Spring 2013 - Cleveland Clinic
advertisement

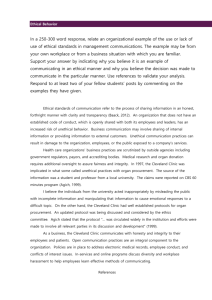
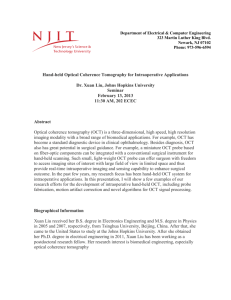
Cole Eye Institute S prin g 2013 Ophthalmology Update Jules and Doris Stein Professorship Awarded for Study of the Genetics of Retinal Ciliopathies Cole Eye Institute, in partnership with Cleveland Clinic develop correlations between specific human mutations Lerner College of Medicine of Case Western Reserve and the degree of visual loss in various ciliopathies, to University, has been granted a Jules and Doris Stein identify novel ciliopathy alleles that contribute to retinal Professorship Award from Research to Prevent Blind- pathology and to understand the cellular mechanisms ness (RPB) to support the research efforts of Brian regulating basal body migration. Perkins, PhD, in ciliopathies in the eye. Brian Perkins, PhD “Our intention is to use the support from RPB to conduct Genetic mutations that disrupt the assembly, structure exciting additional work with zebrafish, which are al- or function of basal bodies and/or cilia result in a spec- ready established as reliable models for genetic testing,” trum of diseases known as ciliopathies. These multi- says Dr. Perkins. “As just a few examples, we will use syndromic disorders cause retinal degeneration, kidney zebrafish to test the in vivo mechanisms that position disease, mental retardation and polydactyly. Dr. Perkins will continue his work using zebrafish, members of the minnow family known for their regenerative ability, to characterize the molecular basis of cilia basal bodies, including the role of cytoplasmic dynein motors, the planar cell polarity (PCP) pathway, and the interactions between PCP signaling and the Joubert syndrome protein Arl13b.” formation in photoreceptor cells. In collaboration with The hope is that the research supported by RPB will en- colleagues at Cole Eye Institute, Dr. Perkins plans to able clinicians to better predict the outcomes of certain Continued on next page Strabismus Surgery in Thyroid Eye Disease Intraoperative Optical Coherence Tomography Looking Back at a Decade in Publishing Biomarkers in Uveal Melanoma Page 3 Page 4 Page 8 Page 10 Clinical Trials, Cole Eye CME and Distinguished Lecture Series Page 11 mutations and improve genetic testing. The lab also plans to develop zebrafish models of diabetic retinopathy and age-related macular degeneration. The award includes up to $1.025 million in grant support, payable over seven years. “I am so pleased that the promise of Dr. Perkins’ re- Third Frontier Grant + Building Campaign = Big Future for CEI Cleveland Clinic’s Cole Eye Institute is preparing to provide its search is being recognized by an organization as distin- superior care to tens of thousands of additional patients and become guished as RPB,” says Daniel F. Martin, MD, Chairman a premier site for research, development and commercialization of of Cole Eye Institute. “I believe that his future work will ophthalmic imaging technologies. The focal point of vision care at continue to build on his notable accomplishments in Cleveland Clinic was recently awarded a $3 million grant from the this research area.” Ohio Third Frontier Program at the same time it began a building The research will add to Dr. Perkins’ work in zebrafish campaign to more than double its size. genetics and biochemistry. Dr. Perkins has been using The grant and another $3 million in matching funds will help launch zebrafish as a model system for retinal degeneration for several new products and services being developed in the Ophthalmic more than 10 years. As a National Institutes of Health Imaging Center, a research, development and commercialization unit (NIH)-funded postdoctoral fellow at Harvard University, within Cole Eye Institute. Specifically, the monies will support the he developed transgenic tools to analyze the photorecep- development of an innovative intraoperative spectral domain optical tor structure in zebrafish and identified several mutants coherence tomography system, including: affecting photoreceptor survival. As the principal inves- • Novel surgical instruments that improve image-based analysis tigator (PI) of two currently funded NIH grants and the PI on a previous NIH subcontract, Dr. Perkins has also conducted studies of zebrafish IFT mutants and other and visualization of surgical sites • Contrast dyes genes that lead to photoreceptor degeneration. • Surgical imaging software RPB supports eye research directed at the prevention, More innovations like this will be possible in the future expansion treatment or eradication of all diseases that threaten of the Cole Eye Institute. A planned additional 135,000-square-foot vision. RPB has committed hundreds of millions of dol- facility will: lars in grant support to medical institutions across the • Create a state-of-the-art ocular imaging research center United States for research into all blinding eye diseases. Jules and Doris Stein RPB Professorships, the highest • Double the size and scope of our basic science research laboratory • Increase education and training space, including an eye surgery award bestowed by RPB, help attract exceptionally tal- simulator, surgical wet lab and dedicated location for international ented basic scientists to careers devoted to eye research. activities To date, the program has supported 45 scientists who seek to devote their research careers to the field of ophthalmology. For more information, contact Dr. Perkins at ophthalmologyupdate@ccf.org. The new building along with renovations to the existing eye building will: • Accommodate an additional 100,000 patients per year • Increase the number of operating rooms from five to eight, incorporating femtosecond laser and other innovative surgical devices • Add more than 50 uniquely designed clinical lanes, with easy navigation for patients with reduced vision • Expand pediatric surgery space • Increase the number of recovery beds, to keep operating rooms at capacity • Double the size and capability of the diagnostic center • E xpand clinical services to include aesthetic surgery, trauma care Adult zebrafish retina stained for cone photoreceptors (green) and and an ophthalmology genetic center the rod photoreceptors (red) 2 Ophthalmology Update | Spring 2013 Strabismus Surgery in Thyroid Eye Disease The medial rectus muscle in a patient with thyroid eye disease has been detached and rests against the globe. Exposure is best obtained with a Helveston Barbie retractor. The muscle will Elias Traboulsi, MD be sutured where the end of the tendon meets the globe with the eye in primary position. Physicians at Cleveland Clinic’s Cole Eye predictability of strabismus surgery. “This is reinserted where it naturally lies. With Institute have recently