Upper and Lower Neural Tube Defects
advertisement

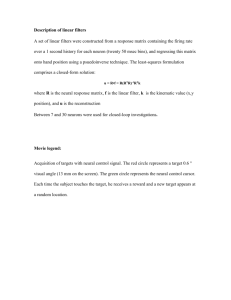
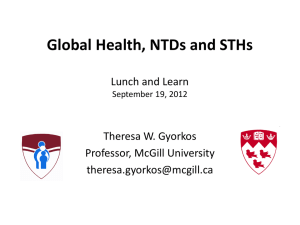
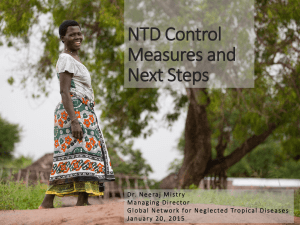
Upper and Lower Neural Tube Defects- Review 1 2 3 Leelavathy N , Sayee Rajangam , Kulkarni RN , 1 2 3 Department of Anatomy , Associate Professor , Professor , Professor & Head 1 2,3 Saptagiri Institute of Medical Science & Research Center , International Medical School, Bangalore ABSTRACT Normally neural tube closes around 18 to 28 days post fertilization. Abnormal closure of the neural folds results in neural tube defects. A defect occurring at the upper end of neural tube results in upper neural tube defects; exencephaly or anencephaly or encephalocele. A defect in the lower end of neural tube leads to lower neural tube defects; lumbosacral myelocele or meningomyelocele. INTRODUCTION Neural tube defects (NTDs) are mostly due to the failure of closure of the neural tube in the anterior and posterior neuropores resulting in the spinal cord or brain being 'open' and its outer surface formed by the wall of the central canal or ventricular system. A defect occurring at the upper end results in upper NTDs (exencephaly, anencephaly, encephalocele) and at the lower end in lower NTDs (spinal lesions, lumbosacral myelocele, meningomyelocele. Defects involving head and cervical and thoracic spines lead to cranio-rachischisis, which are also included in 1 NTDs. Most NTDs have serious consequences . The aim of the present study is to report the examples for the upper and lower neural tube defects. It is also aimed to review the incidence, formation, anomalies, etiology, prenatal diagnosis, prevention and risk assessment of the neural tube defects. Department of Anatomy, International Medical School, Bangalore, has 4 female specimens in the museum: 3 with upper and one with lower neural tube defects: The upper neural tube defects are 2 with anencephaly and rachischisis and one with acrania and rachischisis and the lower neural tube defect is meningomyelocele. The aim of the article is to report the museum specimens with anencephaly and rachischisis, acrania and rachischisis and meningomyelocele, as the examples for the upper and lower NTDs. MATERIAL AND METHOD Information is provided as a resource material for the specimens with neural tube defects in the museum. Department of Anatomy, International Medical School, Bangalore, has 4 specimens in the museum: 2 with anencephaly and rachischisis; one with acrania and rachischisis; and one with meningomyelocele. They were all female fetuses with age range from 4 months to full term. They were considered for the museum as the teaching specimens. KEY WORDS neural tube defects, incidence, sex ratio, types, management, etiology. Figure 1. Dorsal view: Anencephaly, iniencephaly and rachischisis: Note the partial absence of the brain; enlarged foramen magnum and the clefts in the vertebral column till midthoracic region. 1 Anatomica Karnataka, Vol-6, (3), Page 01-14 (2012) Review-Embryology Upper and Lower Neural Tube Defects- Review Figure 2. Dorsal view. Acrania, iniencephaly & rachischisis, sacral dimple: Note the absence of the cranium and a membrane like covering; partial absence of the brain; enlarged foramen magnum and clefts in vertebral arches of the vertebral column till sacral region. Figure 3: Dorsal view. Meningomyelocele: Note the open spina bifida cystica in thoraco-lumbar region with protrusion of meninges and spinal cord through vertebral defects and formation of sac filled with cerebrospinal fluid and covered with a thin membrane. A novel way of review has been attempted. From the text books in Embryology and Human Genetics, the relevant information pertaining to NTDs on the incidence, sex ratio, formation, types of NTDs and associated anomalies, etiology, management, prenatal diagnosis, prevention and risk assessment are presented. Incidence: (Table 1) 2 Anatomica Karnataka, Vol-6, (3), Page 01-14 (2012) Review-Embryology Upper and Lower Neural Tube Defects- Review Table 1: NTDs- Incidence NTDs & types Authors & Year Moore and 3 Persaud 2008 Incidence Spina bifida cystica 1/ 1000 births. UK: South Wales: 4.2/ 1000 births UK: Southeastern England: 1.5/ 1000 births. 10% of normal people. Spina bifida occulta in L5 or S1 vertebra Acrania with anencephaly Bradley –Smith 2 et al. 2010 4 Dudek 2010 Jorde et al. 2010 5 6 Sadler 2010 1/ 1000 births NTDs Northern Ireland: 1/ 300 USA: 1/ 1000 Types: 50%: spina bifida, 40%: anencephaly, 8.5%: encepahlocele 1.5%: iniencepahly NTDs Ireland: 1/200 births USA: 1/ 1000 births NTDs 1- 3/ 1000 newborns Northern China : 6/ 1000 births Hungary: 1/ 300 births NTDs Overall in USA: 1/ 1000 births & in North & South Carolina: 1/ 500 births. Northern China: 1/ 100 births. 