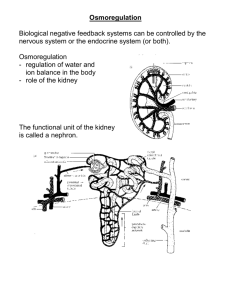
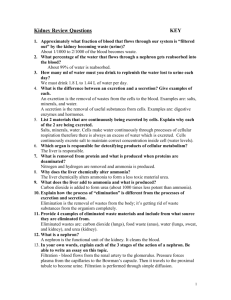
Regulation of Body Fluid Osmolality
advertisement

❖ CASE 24 A 27-year-old woman is being monitored in the intensive care unit after she sustained head trauma in a motor vehicle accident 3 days ago. She has undergone computed tomographic imaging of her head, which revealed cerebral swelling but no evidence of hemorrhage or brain herniation. The patient has been in critical but stable condition. The nurse calls the physician because the patient has developed hypernatremia and has had a significant increase in dilute urine output. The findings are confirmed, and it is determined that the patient has central diabetes insipidus as a result of the head trauma. ◆ ◆ ◆ How are antidiuretic hormone (ADH) levels affected in patients with this condition? What is the effect of high ADH on the late distal tubule and collecting ducts? How does free-water clearance change in the presence of ADH? 196 CASE FILES: PHYSIOLOGY ANSWERS TO CASE 24: REGULATION OF BODY FLUID OSMOLALITY Summary: A 27-year-old woman who suffered head trauma has evidence of central diabetes insipidus. ◆ ◆ Change in ADH: Serum ADH decreased from normal values. Effect of high ADH on distal tubule and collecting duct: Increased permeability of the principal cells to water. ◆ Free-water clearance with presence of ADH: Negative free-water clearance (inability to excrete free water). CLINICAL CORRELATION Diabetes insipidus is a condition that results in the production of diluted urine. This can be a result of decreased ADH secretion or can occur because the kidney is no longer responsive to the hormone. When the production of ADH from the posterior pituitary is decreased, the condition is called central diabetes insipidus. Many conditions can cause central diabetes insipidus, including central nervous system (CNS) trauma or hypoxia (cerebrovascular accident [CVA]), granulomatous disease, tumor and treatment of pituitary tumors, drugs (lithium), and infections. When the ADH is normal but there is still production of dilute urine, the kidney may be resistant to ADH, a condition called nephrogenic diabetes insipidus. Signs and symptoms include polyuria and polydipsia along with the production of dilute urine (< 300 mOsmol/kg). The use of intranasal DDAVP (desmopressin), an analogue of vasopressin, helps concentrate the urine and reduces the polydipsia and polyuria. APPROACH TO BODY FLUID OSMOLALITY Objectives 1. 2. 3. Know about the regulation and secretion of ADH. Describe the cellular action of ADH. Know how to calculate free-water clearance. Definitions ADH (arginine vasopressin): A peptide hormone, secreted from the posterior pituitary, that regulates the water permeability of the kidney collecting ducts; the hormone also has vasoconstrictive properties. Aquaporins: A family of water-permeable channels. CLINICAL CASES 197 Diabetes insipidus: A condition in which secretion of ADH from the posterior pituitary is reduced or lacking, called central or hypothalamic diabetes insipidus, or in which the water permeability of the renal collecting ducts is not responsive to ADH, a much rarer condition called nephrogenic diabetes insipidus. Both conditions lead to the excretion of copious diluted urine. Free-water clearance: The volume of water (urine) cleared from the plasma per unit time in excess (positive free-water clearance) or deficit (negative free-water clearance) from the volume estimated if the urine were isosmotic (with plasma) for the given amount of solute excreted in the same time. A quantitative measure of how dilute (hypotonic) or concentrated (hypertonic) the urine is (milliliters of water/time) relative to the isosmotic state. DISCUSSION Regulation of water balance is achieved largely through regulation of the plasma/extracellular fluid osmolality. This is accomplished by controlling the water permeability of the collecting ducts through the actions of ADH, which regulates the rate of water reabsorption and hence the free-water clearance. The binding of ADH to receptors on the basolateral membrane of principal cells increases the water permeability (see below) of the luminal cell membrane, allowing water to be reabsorbed passively from the tubular lumen into the hypertonic interstitium. Daily urine output is highly variable, related to water and food intake, with typical urine volumes of 1 or 2 L (osmolalities of 200-500 mOsmol/kg or so). The water permeability of