H2 - American Academy of Pediatrics
advertisement

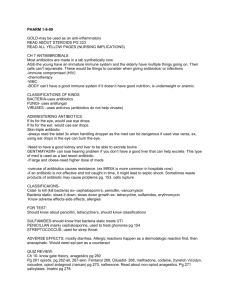
Antibiotic Update: What’s Old? Sunday July 25, 10:15 – 11:25 AM Mark R. Schleiss, MD American Legion Chair of Pediatrics Director, Division of Pediatric Infectious Diseases University of Minnesota, Amplatz Children’s Hospital • Neither I nor any member of my immediate family Disclosure has a financial relationship or interest with any proprietary entity producing health care goods or services related to the content of this CME activity. • I do not intend to discuss an unapproved or investigative use of commercial products or devices. Objectives • Review general classes of antimicrobials used in pediatric practice • Be familiar with the problem of antibiotic resistance including its epidemiology and mechanisms • Understand general classes of new antibiotics including their spectrum and limitations • Re-familiarize with older antibiotics that have fallen out of favor in recent years but may have an important role in the era of antimicrobial resistance 1970s 1980s 2000s 2010s Ureidopenicillins Cephalosporins Betalactamase Inhibitors Carbapenems Fluoroquinolones Streptogramins and Oxazolidinones http://www.kent.ac.uk/secl/philosophy/jw/2009/macits/ http://biogetopics.files.wordpress.com/2008/11/horizontaltransfer.gif http://www.microbiology.mtsinai.on.ca • Rates are on the rise (6.7/1000 in 2002 to 21.1/1000 in 2007) • Median age 3 years • Over 60% present as skin or soft tissue infection Factors Contributing to Antimicrobial Resistance • Resistance to antibiotics is a biological property of microorganisms that can be accelerated by human practice • Overuse of antibiotics in primary care for viral infections • Noncompliance • Over-reliance on new medications • Self-medication and ease of access to OTC antibiotics • Hospitals • Agricultural practices Solution: Judicious Stewardship • No antibiotics for URIs • Use most narrow spectrum agent • “Watchful waiting” for otitis media • Reconsideration of day care policies http://www.lowdensitylifestyle.com/media/uploads/2010/03/antibiotic.jpg Solution: Remove Antibiotics from Agribusiness • 70% of antibiotics used in USA are for animals • AMA, WHO, APHA have called for removal • EU has removed most antibiotics from feed http://www.foodrenegade.com • FDA statement 6/29/10 called this an “urgent public health issue” Industry Reaction • National Pork Producers Council: “there is no science that says antibiotic use in livestock leads to antibiotic resistance in humans” http://www.pewtrusts.org • National Cattlemen's Beef Association: “the causes of antibiotic resistance are complex and should take into consideration human misuse of antibiotics” Solution: Develop New Agents Clinical Infectious Diseases 2010;50:1081-83 Solution: Develop New Vaccines http://www.health.state.mn.us/divs/idepc/newsletters/dcn/sum07/spneumo.html http://www.cdc.gov Pneumococcal Vaccination Update • PCV13 is replacing PCV7 • A, 6B, 7F, 9V, 14, 18C, 19A, 19F, and 23F • A single supplemental dose of PCV13 is recommended for all children 14 through 59 months of age who have received 4 doses of PCV7 or other age appropriate, complete PCV7 schedule Polymyxin B • Cyclic peptide • Disrupts cell membrane via interaction with phospholipids • Highly resistant Pseudomonas infections • 15,000-25,000 U/kg/day (IM or IV) • Intrathecal administration for resistant meningitis • Neurotoxicity and nephrotoxicity Colistin • A member of polymyxin family • Multidrug resistant gram negatives • Two formulations: • Colistin sulfate (1-2 million units TID is an average dose) • Colistimethate sodium (2.5-5 mg/kg/day) • Nephrotoxicity and neurotoxicity • Inhalational form available Macrolides • First isolated from Saccharopolyspora erythraea • Erythromycin, clarithromycin, azithromycin • Active at ribosomal 70S rRNA complex • Emergence of resistance has limited recent use in practice particularly for S. aureus, GAHS, pneumococcus, H. flu • Are there scenarios in pediatric practice where macrolides are still useful? Macrolides • Nongonococcal urethritis/cervicitis • Azithromycin 1 g PO • Erythromycin base 500 mg QID for 7 days • Erythromycin ethylsuccinate 800 mg QID for 7 days • Mycoplasma pneumoniae infection • Legionella infection • Bordetella pertussis (Whooping Cough) • Caution in neonates re: pyloric stenosis Lincosamides • Isolated from Streptomyces 1962 • Clindamycin is the prototype • Protein synthesis inhibitor: binds to the 23s portion of the 50S ribosomal subunit • Activity against anaerobes; most MRSA (without inducible clindamycin resistance); parasites (toxplasmosis, malaria); no gram