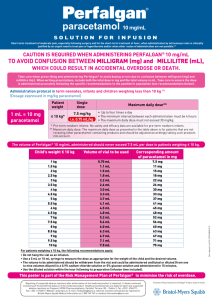
Temperature Conversion Chart
advertisement

Temperature Conversion Chart Centigrade Fahrenheit Centigrade Fahrenheit 34.0 34.2 34.4 34.6 34.8 35.0 35.2 35.4 35.6 35.8 36.0 36.2 36.4 36.6 36.8 37.0 37.2 37.4 37.6 37.8 38.0 38.2 38.4 93.2 93.6 93.9 94.3 94.6 95.0 95.4 95.7 96.1 96.4 96.8 97.2 97.5 97.9 98.2 98.6 99.0 99.3 99.7 100.0 100.4 100.8 101.1 38.6 38.8 39.0 39.2 39.4 39.6 39.8 40.0 40.2 40.4 40.6 40.8 41.0 41.2 41.4 41.6 41.8 42.0 42.2 42.4 42.6 42.8 43.0 101.5 101.8 102.2 102.6 102.9 103.3 103.6 104.0 104.4 104.7 105.1 105.4 105.8 106.2 106.5 106.9 107.2 107.6 108.0 108.3 108.7 109.0 109.4 Pain Assessment Guide Pain Intensity 0-10 0 is no pain, 10 is worst imaginable Words to Describe Pain sharp, dull, burning, shooting, nagging stabbing, aching, squeezing, deep Aggravating and Alleviating Factors How Does Pain affect: sleep, ADLs, appetite, relationships, mood Other Symptoms Constipation, urinary retention, itching, nausea, sleepiness Check V/S, medication history, pain knowledge, Use of alternatives Reassess and Document 60 minutes after PO medication and 30 minutes after IV medication interventions! Measurement for PO Intake Disposable Pitcher 10oz cup 12oz cup 14oz cup Large Milkshake Regular Milkshake Coffee Mug Small Juice Container ½ milk, juice, wine Jello dish Custard Cup Soup Dish Forta Shake Ensure Shake Forta Drink Egg Nogg Ensure Clear/Styrofoam cup 800ml 300ml 360ml 420ml 420ml 240ml 210ml 120ml 120ml 100ml 100ml 180ml 240ml 240ml 240ml 240ml 240ml 210ml REMEMBER: 1 Fluid oz = 30ml Blue 100 “What to Do” Pocket Guide The First 10 Steps 1. Check patient for unresponsiveness and call for help. 2. Check for absence of respiration and pulse. Begin CPR. 3. Initiate Blue 100 by having someone call 1-6666. 4. 2nd responder brings backboard. Begin 2 man CPR. 5. Other Responders, obtain equipment and set up the following: crash cart, defibrillator/monitor, PMR bag, oxygen and suction. Place intubation box at head of bed for Respiratory Therapist 6. Provide patient history to the Code Team on arrival. 7. Assist Code Team as needed. Support family members as needed. 8. Assist with transfer of patient to the ICU. 9. Document in nursing notes patient’s condition, response to code and disposition of patient. 10. Restock crash cart. Dosage Calculations/Abbreviations Weight Volume Gram=g=1 gram Milligram=mg=0.001gram Microgram=mcg =0.001milligram 1000 mcg=1milligram 1000mg=1 gram Liter=L=1L Milliliter=ml=0.001L 1000 ml=1L 1 teaspoon (tsp)=5 ml Amount to be Administered=Dosage Ordered X Quantity Available Dose Available Drip Rate=Volume to be infused X Drop Factor (Gtt/ml) Total Time in Minutes 1 Kilogram(kg)= 2.2 Pounds (lbs) 1inch = 2.54 centimeters (cm Vital Signs Info Diastolic BP < 85 Normal BP 85 - 89 High Normal 90 -104 Mild hypertension 105 - 114 Moderate hypertension 115 Severe hypertension Systolic BP with Diastolic <90 < 140 Normal BP 140-159 Borderline systolic hypertension 160 Systolic hypertension Normal Adult Respiratory Rate 14-18 breaths/minute Normal Adult Pulse Rate 60-100 beats/minute (Average 80 beats/min) Temperature Measurements Oral Temp 98.6° F (37° C) Rectal Temp 99.6° F (37.5° C) Taking Orthostatic BPs; Measures BP change with position changes. Patient may become dizzy and/or faint with position changes that lead to BP drop!! 1. Have patient lie down for at least 3 minutes; Take the BP write it down as lying BP. 2. Assist the patient to sitting. 3. Take the BP after sitting 30 seconds. Write it down as Sitting BP 4. Assist the patient to standing; be aware the patient may become dizzy or faint. 5. Repeat the BP 30 seconds after standing. Write it down as Standing BP. Report values and any dizziness to the nurse Key Resources URMC Intranet: http://intranet.urmc.rochester.edu/Highland Will take you to sites for Highland: Policy Manuals and Procedures Downtime Procedures for Critical Applications Environment of Care Policy Manuel Hospital Policy Manual Highland Promise Human Resources Policy Manual Infection Prevention Policy Manual Nursing Policy and Procedure Manuals Pharmacy Policy Manual Departments Clinical Engineering Construction Clinical Laboratories Pharmacy Formulary Department of Education Provider Privileging Environmental Services Provider Orientation Guide Family Medicine Purchasing Department Human Resources Quality ManagementLibrary Services JCAHO Readiness Materials Management Maintenance Medical Imaging Support Services Nursing Payroll Pharmacy Nutritional Services Key Resources (cont) Resources Intranet Web Services-ISD Infection Prevention How to map a Network Drive? Intranet FAQ www.stronghealth.com Information on services at Strong Health Affiliates, Strong Health providers and patient teaching resources. Highland Digital Library http://eg.miner.rochester.edu/hhdig/hhdig.cgi Micromedex: Access drug information and patient medication teaching sheets. Access through Highland Digital Library. Check Provider’s Privileges: E/Delineate user ID: nursehh Password: nursehh Diverse Patient Resources: http://medlineplus.gov/spanish http://www.cliconhealth.org http://nihseniorhealth.gov http://www.kidshealth.org SPAN: Statewide Peer Assistance For Nurses: A resource for Nurses affected by an alcohol or drug problem. 1-800-457-7261 Unlicensed Assistive Personnel May NOT! ■ Turn on, Adjust or Set oxygen flow ■ Administer Nebulizer treatments ■ Collect blood from Central lines ■ Start IV’s ■ Push PCA button to administer a demand dose ■ Adjust IV pump ■ Silence alarms on any pump ■ Flush any IV line ■ Hang or flush any tube feeding ■ Deep endotracheal suction ■ Insert or discontinue a Foley catheter ■ Disconnect IV tubing for any reason, including changing patient gown ■ Administer medications Disconnect a chest tube from suction Reportable Patient Findings For PCT to Nurse: ~A patient is experiencing difficulty breathing ~A patient is in pain ~Temperature is greater than 38.0C ~Heart rate less than 60 or greater than 100 bpm ~Systolic blood pressure less than 100, greater than 180 ~Oxygen Saturation less than 92% ~Respirations less than 16 or greater than 20 per min. ~Urine output less than 250ml per shift or <30ml/hr ~Inability to draw blood from a patient ~Blood Glucose greater than 250dl or less than 80dl ~A patient having difficulty with chewing/ swallowing ~A patient refused to : Eat Get OOB AM/HS Care Ambulate EKG: Setting up the patient: ■ Enter the patient data prior to attaching leads ■ Check default settings on machine: Speed – 25, Voltage – Full, Standard – Full ■ V1 and V2 should be approximately 2 finger-widths apart, on opposite sides of the sternum ■ Place the electrodes in approximately the same place on the opposite arms and legs To Eliminate Artifact: Check that the patient’s arms and legs are in a relaxed, natural position Place the electrodes on the upper arms and legs Check the electrode representing the lead in which you see artifact. For the limb leads check LA for artifact in Leads I and aVL LL for artifact in Leads II, III and aVF RA for artifact in Lead aVR *Make sure the filter is on Documentation: Make sure the EKG is labeled with the patient’s name, Medical Record #, age, room number, and operator ID # Indicate