1/ 1000 births. 10% of normal people. Spina bifida cystica Spina bifida occulta Sex ratio: 2 More females are known to be affected with NTDs;1M:1.3F. (Bradley-Smith et al 2010) The gathered information from some of the text books in Embryology and Genetics is tabulated. Table 2: Empiric Recurrence Risk for NTDs (Turnpenny and Ellard (2012) Disorder Incidence per 1000 Sex ratio Unaffected Affected parents parent having a having an 2nd affected child affected child - - - - Anencephaly 1.5 1:2 4-5% - Spina bifida 2.5 2:3 4-5% 4% NTDs 7 In general, the recurrence risk for the NTDs may be 10%. Children born to diabetic mothers may have an increased risk for the NTDs with a relative risk of 11.5%. In women with epilepsy, there exists the need for the review of the 2 treatment with the anticonvulsant. (Bradley-Smith et al. 2010) 3 Anatomica Karnataka, Vol-6, (3), Page 01-14 (2012) Review-Embryology Upper and Lower Neural Tube Defects- Review Table 3: Anencephaly and SB: Approximate recurrence risks without folate supplementation in 2 relation to the population incidence (Bradley-Smith et al. 2010) Population incidence of NTD- 0.005 % 0.002 % 0.001 % One sibling 5 3 2 Two siblings 12 10 10 2 1 1 One 3 degree relative 1 0.75 0.5 One parent 4 4 4 Relationship of affected individual to 'at risk' pregnancy nd One 2 degree relative rd NTDs: Formation Carlson (2004)1 The formation of the NT involves around 4 stages: I transformation of the general embryonic ectoderm into the neural plate; ii) changes in the shape of the neural plate, which becomes narrower and longer and also in the neuroepithelial cells as well as the in the rearrangements between the cells; iii) lateral folding of the neural plate resulting in neural groove and neural folds; iv) fusion of the neural folds resulting in the formation of NT. Even though the closure of NT starts at 21 to 22 days old embryo; two unclosed cephalic and caudal ends, the th anterior & posterior neuropores remain open and by 28 day the closure is completed. NTDs are mostly due to the failure of closure of NT in the anterior and posterior neuropores and also in other closure defects resulting in the spinal cord or brain being 'open' and its outer surface formed by the wall of the central canal or ventricular system. Turnpenny and Ellard (2012) 7 NTDs result from the defective closure of the developing st NT, during the 1 month of embryonic life. The different types of NTDs relate to the different embryological closure points of the NT. Dudek and Fix (2008) 8 Anencephaly, an example for upper NTDs occurs because 4 Anatomica Karnataka, Vol-6, (3), Page 01-14 (2012) Review-Embryology Upper and Lower Neural Tube Defects- Review defect is the spina bifida (SB). NTDs: Anomalies 1 Carlson (2004) I & ii. Cranioschisis is the closure defect of the brain and rachischisis is the closure defect of the spinal cord. Cranioschisis results in death; on the other hand rachischisis is associated with a wide variety of severe problems, including chronic infection, motor and sensory deficits and disturbances in the function of the bladder. Usually both defects are accompanied with anencephaly, a lethal defect wherein most of the brain failed to be formed. iii. Meningomyelocele one of the examples for the other closure defects is with bulging or entirely displaced spinal cord into the protruding arachnoid space and associated with displaced spinal roots and neurological problems. Turnpenny and Ellard (2012) 7 I Defects at the upper end of the developing NT results in exencephaly/ anencephaly or encephalocele; ii) defects at the lower end of the NT leads to spinal lesions such as a lumbosacral myelocele or meningomyelocele ; iii) defects involving the head plus cervical and thoracic spines lead to cranio-rachischisis. Most of the NTDs have serious consequences; anencephaly and cranio- rachichisis are not compatible with survival for more than a few hours after birth and large lumbosacral lesions usually cause partial or complete paralysis of the lower limbs and also impaired bladder and bowel continence. Dudek and Fix (2008) 8 I Anencephaly: The resulting changes are the failure in the development of the brain, formation of the lamina terminalis and the bony cranial vault. It is incompatible with extrauterine life; babies are still born