published 10-year makes for a real challenge for the surgeon,” traditional techniques, the muscle is at- outcome data on a technique for improv- says Dr. Traboulsi. “It is hard to predict how tached to an adjustable suture that can ing the outcomes of strabismus surgery far you will need to move the insertions of and does move over time, allowing for in patients with Graves disease. Devel- those extraocular muscles. The tables that postoperative manipulation, and reop- oped by Elias Traboulsi, MD, Head of the inform the surgeon how many millimeters eration rates vary from 8 to 27 percent. Department of Pediatric Ophthalmology at to adjust the muscles back according to In the revised technique the muscle is Cleveland Clinic, the surgery is intended for the level of prism diopter deviation – which attached directly to the sclera where it is the approximately 5 percent of patients with were developed for use on a pediatric popu- more secure, preventing muscle slippage. thyroid eye disease whose illness necessi- lation - do not work because the muscles tates strabismus surgery. are abnormal.” One of the complications of Graves disease To improve the surgical outcomes, Dr. physicians reported that the final outcome is the development of an orbital inflam- Traboulsi and colleagues developed an after one surgery was good or excellent in matory process involving the extraocular intraoperative relaxed muscle positioning 52 patients (90 percent). “Our outcomes muscles that move the eye, particularly the technique that improves ocular alignment also show that exact measurements of how inferior rectus and medial rectus muscles. and relieves diplopia in the majority of much the eye has drifted one way or the As the muscles become inflamed and surgical patients. other are not as important as previously larger in volume, patients develop proptosis. Additionally, inflamed and stiff muscles lead to restrictive strabismus, diplopia and compression damage to the optic nerve. Decompression surgery, wherein bones of the floor of the orbit’s medial wall are surgically broken, provides more volume for the eye to fall back and relieves pressure on the optic nerve. However, this surgery can consequently cause diplopia and strabismus if muscles are trapped or displaced in newly created openings. In contrast to traditional adjustable stra- In the 10 years of experience on approximately 60 patients at Cleveland Clinic, thought,” adds Dr. Traboulsi. bismus surgery, where muscle position Along with achieving very positive out- changes are made when the patient is comes, this approach removes much of awake, this technique is performed while the surgical estimation where to suture the the patient is under general anesthe- muscle. “I have been told many times that sia. “In the traditional adjustable suture surgeons are relieved to have a method that technique, with the patient awake, we ask is simple and predictable and that provides them to look straight ahead; we adjust such good results,” says Dr. Traboulsi. “It the position of the muscle insertion so takes away a lot of the anxiety about what that they are not seeing double, and then to do for their patients.” we tie the suture at that time,” explains Dr. Traboulsi. With the revised technique, The inflammation-induced fibrosis and the eye is placed straight forward with thickened extraocular muscles limit the the patient asleep and the muscle tendon Contact Dr. Traboulsi at ophthalmologyupdate@ccf.org. clevelandclinic.org/OUSpring3 COle EYe Institute Corne al Surgeons Ma ximize Use of Intraoperative 4 Ophthalmology Update | Spring 2013 Cole Eye Institute anterior segment surgeons are incorporating intraoperative optical coherence tomography (OCT) into almost every aspect of their work, from corneal grafting to LASIK and cataract surgery. William J. Dupps Jr., MD, PhD One procedure for which OCT has proven value is Descemet’s OT HE R U S E S FO R IN T R AO PE R AT I V E O C T stripping automated endothelial keratoplasty (DSAEK), in which Another surgery in which intraoperative OCT is likely to prove high-resolution visualization of the layers of corneal tissue is re- valuable is deep anterior lamellar keratoplasty (DALK), in which quired, says Cole Eye Institute surgeon William J. Dupps Jr., MD, PhD. surgeons attempt to keep the endothelium but replace all other “When you are looking through an operating microscope, you are corneal layers, such as in keratoconus. presented with the en face view,” he says. “You can differentiate DALK is technically challenging and time-consuming as it requires features along the x and y axes, but standard scopes do not provide manual dissection of the stroma from Descemet’s membrane (DM). good capabilities for resolving depth, which is the dimension in About half the time, the surgeon perforates DM and has to convert which so much of the progress in corneal surgery is concentrated.” to a full-thickness transplant. With the native endothelial cells lost, Accurately differentiating corneal layers is essential in treating conditions such as Fuchs dystrophy, in which endothelial cells deteriorate prematurely. “Formerly, Fuchs was best treated by a full-thickness cornea transplant. Now we selectively replace the endothelial cells,” Dr. Dupps says. “One of the biggest technical challenges of this surgery involves achieving adherence of the donor tissue to the posterior surface of the recipient cornea. Early in the learning curve and with more complex cases, surgeons often have to take the patient back to the operating room the next day and rebubble the the risk of rejection dramatically increases, and the surgeon has invested an extra hour or more along the way. “We have started to use OCT to visualize exactly how deep we are during our initial dissection in DALK cases. The technique involves putting a cannula tip deep in the cornea and injecting an air bubble to separate the layers,” Dr. Dupps says. “If the cannula is not deep enough, the bubble doesn’t get to the right plane and opacifies the cornea, obscuring the view. Intraoperative OCT appears to improve our ability to put the air bubble in the right place.” “We think that intraoperative OCT — especially once it is integrated graft to reposition it against the back of the cornea.” into the surgical microscope — will lead to more successful DALK To help prevent that problem and better understand the dynamics procedures and improve the efficiency of the procedure,” he says. of graft adherence, Dr. Dupps and his colleagues now routinely pause He and his colleagues also are using intraoperative OCT in LASIK, during surgery to perform OCT with a handheld FDA-approved unit reviewing the flap before performing the ablation. The thin, tem- that attaches to the operating microscope. The cross-sectional