on the requisition and the EKG if the patient was sitting when the EKG was done V1 - 4th Intercostal space, right sternal border V2 - 4th Intercostal space, left sternal border V3 - Mid way between V2 and V4 V4 - 5th Intercostal space, mid clavicular line V5 - Anterior axillary line, horizontal to V4 V6 - Mid axillary line, horizontal to V4 and V5 Note - V4, 5 and 6 do not follow the 5th intercostal space Care of the Pediatric Patient in a Disaster Average Pediatric Vital Sign Ranges Age Group HR RR BP-S Infant 80-150 25-35 65-100 Toddler 70-110 20-30 90-105 Preschool 65-110 20-25 95-110 School-age 60-95 14-22 100-120 Adolescent 55-85 12-18 110-135 BP-D 45-65 55-70 60-75 60-75 65-85 Pediatric Pulse Oximetry Ranges Normal 95-100% Mild hypoxia 91-94% Mod hypoxia 86-90% Severe hypoxia <86% Pediatric Total Water Requirements/ 24 hours Infant 500 -1300 ml Child <6yrs 1150-2000ml Child>6 2000-2700 ml Pediatric Daily Urine Output/ 24 hours 0.5-2ml/kg/hr depending in age and hydration status Infant 350-550 ml Child 500-1000ml Adolescent 700-1400 ml Fast Safety Assessment Is child breathing? Do you observe any signs of distress *Follow the ABCs of CPR What is the child’s color? Is the child on a monitor? *what is the rate and pattern Any IVs? *note type, rate, site Note last set of VS If abnl, check again When was the last output? Do you observe anything unusual that needs immediate attention? If yes, DO IT NOW PEDIATRIC COMA SCALE Pupils Right Left Eyes Open Spontaneously To Speech To pain None Size Reaction Size Reaction ___ ___ ___ ___ 4 3 2 0 ___ ___ ___ ___ Best Motor Obeys Commands 6 Response: Localizes pain 5 use best Flexion Withdrawal 4 arm or leg Flexion Abnormal 3 or age Extension 2 None 1 Best Response Age appropriate Orientation 5 Confused 4 Inappropriate words 3 Incomprehensible words 2 None 1 Endotrach Tube or Trach T ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ Coma Scale Total (<7=Coma; <3 Deep Coma) Pupil reaction: ++=brisk, +=sluggish, - = No reaction C= eyes closed d/t swelling Cardiac/Apnea Monitors for Pediatrics ECG Monitor: White color right side of chest Green color (or red) ground lower abdomen Black color left side of chest Apnea Monitor: 2 Electrodes 2 fingerbreadths (1 each side of chest) below nipple on midaxillary line Respiratory assessment Cardinal Signs of Respiratory failure: Restlessness, Altered LOC Tachypnea/tachycardia Increased work of breathing -grunting, flaring, retracting Cyanosis Diaphoresis Abnormal breath sounds or findings Crackles-air through fluid Wheezes-air through narrow passage Stridor-high pitched noise d/t upper airway obstruction (mucus/foreign body) Head bobbing-sign of dyspnea Vesicular Breath Sounds Heard over entire lung surface Inspiration is louder, longer and higher pitched than expiration Sound is soft swishing sound Bronchovesicular Breath Sounds Heard over manubrium where trachea and bronchi bifurcate Inspiration is louder and higher pitched than vesicular breathing Bronchial breath Sounds Heard only over trachea Inspiratory phase is short and expiratory phase is long Pediatric Assessment of Appearance Tone Interactivity Consolability Look/Gaze Speech/Cry Questions to be answered Is there vigorous movement with good muscle tone, or is the child limp? Is the child alert and attentive to surroundings, or apathetic? Will the child reach for a toy? Does the child respond to people, objects, and sounds? Does comforting the child alleviate agitation and crying? Do the child’s eyes follow your movement, or is there a vacant gaze? Are vocalizations strong, or are they weak, muffled, or hoarse? DEVELOPMENTAL DIFFERENCES IN CHILDREN RELATED TO PAIN AGE COMMENTS Infants Preverbal Signs of possible pain: fisting, Young Child with pain regression, withdrawal, Older Child may types of signs of pain Diffuse body movements, highpitched Cry, stiff posture, worried facial expressions, eyes tightly closed Limited vocabulary interferes verbal expression of pain; uses words like “owie” Can not describe intensity of Signs of possible pain: thrashing arms/legs, clinging, screaming Use pain scale for this group; have trouble distinguishing pain such as sharp or dull. May show fewer overt PEDIATRIC MEDICATION ADMINISTRATION Determining Dosage and Route Variations based on age, weight, body surface area and kidney and liver maturity and function Require provider order specifying wgt., dosage calculation, dosage, route and frequency Routes of Administration PO: use calibrated dropper, syringe or cup Prevent aspiration: elevate head, place med in cheek near back of mouth. Do not dilute med NG or OG: crush pills finely, check tube placement and infuse slowly. Flush tube to clear IM or SQ: use sm. syringe &sm gauge (2523G x 5/8”-1”) based on size. Anticipate resistance: get assistance. Preferred sites: Infants & toddlers: vastus lateralis Older children: deltoid IV: assure patency of line, administer through pump or soluset PEDIATRIC MEDICATION ADMINISTRATION CONT. Administration Check for safety of dose and route Check for drug allergy Have 2 RN check drug calculation and dose Use 2 patient identifiers prior to administration (don’t count on child for verbal info) If po med, give choices when possible (water or juice) Ask parent, if present, suggestions for Giving the med. If po, allow the parent to give Never leave meds at bedside Standard Precautions Blood and body fluids of ALL persons must be considered dangerous. The blood of anyone may be infected with bloodborne pathogens including hepatitis B virus, hepatitis C virus, or HIV, the virus that causes AIDS. Standard Precautions apply to ALL PATIENTS. Hand Hygiene: Done before and after contact with every patient, after handling blood or body fluids,after having contact with the patient’s environment or before an aseptic procedures. Alcohol-based waterless hand rub should be the primary method except: After using the restroom When there is visible soil on the hands Before eating. Gloves: Worn when there is a risk of contact with blood or body fluids. Hands must be sanitized after removing gloves. Gowns/Aprons: Worn when there is a risk of soiling clothing with blood or body fluids or when splashing or splattering of blood/body fluids may occur. Face masks/goggles: Worn when splashing, splattering, or spraying of blood/body fluids may occur. Phlebotomy Quick Reference 1. Always confirm patient's identification: ~Always use 2 means of patient ID ~ Correctly Label Specimen at the bedside. 2. Correct Order of Draw: 1. 2. 3. 4. 5. 6. 7. 