negative coverage; little CNS penetration • Reduction of toxin production uniquely valuable for toxic shock syndrome, invasive GAHS infections http://www.health.state.mn.us Clindamycin • • • • A treatment of choice (with quinine) for babesiosis Clindamycin/primaquine effective for Pneumocystis jirovecii Effective for toxoplasmosis Capsules (clindamycin hydrochloride) preferred over oral suspension (clindamycin palmitate) • The parenteral dose for clindamycin in children is 20 to 40 mg/kg/day divided every 8 hours • The recommended oral dose of clindamycin in children with serious infections is 8-20 mg/kg/day divided every 6-8 hours to a maximum dose of 450 mg QID • Clostridia difficile is intrinsically resistant to clindamycin Tetracyclines • First discovered in 1948 in soil sample • Streptomyces aureofaciens • Original tetracycline: aureomycin (still added to cattle feed) • Works by binding the 30S ribosomal subunit and through interaction with 16S rRNA prevents docking of aminoacylated tRNA • Multiple formulations: rolitetracycline, minocycline and doxycycline, and tigecycline Take Two Beers and Call Me in 1600 Years... • Evidence from mummified remains of Nubian people that tetracycline had been consumed • Tetracycline extracted from bone was shown to be capable of killing bacteria • Believed that brewed beer was likely source • First evidence of toxicity to bones and teeth of children http://www.findarticles.com/p/articles/mi_m1134/is_4_109/ai_62324477 Tetracyclines • First line therapy for: • • • • Rocky Mountain Spotted Fever Q Fever Psittacosis Anaplasma phagocytophilums • Also useful for: • Chlamydia • MRSA • Mycoplasma pneumoniae infection http://www.bada-uk.org/images/buffycoatsmear.jpg http://www.cdc.gov Tetracycline: Toxicities and Cautions • Complications: Eosinophilia, leukopenia and thrombocytopenia (tetracycline) Pseudotumor cerebri Emesis and nausea, Hepatitis Photosensitivity Hypersensitivity reaction (urticaria, asthma exacerbation, facial edema, dermatitis) • Systemic lupus erythematosus–like syndrome (minocycline) • • • • • • • Avoid dairy products, antacids Tetracycline: Cautions • Children under 8 should not receive tetracyclines • Can cause permanent discoloration of teeth • Children as young as 4 years of age can receive up to 4 courses of doxycycline with no evidence of enamel discoloration (Volovitz, Clin Ped, 46:121, 2007) http://www.toothmingle.com/healthy-smile/precaution-antibiotics-can-stain/ http://www.cdc.gov http://www.ok.gov Gerhard Domagk • German physician and chemist • On sabbatical from University of Munster at I.G. Farbenindustrie discovered prontosil • Dramatic protection in animal models but no activity in cell culture • Became the world’s first commercial antibiotic http://nobelprize.org/nobel_prizes/medicine/laureates/1939/domagk-bio.html • Nobel Laureate 1939 Sulfonamides • Protonsil metabolized to Sulfanilamide in vivo • Discovery paved way for many sulfa drugs developed in 1940s-50s • Co-trimoxazole (TMP-SFX) developed in 1960s • Synergy derives from the fact that successive steps in folic acid pathway are inhibited TMP-SFX • Folic acid dietary requirement • Basis of selectivity for bacterial agent TMP-SFX • Combination of mechanisms discourages resistance • Very broad spectrum agent • • • • • • MSSA MRSA H. flu E. coli Listeria monocytogenes Pneumocystis jirovecii • Notably ineffective against GAHS TMP-SFX: Side Effects • GI side effects • Hypersensitivity reactions (rash, urticaria) • Hepatocellular injury • Agranulocytosis • Crystalluria/azotemia • Stevens-Johnson Syndrome (1:1,000,000 prescriptions) • Will all of these increase in the MRSA era? FIGURE 2 Typical pattern of SJS: blisters develop on widespread atypical targets Levi, N. et al. Pediatrics 2009;123:e297-e304 Copyright ©2009 American Academy of Pediatrics Summary • Resistance to antibiotics continues at crisis levels in medicine in 2010 • There are strategies that can help! • New antimicrobials are on the horizon • Older drugs – particularly the polymyxins, sulfonamides, macrolides, lincosamides and tetracyclines – still play an important role in the management of sick children Research Opportunities • Impact of PCV13 on DRSP and evolving patterns of disease • Formulary committee: restriction of quinolones, carbapenems and impact on GNR resistance • CAP in children: RCT of macrolide or tetracycline versus cephalosporin agents and impact on outcomes? • Descriptive studies of tetracycline use and vector-borne disease: regional variation, ICD-9 coding • Cost-benefit analysis of TMP-SFX on management of MRSA infections: are we over-treating or putting our children at risk?