the cortical and medullary collecting ducts is relatively low in the basal state, primarily because of the low water permeability of the luminal (apical) cell membrane of the principal cells. In the presence of ADH, ADH binds to V2 receptors, which mediate the antidiuretic response (reduced urine output). (ADH binding to V1 receptors plays a major role in vasoconstriction of the vasculature). Binding to V2 receptors in the collecting duct principal cells leads to activation of adenylyl cyclase and the production of cyclic adenosine monophosphate (cAMP). The subsequent activation of protein kinase A by cAMP leads to phosphorylation of water channels, namely, aquaporin 2, contained in cytoplasmic vesicles. After phosphorylation, the vesicles move to and fuse with the luminal cell membrane, increasing the water permeability of the luminal membrane. In the cortical collecting duct, water then can be reabsorbed passively from the hypotonic luminal fluid (typically near 100 mOsmol/kg as fluid enters the cortical collecting duct) across the luminal border into the cell. The basolateral membrane normally has significant water permeability as a result of constitutive expression of other aquaporins (typically aquaporins 3 and 4). Hence, as water moves across the luminal border by osmosis, modestly reducing the osmolality of the cytoplasm, the water will diffuse from the 198 CASE FILES: PHYSIOLOGY cell across the basolateral membrane into the isosmotic interstitium by osmosis and be returned to the circulation. The osmotic reabsorption of water in the cortical segment of the collecting duct serves to present a smaller volume, but near isosmotic fluid, to the medullary collecting ducts so that water reabsorption in the medullary segment continues without a major reduction in the hypertonicity of the medullary interstitium. In the medullary segment, the insertion of water channels in the luminal membrane in the presence of ADH continues to allow for passive reabsorption of water from the tubular lumen into the hypertonic medullary interstitium that was set up by the countercurrent multiplier function of the loop of Henle (see Case 23). Water reabsorption continues, increasing the tubular fluid osmolarity, with the fluid approaching osmotic equilibrium with the medullary interstitium, thereby rendering a small but concentrated urine. In the presence of high levels of ADH, the urine osmolality will approach the interstitial osmolality at the tip of the papilla, approximately 1200 to 1400 mOsmol/kg, with a minimal urine volume near 0.5 L/day. A defect in the water channels or in the trafficking of the channel to the luminal membrane will diminish the antidiuretic response, a condition referred to as nephrogenic diabetes insipidus. In the absence of ADH (or with low levels), few water channels are inserted into the luminal cell membrane, and so the water permeability of the collecting ducts is very low, leading to little water reabsorption along the collecting ducts. Hence, the tubular fluid entering the cortical collecting duct (approximately 100 mOsmol/kg) remains hypotonic, leading to excretion of copious but dilute urine (a diuresis). Since NaCl is reabsorbed along the collecting ducts, in extreme cases of ADH depletion, the osmolality of the tubular fluid can decrease modestly along the collecting ducts, rendering the urine osmolality as low as 50 to 60 mOsmol/kg, but in a large volume of urine (typically several liters, with a maximum of 15 to 20 L/day). Hyperosmolality is a major stimulus for ADH secretion, with volume depletion providing a secondary stimulus. ADH is synthesized in the supraoptic and paraventricular nuclei of the hypothalamus, where it is packaged into secretory granules. The granules migrate down the axons of the supraopticohypophysial tract into the posterior pituitary and are stored in the nerve terminals, from where they are released into the plasma. ADH is metabolized in the liver and kidney. Osmoreceptors in the hypothalamus sense the plasma osmolarity (primarily the sodium concentration). It is thought that the shrinkage of these cells with hypertonicity leads to depolarization of these cells, which in turn increases the electrical activity of the supraoptic and/or paraventricular cells, thereby inducing fusion of the secretory granules and release of ADH into the plasma. Similarly, hypovolemia is sensed by both volume receptors in the left atria and pressure receptors, primarily the carotid sinus baroreceptors, which control the activity of the vasomotor center in the medulla and thus the rate of ADH secretion from the paraventricular nuclei. With elevated ADH levels, water reabsorption in the collecting ducts will be increased, leading to accumulation of volume and a reduction in extracellular fluid and plasma osmolality. 