8. Blood Cultures or Isolator Tubes Light blue Red (plain, no gel) Gold gel tubes Green top tubes (gel or plain), Lavender Pink Royal blue tops 3. Hemoconcentration: a. A tourniquet left on for more than one minute may alter lab values b. Release tourniquet for 2 minutes and reapply before collecting blood specimens c. Gently tap a vein to encourage fill d. Opening and closing a fist may alter lab (over) Phlebotomy Quick Reference( con’t) 4. Hemodilution: a. Never draw above a running IV 5. Quantity Not Sufficient (QNS): a. Difficult draw may not allow sample to be analyzed by lab if QNS. b. Patient will need to be redrawn if QNS 6. Clotted Specimens: a. Difficult draw - perform only 2 attempts b. Gently invert specimen tubes end to end to mix any tubes with additives 8X. 7. Hemolyzed Specimens: a. Alcohol prep not allowed to air dry b. Difficult draw c. Tourniquet on too long or too tight d. Too small a needle and too large a tube Blue 100 Documentation Tips Code Log Check Sheet: Be sure the following is completely filled out on the log: Patient Addressograph Date/Time Initial Assessment of Patient Total IV fluid Time Resuscitation Stopped Signatures Rhythm Strips Nurses’ Note Completed (over) Blue 100 Documentation Tips (con’t) PAR note should include: Patient condition prior to code Last time patient was seen and patient condition How patient was found Who found the patient Time Code Blue was initiated Outcome of code: if transferred to ICU, what time Rhythm Strips to include on log: Initial rhythm strip Any changes in the rhythm strip Any defibrillation and post defib rhythms Any rhythms if patient regained a pulse at any time End of code rhythm Commonly Used Words and Phrases English to Spanish Arm = el brazo Bathroom = cuarto de bano Body = el cuerpo Blood = sangre Blood Pressure = presion de sangre Chest = el pecho Discharge to home = dar de alto a su casa Eye = el ojo Foot = el pie Hand = la mano Injection = inyeccion Left = izquierdo Leg = la pierna Mouth = la boca Nose = la nariz Pill = pildora derecho Skin = la piel vena Out of bed = Fuera de la cama Pain = Dolor Right = Urine – orina Vein = la Good Morning = Buenas Dias Do you speak English = Habla ingles? I am a nurse = Soy la enfermera What is your name? = Como se llama? Where is your Pain? = Donde tiene su dolor? Are you nauseated? = Tiene nauseas? Take a deep breath = Respira hondo QUICK EVALUATION OF A SICK CHILD Observation Normal Mod Impairment Severe impairment Cry Strong Normal tone Whimper or Sob Weak, moaning high pitched Reaction to Parents Cries briefly then content State Variation If awake, Wakes with stays awake. prolonged If asleep, stimulation Wakes easily Color Hydration Pink Cries off/on Continual cry Will not rouse or falls to sleep Pale hands, Pale or blue Feet or acroor gray or cyanosis mottled Skin warm Skin & eyes & dry. Eyes& nl, mouth Mouth moist slightly dry Skin doughy or tented & eyes sunken Pediatric FLACC Pain Assessment Tool Rating 0 Face No particular expression or smile 1 Occasional grimace or frown, withdrawn Uneasy, tense restless 2_________ Frequent to constant frown, clenched jaw quivering chin Activity Quiet, moves Easily Squirms, tense, shifts back & forth Arched back, rigid or jerking Cry Moans or whimpers Crying steadily, screams or sobs Reassured by touch, hug or talking Difficult to console or comfort Legs Nl position or relaxed No cry (awake Or asleep) Consol- Content, ability relaxed Age of use 2 mo to 7 yr Nursing 23(3): 293-297 Kicking, legs drawn up Scoring 0= no pain, 10= worstFrom: Pediatric Key Points for Pediatric CPR Assess Responsiveness Open Airway/ Assess breathing ___<1 yr 1-8 yr > 8 yr_to puberty__ For sudden witnessed collapse and unresponsive: activate EMS For unwitnessed collapse: Activate EMS after 5 cycles of CPR Look, listen, feel <10 sec. If no trauma suspected, do head-tilt/chin lift. If trauma, use jaw thrust only. Open airway and give 2 breaths. If 1 st breath does not go in, retilt head & try again Perform rescue Breathing: Give 2 breaths then: 12-20 breaths per min. Approximately 1 breath q 3-5 sec for rescue breathing without CPR 8-10 breaths/ min with advanced airway with CPR Assess pulse Provide Compressions Brachial or femoral Carotid Carotid 1 finger below nipple Heel of 1-2 hands Heel of hands line with 2 fingers lower ½ sternum Center of chest ---------Depress 1/3 to ½ the depth of the chest-----------------100/min 100/min 100/min Compression/ Ventilation ratio 15:2- 2 person 30:2- 1 person 15:2 -2 person 30:2 -1 person 15:2 2 person 30:2 1 person Vascular Device Tips Central Venous Catheters Non-Tunneled Catheters ~Flush with 10ml NS before each use. ~Flush with 10ml NS and 5ml heparin (10units/ml) after each use. ~Unused lumens flush q8hrs with 10ml NS and 5ml Heparin(10units/ml) Tunneled Catheter Hickman/Broviac ~Flush with 10ml NS before each use. ~Flush with 10ml NS and 2.5ml heparin (10units/ml) after each use ~Unused lumens flush everyday with 10ml NS and 2.5ml Heparin (10units/ml). ~ Day shift is responsible to flush all unused lumens during that shift Groshong ~Flush with 10ml NS before each use. ~Flush with 10ml NS after each use. ~Unused lumens flush every 7 days with 10ml NS (over) Vascular Device Tips (cont) Tunneled Catheters (cont) Hohn ~Flush with 10ml NS before each use ~Flush with 10ml NS and 5ml heparin after each use (10units/ml) ~Flush each lumen with 10ml NS followed by 5ml heparin every 8h (10units/ml) IVAD ~ Before each use aspirate for blood return and flush with 10ml NS. ~After each use flush with 10ml NS and 5ml heparin(10units/ml) No heparin if continuous IV started. ~Unused port flush everyday with 10ml NS and instill 5ml heparin (10units/ml) ~Deaccessing Flush with 10ml NS and instill 5ml heparin (100units/ml) PIC/PICC ~Before each use Flush with 10ml NS ~Groshong PICC After use flush with 10ml NS Unused line flush every 24hrs with 10ml NS ~Midlines and PIC/PICC After each use flush with 10ml NS and 5ml Heparin (10units/ml) Unused lines flush q8hrs with 10ml NS and 5ml Heparin (10units/ml) Blood Transfusion Reaction Blood Transfusion Reaction Symptoms: Fever/Shaking Chills Low Back Pain Nausea/Vomiting Hypotension Chest Pain/SOB Hematuria If your patient develops a blood transfusion reaction: ~Stop the transfusion at once and notify physician ~Obtain vital signs ~Change IV tubing ~Treat Symptoms ~Notify Blood Bank ~Draw 1 Purple and 1 red top tube from opposite arm ~Fill out transfusion reaction form ~Return form, blood specimens & unused blood in bag to Blood bank immediately ~Send first urine passed to urinalysis laboratory Latex Allergy Tips 1. Apply red allergy band 2. Post Signs in room and on chart. 3. Remove all latex gloves and products from patient room/care area. 4. Notify pharmacy of allergy to obtain premixed medications/IV solutions if possible. 5. If meds must be drawn through rubber stopper, puncture the stopper only once and withdraw the required amount. Discard the needle after drawing up the med and before mixing/administering the med. 6. Use kling or stockinet to protect patient from possible contact to latex items i.e. BP cuffs. *Current research shows that the micron filter is ineffective in filtering latex protein particles. There is no reason to be using the micron filter. Common Lab Draws Tube Common Labs Red ETOH, acetaminophen, glucose Light Blue Coagulants/Hematology Green Troponin/Ionized Ca Lavender CBC, Diff and Platelets, Ammonia level Pink Blood Bank Gold top Chemistry Point of Care Testing Questions: (stool occult blood, blood glucose) Contact Kristeen Messore 341-8458 ABG NORMALS PH 7.35-7.45 PaCO2 35-45mm Hg PaO2 80-100mm Hg HCO3 21-27 mEq/L O2Sat 95-98% Base Excess +2 mEq/L ABBOTT EPIDURAL Press ON/OFF (unlock keypad prn) Press YES to CLEAR HISTORY Press YES for EPIDURAL MODE Press 1,2 or 3 to select delivery mode. Press YES for ML ONLY Set RATE. Press ENTER Press YES or NO for loading dose. (follow prompts) If BOLUS DOSE is desired, set BOLUS DOSE and press ENTER or follow prompts to set BOLUS DOSE and LOCKOUT 9. Press YES or NO to limit drug amount over time. If yes, Press 1 or 4 to select length of limit. 