image porary layer of bubbles produced by the femtosecond laser at the clearly depicts the corneal layers, allowing the surgeons to assess flap interface allows excellent visualization of the flap’s dimensions graft position and the presence of interface fluid and make any with OCT before it is lifted. If there is any concern about the flap needed adjustments. “We have incorporated a standardized scan routine so we can start thickness or shape, the surgeon can make an informed decision about whether to lift the flap and proceed with LASIK or modify the to tease out the intraoperative factors that promote adherence and surgical plan based on flap morphology. those that don’t matter as much,” he says. In cataract surgery, they are using intraoperative OCT to image fea- Intraoperative OCT has led Dr. Dupps and his colleagues to tures such as the lens capsule, the geometry of the capsulorrhexis make changes in how they perform DSAEK. Since 2005, Cole Eye and the position of the lens implant. Institute surgeons have used an infusion technique during DSAEK in Dr. Dupps and colleagues Justis Ehlers, MD, and Sunil Srivastava, which a cannula is placed in the anterior chamber to increase pres- MD, are working in their labs and collaborating with microscope and sure in the eye, pushing the graft closer to the back of the cornea. OCT manufacturers to develop a system that integrates the technolo- Intraoperative OCT has shown that graft apposition improves during gies. This work is one of the major focuses of a $3 million grant Cole infusion, but also that sweeping the cornea with a cannula, moving Eye Institute recently received from the Ohio Third Frontier Program from the middle outward to evacuate fluid from the interface while (story on page 2). there is high pressure underneath the graft, has a dramatic effect on reducing the space between graft and host tissue, he says. For more information, contact Dr. Dupps at ophthalmologyupdate@ccf.org. clevelandclinic.org/OUSpring5 Intraoperative OCT for Posterior Segment Surgery 1A 1B Justis P. Ehlers, MD Optical coherence tomography (OCT) has revolution- A PIONEER IN E XPLORING POTENTIAL IN THE OR ized the clinical care of patients across ophthalmology. Many questions remain regarding intraoperative OCT, OCT provides high-resolution cross-sectional ana- including clinical validation of its utility and its ideal tomic information at near histological quality and has role in ophthalmic surgery. At the Ophthalmic Imaging become the critical driver for treatment protocols and Center of Cleveland Clinic Cole Eye Institute, our intraop- patient management for numerous conditions. Perhaps erative OCT research team is actively pursuing answers more than any other area, the diagnosis and manage- for many of these questions. Our PIONEER study is ment of vitreoretinal diseases have been transformed a multisurgeon prospective clinical study examining by this technology. intraoperative OCT across ophthalmic surgery utilizing a The near biopsy-level detail provided by OCT is a natural microscope-mounted SD-OCT probe (Figure 1). Our first complement to the operating room. Intraoperative OCT provides immediate feedback to the surgeon regarding the impact of surgical maneuvers and the status of the surgical objectives. It also is a novel tool for evaluating the pathophysiology and intraoperative dynamics Sunil K. Srivastava, MD associated with various vitreoretinal surgical diseases. The field of intraoperative OCT continues to evolve and is still in its infancy. Integrating OCT technology into the operating room theater is still a limiting factor for many surgeons. Currently, modified tabletop units or handheld OCT probes are the most viable options for surgeons. Microscope-integrated OCT systems have been developed and are being tested; however, these systems are not currently commercially available in the United States. 6 year of enrollment recently ended with more than 250 patients enrolled. V I T REO RE T IN A L A PPL I C AT I O N S A RE M A N Y Vitreoretinal surgical conditions that may benefit from intraoperative OCT include macular holes, epiretinal membranes, proliferative diabetic retinopathy, retinal detachment and vitreomacular traction syndrome. Using intraoperative OCT for macular hole surgery, we have found that significant architectural alterations occur following internal limiting membrane peeling. Utilizing novel software algorithms, we have been able to calculate intraoperative geometric changes to the macular hole following manipulation of the internal Ophthalmology Update | Spring 2013 2A 3A 2B Figure 1: Microscope-mounted OCT probe. The mount allows the system to be utilized entirely draped (A) or left undraped (B). Figure 2: Impact of intraoperative maneuvers on macular hole geometry. Significant changes are noted in macular hole geometry from the pre-peel scan (red) to the post-internal limiting membrane peel scan (B) (yellow). Additionally, increased subretinal hyporeflectivity is noted in the area of peeling (A) (white arrow). Figure 3: Epiretinal membrane and intraoperative OCT. Pre-peel intraoperative OCT scan (A) showing prominent epiretinal membrane (yellow arrow). Post-peel scan (B) confirms removal of the epiretinal membrane (orange arrow) and reveals areas of increased subretinal hyporeflectivity in the areas of peeling (red arrow). limiting membrane, including increased macular hole volume, changes in the base area and increased subretinal hyporeflectivity (Figure 2). These findings may be useful in predicting hole closure rate, an area of active research at Cole Eye Institute. 3B NEW TECHNOLOGIES UNDER DEVLOPMENT The generalizable clinical utility of intraoperative OCT remains unknown. We believe the PIONEER study will begin to answer many of these questions and help identify diseases/procedures that should be specifi- Utilizing intraoperative OCT during retinal detachment cally targeted for the application of intraoperative OCT repair, novel changes to foveal architecture have been technology. Areas of active development include optimal noted, including occult full-thickness macular hole microscope integration, enhanced OCT-friendly surgical formation. The foveal configuration appears to have instrumentation, intraoperative OCT software algorithms prognostic significance for visual outcome and may and optimized display systems. Advances in each of also predict future macular hole formation in these these areas are needed to facilitate truly seamless eyes. For epiretinal membrane surgery, intraopera- integration into the operating room theater. From our tive OCT is proving to be useful in confirming both preliminary research, it seems clear that intraoperative completion of peeling and, conversely, the presence OCT provides