Metabolism and Digestion-Lecture 2-Gastric Secretion and Motility
advertisement

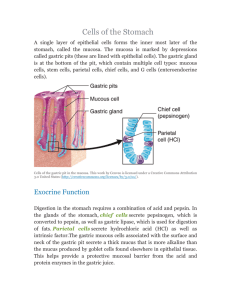
Human Form & Function 2 Gastric Secretion & Motility Dr. Neil Docherty My Teaching Objec/ves • Describe the physiological basis of gastric motility and secretion and explain how they contribute to digestion • Identify the synergies that exist between maximal gastric secretion and motility • Highlight the importance of the pyloric sphincter and the mucus gel barrier and how damage to them is associated with disease The Stomach • Infolded muscular bag lined by glandular epithelium involved in sterilization, preliminary digestion/capture and storage of nutrient Key Phenomena: 1) Filling and Mixing (Motility based Phenomena) Involves-relaxation/contraction of smooth muscle Controlled by-mechanosensitive induction of neural circuitry and endocrine messengers 2) Digestion (Secretion Based Phenomena) Involves the release of glandular secretions Controlled by-chemosensitive and mechanosensitive induction of neural circuitry and endocrine messengers The Stomach FUNDUS-BODY-ANTRUM -Large reservoir capacity -HCl, pepsinogen and intrinsic factor All areas secrete -mucous -bicarbonate -Hormone production -Major site of muscular contraction Major Gastric Secretory Products PRODUCT HCl Intrinsic Factor SOURCE FUNCTION Parietal cell Hydrolysis, sterilisation " Vitamin B12 absorption Pepsinogen Chief cell Protein digestion Mucus Mucous cell Gastric protection Trefoil Factors " " Bicarbonate Parietal cell " Histamine ECL cells Gastrin G cells " Gastrin releasing peptide Nerves " Acetylcholine Nerves " Somatostatin D cells " Regulation of secretion Gastric Glands and Their Secretions Entero-endocrine cells Specialised cells in epithelial lining of intestine which release short peptide hormones Parietal Cell Rearrangements During HCl Secretion canaliculi Fusion of canaliculi and tubulovesicles with plasma membrane Tubulovesicles (inc. H+/K+ ATPase) cAMP/Ca2+ ACh Histamine Gastrin Parietal Cell Rearrangements During HCl Secretion Why all the mitochondria?? -Think active transport H+/K+ ATPase T.E.M.x9600 Cellular Physiology of Acid Secre/on -­‐Ion Fluxes in HCl secre/on K+ channel L U M E N 2K+ K+ K+ H+ Cl- H2O + CO2 Carbonic anhydrase II H+/K+ ATPase Cl- channel Na+/ K+ ATPase H+ + HCO3Cl- 3Na+ Cl-/HCO3exchanger HCO3- START HERE!-Secretory stimuli induce apical plasma membrane localization!!! HCl N.B. Low pH causes autoactivation Of pepsinogen from Chief cells Clinical Correlate -Proton Pump Inhibitors H2 antagonists Gastric HCl Secre/on Overview • Parietal cell in fundic mucosa • Basolateral stimulation with ACh,gastrin and histamine • Stimulation causes profound morphological changes • Cytoskeletal rearrangement, increase in apical surface area densely covered in H+/K+ ATPase • Carbonic Anhydrase II generated H+ secretion matches Cl- secretion into lumen Protection of Gastric Mucosa Secondary Gastroprotective Effects of Basolateral HCO3- Secretion Bloodstream Transport towards luminal mucosa in gastric microvasculature Apical secretion by surface Mucosa=GASTROPROTECTION Negative Feedback Control Duodenal Mucosa Antral G cells fat GIP Bloodstream D cells Somatostatin (-ve reg.) ECL histamine cells Gastrin Chief cells Parietal cells peptides Pepsin +VE -VE Acid Secretion Pepsinogen Secretion Summary • • • • • • • Positive Mechanical Stretch Gastrin Histamine ACh GRP Pepsin derived, peptideinduced, gastrin release • Alcoholic Drinks • Coffee • Negative • pH sensitive D cell somatostatin release • Presence of fat in duodenum causes gastric inhibitory peptide (GIP) release The Three Phases of Gastric Secretion • • • Cephalic Gastric Intestinal Cephalic phase • Higher centres, (sight,smell, taste, anticipation) • Vagal efferents • Stimulation of secretory and motor responses • Direct (Ach-G-cell-Gastrin) • Indirect 1) (ACh-ENS-GRP-G-cells-Gastrin) 2) (ACh-ECL cells-Histamine-G-cells Gastrin) Gastric phase • Quan/ta/vely most important • Short and long reflexes (mechanical, vago-­‐vagal) • Amplifica<on of secre<on • Recep<ve relaxa<on • Increased gastric blood flow • Sustained secre<on possible due to buffering capacity of luminal protein on bulk content pH Intestinal phase • D cell mediated somatostatin release • Duodenal mucosa GIP release Leads to • Reduction in secretory activity • Residual secretory activity serves to sterilize stomach ahead of next meal Gastric Motility Physical Functions of Stomach Reservoir Homogeniser Control of delivery Small particle formation emulsification SMOOTH MUSCLE RELATED FUNCTIONS Basal Electrical Rhythm Slow wavedepolarisation of smooth muscle Pacemaker potential (greater curvature origin) determines: FREQUENCY, VELOCITY and DIRECTION Only result in contraction when superimposed with stimuli sufficient to generate an action potential 3 cycles/min e.g ACh release from vago-vagal response to baroreceptor stimulation Relaxation of Stomach Upon Feeding DEF: Relaxation of stomach to increase volume RESERVOIR FUNCTION Two reflexes 1 Receptive Swallowing 2 Accomodative Following gastric mechanoreceptor stimulation Adaptive Relaxation Involves the same mediators as gastric secretion and input from Arrival of bolus in duodenum Contraction and Mixing and Grinding Fed pattern motility Distal stomach Rapid phasic contractions Gastric Emptying Following feeding Pyloric Sphincter duodenal feedback OPEN CLOSED Only small triturated particles <2mm can pass Effect of Composition on Gastric Emptying Lag phase prolonged further by fatty meals due to endocrine derived negative feedback on pyloric sphincter opening induced by Hormone release in the duodenum Gastric Motility During Fasting Migratory Motor Complexes 100 mins Phase 1: 40-60% of cycle=quiescence Phase 2: =low grade contraction Phase 3: 5-10% of cycle=intense contractions pylorus fully open Phase 3 antral contractions In dog ONSET OF FEEDING In response to fasting induced motilin release from duodenum Gastroparesis Collection of disorders Delayed gastric emptying Satiety, nauseas vomiting Systemic disease related neuromuscular dysfunction (diabetes mellitus-vagal nerve dysfunction) Vagal nerve injury during surgery Small liquid based meals low in fat recommended Why???? Your Learning from Today Should focus on being able to; • Describe the physiology basis of gastric motility and secretion and explain how they contribute to digestion • Link gastric secretion and motility in terms of activators • Appreciate and describe the importance of the pyloric sphincter and the mucus gel barrier and how damage to them is associated with disease