Apr03: FIXATION OF THE ANTERIOR MALLEAR LIGAMENT
advertisement

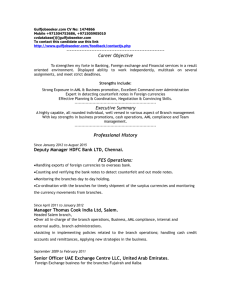
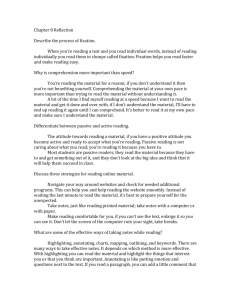
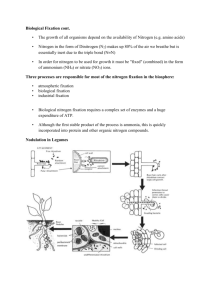
Ann Otol Rhinol Laryngol 112:2003 Ann Otol Rhinol Laryngol 112:2003 REPRINTED FROM ANNALS OF OTOLOGY, RHINOLOGY & LARYNGOLOGY April 2003 Volume 112 Number 4 COPYRIGHT© 2003, ANNALS PUBLISHING COMPANY FIXATION OF THE ANTERIOR MALLEAR LIGAMENT: DIAGNOSIS AND CONSEQUENCES FOR HEARING RESULTS IN STAPES SURGERY ALEXANDER HUBER, MD ZURICH, SWITZERLAND TAKUJI KOIKE, PHD HIROSHI WADA, PHD SENDAI, JAPAN SENDAI, JAPAN VEL NANDAPALAN, MD UGO FISCH, MD LIVERPOOL, ENGLAND ZURICH, SWITZERLAND In the search for possible causes of unfavorable results after stapes surgery, the study reported here focused on the anterior mallear ligament, since it has been previously reported that partial mallear fixation (PMF) leads to functional failure in 38% of cases of stapes revision surgery. The aims of the study were to identify effective methods for the diagnosis of PMF and experimentally assess the conductive hearing loss that results from PMF. The study included vibration amplitude measurements of the ossicles by laser Doppler interferometry (LDI) in 19 patients and 5 fresh human temporal bone (TB) specimens. Analysis of their dynamic behavior was performed by finite element modeling (FEM). Similar, significant changes of manubrium vibration patterns for PMF were found by FEM calculations, in TB experiments, and in patients. We could identify PMF either before operation, using LDI, or during operation, by manual palpation. In the TB experiments and FEM calculations, the attenuation of the stapes displacement due to an isolated PMF was approximately 10 dB and frequency-dependent. Untreated anterior mallear ligament fixation produced a persistent air-bone gap of approximately 10 dB after stapedioplasty. KEY WORDS — anterior mallear ligament, conductive hearing loss, laser Doppler interferometry, mallear fixation, malleus, middle ear mechanics, otosclerosis, stapes surgery. INTRODUCTION nosis of AML fixation? and What loss in sound conduction results from isolated fixation of the AML? Since AML fixation occurs in combination with otosclerosis, these questions cannot be answered directly by a clinical study. Therefore, a 3-pronged study of clinical data, human TB experiments, and analyses of a mathematical middle ear model was conducted to ensure maximum reliability of the conclusions. Complete bony fixation of the malleus is a welldocumented disorder that can occur alone or in conjunction with otosclerosis,1-4 and it leads to a conductive hearing loss of 15 to 30 dB.5-7 The fixation is easily detected during operation by palpation with a hook. Partial fixation of the malleus, on the other hand, has been reported only recently in the literature. In a study on revision surgery for otosclerosis, 37.5% of patients exhibited partial fixation of the malleus caused by calcification of the anterior mallear ligament (AML) and anterior mallear process (AMP), which made malleostapedotomy necessary.1 Histopathologic investigation of our temporal bone (TB) collection has confirmed the presence of severe hyalinization of the AML in 30% of 43 otosclerotic specimens.8 Although attenuation of sound conduction through the middle ear is expected with partial mallear fixation, no quantitative figures have appeared in the literature. MATERIALS AND METHODS A laser Doppler interferometry (LDI) system was used to measure the vibration of the middle ear. Preoperative mallear vibration patterns were measured in the clinical study in patients with otosclerosis, and were compared with the intraoperative diagnoses of AML fixation. In the TB experiments, vibration patterns of the malleus and stapes were measured in the normal situation and after the AML was experimentally fixed. All experimental data were then compared to the response of a mathematical middle ear model. Clinical Trial. Nineteen patients with an intraoperatively confirmed diagnosis of otosclerosis and no The study reported here was designed to answer 2 questions: Are there effective methods for the diag- From the Department of Otorhinolaryngology–Head and Neck Surgery, University Hospital of Zurich (Huber, Nandapalan), and the Otorhinolaryngology Center, Hirslanden Clinic (Fisch), Zurich, Switzerland, and the Department of Mechanical Engineering, Tohoku University, Sendai, Japan (Koike, Wada). Presented in part at the meeting of the Association for Research in Otolaryngology, St Petersburg Beach, Florida, February 4-8, 2001. CORRESPONDENCE — Alexander Huber, MD, Dept of Otorhinolaryngology–Head and Neck Surgery, University Hospital of Zurich, Frauenklinikstrasse 24, 8091 Zurich, Switzerland. 