10. Set CONTAINER SIZE. Press ENTER 11. Select AIR SENSITIVITY 12. LOCK PUMP 13. Press RUN/STOP to begin infusion IF VOLUME DIFFERENT THAN PREVIOUSLY PROGRAMED: 1. Press REVIEW/CHANGE 2. Press 2 for CHANGE 3. Press 1 for CHANGE PROGRAM 4. Follow prompts 5. Set AIR SENSITIVITY 6. Press RESET 7. Press 2 for NEW CONTAINER *ALWAYS LOCK KEYPAD WITH PATIENT INFUSIONS. TO VERIFY PROGRAM: 1. Press REVIEW/CHANGE 2. Press 1 for REVIEW 1. 2. 3. 4. 5. 6. 7. 8. 3. Use up arrow to scroll through program 4. Press SILENCE to return to main screen TO OBTAIN TOTALS 1. Press HISTORY 2. Press 2 for VOLUME Info 3. Press 1 for SHIFT, (Press 2 for CONTAINER). 4. Use up arrow or HISTORY button to scroll through 5. Press SILENCE to return to main screen. DELIVER LOADING DOSE 1. Press RUN/STOP and unlock keypad 2. Press LOADING DOSE 3. Press YES 4. Set dose and press ENTER 5. Press YES 6. Press LOADING DOSE to begin delivery 7. Press RUN/STOP and LOCK Keypad *ALWAYS LOCK KEYPAD WITH PATIENT INFUSIONS. When loading dose is complete, pump will alarm if set. CHANGE CONTAINER 1. Press RUN/STOP and unlock keypad 2. Press RESET 3. Press 2 to set a NEW CONTAINER (same volume as previously programmed) 4. Press RUN/STOP and lock keypad CLEAR SHIFT TOTAL FROM STOP MODE & UNLOCK KEYPAD 1. Press RESET 2. Press 1 for NEW SHIFT TOTAL Pump returns to stop mode & lock keypad. CHANGE PROGRAM, RATE, OR VOLUME: FROM STOP MODE & UNLOCK KEYPAD 1. Press REVIEW/CHANGE 2. Press 2 to CHANGE 3. Press 1 to CHANGE PROGRAM 4. Follow prompts to change entries & lock keypad. ENTER NEW PROGRAM FROM STOP MODE: & UNLOCK KEYPAD: 1. Press REVIEW/CHANGE 2. Press 2 to CHANGE 3. Press 2 for NEWS PROGRAM 4. Press NO to CLEAR HISTORY Does not reset shift; clears current program only. 5. Follow prompts to set new program (See programming.) 6. At time of NEW PROGRAM CHANGE, enter actual container volume remaining. When CHANGING TO NEW CONTAINER, enter new bag volume. Always Lock keypad with Patient Infusion To LOCK the pump 1. Press RUN/STOP 2. Press ENTER 3. Press down arrow 3 times To UNLOCK pump 1. Press RUN/STOP 2. Press ENTER 3. Press up arrow 2 times Medley PCA Module 1. 2. 3. Security Lock Key Positions a. Unlock: unlocks the security door. The key must be in this position when loading or changing a syringe b. Program: allows for changes in programming the device with out unlocking the security door. c. Lock: Locks the security door. The key must be in this position to start an infusion Preparing Infusion a. Press Channel Select key (Key must be in program position) b. Press soft key next to installed syringe type and size (selection will be highlighted) c. To accept, press Confirm soft key Priming Tubing a. Press Options key b. Press Prime Set with Syringe c. Set key to Program position d. Press and hold Prime soft key until fluid flows and priming of tubing is complete. Release prime key when complete e. 4. To return to main screen, press Exit soft key Programming an Infusion a. Perform steps in preparing syringe and administration set b. Power on system c. Choose Yes or No to New Patient d. Select profile if required (ex. ICU, West 5) e. Enter patient identifier if required f. Press Channel Select key g. Unlock security door or set key to Program position h. Confirm time of day and change if needed i. Press soft key next to desired drug and concentration j. Confirm the drug and concentration selection and press Yes soft key. To change selection press No soft key and follow prompts k. If Yes was selected and facility has defined a clinical advisory for that drug, a message appears. To continue programming, press Confirm soft key l. Drug amount and diluent volume will appear. Press Next soft key to confirm 5. 6. Setting up PCA Dose Only a. Press PCA dose only soft key from infusion mode screen b. Use numeric data entry keys to enter PCA dose c. To enter Lockout interval, press Lockout Interval soft key and use numeric data entry keys d. To enter Max Limit, press Max Limit soft key, press Yes soft key and use numeric data entry keys e. To enter Loading Dose, press Load Dose soft key, press Yes soft key and use numeric data entry keys f. Verify parameters are correct and press Confirm soft key g. Close and lock security door h. Verify parameters on second nurse summary screen are correct and press Start key Setting up Continuous Infusion Only a. Press Continuous Infusion soft key from infusion mode screen b. To enter continuous infusion dose, press Cont Dose soft key and use numeric data entry keys c. 7. To enter Max Limit, press Max Limit soft key, press Yes soft key and use numeric data entry keys d. To enter Load Dose, press Load Dose soft key, press Yes soft key and use numeric data entry keys e. Verify parameters are correct and press Confirm soft key f. Close and lock security door g. Verify programming parameters are correct and press Start key Setting up PCA Dose and Continuous Infusion a. Press PCA Dose + Continuous soft key from infusion mode screen b. To enter PCA dose, press PCA Dose soft key and use numeric data entry keys c. To enter Lockout interval, press Lockout Interval soft key and use numeric data entry keys d. To enter Continuous Dose, press Cont Dose soft key, press and use numeric data entry keys e. To enter Max Limit, press Max Limit soft key, press Yes soft key and use numeric data entry keys f. 8. 9. To enter Loading Dose, press Load Dose soft key, press Yes soft key and use numeric data entry keys g. Verify parameters are correct and press Confirm soft key h. Close and lock security door i. Verify parameters on second nurse summary screen are correct and press Start key Setting Loading Dose Only a. Press Loading Dose Only soft key from infusion mode screen b. Use numeric data entry key to enter dose value c. Verify dose value is correct and then press Confirm soft key d. Close and lock security door e. Verify parameters on summary screen are correct and press Start key f. When loading dose is complete The Loading Dose has Completed appears on the main display g. Press Confirm Setting Bolus Dose a. Press Channel Select on PCA module b. Press Bolus Dose soft key c. Set key to Program position or enter 4 digit authorization code and press Confirm d. Use numeric data entry keys to enter does value e. Press Confirm f. If authorization code is disabled, door must be locked prior to starting bolus dose g. Verify dose value is correct and then press Start soft key h. Once bolus complete, programmed infusion resumes 10. Stopping a Loading, PCA or Bolus Dose a. Press Channel Select key on PCA Module b. Press Stop Load, Stop PCA or Stop Bolus soft key as applicable c. To stop dose and resume current program, press Yes soft key 11. Changing Program Parameters During an Infusion a. Press Channel Select key b. Press Program soft key c. Set Key to Program position or if authorization code is enabled, enter 4 digit code d. Press Change Modes soft key e. f. Select desired infusion mode Continue programming as outlined above for infusion mode selected g. Verify