or survive only a few hours or weeks after birth and it is the most common serious birth defect in stillborn fetuses. ii. Rachischisis (cleft vertebral column) refers to the vertebral abnormalities in a complex group of anomalies (axial dysraphic disorders) affecting primarily the axial structures. iii. The most severe type of SB causes paralysis from the 5 Anatomica Karnataka, Vol-6, (3), Page 01-14 (2012) Review-Embryology Upper and Lower Neural Tube Defects- Review the sac which is filled with cerebrospinal fluid. It is a severe type of SB cystica; the spinal cord and or nerve roots are included in the sac; may be covered with skin or a thin membrane and is associated with marked neurological defects inferior to the level of the protruding sac. Nervous tissue incorporated in the wall of the sac impairs the development of the nerve fibers. Hence, SB with meningomyelocele is a more common and a much more severe anomaly than SB with meningocele. level of the defect caudally and presents clinically as an open NT that lies on the surface of the back. The neural and vertebral defects may be extensive or restricted to a small area. Moore and Persaud (2008) 3 NTDs involve neural and non-neural structures, such as meninges, vertebrae, muscles and skin. I In acrania, the calvarium is absent; extensive defects of the vertebral column are often present and are incompatible with life. Severe cases of SB with meningomyelocele involving several vertebrae are often associated with partial absence of the brain- merencephaly. Sphincter paralysis (bladder and or anal sphincters) is common with lumbosacral meningomyelocele. There is almost invariably a saddle anesthesia when the sphincters are involved (loss of sensation when the body region that would contact the saddle during horseback riding). ii. Anencephaly results from the failure of the cranial end of th the neural tube to close during the 4 week and then it causes subsequent failure in the formation of the calvaria. iii. Meroencephaly (partial absence of the brain) is the most severe NTD as well as the common anomaly affecting CNS. The term anencephaly is in use; but it is a misnomer because a remnant of the brain tissue may be present. iv.1.C. Some meningomyelocele associated with craniolacunia (defective development of the calvaria) result in the depressed non- ossified areas on the inner surfaces of the flat bones of the calvaria. iv. SB is the general term in use for the NTDs affecting the spinal region. SB consists of the splitting of the vertebral arches and may or may not include the nerve tissue; based on which SB further classified as the SB cystica (iv.1) and SB occulta (iv.2.) iv.1.D. SB myeloschisis or rachischisis occurs occasionally; because the neural folds did not elevate and remained as a flat mass of neural tissue. SB with myeloschisis may result from NTDs caused by a local overgrowth of the neural plate resulting in the failure of the closure of the caudal th neuropore, at the end of 4 week. Myeloschisis the most severe type of SB; the spinal cord in the affected area is open because the neural folds failed to fuse; as a result the spinal cord is represented by a flattened mass of nervous tissue. iv.1. SB cystica, severe types of SB, involving protrusion of the spinal cord and or meninges through the defects in the vertebral arches are referred collectively as SB cystica because of the cyst like sac that is associated with these anomalies. SB cystica shows varying degrees of neurological deficits depending on the position and extent of the lesion. There is usually a corresponding dermatome loss of sensation along with complete or partial skeletal muscle paralysis. The level of the lesion determines the area of anesthesia and the muscles affected. SB cystica is found to be common in the lumbosacral region & further studied as the meningocele with only fluid- filled meninges or meningomyelocele with neural tissue in the sac. Bradley-Smith et al.