348 349 Huber et al, Anterior Mallear Ligament Fig 1. Intraoperative exposure of incudomalleal joint, anterior mallear ligament (AML), and anterior mallear process (AMP) by endaural approach with superior canaloplasty. MA — malleus, IN — incus, LMP — lateral mallear process, CT — chorda tympani, TMF — tympanomeatal flap. history of previous surgery on the ear of interest were included in the study. All patients were evaluated before operation by audiometry, tympanometry, and LDI. The average age of the patients was 41 years (range, 19 to 67 years), and 13 of them were female. Preoperative audiometry revealed a conductive hearing loss in all cases. The following tympanograms were presented: normal (type A) in 6 patients, deep type (type Ad) in 3 patients, and shallow type (type As) in 10 patients. The stapedius reflex was absent in all cases. For further analysis, the patients were divided into “otosclerosis” and “otosclerosis and AML fixation” groups, corresponding to the intraoperative findings. Informed consent to participate in the study was obtained from all patients. An endaural approach with superior canaloplasty was performed in all patients to enable an overview of the anatomic structures that may limit the mobility of the ossicles. Figure 1 shows the view of the AML, AMP, and incudomalleal joint that is achieved by this technique. The mobility of the malleus was assessed by gentle palpation of the malleus handle with a 1.5-mm, 45° hook in the horizontal and vertical planes. This maneuver allowed a distinction to be made between normal mobility and total or partial fixation of the malleus. If there was any doubt about this, the maneuver was repeated after disruption of the incudostapedial joint. Ears with total fixation of the malleus were excluded from the study. Intraoperative assessment of the malleus was considered the gold standard. All patients with normal mobility of the AML underwent conventional stapedotomy. If a partial mallear fixa- 349 tion was found during operation, a malleostapedotomy was performed. A more detailed description of the operative technique is available elsewhere.1 Temporal Bone Preparation. Six fresh human TBs were used for the study. The material was harvested within 24 hours after death, stored in a 0.1% Cialit (sodium-2-ethylmercurimercapto-benzoxazol-5-carbonide) solution (ASID Veterinär Vertriebs GmbH, Unterschleissheim, Germany) at 5°C, and used for measurements within 5 days. Inspection of the tympanic membrane and middle ear with an operating microscope revealed that 1 TB exhibited tympanosclerosis, so only the remaining 5 TBs were included in the study. The anterior wall of the external auditory canal was drilled down to a 1-mm rim, and a transparent sound chamber (plastic tube, closed by a cover glass) with a volume of 2 cm3 was placed over the tympanic membrane. Mastoidectomy, posterior tympanotomy, and partial removal of the facial nerve were performed to allow maximum visualization of the stapes footplate. The AMP and AML were approached through the tegmen tympani, with great care being taken not to injure the superior mallear ligament. All measurements were conducted with an intact tympanic membrane, ossicular chain, ligaments, muscles, and inner ear, and the middle ear cavity was not sealed from ambient air. Baseline LDI measurements of the motion of the manubrium and the stapes footplate were conducted before changing the properties of the AML and AMP. The mobility of the AML was reduced by using a needle to apply 1 drop of Histoacryl (B. Braun Medica AG, Emmenbrücke, Switzerland) to the AML through the tegmen tympani. This adhesive hardens within a few seconds in the presence of wet tissues and is therefore able to induce a partial mallear fixation. The LDI measurements of the motion of the manubrium and the stapes were then