CFDFL Brief Mental Status Exam Template
advertisement

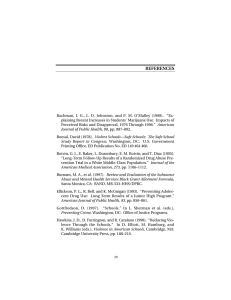
THE CENTER FOR DRUG-FREE LIVING, INC. Brief Behavioral Health Status Exam ( 1091 ) CLIENT NAME: NUMBER: Start Time: Purpose of Exam: Setting: Evaluate Clinical Necessity Residential Outpatient APPEARANCE: Looks Stated Age: Clean Yes EYE CONTACT: Appropriate ORIENTATION: MEMORY: End Time: X 4: Neat No Detox Unkempt Disheveled Younger Older Place Deficient: Person Immediate ATTENTION: Adequate Inadequate PERCEPTION: Adequate Inadequate MOTOR ACTIVITY: Normal COGNITIVE PERFORMANCE: Other: Other: Inappropriate Time Normal Limits Other: Evaluate Service Needs Slowed Restless Situation Recent Remote Agitated Normal Limits Poor memory Low self-awareness Short attention Developmental disability Poor concentration Impaired judgement Slow processing THOUGHT PROCESS: Normal limits Illogical Delusional Hallucinating (visual, auditory, tactile) Paranoid Ruminative Intact Derailed thinking Loose association Anti-psychotic medication DANGER TO OTHERS: Does not appear dangerous to others Violent temper Threatens others Physical abuser Hostile Assaultive Homicidal ideation Homicidal threats Homicide attempt DANGER TO SELF: Does not appear dangerous to self Suicidal ideation Current plan/means Recent attempt Past attempt Self-injury Self-mutilation SENSORY DEFICITS: None or Speech Hearing Vision THE CENTER FOR DRUG-FREE LIVING, INC. Brief Behavioral Health Status Exam ( 1091 ) Continued CLIENT NAME: SPEECH: MOOD: NUMBER: Clear Minimal Euthymic Labile AFFECT: Slurring Incoherent Slowed Other: Unremarkable Other: Full range Depressed Constricted range INSIGHT INTO PROBLEM: Loud Tearful Pressured Anxious Excessive Manic Flat Takes responsibility Slight awareness BEHAVIOR DURING INTERVIEW: Soft Cooperative Oppositional Other: Intellectual insight Blames others Guarded Hostile Emotional insight Complete denial Withdrawn Passive Acting Out ADDITIONAL OBSERVATIONS: CLIENT STRENGTHS: SERVICE NEEDS: PROVISIONAL IMPRESSION/DIAGNOSIS: PLAN OF TREATMENT: 303.90 Alcohol Dependence 311.00 Depressive Disorder NOS Individual Therapy Family Therapy Group Therapy Psychiatric Referral DISCHARGE CRITERIA: Clinician Signature: ____________________________________________ Date: _________ If Medicaid client: LPHA, M. CAP Signature: ________________________Date: _________ Revised 3/05 HRB