new and important information to the sur- of residual membranes requiring attention. Addition- geon in select cases. Identifying those areas of greatest ally, areas of increased subretinal hyporeflectivity are impact on patient care and surgical outcomes continues common following membrane peeling (Figure 3), pos- to be a major focus of the intraoperative OCT research sibly indicating photoreceptor stretching or distortion. team at Cole Eye Institute. The functional significance of this remains unknown. In vitreomacular traction syndrome, intraoperative OCT can be used to confirm release of traction and Contact Drs. Ehlers and Srivastava at ophthalmologyupdate@ccf.org. may reveal small occult unroofing of foveal cysts, which would impact the surgical plan. clevelandclinic.org/OUSpring7 Decade in Medical Publishing Saw Beginning of New Era in the Treatment of Retinal Dise ase I n J a n u a r y 2013, A n d r e w S c h a c h a t , MD, Vice Chairman for Clinical Affairs at the Cole Eye Institute and Director of Clinical Research, stepped down after 10 years of service as Editor-in-Chief of one of the premier journals in the field of ophthalmology, the American Academy of Ophthalmology’s Ophthalmology. During that time, Dr. Schachat has not only seen significant medical changes within ophthalmology, but had helped to usher in those changes. In addition to his own practice in clinical research, his editorial position was critical to relaying those changes to those practicing and performing research in the field. “I had the good fortune to be editor of Ophthalmology during a time of transition from paper publishing to a web-based manuscript management system,” says Dr. Schachat. The consequences of that shift include reducing by 75 percent the time it takes to review a submitted paper. The median time to decision-making once a manuscript is received is now approximately 30 days. “The journal, authors and readers have all benefited from that because we all want timely information,” he adds. “And not only has production gone electronic, but so has digestion of the material.” Although 30,000 copies of Ophthalmology are mailed monthly, most of the articles are consumed online. Since 2003, Dr. Schachat has overseen a significant transition to an increasingly international readership. Today, of the approximately 1,800 manuscripts received yearly at the journal, 72 percent of them are from an international primary author, compared with about half of the manuscripts submitted in 1999. And about half of the journal’s readers are non-U.S. subscribers. “Much of ophthalmology has become very international, and we are really learning much more from each other,” he says. “I think electronic access is largely responsible for that, and it is something that has been exciting to participate in as editor of Ophthalmology.” Advancements in the treatment of certain eye diseases have been particularly striking. In the last three to four years, Dr. Schachat noted tremendous strides related to new drugs and new treatments in leading retinal diseases such as macular degeneration and diabetic retinopathy. When Dr. Schachat became Editor-in-Chief, 8 Ophthalmology Update | Spring 2013 “Much of ophthalmology has become very international, and we are really learning much more from each other. I think electronic access is largely responsible for that, and it is something that has been exciting to participate in as editor of Ophthalmology.” – Andrew Schachat, MD the field of ophthalmology lacked an anti-VEGF therapy. “When I became editor, 90 percent of patients with macular degeneration lost vision,” he recalls. “Now, anti-VEGF therapy is the norm, and 90 percent of treated patients have stable disease.” The surge in refractive surgery over the past decade has continued as more patients choose elective laser surgery to eliminate the need to wear glasses. The results have been so successful that patients who are inconvenienced by eyewear now consider the treatment normative. Similarly, Dr. Schachat has seen a great change in patient outcomes and expectations for cataract surgery over the past 10 years. He comments that the expectation for fantastic outcomes in cataract surgery clearly has continued to increase tremendously. “The expectation used to be to get back to better vision,” he adds. “Now the expectation is to get back to better vision faster, with very high and specific patient demands for superb outcomes that 10 years ago were not really possible but are today.” Looking forward, Dr. Schachat embraces the “absolute revolution” in the number of papers related to genetics of eye diseases. “We don’t have treatments yet but there has been a revolution in figuring out what the defect is or what has gone wrong,” he says. “I think in the next 10 to 20 years we should see an explosion in targeted therapies for genetic diseases.” He is also encouraged by the engineering tour de force exhibited in artificial retina devices. “I think in the next 10 years, if that moves ahead at a third or even a tenth of the pace that computers moved ahead, there are going to be tremendous advances for patients.” He is also hopeful that the increasingly large amount of data and promise in understanding the underlying mechanisms involved in glaucoma will result in significant leaps in glaucoma therapy. “It has been a privilege to serve as the Editor-in-Chief of Ophthalmology,” says Dr. Schachat, who will remain on the journal’s editorial board and continue to manage retinarelated manuscripts. “It has been a fantastic opportunity to have been in a leadership role at a time when both the business of medical publishing and the treatment of some important eye diseases have changed so substantially.” Retina , Fifth Edition, now available Just released, Retina, Fifth Edition, published by Elsevier, is the most comprehensive reference to date about retinal diagnosis, treatment, development, structure, function and pathophysiology. The three-volume set draws on the extensive knowledge and experience of editors Stephen J. Ryan, MD; Andrew P. Schachat, MD (Vice Chairman of Cleveland Clinic Cole Eye Institute); Charles P. Wilkinson, MD; David R. Hinton, MD; SriniVas R. Sadda, MD; and Peter Wiedemann, MD. With insights from hundreds of world authorities across Europe, Asia, Australasia and the Americas, Retina, Fifth Edition, will keep ophthalmologists on the leading edge of today’s newest technologies, surgical approaches, and diagnostic and therapeutic options for retinal diseases and disorders. clevelandclinic.org /OUSpring9 Blood Biomarkers to Guide Surveillance and Treatment of Uveal Melanoma Being Explored Overall mortality in uveal melanoma is high due to Arun D. Singh, MD metastatic disease that develops despite advances in its E arly B iomarkers