repeated. The difference between the stapes vibration amplitudes measured with and without isolated AML fixation was calculated as an equivalent sound conduction loss. Laser Doppler Vibrometry Interferometry Measurement Setup. A measurement system based on a scanning helium-neon laser Doppler interferometer (PSV200; Polytec GmbH, Waldbronn, Germany) was used for the measurements. The sensor head and the scanning unit were suspended from a balanced operating microscope stand (Contraves, Zurich, Switzerland). A built-in camera and a computer-driven mirror system controlled the position of the laser spot (diameter, 10 µm) on the object with a spatial resolution of 5 µm. A multisinusoidal signal tone containing 31 frequencies between 500 and 8,000 Hz was applied to a sound chamber positioned over the tympanic membranes of the patients and the TB prep- 350 Huber et al, Anterior Mallear Ligament 100 picometers over all frequencies. All amplitudes are given in terms of the peak displacement, and no angle correction was performed. A more detailed description of the system has been published elsewhere.9 In the human subjects, a silicone tube probe microphone and a loudspeaker were placed in the ear canal through a custom-made ear speculum, so that the tip of the tube microphone was a distance of less than 3 mm from the center of the eardrum. The ear speculum was held in place by means of earmold material (Otoform-A/Flex; Dreve Otoplastik GmbH, Unna, Germany), and the head of the subject was held steady by a vacuum pillow. Scanning LDI was typically recorded from 100 points on the tympanic membrane; however, only the movement patterns of the umbo and the short process of the malleus were analyzed for this study. In the TB preparations, the acoustic stimulation was applied to a transparent sound chamber and controlled by a tube probe microphone placed 1 to 2 mm from the tympanic membrane. The manubrium vibrations were recorded in a way similar to that used for the human subject measurements and were followed by assessment of the stapes footplate vibration amplitude. Stapes vibrations were recorded through the enlarged facial recess, which yielded visualization of the stapes footplate at an angle of 30° to its major displacement axis. Finite Element Model. Finite element modeling (FEM) is a mathematical method that allows the dynamic behavior of mechanical systems to be modeled with a high degree of spatial resolution. This method has been applied widely in studies of the mid- Fig 2. Finite element model of middle ear. Properties of AML (a) and annular ligament (b) were modified in this study. arations. The sound produced by a loudspeaker (ER2; Etymotic Research, Elk Grove, Illinois) was monitored by a probe microphone (ER-7; Etymotic Research). The sound pressure level was calibrated to be 80 dB SPL for each tone in the stimulation signal, resulting in a total sound pressure of the stimulus of 94 dB. For the analysis, only results with a coherence of 90% or better were used, which corresponds to signal-to-noise ratios of 10 to 25 dB. The threshold sensitivity of the LDI used is 300 nm/s, which equals displacement amplitudes of less than A 350 B Fig 3. Mean and standard deviation of preoperative pure tone audiograms of 14 patients with otosclerosis and 5 patients with otosclerosis and partial mallear fixation. A) Air conduction thresholds. B) Bone conduction thresholds. 351 Huber et al, Anterior Mallear Ligament A 351 B Fig 4. Average displacement amplitudes of malleus in response to acoustic stimulation at 80 dB sound pressure level (SPL) in 14 patients with otosclerosis, and in 5 patients with otosclerosis and fixation of AML and normal displacement range. A) Umbo. B) Short process (SP) of malleus. dle ear.10-14 It is particularly effective in assessing disorders that are difficult to evaluate in experimental or clinical studies. The model used in this study has been extensively tested, and a full description of it is available elsewhere.10 Figure 2 shows the components of the model. To simulate partial mallear fixation with a calcified AML, the Young’s modulus of the normal AML (EAML normal = 2.1 × 107 N/m2) was increased by a factor of 1,000. Thereby, mechanical properties similar to those of human bone are obtained (Young’s modulus of human humerus = 1.2 × 1010 N/m2).15 To simulate otosclerosis, we increased the Young’s modulus of the annular ligament of the stapes until an attenuation of sound conduction of approximately 30 dB, mainly at low frequencies, was achieved. An increase in Young’s modulus of 100 times was required. The results of all calculations performed are given in terms of the peak displacement amplitudes in response to an 80 dB SPL sound stimulus at the tympanic membrane. RESULTS Clinical Trial. The means of preoperative air con- A duction and bone conduction thresholds and the standard deviations are given in Fig 3. The patients are divided into “otosclerosis” and “otosclerosis and AML fixation” groups, corresponding to the intraoperative mallear mobility assessment (normal vibration versus partially fixed malleus, respectively). Solitary otosclerotic stapes fixation was found in 14 patients; in 5 patients, this occurred in combination with AML fixation. There is no statistically significant difference between these 2 groups according to the Mann-Whitney rank sum test. In the “otosclerosis and AML fixation” group, 3 patients presented with normal tympanograms (type A), and 2 patients with shallow tympanograms (type As). In the “otosclerosis” group, 3 patients presented with normal tympanograms (type A), 8 patients with shallow tympanograms (type As), and 3 patients with deep tympanograms (type Ad). Again, no statistically significant difference was found according to a χ2 test. The results of the LDI evaluation of the otosclerotic patients is given in Fig 4, which shows the average displacement amplitudes of the umbo and the short process of the malleus. The normal ranges of displacements for both the umbo and the short pro- B Fig 5. Individual displacement amplitudes of short process of malleus in response to 80 dB SPL acoustic stimulation at tympanic membrane. A) In 14 patients with otosclerosis. B) In 5 patients with otosclerosis and fixation of AML. 352 Huber et al, Anterior Mallear Ligament 352 Fig 6. Average displacement amplitudes of A) umbo, B) short process (SP) of malleus, and C) stapes in 5 temporal bone preparations in response to 80 dB SPL acoustic stimulation at tympanic membrane. Baseline results (Normal) and results after experimental AML fixation are given. A B C cess are also included.9 Figure 4A shows that there is only a small difference in the umbo vibration amplitudes between the 2 groups, with the maximum 1.7-fold difference (4.5 dB) occurring at 2,200 Hz. The differences are not statistically significant (p > .05) as assessed by the Mann-Whitney rank sum test. The displacements of the short process, however, were significantly different between the 2 groups (p < .05) at frequencies between 1,500 and 2,200 Hz, with a maximum 3.5-fold difference (10 dB) at 2,000 Hz. Figure 5 gives the individual displacement amplitudes of the short process of the malleus for all patients in the “otosclerosis” and “otosclerosis in combination with AML fixation” groups. All patients with AML fixation showed a significant notch in the range 1,300 to 3,000 Hz. In the patients with otosclerosis, on the other hand, the displacement of the short process increased up to a maximum at approximately 3,000 Hz, and decreased beyond this frequency. One patient, however, showed a notch between 2,000 and 3,000 Hz (Fig 5A). Temporal Bone Preparations. The average umbo displacements in normal TBs and in TBs in which the AML was fixed with Histoacryl glue are given in Fig 6A. Fixing the AML had a noticeable effect only at frequencies below 1,000 Hz, with a maximum 2fold difference (6 dB) at 700 Hz. The graph also shows the range of displacements in 129 normal ears of live human subjects.9 The average vibration displacement of the short process is given in Fig 6B. Similar displacement amplitudes are present in normal TBs and in TBs with a fixed AML, except for a notch at 1,600 Hz in which there is a 1.6-fold difference (4 dB). At frequencies up to 2,400 Hz, differences in the stapes displacement are in the range of 1.8-fold to 4-fold, corresponding to an attenuation of the middle ear transfer function of 5 to 12 dB (Fig 6C). Finite Element Model. The calculated displacement amplitudes for the umbo, the short process of the malleus, and the stapes for normal, otosclerotic, and