or change program settings and press Confirm key h. Close and lock door i. Verify programming parameters on summary screen are correct and press Start key 12. Viewing Patient History a. Press Channel Select key b. From main display, press Options key c. Press Patient History soft key d. Press Zoom soft key to select desired time period e. Press Detail soft key to view detailed patient history f. To return to Main Patient History, press Main History soft key g. To return to Main Display, press Exit soft key 13. Clearing Patient History a. Press Clear History soft key, a confirmation screen appears b. To continue and clear patient history, press Yes soft key c. To cancel and return to patient history, press NO soft key d. Once patient history is cleared, the last 24 hours of patient history data may be retrieved and viewed. e. Select 24h Totals soft key from patient history screen to retrieve last 24 hours f. Press Shift Totals soft key to return to patient history view 14. Viewing drug Event History a. Press Channel Select key b. From main display, press Options key c. Press Drug Event History soft key d. Press Page Down soft key to scroll through history e. To return to main display, press Exit soft key 15. Restoring Infusion Following Syringe Empty a. Unlock security door b. Remove existing syringe and load new syringe and administration set c. Select syringe type and size d. Prime tubing e. To restart infusion using restored parameters, press Restore soft key and continue with next step f. Verify parameters are valid and press Confirm soft key g. To start a new infusion, select drug form guardrails drug library and follow steps for PCA infusion modes h. Close and lock security door i. Verify programming parameters on summary screen are correct and press Start key 16. Viewing and Clearing Volume Infused a. To view volume infused, press Volume Infused soft key from main display b. To clear volume infused: 1. To clear all channels, press Clear All soft key 2. To clear selected channels: press soft key next to selected channel and press Clear Channel soft key 17. Changing Syringe During Infusion a. To stop infusion, press Pause key on PCA Module b. Unlock the door c. Open plunger grippers and syringe barrel clamp d. Replace syringe e. Load new syringe f. Select syringe type and size g. Press Confirm soft key h. Prime administration set i. j. k. Press Restore soft key, press Next soft key, and confirm programming parameters Lock the door To begin infusion, press Start soft key CATEGORIES Cry SCORE 0 No particular expression or smile Content, Relaxed Normal position Relaxed Lying quietly Normal position Moves easily No cry (awake or asleep) Consol ability Content, Relaxed Face Legs Activity SCORE 1 Occasional grimace or frown. Withdrawn, distressed Uneasy, Restless Tense Squirming, Shuffling back and forth Tense Moans or whimpers Occasional complaint Reassured by occasional touching, hugging or being talked to. Distractible SCORE 2 Frequent to Constant quivering chin, clenched jaw. Kicking, drawing up legs Arched, rigid or jerking Crying steadily. Screams or sobs frequently. Frequent complaints Difficult to console or comfort The FLACC scale for noncommunicative patients Assess each of the categories in the far left column to obtain a score of 0-2 Add the scores for all five categories to obtain a score of 0-10 Process for Obtaining Foreign Language, Hearing impaired and/or Visually Impaired Resources Hearing Impaired/Foreign Language Interpreters: Monday-Friday 8am to 4:30pm Call Patient Care Services at 341-6718 Evenings (after 4: 30pm), nights, weekends and Holidays: Contact the Nursing Supervisor pager #220-8098 Services/Equipment Available for Hearing and Visually Impaired Patients: Equipment is located in the Telecommunications Department *TTY Services *SIGNAL PHONES *AMPLIFIED RECEIVERS *CLOSED CAPTIONING *LARGE NUMBERED PHONE RECEIVER Telephone Numbers Admit Pharm. Blood Bank Hem Chem CT Micro Dialys In 16748 37967 18554 16810 16803 18061 16818 16502 Dietary 37951 APC 16526 ED 16880 E3 M/B 16836 E3 L&D 16875 E5 18190 E6 10166 E7 16643 ICU 16932 W4 16840 W5 18422 Infection Prevention 10654 W6 16850 W7 16855 Infusion 18113 Health 18017 Sterile Prod. 37806 Transp/Serve 17378 Ultrasound 1806 Storeroom 16341 Cardio. 16780 NucMed 18062 Dottie Haelen 18058 Credit Union 37979 DOOL 16709 Security 16899 OR 16269 PACU 38920 Medical Image 16785 SW 16718 Sally Nordquist Diabetes Nurse Educator 16425 Employee Health 18017 PT Pager Numbers Bed Coordinator Housekeeping Infusion Nurse Nurse Supervisor Resp Therapy SWAT Nurse Transport Vascular Lab Infection Prevention 220-4434 220-8053 220-8551 220-8098 220-8019 220-8140 220-8164 220-4170 220-8160 220-0228 220-8307 Disaster Pocket Guide A Just-in-Time Reference for Highland Disaster Staff & Volunteers The Disaster Pocket Guide is designed as a quick reference. Users should refer to the current policy and protocols of the organization to ensure the most current and complete information. When finished with this Pocket Guide, please return to the Incident Command Center. Revised 8/07 Patients with Insulin Pump Highland Protocol for Management of Patients Receiving Insulin Therapy states that patients may use their own Insulin Pumps if they meet the criteria for safety: Diabetic Health Source is contacted (341-6425) The patient is alert and oriented Independent in ADLs Agrees to sign the “Insulin Pump Therapy Patient Contract” When Criteria is met: MD completes preprinted order form #10894 Pt. signs contract, keeps yellow page Patient uses own pump and tubing set Hospital Insulin must be used Patient will provide basal & bolus insulin rates. Pt. assessed EVERY hour for mental status, site status and correct infusion rate. Patients with Insulin Pump (cont) Patient must continuously meet criteria. If condition changes, pump is discontinued and Pt is switched to either Lantus SQ@ HS with Novolog SQ AC meals OR Regular Insulin IV continuous infusion. BGs must be monitored (by staff or pt with RN supervision) with hospital meter (FBS, AC meals, 2hr after each insulin bolus, HS & 0300 & prn s/s hypoglycemia) Hypoglycemic treatments: BG<70 If PO: Give oral glucose gel; if refused 4 oz. juice (15gm Carb) Recheck in 15 minutes Repeat until BG> 70. If NPO: Give 50 ml (1amp) dextrose 50% IVP Notify MD/PA/NP Recheck BG 15 min after treatment If BG<70 repeat above Recheck bg every 15 minutes; if at 1 hour bg remains <70 start IV D10% at 150 ml/hr Refer to SOC: Diabetes Management in the Hospitalized Patient. Organ and Tissue Donation All anticipated (withdrawal of life support) and actual deaths must be referred to the donor hotline at 1-800-774-2729 whether or not they are suitable for potential donation. The Organ Procurement Office (OPO), Finger Lakes Donor Recovery Network (FLDRN) and the Rochester Eye and Tissue Bank (RETB) coordinate the donation of all organs and tissue. Any health care provider involved with the patient’s care can make referrals to the Donor Hotline; the unit secretary usually makes the call at Highland. Document referral in chart. ONLY FLDRN coordinators conduct the consent process and offer the option of donation to the families. . Elevate head, place NS drops