of Micrometastases Needed diagnosis and improvements in local tumor control. Several The identification and validation of blood biomarkers may lines of evidence indicate that micrometastases are pres- permit early detection of uveal melanoma metastasis and ent in many patients with uveal melanoma at the time of could potentially allow for adoption of effective strategies ophthalmic diagnosis. In partnership with Pierre Triozzi, to suppress micrometastases before they progress, thereby MD, of the Taussig Cancer Institute, we have explored new improving prognosis. Cole Eye Institute is actively exploring options to treating this challenging disease. An effective the utility of immune regulation factors in the blood and strategy to improve survival in uveal melanoma would be to other new blood biomarkers in an effort to better define identify patients with micrometastases and suppress those prognosis and monitor disease progression in patients with micrometastases before they progress to macrometastases. uveal melanoma. Chromosomal aberrations (monosomy-3 and others) and gene expression profiling of tumors are superior to clinical and histopathological factors in predicting metastasis. Detection of circulating melanoma cells is a convenient test that may be potentially useful for diagnosis, risk stratification, identification of metastasis and treatment monitor- Fine-needle aspiration biopsy of tumors at the time of local ing in uveal melanoma. The results of polymerase chain therapy (plaque radiation), tumor resection and enucleation reaction-based and immunomagnetic techniques tested to are the methods applied to obtain material for molecular date are controversial and cannot be interpreted reliably. prognostication. The time from diagnosis of the primary tumor to discovery of metastasis can range from weeks to decades. Assessment of tumor tissue, however, does not indicate whether tumor cells have actually been shed or are forming metastasis, and whether adjuvant treatment is reducing micrometastasis. A variety of blood constituents, ranging from melanoma-associated mRNA, vascular endothelial growth factor, hepatocyte growth factor, epidermal growth factor and insulin-like growth factor-1 (IGF-1) have been implicated in progression of uveal melanoma and are measurable in patient serum or in experimental models of uveal melanoma. For various biological and technical reasons, these biomarkers have not demonstrated to date the sensitivity, specificity and predictive values necessary to monitor metastasis in patients with uveal melanoma. Beta2-microglobulin (B2M) is a component of the HLA class I molecule light chain. Like the HLA class I heavy chain, tumor B2M expression by immunohistochemistry has been associated with metastasis in uveal melanoma. Because it is noncovalently associated, B2M can circulate. We studied 76 patients, 47 treated by plaque brachytherapy and 29 treated by enucleation. Thirty-three (43 percent) of the tumors manifested monosomy-3. Most tumors were large, were located in the choroid and were of mixed cell type. Blood was drawn in patients without metastatic disease prior to fine-needle aspiration biopsy. Tumor chromosome 3 status was determined by fluorescence in situ hybridization. Levels of B2M, IGF-1 and insulin-like growth factor-binding protein-3 (IGFBP-3) were determined by enzyme-linked immunosorbent assays. Blood levels of IGF-1 Figure. Fundus photograph of a large choroidal melanoma and IGFBP-3 were not associated with tumor monosomy-3. In contrast, increases in blood B2M (p ≤ 0.02) were. 10 Ophthalmology Update | Spring 2013 CME Opportunitie s The independent association of increased blood level of B2M and tumor monosomy-3 status was confirmed in multivariable analysis. Measuring blood levels of B2M in patients with primary uveal Mark your calendars for continuing medical education melanoma may therefore have prognostic value and symposia hosted by Cole Eye Institute. You’ll gain insights may help guide surveillance and adjuvant therapy recommendations. For more information, contact Drs. Singh and Triozzi at ophthalmologyupdate@ccf.org. References 1. Schaller UC, Bosserhoff AK, Neubauer AS, et al. Melanoma inhibitory activity: a novel serum marker for uveal melanoma. Melanoma Res. 2002 Dec;12(6):593-599. 2. Missotten GS, Tang NE, Korse CM, et al. Prognostic value of S-100-beta serum concentration in patients with uveal melanoma. Arch Ophthalmol. 2003 Aug;121(8):1117-1119. 3. Callejo SA, Antecka E, Blanco PL, Edelstein C, Burnier MN, Jr. Identification of circulating malignant cells and its correlation with prognostic factors and treatment in uveal melanoma. A prospective longitudinal study. Eye (Lond). 2007 June; 21(6):752-759. 4. Ulmer A, Beutel J, Süsskind D, et al. Visualization of circulating melanoma cells in peripheral blood of patients with primary uveal melanoma. Clin Cancer Res. 2008 Jul;14(14):4469-4474. 5. Triozzi PL, Singh AD. Blood biomarkers of uveal melanoma metastasis. Br J Ophthalmol. 2011 Jan;95(1):3-4. 6. Crosby MB, Yang H, Gao W, Zhang L, Grossniklaus HE. Serum VEGF levels correlate with number and location of micrometastases in a murine model of uveal melanoma. Br J Ophthalmol. 2011 Jan;95(1):112-117. 7. Torres V, Triozzi P, Eng C, Tubbs R, Schoenfiled L, Crabb JW, Saunthararajah Y, Singh AD. Circulating tumor cells in uveal melanoma. Future Oncol. 2011;7:101-9. 8. Singh AD, Turell ME, Topham AK. Uveal melanoma: trends in incidence, treatment, and survival. Ophthalmology. 2011 Sep;118(9):1881-1885. 9. Triozzi PL, Singh AD. Blood biomarkers for uveal melanoma. Future Oncol. 2012 Feb;8(2):205-215. 10. Turell ME, Tubbs RR, Biscotti CV, Singh AD. Uveal melanoma: prognostication. Monogr Clin Cytol. 2012 Oct;21:55-60. 11. Triozzi PL, Elson P, Aldrich W, Achberger S, Tubbs R, Biscotti CV, Singh AD. Elevated blood beta-2 microglobulin is associated with tumor monosomy-3 in patients with primary uveal melanoma. Melanoma Res. 2013;23:1-7. into state-of-the-art diagnostic, medical and surgical techniques and learn about the promise that research holds for patients with ophthalmic conditions. Ophthalmic Ultrasonography: Practical Aspects For ophthalmologists, optometrists, nurses, technicians, photographers and others Friday-Saturday, March 15-16, 2013 Location: InterContinental Hotel and Conference Center, Cleveland, Ohio Activity Directors: Arun D. Singh, MD Brandy Hayden Uveitis Update For general ophthalmologists, uveitis and vitreoretinal specialists, Internists, rheumatologists, and pulmonary and paramedical personnel Saturday, April 20, 2013 Location: InterContinental and Conference Center, Cleveland, Ohio Activity Directors: Careen Lowder, MD, PhD Sunil K. Srivastava, MD Retina Summit For vitreoretinal specialists North Coast Retina