AML and AMP fixation models are shown in Fig 7. Figure 7A includes the umbo displacements for the normal, otosclerotic, and partially fixed mallei in combination with otosclerosis. Virtually no differences are present between the normal and otosclerotic models. In the case of the partially fixed malleus, the displacement at low frequencies shows a frequency dependence that is similar to that in the normal model (approximately constant at 2.5-fold, or 8 dB). Local maxima are present in the range 1,000 to 2,000 Hz and increase with the stiffness of the middle ear. At frequencies higher than 3,000 Hz, no differences are evident. Figure 7B shows the corresponding results for the displacement of the short process. Again, only minor differences are present between the normal and otosclerotic models. However, for otosclerosis in com- 353 Huber et al, Anterior Mallear Ligament 353 Fig 7. Results of finite element model calculations for displacement amplitudes of A) umbo, B) short process of malleus, and C) stapes in response to 80 dB SPL acoustic stimulation. A B C bination with the partially fixed malleus, 5.5-fold differences (15 dB) between the normal and otosclerotic models are present at low frequencies. A maximum 10-fold difference (20 dB) is seen at 1,400 Hz, where a notch is present. At frequencies higher than 3,000 Hz, only small differences are evident (1.6fold, or 4 dB). The displacement amplitudes are in general lower than those found at the umbo. Figure 7C shows the calculated displacements of the stapes for a fixed sound pressure level at the tympanic membrane. The amplitudes of normal vibration are in good agreement with the results of the TB study. The differences in stapes vibration between normal and pathological situations correlate well with the model simulations in which similar air-bone gaps are present. Otosclerosis results in attenuation mostly at low frequencies (30-fold, or 30 dB). Additional partial fixation of the malleus increases this 3- to 4fold (9 to 12 dB) at frequencies below 1,000 Hz. For isolated AML fixation, most differences are found at frequencies below 1,000 Hz and around 1,800 Hz, ranging from 1.8-fold to 2.5-fold (5 to 8 dB). tion audiograms. The results on the motions of the umbo and the short process from patient measurements, the TB preparations, and the FEM calculations are in good agreement. No substantial differences are evident in the displacement of the umbo for the normal, otosclerotic, and partial mallear fixation cases (Figs 4A, 6A, and 7A). The short process, on the other hand, presents a considerable notch at 1,000 to 2,000 Hz in all 3 measurement methods (Figs 4B, 6B, and 7B). Such a notch in the vibration amplitude of the short process is therefore a reliable indicator of partial mallear fixation. Of the 19 patients in the clinical study, 14 presented with normal mallear mobility and 5 with partial mallear fixation. The notch described was found in all 5 patients with AML fixation and in 1 of the 14 patients with normal mallear mobility. The LDI analysis was therefore in agreement with the observations of the surgeon in 95% (18 of 19) of cases. Whether partial mallear fixation was wrongly suspected on the basis of LDI in this 1 remaining patient, or whether the mallear fixation was too weak to be identified by palpation, cannot be answered by this study. The patient, however, underwent stapedotomy and has a good functional result with an air-bone gap pure tone average of 10 dB (at 0.5, 1, and 2 kHz). Although the surgeon sometimes knew of the LDI results, this is not believed to introduce any bias into the results, since the clinical assessment was per- DISCUSSION By conventional preoperative audiological diagnostics, the difference between isolated stapes fixation and otosclerosis and AML fixation could not be distinguished, since there was no particular pattern of tympanograms or preoperative air or bone conduc- 354 Huber et al, Anterior Mallear Ligament Fig 8. Vibration patterns of ossicles in normal ear and in case of isolated AML fixation. formed before the TB and FEM investigations, and the specific LDI patterns for AML fixation were therefore not known at the time of the clinical study. Thus, there was no preoperative diagnosis by LDI at that time. Generally, the results of the 