In This Issue
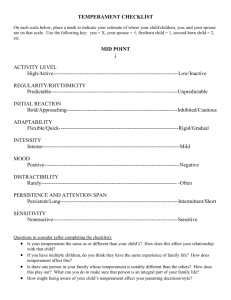
advertisement

ResNet Magazine of the UQMS Research Network In This Issue: Burns, Trauma & Critical Care Research Centre UQ Centre for Clinical Research UQMS Call for Abstracts Issue 1, 2009 Foreword by Professor David Wilkinson From the Editorial Team From the UQMS President Welcome to the first edition of ResNet – the research magazine compiled by students for students! Whatever your interest level or previous experience in research, we hope you will find something that appeals to you within. Why should medical students be interested in research? Isn’t there enough to do? The MBBS program itself, family, friends, interests, earning some dollars? Perhaps research is something a bit distant from your priorities right now, but that may not always be the case, and for some students research is an interest now for many reasons. My own first exposure to research was when I did an intercalated degree in pharmacology between MBBS 2 and 3 at the University of Manchester. That experience was lab research, and to be honest it did not really excite me. My next exposure was when working in Africa after my intern year in the UK. I found myself asking all sorts of questions: why did these babies die this way? / how can I improve outcomes of kids with malnutrition? / what is a better way to improve treatment completion among kids with TB? And so on. I then got excited because the questions and answers were of direct relevance to my clinical work. And, I found, I had a restless and enquiring mind. I soon found that I HAD to know the answers, and I soon found great joy and satisfaction in designing and executing studies well, so that the answers were ‘true’. Publishing also led to a buzz. For me a significant research career followed, one that allowed me to meet some great people, travel the world, and make some pretty significant contributions to knowledge. Here at the School we are keen to offer meaningful research opportunities to students that want them. The main mechanism in the future for this is the 1 year MPHIL degree between MBBS2 and 3, with a scholarship provided to support living costs. Well done to UQMS (again) for showing initiative with ResNet, and here’s hoping that for some of you, at some stage in your careers, research forms a part of it. ResNet is an initiative of the newly formed UQMS Research Network, and is aimed at helping students to get more involved in research. Throughout the magazine you will find some high-quality abstracts from both honours and research higher degree students within the School of Medicine. We have also endeavoured to allow the experts share their experience with us. These articles will help you integrate research into your clinical practice in your future medical careers and demonstrate the wide scope of possible research topics. And of course, research is of no use if it is not applied effectively. For this reason we have included EBM corner. These articles are written by students encountering clinical problems, with expert commentary provided by the guru of all things EBM - Dr David King. You will also be able to read profiles on worldclass research facilities, book reviews on the latest research textbooks, and almost anything else related to research! Finally, and perhaps most importantly, we have started a ‘Research Classifieds’ section in the magazine. In the future we hope this will evolve to become a core hub of the student research network, including advertisements for research assistant positions, recruiting drives for subjects, as well as interest groups within each clinical schoolwatch this space! Welcome to the first edition of ResNet, the first of many publications to promote medical student research at the University of Queensland. Firstly I would like to extend my congratulations to the Research Subcommittee (Mike Tuppin and Pete Stickler) for their hours of hard work and initiative on this project and indeed, the plethora of research support initiatives that UQMS is now able to provide their students. Why ResNet? It is our belief that our UQ medical students produce amazing research of extremely high quality which deserves recognition and support form their student body. This publication is about ensuring our wider community of fellow peers, staff and beyond, are aware of the fascinating work that our students produce; we believe it is essential that our students set a standard of excellence to inspire others to do the same. Only by nurturing such a culture can we hope to encourage all of our students to embrace medical research and continue with this in their future directions. We hope it will assist in informing, inspiring, and above all, recognising that there are many, many individuals out there that share the same passions in research. These are your colleagues and this is the amazing network you too will become a part of, whether you make research a career in itself or when you utilise these discoveries in your own medical practice. We look forward to seeing your name in ResNet in the near future. Tanya Trinh, UQMS President Michael Tuppin & Peter Stickler If you would like to become more involved in ResNet, then we would love to hear from you! Please email your interest to the editor: m.tuppin@uq.edu.au Highlights This Issue • This issue’s profile piece is on the Burns, Trauma