Symposium IV For vitreoretinal specialists Friday-Saturday, May 17-18, 2013 Location: Cole Eye Institute, Cleveland, Ohio Activity Directors: Daniel F. Martin, MD Sunil K. Srivastava, MD Optical Coherence Tomography & Imaging: Panel Experts Review (OCTIPER) For vitreoretinal specialists Friday, August 23, 2013 Location: Toronto, Canada Activity Directors: Peter Kaiser, MD Sunil K. Srivastava, MD Justis P. Ehlers, MD International Society of Ocular Oncology (ISOO 2013) - NON-CME For ophthalmic oncologists, ophthalmologists, medical students, residents and fellows Friday, May 3, 2013 (pre-ARVO) Sunday-Thursday, Sept. 29-Oct. 3, 2013 Location: The W Seattle Hotel Seattle, Wash. Location: InterContinental Hotel and Conference Center, Cleveland, Ohio Activity Directors: Peter Kaiser, MD Sunil K. Srivastava, MD Activity Director: Arun D. Singh, MD For details, exact locations or to confirm dates for any of our 2013 CME courses, please contact Jane Sardelle at sardelj@ccf.org. clevelandclinic.org/OUSpring11 Distinguished Lecture Series Cole Eye Institute is proud to present the 2013 Distinguished Lecture Series, which provides a forum for internationally renowned researchers in the visual sciences to present their latest findings on basic and clinical ophthalmic research. Ample opportunity for questions and answers is provided after lectures. Feb. 21, 2013 May 16, 2013 Nov. 21, 2013 Mitochondrial Dysfunction: A Potential Mechanism for Age-Related Macular Degeneration Lerner Research Institute, NA1-140 Global Blindness: Can We Control It? Lerner Research Institute, NA1-140 Leukocytes Take Directives from the Extracellular Matrix in Ocular Infections and Inflammation Location: TBD Deborah Ferrington, PhD Associate Professor Departments of Ophthalmology and Visual Neurosciences University of Minnesota Minneapolis, Minn. March 14, 2013 The Role of the Choriocapillaris in Early AMD Lerner Research Institute, NA1-140 Robert Mullins, PhD Hansjoerg E.J.W. Kolder, MD, PhD Associate Professor of Best Disease Research, Department of Ophthalmology & Visual Sciences University of Iowa Iowa City, Iowa April 18, 2013 Genetic Control of Angiogenesis: Implications for ARMD Lerner Research Institute, NA1-140 Robert D’Amato, MD, PhD Judah Folkman Chair in Surgery Professor of Ophthalmology Harvard Medical School Vascular Biology Program Boston Children’s Hospital Boston, Mass. 12 Gullapalli Rao, MD Chairman, LV Prasad Eye Institute L V Prasad Marg Banjara Hills Hyderabad, Andhra Pradesh India Sept. 19, 2013 Responding to Clinical Need: Taking OCT Imaging Beyond Standard Clinical Applications Location:TBD Cynthia A. Toth, MD Professor of Ophthalmology and Biomedical Engineering Duke University Eye Center Durham, N.C. Oct. 17, 2013 The Hypoxic Response: Sought and Dreaded by the Retina Location:TBD Shukti Chakravarti, PhD Professor Departments of Medicine, Cell Biology and Ophthalmology Johns Hopkins University School of Medicine Baltimore, Md. Please join us for these insights into ophthalmic research and the promises they hold for patient care. No registration is required; call 216.444.5832 with any questions. The Distinguished Lecture Series is held from 7 to 8 a.m., in the locations listed; check our website for locations of events that are listed as TBD. Attendees should park in the East 102nd Street parking lot (facing the front of Cole Eye Institute) or the visitor’s parking garage at East 100th Street and Carnegie Avenue. We will validate your parking ticket. Christian Grimm, PhD Professor for Experimental Ophthalmology Department of Ophthalmology University of Zurich Schlieren, Zurich Switzerland Ophthalmology Update | Spring 2013 Clinical Trials All studies have been approved by the Institutional Review Board. The featured studies are currently enrolling. Retinal Diseases Uveitis Ozurdex for Diabetic Macular Edema Treated with Pars Plana Vitrectomy and Membrane Removal (OPERA) A Proof-of-Concept Study of Intravitreal LFG316 in Patients with Multifocal Choroiditis (MFC) Objective: This study will evaluate the use of Ozurdex in patients needing surgery for epiretinal membrane with diabetic macular edema. Objective: The study is designed to provide information on the safety, tolerability, pharmacokinetics, pharmacodynamics and efficacy of successive intravenous doses of LFG316 in eligible patients with neovascular age-related macular degeneration. R Contact: Sunil Srivastava, MD, 216.636.2286 or Kim Baynes, 216.444.2566 Investigator-Initiated Observational Study of Intravitreal Aflibercept Injection for Exudative Age-Related Macular Degeneration Previously Treated with Ranibizumab or Bevacizumab Objective: This observational study will assess the efficacy of intravitreal aflibercept injection in subjects previously treated with ranibizumab or bevacizumab on central retinal thickness as measured by spectral domain optical coherence tomography (SDOCT). Contact: Rishi P. Singh, MD, 216.445.9497, or Stephanie Bennett, 216.445.6497 Fluocinolone Acetonide Intravitreal Inserts for Vein Occlusion in Retina (FAVOR) Objective: This study will assess the safety and efficacy of fluocinolone acetonide intravitreal inserts in subjects with macular edema secondary to RVO. Contact: Peter K. Kaiser, MD, 216.444.6702, or Gail Kolin, RN, 216.445.4086 Contact: Sunil Srivastava, MD, 216.636.2286, or Laura Holody, 216.445.3762 Pediatric Eye Disease HTS1-Glasses vs. Observation for Moderate Hyperopia in Young Children Objective: The purpose of this study is to compare visual acuity outcomes and development of strabismus after a three-year follow-up period in children ages 12 to < 60 months with moderate hyperopia who are prescribed glasses either immediately or only after confirmation of prespecified deterioration criteria. Contact: Elias Traboulsi, MD, 216.444.4363, or Sue Crowe, 216.445.3840 Bilateral Lateral Rectus Recession vs. Unilateral Recess-Resect for Intermittent Exotropia (IXT1) Objective: The purpose of this study is to evaluate the effectiveness of bilateral lateral rectus muscle recession vs. unilateral lateral rectus recession with medial rectus resection procedures for the treatment of strabismus. Contact: Elias Traboulsi, MD, 216.444.4363, or Sue Crowe, RN, 216.445.3840 Increasing Patching for Amblyopia in Children 3 to < 8 Years Old (ATS15) Objective: This study is designed to evaluate the effectiveness of increasing prescribed patching treatment after visual acuity has stabilized with initial treatment and amblyopia is still present. Contact: Elias Traboulsi, MD, 216.444.4363, or Sue Crowe, RN, 216.445.3840 Genetics Molecular Genetics of Eye Diseases Objective: The objective of this project is to study the molecular genetics of ophthalmic disorders through the compilation of a collection of DNA, plasma and eye