(2010) 2 Included in the NTDs are the anencephaly, encephalocele, m y e l o c e l e o r r a c h i s c h i s i s , i n i e n c e p h a l y, meningomyelocele, spina bifida and spina bifida occulta. I Anencepahly, the lethal NTD is due to the failure of fusion of the caudal folds of the NT from 18 to 28 days of intrauterine life of the fetus with the result in the failure of the development of the forebrain. iv.1.A. SB cystica meningocele: The sac contains meninges and CSF; the spinal cord and the spinal roots are in their normal position; but there may be spinal cord abnormalities. ii. Chiari II malformation is the downward protrusion of the medulla below the foramen magnum thereby it overlaps the spinal cord and is seen in 70% of the cases with meningomyelocele and the symptoms increase with age. iv.1.B. SB cystica meningomyelocele occurs in the thoracolumbar region with protrusion of meninges and spinal cord through the vertebral defect and the formation of 6 Anatomica Karnataka, Vol-6, (3), Page 01-14 (2012) Review-Embryology Upper and Lower Neural Tube Defects- Review iii. Encepahlocele is the out-pouching of the brain mostly through the occipital bony defect either in the apical part of the occipital bone or through the posterior fontenelle. diagnosed prenatally and the pregnancies terminated. ii. Children with SB lose a degree of neurological function based on the spinal cord level of the lesion and its severity. Most defects of the spinal cord result from the abnormal rd th closure of the neural folds in the 3 and 4 weeks of development. The resulting NTDs may involve the meninges, vertebrae, muscles and skin. SB is the general term for NTDs affecting the spinal region. It consists of splitting of the vertebral arches and may or may not involve the underlying neural tissue. iv and v. Iniencepahly/ cranioschisis are the development abnormality of the skull and upper spines. vi. SB cystica is the result of the failure of the fusion of the rostral folds of the NT between the 18 to 28 days of gestation. Lesions are common in the lumbosacral region. vi.1. In SB meningomyelocele the spinal cord is also the component of the cyst. Two different types of spina bifida occur. One of the most serious vertebral defects is the result of imperfect fusion or non-union of the vertebral arches. Such an abnormality, cleft vertebrae or spina bifida may involve only the bony vertebral arches, leaving the spinal cord intact. The bony defect is covered by skin and no neurological defects then it is spina bifida occulta (ii.1). A more severe abnormality is spina bifida cystica (ii.2.) in which NT fails to close, vertebral arches fail to form, and neural tissue is exposed. Any neurological defects depend on the level and extent of the lesion. vii. Isolated NTDs are usually associated with vertebral anomalies and hydronephrosis. Jorde et al. (2010) 5 NTDs, one of the most important groups of birth defects and include anencephaly, spina bifida and encepahlocele. I Anencephaly is characterized by the partial or complete absence of the cranial vault and calvarium and also the cerebral hemispheres. 75% of the anencephaly is still born and the full term deliveries with anencephaly do not survive more than few hours or days. ii.1. SB occulta: A defect in the vertebral arches that is covered by skin and usually does not involve underlying neural tissue. It occurs in the lumbosacral region and usually marked by a patch of hair overlying the affected region. The defect is due to lack of fusion of the vertebral arches. ii. SB bifida is the most common type in NTDs with protrusion of spinal tissue (meninges, spinal cord, nerve roots) through the vertebral column. Nearly, 75% of the patients affected with SB have secondary hydrocephalus, which in turn gives rise to mental retardation. The other observed anomalies are the paralysis or muscle weakness, lack of sphincter control and club feet. The survival rates for the SB patients have been studied in British Columbia and it has showed a dramatic improvement over the past decades: less than 30% of children born between 1952 and 1969 have survived to 10 years of age; whereas it is 65% for the children born between 1970 and 1986. ii.2. SB cystica is a severe NTD in which the neural tissue and or the meninges protrude through the defect in the vertebral arches and skin to form a cyst-like sac. Most lie in the lumbosacral region and result in neurological deficits, but are not associated with MR. ii.2.A. SB with meningocele: In some cases with only fluid filled meninges protrude through the defect. iii. Encephalocele consists of the protrusion of the brain into an enclosed sac and never compatible with survival. ii.2.B. SB with meningomyelocele: In others with neural tissue inclusion in the sac. Vertebral anomalies and hydronephrosis are commonly seen in isolated NTDs. Additional anomalies may be present in 20% of the cases with NTDs; then the possibility of the syndrome with single gene disorder or chromosomal anomaly should be considered. Sadler (2010) iii. Occasionally the neural folds do not elevate but remain as a flat mass of neural tissue SB with myloschisis or rachischisis. 