3 methods used in this study are in good agreement. However, technical differences between the methods lead to some of the variance seen in the data: 1) the small sample sizes of 5 and 19 for the TB and clinical studies, respectively; 2) the individual variance in vibration amplitudes; 3) the use of non–angle-corrected displacement data; 4) the use of cadaver TB preparations in which autolytic tissue changes cannot be excluded; 5) the use of different age groups; 6) the use of an open (TB and FEM) or closed (clinical study) middle ear cavity; and 7) the technical difficulty of applying the glue to the AML. (Although microscopic inspection revealed firm fixation in all cases, a fluid film was found underneath the glue in some preparations at the end of the experiment. Such a fluid film, even if it is very thin, may allow relative motions in the nanometer range, and so the results of the TB study may underestimate the transmission loss.) It is still unclear why hyalinization and calcification of the AML occur in certain patients with otosclerosis. The notch in vibration amplitude occurring at 1,000 to 2,000 Hz on the short process but not at the umbo, on the other hand, can be explained by the 3-dimensional movement patterns of the ossicles. From FEM calculations, it can be seen that in the normal ear, at frequencies in the range of 1,000 Hz, the mostly rotatory movement of the malleus changes to a complex movement pattern with a significant translation of the AMP, which moves in a lateral-medial direction. The short process has thereby a relatively large vibration amplitude. By contrast, in the case of AML fixation, the translational movement of the malleus is reduced. Since the mal- 354 Fig 9. Stapes displacement amplitude differences in temporal bone preparations and in finite element model calculation. leus rotates around the classic rotation axis that goes through the short process of the incus and the AMP, the lateral mallear process, which is close to the center of the rotation, has a smaller amplitude than in the normal ear, whereas the umbo motion is virtually unchanged (Fig 8). In cases of additional stapes fixation, these vibration patterns were not changed; only the amplitudes were decreased collectively. The influence of stapes fixation on manubrium motion is most dominant at low frequencies, but appears surprisingly small. However, the 2 ossicular joints involved may yield sufficiently to produce almost normal movements of the malleus. The findings of routine tympanometry are similar, indicating a tendency toward type As tympanograms, but they do not allow reliable identification of otosclerosis.9 Assessment of mallear mobility necessitates a high degree of surgical experience. A modified operative approach that allows an extended view over the incudomalleal joint and the AML and AMP, however, makes identification of partial mallear fixation less difficult. The FEM calculations in this study revealed that surgical evaluation by palpation on the malleus neck, represented by a pinpoint force of 0.1 N, leads to a displacement of the AMP tip of 0.04 mm and 0.003 mm for the normal AML and fixed AML, respectively. The displacement in the normal ear, though small, can still be identified by an operating microscope, but the displacement in case of a fixed AML cannot be detected. At the umbo, the displacement amplitudes are virtually equal. A view over the AML and AMP is hence required to reliably identify partial mallear fixation. The malleus and stapes have entirely different frequency response characteristics, because of the complex 3-dimensional nature of sound conduction by the middle ear. The similarity between the results from the experimental work and the model calculations proves that 3-dimensional FEM is an excellent meth- 355 Huber et al, Anterior Mallear Ligament od for simulating the effects of modifying individual components of the middle ear. In the study reported here, stapes vibration was considered to be the effective stimulus to the cochlea. Differences between the stapes displacements before and after AML fixation correspond, therefore, to the prospective air-bone gap in patients with isolated partial mallear fixation. Such an air-bone gap is expected after operation in patients with otosclerosis and AML fixation