tissue samples from patients and from families with a broad range of eye diseases and malformations. Contact: Elias Traboulsi, MD, 216.444.4363, or Sonal Uppal, PhD, 216.444.7137 Cornea/Refractive Surgery LASIK Flap Thickness and Visual Outcomes Using the WaveLight FS200 Femtosecond Laser Objective: To evaluate the visual outcome, accuracy and predictability of LASIK flap thickness using the new WaveLight® FS200 femtosecond laser and compare these results to those obtained using the IntraLaseTM FS60 femtosecond laser. Contact: Ronald Krueger, MD, 216.444.8158, or Laura Holody, 216.445.2264 Continued on next page clevelandclinic.org/OUSpring13 Clinical Trials continued from previous page Ophthalmology Update, a publication of Cleveland Clinic’s Cole Eye Institute, provides information for ophthalmologists about state-of-the-art diagnostic and management techniques and current research. Please direct any correspondence to: Long-Term Safety Follow-up for Subjects Previously Implanted with the AcrySof Cachet Phakic Lens in Clinical Studies C-02-23, C-02-40, C-03-21 and C-05-57 Objective: To estimate the annualized endothelial cell loss rate (for up to 10 years following date of implantation) of subjects previously implanted with the L-series AcrySof® Cachet™ Phakic Lens from clinical studies. Contact: Ronald Krueger, MD, 216.444.8158, or Laura Holody, 216.445.2264 Other Open Studies Safety Study of a Single IVT Injection of QPI-1007 in Chronic Optic Nerve Atrophy and Recent-Onset NAION Patients (NAION) Contact: Rishi P. Singh, MD, 216.445.9497, or Laura Holody, 216.445.2264 The following studies have completed patient enrollment in the past year at Cole Eye Institute and are in follow-up: Home Vision Monitoring Using the ForseeHomeTM Device Following Treatment of Neovascular Age-Related Macular Degeneration Comparing the Effectiveness of Treatment Strategies for Primary Open-Angle Glaucoma A Phase II Dose-Ranging Study of Pazopanib to Treat Neovascular Age-Related Macular Degeneration (GSK AMD) Objective: This is an open-label, dose escalation, safety, tolerability and pharmacokinetic study, where the active study drug (QPI-1007) will be given to all patients who participate. This study will determine whether QPI-1007 is safe when it is injected into the eye. The study will also reveal if there are any side effects of the drug and how long it takes for the body to clear the drug. Cleveland Clinic E xecutive Education Learn From Top Healthcare Executives ophthalmologyupdate@ccf.org Institute Chairman Daniel F. Martin, MD Managing Editor Kimberley Sirk Art Director Michael Viars Marketing Manager Bill Sattin, PhD Marketing Associate Mary Anne Connor Cole Eye Institute, one of 26 institutes at Cleveland Clinic, is one of the few dedicated, comprehensive eye institutes in the world. Our internationally recognized staff diagnoses and treats the entire spectrum of eye conditions, caring for more than 170,000 patients and performing more than 7,500 surgeries annually. Cleveland Clinic is a nonprofit, multispecialty academic medical center consistently ranked among the top hospitals in America by U.S. News & World Report. Founded in 1921, it is dedicated to providing quality specialized care and includes an outpatient clinic, a hospital with more than 1,300 staffed beds, an education institute and a research institute. Ophthalmology Update is written for physicians and should be relied on for medical education purposes only. It does not provide a complete overview of the topics covered and should not replace the independent judgment of a physician about the appropriateness or risks of a procedure for a given patient. Physicians who wish to share this information with patients need to make them aware of any risks or potential complications associated with any procedures. © 2013 The Cleveland Clinic Foundation The competencies needed to lead and manage differ from those needed to be an effective administrator, clinician or scientist. Take advantage of this opportunity to acquire skills and insights into the business of healthcare excellence from top executives at Cleveland Clinic. Two-day and two-week programs are open to healthcare executives, including physicians, nurses and administrators. Visit clevelandclinic.org/ExecutiveEducation for details, including the opportunity to earn 72.5 CME credits. 14 Ophthalmology Update | Spring 2013 Cole Eye Institute Staff Chairman, Cole Eye Institute Daniel F. Martin, MD............................................ 216.444.0430 Institute Vice Chairman | Institute Quality Review Officer Andrew P. Schachat, MD....................................... 216.444.7963 Institute Vice Chairman for Education Elias I. Traboulsi, MD........................................... 216.444.2030 Comprehensive Ophthalmology John Costin, MD.................................................. 440.988.4040 Richard E. Gans, MD, FACS.................................. 216.444.0848 Philip N. Goldberg, MD ....................................... 216.831.0120 Michael Gressel, MD............................................ 440.988.4040 Mohinder Gupta, MD............................................ 419.289.6466 Martin A. Markowitz, MD ..................................... 440.461.4733 Shari Martyn, MD ............................................... 216.831.0120 Peter McGannon, MD........................................... 216.529.5320 Michael E. Millstein, MD ...................................... 216.831.0120 Wynne Morley, MD............................................... 440.366.9444 Sheldon M. Oberfeld, MD .................................... 440.461.4733 Allen S. Roth, MD ............................................... 216.831.0120 David B. Sholiton, MD ......................................... 216.831.0120 Scott A. Wagenberg, MD ...................................... 440.461.4733 Cornea and External Disease William J. Dupps Jr., MD, PhD.............................. 216.444.2020 Jeffrey M. Goshe, MD........................................... 216.444.0845 Roger H.S. Langston, MD ..................................... 216.444.5898 Martin A. Markowitz, MD ..................................... 440.461.4733 Peter McGannon, MD........................................... 440.529.5320 David M. Meisler, MD .......................................... 216.444.8102 Wynne Morley, MD............................................... 440.366.9444 Sheldon M. Oberfeld, MD .................................... 440.461.4733 Allen S. Roth, MD ............................................... 216.831.0120 Scott A. Wagenberg, MD ...................................... 440.461.4733 Steven E. Wilson, MD .......................................... 216.444.5887 Glaucoma Jonathan A. Eisengart, MD ................................... 