9 Dudek (2011) 6 NTDs, the congenital malformations of the nervous system are further classified as per the sites and the contents of the I Anencephaly is a lethal defect and most of these cases are 7 Anatomica Karnataka, Vol-6, (3), Page 01-14 (2012) Review-Embryology Upper and Lower Neural Tube Defects- Review defects. I Cranium bifidum (CB) occurs because of the failure in the formation of the bony skull, with defect in the skull, usually in the occipital region. i.1. CB with meningocele has the protruding meninges through the defect in the skull and form the sac filled with CSF. i.2. CB with meningoencephalocele has the meninges and the brain protruding through the skull defect and the form the sac filled with CSF. The outcome of the defect is poor ; the infants either die or have severe mental retardation. i.3. CB with meningohydroencephalocele occurs when the meninges, brain and portion of the ventricle protrude through the defective skull. ii. Anencephaly or meroanencephaly, the example for the upper NTDs is due to the failure of the closure of the th anterior neuropore, during the 4 week of development. It has failure of the development of the brain (? rudimentary brain may be present), formation of the lamina terminalis and the cranial vault. The condition is incompatible with extrauterine life. Mostly the infants are stillborn or survive from only a few hours to a few weeks. iii. SB is formed because of the failure in the proper formation of the bony vertebral arches, usually in the lumbosacral region. SB includes SB with meningocele, SB with meningomyelocele and SB with rachischisis. iii.1. SB with meningocele: The meninges protruding through the vertebral defect form a sac filled with CSF and the spinal cord is normal in its position. ii.2. SB with meningomyelocele: The meninges and the spinal cord protrude through the defect in the vertebral column and form a sac filled with CSF. iii.3. SB with rachischisis: Due to the failure in the closure of th the posterior neuropore during the 4 week of development. The most severe type of SB with paralysis from the level of the defect caudally. The variation presents clinically as the open NTDs on the surface of the back. The condition is also under the classification of the lower NTDs. iv. Arnold-Chiari malformation shows the herniated caudal vermis and tonsils of the cerebellum and the medulla oblongata through the foramen magnum. Clinical signs are 8 Anatomica Karnataka, Vol-6, (3), Page 01-14 (2012) Review-Embryology Upper and Lower Neural Tube Defects- Review possible adverse environmental factors. risk for the NTDs with a relative risk of 11.5%. Environmental factors involved in the etiology of NTDs have been identified and include poor socio economic status, multiparity and valproic acid embryopathy. The increased risk is also proposed for the NTDs with prepregnancy obesity in women. Dudek and Fix (2008) Folic acid antagonist, valproate, the anti-convulsant is st considered to be teratogenic in the early 1 trimester of the pregnancy. 9 The failure of fusion of NT is because of the faulty induction by the underlying notochord or from the action of teratogenic agents on the neuroepithelial cells in the neural folds. NTDs with genetic etiology are part of the chromosomal abnormality (Trisomy 13 or 18) or single gene disorders (Meckel syndrome with autosomal recessive mode of inheritance). Moore and Persaud (2008) Jorde et al. (2010) The formations of the NTDs are because of the combination of the genetic and or environmental factors. Sadler (2010) 6 Environmental: Hyperthermia, valproic acid and hypervitaminosis A produce NTDs as do a large number of other teratogens. The origin of most NTDs is multifactorial and the likelihood of having a child with such a defect increases significantly once one affected offspring is born. 3 Mostly NTDs are isolated and then the etiology is genetic and or environmental with multifactorial mode of inheritance. For the genetic, it is considered to be the additive effect of many genes and for the environmental, it could be viral, occupational hazards, chemicals and drugs. The considered teratogens may be the hyperthermia, valproic acid and hypervitaminosis A. It is suggested that the teratogen primarily disturbs the fate of the cells, adhesion between the cells and the mechanisms behind the closure of the NT. Valproic acid, an anticonvulsant drug causes NTDs in 1 to 2% of pregnancies, if given in early th pregnancy i.e. 4 week of development and also at