into the eyes and ice packs over the eyes in anticipation of eye donations. (over) Organ and Tissue Donation (cont) There is no cost to family. No disfigurement will result. Eyes will be retrieved in the morgue. If time is of the essence, eyes may be removed in the Emergency Department from patients who have died there. RETB will arrange transportation for the recovery of other tissues with the family and hospital staff. Tissue removal documentation will be provided by the recovery agency for the medical record. Highland Staff will give condolence Card to the family if tissue/organs are determined suitable for donation. Alaris Pump Points Refer to the Alaris Medley Medication Safety System Operator’s Quick Reference Guide for Priming, Loading, Programming and Troubleshooting instructions. These are laminated and should be attached to pumps. Be sure correct priming and loading sequence is followed. Misloading can lead to unregulated flow of medication to the patient. Remember to open roller clamp for IV piggybacks to infuse. If receiving a patient transferred from another unit with a pump, ensure proper unit specific guardrails are selected. Keep pump units plugged in when not in use to recharge battery. Return unused pumps to SPD for cleaning between patients. Highland Adult Normal & Therapeutic Lab Values Acetone Negative Albumin 3.2-4.8 gm/dl Alk. Phos 45-129 U/L Ammonia 10-47 umol/L Amylase 30-118 U/L Bilirubin-Total 0.3-1.5 mg/dl Bilirubin-Direct 0.0-0.5 mg/dl BUN 9-23 mg/dl Chloride 99-109 meq/l CO2 20-32 meq/l CPK-Male 38-174 U/L CPK-Female 26-140 U/L Creatinine-Male 0.7-1.4 mg/dl Creatinine-Female 0.6-1.1 mg/dl Glucose 74-106 mg/dl Iron-Female 38-138 ug/ml Iron-Male 40-159 ug/ml TIBC 250-450 ug/ml Potassium 3.5-5.5 meq/l Sodium 132-146 meq/l TSH 0.35-5.50 uU/ml Tegretol 8.0-12.0 ug/ml Digoxin 0.9-2.0 ng/ml Phenytoin (Dilantin) 10-20 mcg/ml Salicylate 20-25 mg/dl Theophylline 10-20 ug/ml 0 1 0 -- 0.45 0.91 1.36 1.81 2.27 2.72 3.18 3.63 4.08 20 9.07 9.53 9.98 10.43 10.89 11.34 11.79 12.25 12.70 13.15 40 18.14 18.60 19.05 19.50 19.96 20.41 20.87 21.32 21.77 22.23 60 27.22 27.67 28.12 28.58 29.03 29.48 29.94 30.39 30.84 31.30 80 36.29 36.74 37.19 37.65 38.10 38.56 39.01 39.46 39.92 40.37 100 45.36 45.81 46.27 46.72 47.17 47.63 48.08 48.53 48.99 49.44 120 54.43 54.88 55.34 55.79 56.25 56.70 57.15 57.61 58.06 58.51 140 63.50 63.96 64.41 64.86 65.32 65.77 66.22 66.68 67.13 67.59 160 72.57 73.03 73.48 73.94 74.39 74.84 75.30 75.75 76.20 76.66 180 81.65 82.10 82.55 83.01 83.46 83.91 84.37 84.82 85.28 85.73 200 90.72 91.17 91.63 92.08 92.53 92.99 93.44 93.89 94.35 94.80 220 99.79 100.24 100.70 101.15 101.61 102.06 102.51 102.97 103.42 103.87 240 108.86 109.32 109.77 110.22 110.68 111.13 111.58 112.04 112.49 112.95 260 117.93 118.39 118.84 119.30 119.75 120.20 120.66 121.11 121.56 122.02 280 127.01 127.46 127.91 128.37 128.82 129.27 129.73 130.18 130.64 131.09 300 136.08 136.53 136.99 137.44 137.89 138.35 138.80 139.25 139.71 140.16 320 145.15 145.60 146.06 146.51 146.96 147.42 147.87 148.33 148.78 149.23 340 154.22 154.48 155.13 155.58 156.04 156.49 156.94 157.40 157.85 158.30 360 163.29 163.75 164.20 164.65 165.11 165.56 166.02 166.47 166.92 167.38 380 172.37 172.82 173.27 173.73 174.18 174.63 175.09 175.54 175.99 176.45 400 181.44 181.89 183.34 182.80 183.25 183.71 184.16 184.61 185.07 185.52 # 2 3 4 5 6 7 8 Weight Conversion Chart: Pounds and Kilograms 9 Code 15(Stroke) Process Evaluate patient for acute stroke symptoms. Call for Rapid response team RRT will assess for need to call Code 15. If Code 15: Call 1-6666 for operator to page. Bring patient chart, Crash Cart and defibrillator to patient room. Obtain “Stroke Kit” from Crash Cart notebook – Code 15 log has all necessary documentation Obtain “Acute Stroke Triage Orders” from the Stroke Packet folder Record last time the patient was seen without stroke symptoms Anticipate need for emergent head CT and blood draws Labs: obtain reqs in HBOC under “Stroke Panel” Page CT tech and lab to alert of potential tPA candidate; process has changed – only 1 page now alerts CT, lab and neurology in addition to the Code 15 team Prepare for potential patient transfer to CT Complete progress note about events Prepare for possible transfer to ICU or the Stroke Unit (W7). Goal: Stroke Team evaluation within 15 minutes BLS ADULT/PEDIATRIC CPR UNRESPONSIVE Person - Phone 16666 or call for Help ■ Send someone to get AED ■ Pediatric - Do 2 min. CPR then AED AIRWAY - Open airway; head tilt-chin lift BREATHING - Look, Listen, Feel 10 sec. ■ Not breathing give 2 breaths- 1 sec per breath CIRCULATION- Check pulse < 10 seconds: ■ Adult/child – carotid pulse ■ Infant – brachial Pulse Present/No Breathing: Rescue Breaths ■ ■ ■ Adult 1 breath every 5-6 sec Infant/Child 1 breath every 3-5 sec. Recheck Pulse every 2 min Pulse Absent; Begin compressions ■ ■ 30 compressions/2 breaths Infant/child 2 person: 15 compressions/2 breaths DEFIBRILLATION: Goal is Less Than 3 minutes to SHOCK AED/Defibrillator Arrives 1. AED ON - Turn ON Power 2. Apply Pads per package ■ Use Pediatric Pads if needed 3. Connect Pads Cable & Plug in connector 4. Analyzes Heart Rhythms; Do Not Touch Patient NOTE: use manual mode for pediatric patients < 55 lbs Procedure for Assisting Patients with a Bedpan Patient has requested a bedpan: 1. Gather needed supplies: clean gloves, bedpan, toilet tissue 2. Close door and pull privacy curtains 3. Instruct patient to bend his/her knees and press down with feet and slip the bedpan beneath the patient’s buttocks. OR if patient is unable to lift themselves: Lower head of bed, roll patient to their side and position the bedpan. 4. Raise the head of the bed, ensure toilet tissue and call light are within reach. 5. Instruct patient to call for assistance when they are done. 6. Return and, with gloved hands, remove bedpan having patient repeat same process as above. 7. Assist with removing residue of urine, feces from the skin. 8. Help position patient for comfort. 9. Provide handwashing supplies. 10. Dispose of bedpan contents in patient’s toilet. Measure and record volume of urine if patient’s intake and output are being monitored. Procedure for Assisting Patients with their Hygiene Needs Partial Bedbath: when an alert patient needs to bathe in bed or sitting in a chair at their bathroom sink: 1. Gather needed supplies: towels, wash cloth, soap, tooth brush, toothpaste, comb, deodorant, clean gown, wash basin, kidneyshaped basin, clean cup. 2. 3. 4. 5. 