216.445.9429 Edward J. Rockwood, MD .................................... 216.444.1995 Shalini Sood-Mendiratta, MD................................ 216.445.5277 Keratorefractive Surgery William J. Dupps Jr., MD, PhD.............................. 216.444.2020 Ronald R. Krueger, MD, MSE................................. 216.444.8158 Michael E. Millstein, MD ...................................... 216.831.0120 Allen S. Roth, MD ............................................... 216.831.0120 Steven E. Wilson, MD .......................................... 216.444.5887 Neuro-Ophthalmology Gregory S. Kosmorsky, DO.................................... 216.444.2855 Lisa D. Lystad, MD ............................................. 216.445.2530 Oculoplastics and Orbital Surgery Mark Levine, MD................................................. 440.988.4040 Julian D. Perry, MD ............................................. 216.444.3635 Ophthalmic Anesthesia Marc A. Feldman, MD ......................................... 216.444.9088 M. Inton-Santos, MD............................................ 216.445.1016 J. Victor Ryckman, MD......................................... 216.444.6330 Sara Spagnuolo, MD ............................................ 216.444.6324 Ophthalmic Oncology Arun D. Singh, MD .............................................. 216.445.9479 Ophthalmic Research Bela Anand-Apte, MBBS, PhD............................... 216.445.9739 Vera Bonilha, PhD................................................ 216.445.7960 John W. Crabb, PhD............................................. 216.445.0425 William J. Dupps Jr., MD, PhD.............................. 216.444.2020 Stephanie Hagstrom, PhD..................................... 216.445.4133 Joe G. Hollyfield, PhD.......................................... 216.445.3252 Neal S. Peachey, PhD........................................... 216.445.1942 Brian Perkins, Ph.D.............................................. 216.444.9683 Pediatric Ophthalmology and Adult Strabismus Fatema Ghasia, MD............................................. 216.444.0999 Andreas Marcotty, MD ......................................... 216.831.0120 Paul Rychwalski, MD .......................................... 216.444.4821 Elias I. Traboulsi, MD .......................................... 216.444.2030 Retina Amy Babiuch, MD................................................ 440.366.9444 Ryan Deasy, MD.................................................. 440.695.4010 Justis P. Ehlers, MD ............................................. 216.636.0183 Peter K. Kaiser, MD ............................................. 216.444.6702 Daniel F. Martin, MD ........................................... 216.444.0430 Andrew P. Schachat, MD ...................................... 216.444.7963 Jonathan E. Sears, MD......................................... 216.444.8157 Rishi P. Singh, MD............................................... 216.445.9497 Sunil K. Srivastava, MD........................................ 216.636.2286 Richard Wyszynski, MD........................................ 440.988.4040 Alex Yuan, MD..................................................... 216.444.0079 Uveitis Careen Y. Lowder, MD, PhD.................................. 216.444.3642 Sunil K. Srivastava, MD........................................ 216.636.2286 Patient Referrals To refer a patient to Cole Eye Institute, please call 216.444.2020 or 800.223.2273, ext 42020. clevelandclinic.org/OUSpring15 Cole Eye Institute The Cleveland Clinic Foundation 9500 Euclid Avenue / AC311 Cleveland, OH 44195 Ophthalmology Update 24/7 Referrals Referring Physician Hotline 855.REFER.123 (855.733.3712) Physician Directory View all Cleveland Clinic staff online at clevelandclinic.org/staff. Track Your Patient’s Care Online DrConnect is a secure online service providing real-time Hospital Transfers information about the treatment your patient receives 800.553.5056 at Cleveland Clinic. Establish a DrConnect account at On the Web at clevelandclinic.org/refer123 Stay connected with us on … Twitter/YouTube/Facebook clevelandclinic.org/drconnect. Critical Care Transport Worldwide Cleveland Clinic’s critical care transport teams and fleet of vehicles are available to serve patients across the globe. •T o arrange for a critical care transfer, call 216.448.7000 or 866.547.1467 (see clevelandclinic.org/criticalcaretransport). About Cleveland Clinic Cleveland Clinic is an integrated healthcare delivery system with local, national and international reach. At Cleveland •F or STEMI (ST elevated myocardial infarction), acute stroke, ICH (intracerebral hemorrhage), SAH (subarachnoid hemorrhage) or aortic syndrome transfers, call 877.379.CODE (2633). Clinic, 2,800 physicians represent 120 medical specialties Outcomes Data and subspecialties. We are a main campus, 18 family health View clinical Outcomes books from all Cleveland Clinic centers, eight community hospitals, Cleveland Clinic Florida, institutes at clevelandclinic.org/outcomes. the Cleveland Clinic Lou Ruvo Center for Brain Health in Las Vegas, Cleveland Clinic Canada, Sheikh Khalifa Medical City and Cleveland Clinic Abu Dhabi. In 2012, Cleveland Clinic was ranked one of America’s top 4 hospitals in U.S.News & World Report’s annual “America’s Best Hospitals” survey. The survey ranks Cleveland Clinic among the nation’s top 10 hospitals in 14 specialty areas, and as the top hospital in three of those areas. Clinical Trials We offer thousands of clinical trials for qualifying patients. Visit clevelandclinic.org/clinicaltrials. CME Opportunities: Live and Online The Cleveland Clinic Center for Continuing Education’s website offers convenient, complimentary learning opportunities. Visit ccfcme.org to learn more and use Cleveland Clinic’s myCME portal (available from the site) to manage your CME credits. Resources for Physicians Executive Education Referring Physician Center and Hotline leaders — the Executive Visitors’ Program and the two-week Samson Cleveland Clinic’s Referring Physician Center has established Global Leadership Academy immersion program. Visit clevelandclinic. a 24/7 hotline — 855.REFER.123 (855.733.3712) — to org/executiveeducation. streamline access to our array of medical services. Contact the Referring Physician Hotline for information on our clinical specialties and services, to schedule and confirm patient appointments, for assistance in resolving service-related issues, and to connect with Cleveland Clinic specialists. Cleveland Clinic has two education programs for healthcare executive Same-Day Appointments Cleveland Clinic offers same-day appointments to help your patients get the care they need, right away. Have your patients call our sameday appointment line, 216.444.CARE (2273), or 800.223.CARE (2273).