the time when the neural folds are fusing and it is also associated to the increase in the risk of meningomyelocele. It has been shown that there may be evidence consistent with a maternal effect, as well as a sex-influenced effect on 10 NTD (Kristen, 2008) NTDs- Prenatal Diagnosis (PND): PND procedures such as the elevated á-fetoprotein (AFP) in the maternal serum or amniotic fluid and ultrasonography detect the presence of the NTDs. The prenatal diagnosis is considered to be the causes, in the decline in the incidence of the open NTDs in live- and still- births and the other factors are the general improvement in the diet and the intake of the periconceptional folic acid. In England and Wales, over the duration of 20 years, the combined incidence of the anencephaly and the spina bifida in live births and stillborn babies are declined from 1 in 250 in 7 1973 to 1 in 6250 in 1993. (Turnpenny and Ellard 2012) Pregnant animals exposed to hyperthermia or high levels of vitamin A are also associated to produce offsprings with NTDs. NTDs may also be secondary to or linked to lesions affecting the degree of flexion imposed on the neural plate, during the folding of the embryo. - AFP: In 1972, it was recognized that many pregnancies in which the baby had open type of NTDs, the NTDs could be detected at 16 weeks gestation by the AFP assay in maternal serum. AFP, the fetal equivalent of albumin is the major protein in the fetal blood. In the fetus with open NTD, the AFP level is increased in the amniotic fluid as well as in the maternal serum as the result of the leakage from the open NTD. Open NTDs are serious disorders; anencephaly is fatal and between 80 and 90% of the babies who survive with open lumbo-sacral lesions are severely handicapped. Maternal serum AFP screening for the NTDs is 100% neither sensitive nor specific. There exists the overlap, in Nutritional and environmental factors undoubtedly play a role in the formation of NTDs. Bradley-Smith et al.(2010) 5 2 Isolated NTDs are categorized into the mutlfactorial mode of inheritance with genetic and or environmental factors, as the causes. Several genes are implicated in the process of the elevation of the neural folds, which fuse to form the NT. Children born to diabetic mothers may have an increased 9 Anatomica Karnataka, Vol-6, (3), Page 01-14 (2012) Review-Embryology Upper and Lower Neural Tube Defects- Review 10 Anatomica Karnataka, Vol-6, (3), Page 01-14 (2012) Review-Embryology Upper and Lower Neural Tube Defects- Review 11 Anatomica Karnataka, Vol-6, (3), Page 01-14 (2012) Review-Embryology Upper and Lower Neural Tube Defects- Review of folic acid is neither known nor suspected for the proposed daily dose of folic acid and there are no contraindications too. In spite of the high- dosage of folic acid, the recurrence of NTD has occurred; then the association of the NTD with any syndrome has to be reconsidered. The recurrence risk may be 10% and irrespective of the benefits, the high-dosage folate supplementation should be continued for the next pregnancy. In women with epilepsy, there exists the need for the review of the treatment with the anticonvulsant. In general, because of the improved maternal nutrition, the birth prevalence of the NTDs seemed to be declining. (Bradley2 Smith et al 2010) Folic acid supplementation to mothers at the time of the conception is a major epidemiological finding in the prevention of NTD births. Several population studies have confirmed the finding. 50 to 70% of NTDs are preventable by dietary folic acid supplementation and folic acid deficiency could account for part of the elevated sibling recurrence risks for NTDs. However, there could be genetic variation in the response to the folic acid and it may be the reason that mothers with folic acid deficiency may not give rise to births with NTDs and mothers with folic acid supplementation may still give rise to births with NTDs. Research is being carried out to test the associations between NTDs and variants in several genes whose products are involved in folic acid metabolism (MTHR5 methylene tetrahydrofolate reductase). (Jorde et al. 2010) It is not clear whether the protective effect is due to the folic acid or the combination of folic acid and other vitamins; but studies have indicated that the periconceptional vitamin supplementation is an effective prevention strategy. The mechanism for the apparent effect is also not known. Regarding the use of folate, two recommendations are put forward: i) women who have had a child with NTD should