6. Sit patient up in bed, at bedside or assist them to bathroom. Assisting Patient with Oral Care a. For patient in bed, obtain fresh cool water and kidney shaped basin. b. Assist/allow patient to brush teeth, rinse and spit into kidney basin. c. If patient has denture/partials and needs assistance: Apply clean gloves, gently brush dentures/partial using toothbrush and toothpaste. Rinse. Assist patient to put dentures in place if needed. d. Dispose of water and contents of basin when patient is done. Obtain basin full of warm water. Close door, pull privacy curtains and leave call bell in reach. Instruct patient to wash all areas of body they are able to comfortably and safely reach. Advise patient to use call bell to ask for help when they are done. Return, obtain fresh warm water, apply gloves and assist patient to wash legs, back, and provide perineal area. Administering Perineal Care: a. Assist patient to lie on their back. b. For the female patient: Bend the patient’s knees and spread the legs. Separate skin folds. Using clean area of the cloth for each stroke, wash from pubic area toward anus (top to bottom). Never go back over an area that has already been cleansed. Pat area dry gently with towel. c. For the male patient: Grasp the penis and retract the foreskin if the patient is uncircumcised. Clean the tip of the penis using circular motions. Never go back over an area that has already been cleansed. Replace the foreskin. Wash the shaft of the penis in downward motion. Spread the legs and wash the scrotum. Pat skin dry with a towel. d. Turn patient to the side and wash from the perineum to anus (“clean” area to “dirty” area). Pat dry 7. Assist patient into clean gown and cover them with a blanket/sheets. 8. Empty and rinse bedpan, put dirty linen in hamper. 9. Remove gloves and wash hands. 10. Position patient comfortably with call bell in reach. Complete Bedbath: when a non-alert patient needs to be given a bed bath: 1. Gather needed supplies: Bath blanket, towels, wash cloths, soap, wash basin, clean gown, deodorant, comb. 2. Close door, pull privacy curtain and raise bed to an appropriate height. 3. Position patient on his/her back. 4. Cover patient with bath blanket and remove patient’s gown. 5. Obtain warm basin full of water and place on overbed table. 6. Apply clean gloves, wet wash cloth and fold it to fashion a mitt. 7. Lather wet washcloth with soap and wash the patient’s face. 8. Rinse washcloth, remove soapy residue, they gently dry well. 9. Bathe each of patient’s arms separately; chest, then axillae (underarm). Rinse and dry well. 10. Apply deodorant or antiperspirant if wanted/available. 11. Place each hand in the basin of water as it is washed. Cleanse under fingernails if needed, but never cut patient’s fingernails or toenails. 12. Discard and replace the water in the wash basin; rinse the washcloth well or replace it with a clean one. 13. Wash the abdomen, each leg, and the feet, following the steps described for the upper body. 14. Help the patient roll onto his/her side. 15. Change the water and bathe the patient’s back 16. Wash buttocks and perineal area last (see Administering Perineal Care) 17. Assist patient to apply clean gown. 18. Change sheets of bed (see Making Occupied Bed) 18. Discard water, put dirty laundry into appropriate hamper. 19. Return bed to lowest position References: Timby, B.K. (1996). Fundamental Skills and Concepts in Patient Care (6th ed.). Philadelphia, PA: Lippincott-Raven Publishers. Procedure for Making an Occupied Bed Plan to change the linen after the patient’s hygiene needs have been met. 1. Obtain assistance if the patient is too weak or unable to cooperate. 2. Gather needed supplies: fitted sheet, sheet, pink pad, pillow case, blanket. 3. Close door and pull privacy curtain 4. Apply gloves and raise the bed to an appropriate working height. 5. Cover patient with a bath blanket or leave top sheet loosened, but in place. 6. Check for personal items that may be in bed. Move them to a 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. secure location. Loosen bed linen from where it has been tucked under the mattress. Lower the side rail on the side of the bed where you are standing and roll the patient toward the side rail on the far side of the bed. Roll the soiled bottom sheets as close to the patient as possible. Apply fitted sheet to top and bottom of side of bed closest to you and spread toward the middle of the bed. Position and apply pink sheet on top of fitted sheet on side closest to you. Roll excess fitted sheet and pink sheet tightly and tuck under soiled bottom sheets as close to patient as possible. Use a towel as a barrier between clean and dirty linens if necessary to keep clean linen dry. Raise side rail and assist patient to turn onto their other side over the roll of linens. Go to other side of bed, or if working with another person, help patient maintain side-lying position. Roll of linens may now be pulled through under patient. Soiled linens may be put aside for later placement in appropriate hamper. Clean fitted sheet should be applied to top and bottom, and pink pad pulled through and smoothed under patient. Patient may be assisted onto back. Place clean sheet and blanket (if patient desires) over patient, and remove dirty sheet. They may be tucked under mattress if patient wishes, but be sure to leave room for patient’s toes to move freely under blankets. 20. Return bed to lowest position. 21. Assist patient into comfortable position. 22. Ensure call bell is within patient’s reach. Principles of Positioning Patients 1. Patient’s are encouraged and assisted to change positions at least every 2 hours. 2. Bed is raised to an appropriate height. 3. All pillows and positioning devices are removed before repositioning. 4. Drainage tubes are unfastened from the bed linen. 5. The patient is turned as a complete unit (log rolled) to avoid twisting the spine. 6. The body is placed in good alignment with joints slightly flexed/bent. 7. Pillows and positioning devices are replaced after repositioning. 8. Elevate/raise on pillows those areas that are swollen/enlarged. 9. Notice any areas where skin has become red. Do not rub if red. Position patient to relieve/remove pressure on red areas – notify nurse. 10. Once repositioned, ask patient or look at them and ask yourself if they seem comfortable the way that you have positioned them. Are all parts of the body supported and in alignment/straight? If no, reposition. Patient Feeding Serving Trays Match tray to patients name on ticket. Verify correct diet Open lids and identify foods Call bell within reach Amount of assistance will vary, cutting food, preparing coffee, butter bread Patient Feeding Offer hand towelett for hand hygiene Patience is important Test temperature of food, steam, stir, feel outside of bowl Fill spoon ½ way only Do not give more food until read Alternate solids and liquids Dysphagia Difficulty chewing and/or swallowing Increased risk of choking Thin liquids are highest risk of causing choking Care: Thickened liquids, soups etc. No thin liquids No straws Never position flat on back Keep head of bed up at least 30 degrees Observation & Reporting Information collecting Constant ongoing process Important job function What to Observe Color of skin, temperature of skin Patient level of alertness, mental status changes Breathing sounds, work of breathing, cough Movements, ability to move, ability to transfer, walk, etc Patient reports of pain other discomforts Report Report accurately and promptly Report patient name and location Falls and Restraints What is the patient’s status for Falls Risk: History of falls Mobility problems Certain medications Age >65 Confusion, agitation Incontinence Physical conditions Falls prevention Use side rails if needed Assist with walking Use lights/night lights Frequent visual checks Clean up spills immediately Falls and Restraints cont. Keep assistive devices in reach such