.), & once the equilibrium is disturbed the Na-K-ATPase pump functions. ** Other substances leave under the effect of their concentration gradient through facilitated diffusion. 4 Summation of Na+ reabsorption in proximal tubules: 1. Na enters to cell coupled to organic solute transport such as(glucose, aminoacids, phosphate , sulfate, or lactate…etc.) 2. The electrochemical gradient changes(+ve net charge due to entry of Na+) 3. Na-K-ATPase pump functions(moving 3 Na+ out of the cell in to the peritubular capillries, & 2 K+ in to the cell). 4. Paracellular & transcellular passage of Cl- too. 5. [ NaCL ] increase within the cell Osmotic pressure rises Mass movement of water through the cell which drags along Ca2+, Mg2+ & K+ across tight junctions in a process called SOLVENT DRAG. 2. In Henle's loop(1): The main reabsorption of Na+ occurs in the thick ascendind limb, where approximately 20% of filtered Na+ is reabsorbed, & consequently approximately 17% of water is reabsorbed. Reabsorption occurs in 2 pathways: -Transcellular pathway: Reabsorption of Na+ occurs through Na-K-Cl cotransporter(specific carrier NKCC2) which transports 1 Na+, 1 K+ & 2 Cl- , driven by the concentration gradient of both Na+ & Cl-. **The electrochemical difference across the membrane causes the Na-K-Cl pump(NKCC2) to function & cause the inward movement of Na+,K+& 2Cl- ions. -Paracellular pathway: K+ is passively transported along its concentration gradient through a K+ channel in the apical aspect of the cells, back into the lumen of the ascending limb. This K+ "leak" generates a positive electrochemical potential difference in the lumen. The electrical gradient drives more reabsorption of Na+, as well as other cations such as magnesium (Mg2+) and importantly calcium (Ca2+). (1)Henle's loop can be divided into five parts: 1.thick descending limb of loop of Henle: has low permeability to ions and urea, while being highly permeable to water. 2.thin descending limb of loop of Henle: has low permeability to ions and urea, while being highly permeable to water. 3.thin ascending limb of loop of Henle: limb is not permeable to water, but it is permeable to ions. 4.medullary thick ascending limb of loop of Henle:mentioned above. 5.cortical thick ascending limb: drains urine into the distal convoluted tubule 5 Absorption in the thick ascending limb ** It's important to REMEMBER that the thick ascending limb is impermeable to water & it's called Diluting segment, & the initial part of the distal tubule is also impermeable to water.. 3. Distal tubules: Reabsorption of Na+, Cl-, Ca2+ & Mg2+ occurs in distal tubules. 4. Late distal & collecting tubules: The collecting duct system is the final component of the kidney to influence the body's electrolyte and fluid balance. In humans, the system accounts for 4-5 percent of the kidney's reabsorption of sodium and 5% of the kidney's reabsorption of water. *Na+ reabsorption in these nephron segments is Transcellular & is mediated by 2 types of cells: - Principal cells: (reabsorbs NaCl & secretes K+) & also reabsorb water under the effect of anti diuretic hormone ADH. -When ADH increase water reabsorption increases. -In the absence of ADH no reabsorption of water in late distal & collecting tubules Diabetes Insipidus. -ß-intercalated cells: Absorbs bicarbonate (HCO3-) & K+, & secretes H+. 6 ** Distal & collecting ducts are important in determining the amount of Na+, K+ & H+ excreted by the kidneys; where they absorb approximately 12% of the filtered Cl- & water(under the effect of ADH) & secrete K+ & H+. **Regulation of Na+-Cl- transport: - Changes in Na+ excretion would occur as a result of changes in GFR if there were no cochemical changes in Na+ reabsorption. - Therefore, whatever was the amount of Na ingested, the amount of Na reabsorbed doesn't change( almost constant=65%). - & even if GFR changes, the amount of Na reabsorbed will still be constant..which is called Glumerulotubular balance(1). **Hormones that affect Na & water reabsorption: 1) Aldosterone : that increases the reabsorption of sodium ions and water, which increases blood volume and, therefore, increase blood pressure. 2) Angiotensin II: -Stimulates the secretion of aldosterone. - Increases the reabsorption of Na at both luminal & basal membranes. - Vasoconstricts efferent arterioles, which increases colloidal osmotic pressure, Leading to decreasing the pressure inside peritubular capillaries. 3) Vasopressin (AVP, VP or ADH): Increases water permeability in the distal convoluted tubule and collecting duct of nephrons, thus promoting water reabsorption and increasing blood volume. 4) Parathyroid hormone: affects the reabsorption of phosphate & Calcium. (1)Glumerulotubular Balance: The constancy of fractional Na reabsorption along the proximal tubule. 7 ** Absorption of fluid in the peritubular capillaries depends on Starling Forces: -Starling forces acting on peritubular capillaries: Fluid movement depends on hydrostatic pressure gradient & osmotic pressure gradient across the capillary membrane. -Filtration force =capillary HP +interstitial=13+15=28 mmHg. -Absorption force =capillary OP+ interstitial HP=6+32= 38 mmHg. -Net Reabsorption force=38-28=10 mmHg. OP 32mmHg Renal interstitial OP 15 mmHg HP=13mmHg peritubular capillary Renal interstitial HP 6 mmHg Remember..Reabsorption of fluid in proximal tubules & Henle's loop depend on Starling forces, while it depends on ADH action in Both Distal & Collecting tubules… **Approximate pressure at different points in vessels & tubules: ( Depending on the slides which weren't available,& I checked the book & the net but I didn’t find anything…:S..so I don’t know if the numbers are accurate..Srry!:S) -Inside glumerulus = 16 mmHg - In the proximal tubule= 18 mmHg - In peritubular capillaries: At the beginning=18 mmHg At the end= 10 mmHg - At the end of distal tubules=10 mmHg - In Interstitial Fluid = 6 mmHg Wish u all the Best..:) Done By:Yasmin Baghal 8