199 CLINICAL CASES Conversely, in the presence of a hypotonic plasma, or volume expansion, the reduced stimulation of the osmoreceptors or volume/baroreceptors, respectively, will result in a reduced release of ADH from the posterior pituitary. Less water will be reabsorbed from the collecting ducts, with an associated loss of extracellular fluid and plasma volume and a decrease in extracellular fluid and plasma volume back toward normal values. A defect in the synthesis or release of ADH also leads to a reduction in the reabsorption of water from the collecting ducts, leading to a diuresis with a hypotonic urine, a condition referred to as hypothalamic or central diabetes insipidus. As long as an individual has access to water, this is not a life-threatening condition. Further, an analogue of vasopressin (DDAVP) is available in nasal spray form that can be administered to regulate water excretion. The ability to excrete or retain water is reflected in the osmolality of the final urine. It is the solute-free water retained or excreted that alters the osmolality of the extracellular fluids and can be calculated as the free-water clearance, CH2O. The urine volume can be viewed as having two components: one containing all the excreted solutes in an isotonic solution, normally denoted as COsm, and one containing only “solute-free” water, that is, pure water, normally denoted CH2O. For a hypotonic urine, CH2O is the solute-free water that must be added to the theoretical isotonic urine volume, COsm, to provide for the actual urine volume per unit of time, V, and its hypotonicity. For a hypertonic urine, CH2O is the solute-free water that must be subtracted from the theoretical isotonic urine volume to provide for the actual urine volume per unit of time, V, and its hypertonicity. That is, CH2O is the additional water reabsorbed that will alter the osmolality of the extracellular fluids. COsm can be calculated as COsm = U Osm × V POsm where UOsm is the actual urine osmolality and V is the actual urine volume per unit time (eg, milliliters per minute or liters per day). COsm is equal to the clearance of osmotic solutes that appear in the urine per unit time. Urine volume per unit time thus can be thought of as having two components: V = CH2O + COsm Hence, CH2O = V − COsm For an isotonic urine, V and COsm are identical, meaning that CH2O is zero so that there is no alteration of extracellular fluid osmolality. For hypotonic urine, V is greater than COsm, and so CH2O is positive, meaning that an excess of water is being excreted, thereby increasing extracellular fluid osmolality. For hypertonic urine, V is less than COsm, and so CH2O is negative, meaning that an excess of water is being retained in the body, thereby decreasing extracellular 200 CASE FILES: PHYSIOLOGY fluid osmolality. CH2O provides a method to assess quantitatively the extent to which the kidney is either excreting or retaining free water and hence provides a measure of the degree of regulation of the osmolality of the extracellular fluid. COMPREHENSION QUESTIONS [24.1] A new patient is complaining about having to micturate numerous times during the day and being forced to get up multiple times throughout the night. Her diet has not changed, but she complains of being fatigued throughout the day (and frustrated with her shortened sleep periods). When she moves from a supine to an erect position, her blood pressure is observed to decrease modestly and her heart rate increases slightly. Blood chemistries reveal that she is modestly hypernatremic, and plasma arginine vasopressin and renin levels are markedly elevated. Urinalysis revealed copious diluted urine. The patient most likely has which of the following conditions? A. B. C. D. E. [24.2] If an individual becomes hypovolemic, such as during periods of diarrhea or excessive sweating, plasma ADH, or arginine vasopressin, levels are elevated rapidly and urine volume is decreased (antidiuresis). This effect of ADH on water excretion predominantly occurs in the collecting ducts by ADH-induced activation/inhibition of which of the following steps/processes? A. B. C. D. E. [24.3] Central