take 4 mg/day of folic acid in case of planning another pregnancy ii) all women of reproductive age should take 0.4 mg/day of folic acid, the amount available in a typical multivitamin tablet, throughout their reproductive years. The second recommendation is in view of the fact that nearly 50% of pregnancies in USA are unplanned. In USA and other nations, folic acid is fortified to wheat and other grain products and in the past decade, after the initiation of the food fortification program, studies have demonstrated a 12 Anatomica Karnataka, Vol-6, (3), Page 01-14 (2012) Review-Embryology Upper and Lower Neural Tube Defects- Review effectiveness of surgery on NTDs. (Jorde et al. 2010) 5 A new treatment for the defect is to perform surgery in- utero at approximately 28 weeks of gestation; the baby is exposed by caesarian section, the defect repaired and the infant is placed back in the uterus. Preliminary results indicated that the approach reduced the incidence of hydrocephalus, improved the bladder and bowel control and increased motor development to the limbs. (Sadler. 6 2010) NTDs: Risk Assessment: Being multifactorial, the chances of having a child with NTD increases significantly in the presence of an affected offspring to the couple seeking genetic counseling and also with positive family history. Appropriate measures could be planned following genetic counseling under medical guidance. st Empirical recurrence risk to the 1 degree relatives (siblings and offsprings) vary according to the local population incidence and are as high as 4 to 5% in areas where NTDs are common. The incidence in the UK is highest in the people of Celtic origin. Such individuals move from their country of origin to another part of the world, the incidence of NTDs in their offsprings declines, but remain higher than amongst the indigenous population. These observations have suggested that there is a relatively high incidence of adverse susceptibility genes in the Celtic 7 population. (Turnpenny and Ellard 2012) Careful evaluation of the pedigree is necessary to determine the risk that applies to each pregnancy. Risks can be determined based on empiric data. In high-risk situations amniocentesis with assay of the chemical AFP has been used for PND in the past. Scanning of the fetus in conjunction with assay of maternal serum AFP has proved equally if not more reliable. Even with the best possible equipment and experienced sonographer, small closed NTDs could still be missed. Fortunately, the latter types of NTDs are not usually associated with the serious problems seen with the large open NTDs. (Turnpenny and Ellard 7 2012) Risk could be calculated for single gene disorders with the help of basic mendelian genetics and the applied probability theory. There are situations wherein, the disorder does not manifest single gene inheritance or 13 Anatomica Karnataka, Vol-6, (3), Page 01-14 (2012) Review-Embryology Upper and Lower Neural Tube Defects- Review Pvt.Ltd; 2008 th 9. Dudek RW. Embryology. 5 edition. Board Review Series. New Delhi, India: Wolters- Kluwer (India) Pvt.Ltd; 2011 10. Kristen L. Deak, Deborah G. Siegel, Timothy M. George, Simon Gregory, Allison Ashley-Koch, Marcy C. Speer. Further evidence for a maternal genetic effect and a sex-influenced effect contributing to risk for human NTDs, Birth defect research 2008; 82(10):662-669 11 . M o n i k a J a q u i e r. w w w. a n e n c e p h a l i e info.org/e/prevention.php 12. Pitkin RM. Folate and neural tube defects, Am J Clin Nutr 2007; 85(1)2855-2885 13. Hesekar HB, Mason JB, Selhub J, Rosenberg IH, Jacques PF. Not all cases of NTD can be prevented by increasing the intake of folic acid, Br J Nutr 2009; 102(2):173-180 14. Heseker H. Folic acid and other potential measures in the prevention of neural tube defects, Ann Nutr Metab 2011; 59(1):41-45 15. Koumudi Godbole, Urmila Deshmukh, Chittaranjan Yajnik. Nutri-genetic determinants of neural tube defects in India, Indian Pediatrics 2009; 46:467-475 16. Ashok Kumar. Neural tube defects: A neglected problem, Indian Pediatrics 2009; 46:665-667 17. Shubha Phadke, Meenal Agarwal. Neural tube defects: A need for population based prevention program, Indian J Hum Genet 2012; 18(2):145-147 CORRESPONDENCE ADDRESS Dr. Leelavathy N Associate Professor, Department of Anatomy Saptagiri Institute of Medical Science & Research Center, Chikkasandra, Hesaragatta Main Road, Bangalore 560090 Mobile: 91 99010 24059, <rrleela@rediffmail.com>, <rrleela@gmail.com>, 14 Anatomica Karnataka, Vol-6, (3), Page 01-14 (2012)