who undergo stapedioplasty with no correction of the partial mallear fixation. Figure 9 gives these displacement differences in decibels for the TB preparations and the FEM calculations. The FEM calculations predicted an attenuation of stapes mobility of −8 to −7 dB at frequencies up to 1,000 Hz, and −7 to 0 dB at higher frequencies. From the TB experiments, valid data are available from 500 to 4,000 Hz. The results are 2 to 4 dB lower than those from the FEM calculations, but with a similar frequency dependence. These values, however, may deviate by a few decibels from reality, as AML fixations clinically occur in combination with otosclerosis, and patients therefore have a prosthesis replacing the stapes rather than a normal middle ear after surgery. We found AML fixation in 26% of the ears with otosclerosis in this study. This rate confirms the importance of a thorough intraoperative evaluation of mallear mobility. This figure is in accordance with a histopathologic study8 and a clinical study on revision stapes surgery.1 A complete bony fixation of the malleus causes a 355 15 to 30 dB conductive hearing loss,5-7 but a partial mallear fixation results in a milder hearing loss. The air-bone gap due to a partial mallear fixation is approximately 10 dB and is low-frequency–dominant. We have started a clinical survey to examine whether a malleostapedotomy yields better functional results than does incus stapedotomy in primary otosclerosis combined with AML fixation. CONCLUSIONS 1. Partial fixation of the malleus can be identified either before operation with LDI or during operation by palpation with observation of the AML and AMP. 2. Untreated AML and AMP fixation after stapedioplasty produces a persistent air-bone gap of approximately 10 dB at low and middle frequencies. The confirmation of its relevance in this study is one step forward in the process of analyzing the causes of unfavorable results of stapedioplasty. 3. Laser Doppler interferometry is uncommon in clinical practice, because it is expensive and timeconsuming. The technique may, however, become of greater practical importance in the future as its validity in preoperative, intraoperative, and postoperative diagnostics becomes better documented. 4. The study reported here was an example of combining experimental research with an existing mathematical middle ear model to address a question with clinical implications. REFERENCES 1. Fisch U, Acar GO, Huber AM. Malleostapedotomy in revision surgery for otosclerosis. Otol Neurotol 2001;22:77685. 2. Tos M. Bony fixation of the malleus and incus. Acta Otolaryngol (Stockh) 1970;70:95-104. 3. Subotic R, Mladina R, Risavi R. Congenital bony fixation of the malleus. Acta Otolaryngol (Stockh) 1998;118:8336. 4. Causse J, Causse JB. Eighteen-year report on stapedectomy. I. Problems of stapedial fixation. Clin Otolaryngol 1980;5: 49-59. 5. Plester D. Atlas der Ohrchirurgie. Stuttgart, Germany: Kohlhammer, 1989. 6. Powers WH, Sheehy JL, House HP. The fixed malleus head. A report of 35 cases. Arch Otolaryngol 1967;85:177-81. 7. Moon CN Jr, Hahn MJ. Primary malleus fixation: diagnosis and treatment. Laryngoscope 1981;91:1298-307. 8. Nandapalan V, Pollak A, Langner A, Fisch U. The anterior and superior malleal ligaments in otosclerosis: a histopath- ologic observation. Otol Neurotol 2002;23:854-61. 9. Huber AM, Schwab C, Linder T, et al. Evaluation of eardrum laser Doppler interferometry as a diagnostic tool. Laryngoscope 2001;111:501-7. 10. Wada H, Metoki T, Kobayashi T. Analysis of dynamic behavior of human middle ear using a finite-element method. J Acoust Soc Am 1992;92:3157-68. 11. Eiber A. Mechanical modeling and dynamical behavior of the human middle ear. Audiol Neurootol 1999;4:170-7. 12. Ladak HM, Funnell WR. Finite-element modeling of the normal and surgically repaired cat middle ear. J Acoust Soc Am 1996;100:933-44. 13. Williams KR, Lesser THJ. A finite element analysis of the natural frequencies of vibration of the human tympanic membrane. Part I. Br J Audiol 1990;24:319-27. 14. Beer HJ, Bornitz M, Hardtke HJ, et al. Modelling of components of the human middle ear and simulation of their dynamic behaviour. Audiol Neurootol 1999;4:156-62. 15. Evans FG. Mechanical properties of bone. Springfield, Ill: Charles C Thomas, 1973:35-6.