diabetes insipidus Nephrogenic diabetes insipidus Psychogenic polydipsia Excessive consumption of alcohol Brain trauma Inhibition of sodium reabsorption Activation of potassium secretion Increased leakiness of the collecting duct to water and solute Insertion of sodium channels in the luminal membrane Insertion of aquaporin channels in the luminal membrane A 34-year-old woman feels compelled to drink water “all the time.” She does not drink Gatorade or other solute drinks but takes pure water. Her serum sodium is low, as is her serum osmolality. The physician is unsure whether this patient has psychogenic water intoxication versus diabetes insipidus. Which of the following would reliably differentiate between these two disorders? A. B. C. D. Urinary electrolytes compared with serum electrolytes Urinary osmolality compared with serum osmolality Serum ADH levels Restriction from drinking water CLINICAL CASES 201 Answers [24.1] B. Nephrogenic diabetes insipidus (nephrogenic DI) is a relatively rare disease that arises from defective water channels (aquaporins) or pathways regulating the water channels in the collecting ducts. It is characterized by high levels of ADH in the plasma and excretion of copious diluted urine. This contrasts with central diabetes insipidus, the more common form of DI, which is characterized by low synthesis and secretion of vasopressin from the posterior pituitary, giving rise to low levels of vasopressin in the plasma, but with the effect on urinary excretion being the same. [24.2] E. A key step in regulating water reabsorption in the collecting ducts is controlling the insertion and removal of aquaporins (water channels) at the luminal cell membrane. In the presence of ADH, ADH binds to a V2 vasopressin receptor on the basolateral membrane of the cells, leading to production of cAMP and the protein kinase A-induced phosphorylation of intracellular aquaporin channels retained in cytoplasmic vesicle pools. The phosphorylation leads to the insertion of the vesicles, along with the aquaporins, into the luminal membrane, thereby increasing the water permeability of the luminal membrane. [24.3] D. Psychogenic water intoxication has the appearance of diabetes insipidus. Owing to the marked hypotonic fluid ingestion, the body attempts to excrete free water, and thus ADH secretion is inhibited. Both serum and urine sodium and osmolality are very low. However, in psychogenic water intoxication, when water is restricted, the body will produce ADH eventually, leading to normalization of the serum osmolality and concentration of urine. In diabetes insipidus, because of a problem with ADH production and secretion, even with water restriction the patient will produce very dilute urine and will not be able to concentrate the urine. 202 CASE FILES: PHYSIOLOGY PHYSIOLOGY PEARLS ❖ ❖ ❖ ❖ ❖ Antidiuretic hormone regulates water reabsorption by the cortical and medullary collecting ducts by regulating the insertion of water channels (aquaporins) in the luminal cell membrane. Secretion of ADH from the posterior pituitary is regulated predominantly by osmoreceptors in the hypothalamus that sense plasma osmolality and secondarily by volume receptors in the left atria and pressure receptors (eg, carotid sinus baroreceptors). Diabetes insipidus is characterized by a reduction or a complete loss of secretion of ADH from the posterior pituitary (central or hypothalamic DI) or a decreased responsiveness of the collecting ducts to ADH (nephrogenic DI). Both conditions lead to excretion of copious diluted urine. Sodium chloride reabsorption from the thick ascending limb is critical for establishing a hypertonic medullary interstitium, which in turn provides the osmotic gradient for passive reabsorption of water from the medullary collecting ducts. Free-water clearance is a quantitative measure of the volume of “solute-free” water (per unit time) that is excreted (a hypotonic urine) or retained by the body (a hypertonic urine), leading to an increase or a decrease, respectively, in extracellular fluid osmolality. REFERENCES Giebisch G, Windhager E. Urine concentration and dilution, and transport of potassium. In: Boron WF, Boulpaep EL, eds. Medical Physiology: A Cellular and Molecular Approach. New York: Saunders; 2003:Chaps 37 and 36. Schafer JA. Regulation of body fluid osmolality. In: Johnson LR, ed. Essential Medical Physiology. 3rd ed. San Diego, CA: Elsevier Academic Press; 2003:Chap 28.