as canes Keep personal items such as glasses in reach Safe footwear or slipper socks on patient Locks on bed/wheelchair at all times Frequent toileting Keep patients surroundings free of obstacles Restraints Last resort only Restraints are not a means to prevent falls May be used if patient is a danger to themselves or others Used when we are unable to provide care safely Must have order Patient Care when restrained: Visual checks every 15-30 min Release restraint every 2 hours Never restrain patient flat on back Position patient comfortably Meet patient’s needs such as hygiene, nutrition/feeding, elimination, positioning and emotional support. Safe Mobilization of Patients When ambulating patients assure that the patient is safe while they are up and moving around. You are also responsible for protecting yourself (ie. your back/body) while assisting that patient. It is important, not only to think about safety for the patient, but also anybody who is taking care of that patient. Make sure there is an out of bed activity order before getting a patient out of bed. You can do this by checking with the nurse Be aware of any weight bearing limitation orders. Utilize pink pads/bedrails to minimize lifting/pulling. Always have slipper socks or shoes on the patient. Indications for 2 assist – Very agitated, very weak, a lot of equipment/attachments. A mechanical Safe Mobilization of Patients cont. lift is indicated for patients that are too weak to stand. Use an assistive device if it is recommended or in the room for the patient to use (including gait belts, walkers, canes, etc.). Avoid or be aware of unnecessary clutter or tubing that the patient can become caught in or trip over, such as: IV poles, oxygen tubing, and Foley catheters. If getting a patient out of bed and into a chair: Choose an appropriate chair. Determine if you need a second assist. Set the chair up (with a sheet and pink pad) close to the bed. Make sure the chair and bed brakes are on. Allow the patient to do as much as she can to help. Safe Mobilization of Patients cont Allow the patient to sit at the edge of the bed for a few minutes before standing in case of dizziness/light headedness. Place assistive device directly in front of the patient. Place gait belt on patient if using one Make sure any oxygen or IV tubing is in place. Encourage the patient to stand, pushing from the bed with her hands to prevent the walker from falling on her. Assist the patient to standing, if needed, with one hand under the patient’s shoulder and the other hand around her waist (or holding gait belt). Give the patient time to do as much of the transfer as she can on her own. Encourage the patient to take small steps until she feels the chair against the back of her leg. Safe Mobilization of Patients cont Have the patient reach both hands back and hold onto the chair. Assist the patient slowly into the chair. Encourage the patient to scoot all of the way back into the chair. If they need assistance, you can use the pink pad to boost the patient back into the chair, or you can place an upright pillow behind their back to boost them forward. If walking a patient: Follow above steps If the patient is using a walker, make sure they do not walk too close to the front of the walker or too far behind it. It is recommended that patients try to keep their feet in line with the back of the walker. Within reason, allow the patient to dictate direction. This will give them some control. Defer to the nurse for specifics regarding how long a patient should stay out of bed or how far she should walk. INFECTION PREVENTION HAND HYGIENE Use 15-20seconds of rubbing when sanitizing hands. Proper hand hygiene using waterless hand rubor soap and water (always choose soap and water if hands are visibly soiled, after using restroom, before eating). Always clean hands: before and after direct contact with a patient before surgical procedures after removing gloves before giving meds after moving from a contaminated body site to a clean body site during patient care after contact with inanimate objects in the INFECTION PREVENTIONcont immediate vicinity of patient after coughing or sneezing before and after meals and food breaks after using toilet facilities after contact with blood or body fluids PROPER USE OF PERSONAL PROTECTIVE EQUIPMENT (PPE) The following items are worn for PPE: gowns gloves masks goggles/face shield/side slip-on shield GOWNS - should be water resistant - should be worn if clothing might l be splashed/soiled INFECTION PREVENTIONcont - put on before entering patient’s room and removed before leaving room - should be worn once unless severe shortage exists.- when removed, gown should be rolled “outside in” to prevent re-contamination from the outside of the gown GLOVES - must be changed between patients - must be worn to enter room - hand hygiene must be performed after removing - should be changed when going from a “dirty site” to a “clean site” INFECTION PREVENTIONcont (i.e. urinary catheter to an IV site) MASKS- should be worn within 6 feet of any person coughing are either on or off – never allowed to hang around neck must be changed if they become moist particulate respirator masks(N95) are required for aerosol generating procedures. PROPER SEQUENCE FOR PUTTING ON PPE: (graphics go with this one) PROPER SEQUENCE FOR REMOVING PPE: (see graphics) COUGH ETIQUETTE Follow the steps of cough etiquette at all times: use tissues to cover mouth/nose when coughing or sneezing - if tissues are not available, use sleeve dispose of tissues in the nearest waste receptacle immediately after use avoid touching eyes, nose or mouth perform hand hygiene with either a waterless hand sanitizer or soap and water ASAP wear a mask if coughing frequently DO NOT EAT OR DRINK in patient care or clinical areas. DO NOT COME TO WORK if you have the following symptoms: fever > 37.8◦C or 100.4o F sore throat diarrhea flu-like symptoms VENTILATOR BASICS Some things to remember: 1. All ventilated patients must have a manual resuscitation bag with them at all times. Resuscitation bags for patients requiring PEEP ≥ 10 cm. H2O must be equipped with a PEEP valve. 3. Never silence ventilator alarms and leave patient alone. 4. The safest action for a ventilated patient experiencing respiratory distress with an unknown cause is: 1. Disconnect patient from ventilator 2. Manually ventilate patient using resuscitation bag. 3. Call Respiratory Care immediately. Suctioning: • Suctioning is done as needed, NOT a scheduled activity. • Use Normal Saline ampules for lavage if needed. • Suction if patient is coughing frequently with mucus in E-T or Tracheostomy tube, ventilator is high pressure limiting or oxygen saturation is dropping. • Notify Respiratory Therapist if patient’s secretions are getting thicker, oxygen saturation is dropping or you get thick mucus plugs when you suction. Call Respiratory Care for any situation if you are unsure of the needed action. • IMPORTANT: If patient has a tracheostomy tube and you think that the tube may be plugged, first try to suction. If you can’t pass the suction catheter, remove the inner cannula, ventilate the patient manually using resuscitation bag and call Respiratory Care 2.