and Critical Care Research Centre at the Royal Brisbane & Women’s Hospital. Feature researcher is Dr Jason Roberts. • We also profile the UQ Centre for Clinical Research at the Royal Brisbane and Women’s Hospitalmandatory reading for anyone considering a PhD! • Dr Ian Yang gives us some insight into how to get started in research • Dr Diann Eley shares her research examining the influence of character and temperament on rural workforce shortages. • Dr Mark Schubert shares his thoughts on qualitative research in ‘The Last Word’ • We review the book ‘Introduction to Research in the Health Sciences’ • Call for abstracts for the 2009 UQMS Research Network Colloquium emergency physicians, scientists, physiologists, nutritionists, physiotherapists and intensive care nurses. From Bench To Bedside... In the Burns, Trauma & Critical Care Research Centre, laboratory research is closely allied with clinical research to ensure translation from bench to bedside. The major themes within the centre are: Antibiotic resistance and infection control in the critically ill. Profile Piece In hospitals today, especially in ICU, there are a number of pathogens emerging which are resistant to most drugs. These commonly occur in long stay, debilitated patients and contribute to increased risk of death, longer hospital stay, further weakness and long term dysfunction. Studies that address antibiotic resistance and infection control are thus, an imperative. Pharmacokinetics and drug distribution in the critically ill. Bali Bombings Give Rise to the Burns, Trauma and Critical Care Research Centre... In 2002, the devastation and tragedy of the Bali bombings focused national and international attention on burns victims. The outstanding response from the critical care and burns staff of Royal Brisbane & Women’s Hospital (RBWH) and The University of Queensland (UQ) highlighted the skill and expertise possessed in this area. Nonetheless, the event emphasised that there was a critical need to improve the treatment and outcomes of burns and critically ill patients. In response, the Burns Trauma and Critical Care Research Centre (BTCCRC) was established to further advance and improve the level of treatment and care given to burns and critically ill patients through world-class research-based clinical practice. Initially a collaborative venture between the RBWH Burns and Intensive Care Units (ICU) and UQ, the Department of Emergency Medicine (DEM) was incorporated into BTCCRC in 2008. BTCCRC is headed by Director, Professor Jeffrey Lipman, and chaired by Dr Jenny Paratz. The main aims of the research centre are to: • Improve both the survival and outcome of patients through high quality researchdriven evidence base for clinical practice in the burns, trauma and critical care areas. • Establish national and international collaboration in the above areas, thus increasing research opportunities. • Enhance the research training and knowledge base of postgraduate students and staff. Since its inception in 2002, the BTCCRC has expanded from 3 staff to an impressive 46 staff and students in 2008. With this growth, the research focus on burns, critical care and trauma over the years has expanded to include anaesthesia and, more recently, emergency medicine. Our clinical research is based on a solid foundation of multidisciplinary collaboration between intensivists, burns surgeons, anaesthetists, cardiologists, neurosurgeons, Critically ill patients often require different doses of antibiotics and other drugs, particularly if they are on renal dialysis. Professor Jeffrey Lipman has pioneered work that demonstrates that patients in ICU are not receiving enough antibiotics to achieve optimal levels to kill pathogens. Our centre uses the specialized technique of microdialysis for in vivo monitoring of local concentrations of drugs and metabolites in tissue, in an attempt to determine optimal antibiotic administration. Management and outcome of critically ill, trauma, head injury and long stay ICU patients. Patients who survive intensive care often are weak, debilitated and with a poorer quality of life compared to their pre-morbid status. We are actively investigating methods to prevent weakness and loss of function in long stay ICU patients ensuring the best quality of care is offered. Critically ill patients with renal dysfunction. This is a relatively new area of collaboration with the Department of Renal Medicine. Patients with existing renal dysfunction can have additional problems if they become Intensive care unit (ICU) patients that develop sepsis represent a huge financial burden to the healthcare system. Sepsis occurs in 12% of patients admitted to ICUs and has mortality rates approaching 50% for severe sepsis. Antibiotic therapy has been shown to be the most effective intervention available to clinicians and further efforts to maximize antibiotic efficacy has been suggested to provide greater reductions in morbidity and mortality. Broad spectrum β-lactam antibiotics are commonly used for empiric treatment of sepsis, although little is known about the pharmacokinetics (PK) and pharmacodynamics (PD) of these antibiotics in interstitial fluid which is the ‘target site’ of most infections. Significant laboratory data suggests that administration of β-lactams by a continuous infusion (CI), as opposed to intermittent bolus (IB) doses, maximizes antibiotic activity, although this mode of administration is rarely used clinically for these antibiotics. The aims of this research were: (1) to determine the comparative tissue PK and PD of IB dosing and CI for two β-lactam antibiotics, piperacillin and meropenem, in ICU patients with sepsis, using a novel technique called microdialysis; (2) to determine the differences in clinical outcome between both modes of administration for another broad spectrum β-lactam antibiotic, ceftriaxone, in a small prospective pilot study; and (3) to metaanalyse the data from all known published studies comparing clinical outcomes between IB dosing and CI. The first two studies demonstrated that CI maintains a statistically significant superior PK profile compared with IB for critically ill especially with issues of drug dosage, weaning from mechanical ventilation and overall outcome. Management and outcome of burns patients including pain control, myocardial dysfunction, exercise and metabolism, fluid and nutritional management post burn. Thermal injury is a devastating injury, not only for the immediate concern of loss of life and extreme pain, but in the long term cosmetic and functional issues. Therefore a need to improve treatment and outcomes of burns patients is critical. Our burns unit, one of the largest in Australia, has instituted a large number of studies investigating initial cardiac function ORIGINAL ABSTRACT An investigation of the utility of continuous infusion vs intermittent bolus dosing of beta-lactam antibiotics in critically ill patients with sepsis Dr Jason Roberts BAppSc, BPharm(Hons I), PhD the antibiotics piperacillin and meropenem, in the plasma and subcutaneous tissue of ICU patients with sepsis (P<0.05) (Crit Care Med 2009;37(3):926-33; J Antimicrob Chemother 2009; in press). CI therefore achieves superior PD targets at the target site of infections in this patient population. The third study demonstrated that in a small cohort of ICU patients (n=58) with severe infections requiring 4-or-more days ceftriaxone therapy will have statistically superior clinical (p<0.05) and bacteriological (p<0.05) outcomes when administered by CI ( J Antimicrob Chemother 2007;59(2):28591). The final study, a meta-analysis that combined the data from all clinical studies, demonstrated no difference in mortality (P=1.00) or clinical cure (P=0.83) between β-lactam administration by IB or CI in all hospitalized patients (Crit Care Med 2009; with large burns, management of pain, antibiotic efficacy, nutrition issues, exercise post burns and prevention of heterotopic ossificans (bone formation outside of the skeleton, usually in soft tissue). Anaesthesia. Currently, there is a steady stream of research in difficult airway management needed for a growing teaching arm in this area. Our research focuses on the need for classification of difficult airways. Our proposed model “Model for Direct Laryngoscopy and Tracheal Intubation” which has been used by others - addresses the need for a structured, logical approach to airway assessment. Additionally, 37(6) in press). The heterogeneity of patient groups included in this study, some of which were ICU cohorts with inexplicably low mortality rates, may have prevented any advantages of CI or IB emerging. However, large confidence intervals were observed suggesting that a difference may still exist. The research described above has significant implications for world-wide medical practice and future research in this area. We have been able to show that CI achieves superior PD targets in both plasma and interstitial fluid providing strong support for administration of β-lactams by CI to ICU patients with sepsis. Optimizing β-lactam activity, using CI, in these patients may have profound effects on patient morbidity and mortality. The meta-analysis data suggests this advantage of CI is likely to be limited to ICU patients, with the greater hospital population less likely to derive clinical benefit. Validation of these results with a large prospective multi-centre randomized controlled trial in ICU patients with sepsis, requiring at least 4-days β-lactam therapy, is suggested. Dr Jason Roberts completed his PhD in the UQ School of Medicine in 2009, under the supervision of Prof J Lipman. He is a clinical pharmacist working at the Royal Brisbane & Women’s Hospital, and is an academic staff member of the Burns, Trauma & Critical Care Research Centre. in order to understand the changes in airway morphology with different head and neck positions, we have developed a new TwoCurve Theory which is the basis for the development of clinically-relevant difficult airway algorithms. Both areas of research and development attempt to reassess the current trends in this area. Emergency medicine. New to the research centre, DEM research focuses on improving outcomes and evaluating new processes for treating patients in the Emergency Department. ORIGINAL ABSTRACT Can we alter risk factors for oesophageal cancer with exercise? The BTCCRC boasts worldclass facilities... The BTCCRC boasts bioanalysis capabilities that are out of the reach of most ICU’s worldwide. For over a decade, they have been measuring drug levels in plasma, ultrafiltrate, urine and microdialysate by techniques of HPLC and ELISA. With exclusive access to an Applied Biosystems API2000 LC-MS/ MS, analysis of smaller and less concentrated samples is now possible. Last year saw the expansion of the bioanalysis facility into the new University of Queensland Centre for Clinical Research (UQCCR) building, fitting accommodation for our new Shimadzu Prominence HPLC system. Additionally, the BTCCRC Tissue Culture Laboratory also moved into the stylish, advanced facilities of the new UQCCR. The move has helped facilitate collaborations between the centre and other researchers within UQCCR and has allowed us access to state-of-the-art equipment and facilities. This, together with our links to the Tissue Banking Facility at the RBWH, will help to align our clinical research in tissue burns with our lab-based cell culture research. Dr Sia Athanasas-Platsis WANT TO WRITE ARTICLES FOR RESNET? Do you want to get more out of ResNet? Want to unleash your creative talents? Then we want to hear from you! You can contribute to ResNet through writing book reviews, profile pieces, research abstracts, EBM articles, reflective commentaries and so much more! You can also flex your creative muscle by helping with the design and editorial process. So what are you waiting for? Contact the ResNet team today! To contact, email your interest to the editor at: m.tuppin@uq.edu.au Brooke Winzer BPhty(Hons I), PhD candidate Oesophageal adenocarcinoma is rising rapidly in incidence as a consequence of populationwide increases in obesity. Barrett’s oesophagus (BE), the precursor to adenocarcinoma, is also rising in incidence, but currently there is an absence of evidence about ways to reduce the rate of progression to cancer. Patients with BE are known to have disturbances across an array of biochemical and hormonal axes, including elevated serum concentrations of the adipokine leptin, insulin and the inflammatory mediators interleukin-6 and tumour necrosis factoralpha. It is likely that these disturbances would promote cancer development. There is some trial evidence that moderate-intensity exercise training can abrogate hormonal perturbations in overweight people without BE, but to date, no such evidence exists for patients with BE. By randomising 120 overweight, sedentary males with BE to either an exercise group or a stretching control group, we aim to determine whether 24 weeks of moderate-intensity exercise training (1hr, 5 days per week) will lead to changes in levels of certain hormones associated with oesophageal adenocarcinoma development. This will be one of the first exercise intervention trials with the goal of changing the hormonal milieu of patients with BE to reduce oesophageal adenocarcinoma risk. Through studying a population with a pre-malignant condition we also hope to gain information regarding the capacity of exercise to prevent cancer and the mechanisms involved. Brooke Winzer completed her physiotherapy degree at LaTrobe University in 2005. She is a PhD student in the School of Medicine under the supervision of Dr J Paratz from the BTCCRC. Her study is funded by a Wesley Research Institute Grant. Thinking about medical research? It’s time to ask questions! Why do research? For researchers in the field of biomedical research, the lifelong journey of answering important medical questions often starts with a spark, and then grows to a passion. The seeds for ideas most frequently come from our patients, their health and disease. Ultimately our goal as clinicians, researchers and teachers is to improve outcomes for our patients, by pushing the boundaries of understanding disease pathogenesis, ensuring early and timely diagnosis, and developing and using the most effective prevention and treatment. Answering these questions is both challenging and exciting. How to start The best way to start is to develop curiosity, interest and awareness about how research works, and to find out about research opportunities that are available. Biomedical research covers many disciplines e.g. epidemiology of acute and chronic diseases, application of basic sciences to clinical medicine, diagnostic strategies, development of therapeutics and testing through clinical trials etc - just to name a few. There are many opportunities available for keen early career researchers in the School of Medicine’s Clinical Schools, Disciplines, Research Centres and teaching hospitals. Joining a multidisciplinary team that does research can be made easier by making links with established clinical researchers, such as through the UQMS Research Network, or through your colleagues and clinical tutors. Research opportunities exist at any career stage - for undergraduate students, higher degree students, and for health professionals after graduation. factor), compared to weekday admissions (Comparison) experience worse in-hospital mortality (Outcome)? Another example is a research project we’re working up with our pharmacy colleagues: In patients on long term oxygen therapy (Population), does sesame oil (Intervention), compared to other nasal barrier treatments (Comparison) reduce nasal irritation and encourage adherence to oxygen therapy in patients using nasal prongs for oxygen delivery (Outcome)? Once the question is framed, and the hypothesis is defined, further details about background information (literature review), study design, methodology and statistical analysis can be prepared for research proposals, ethics applications and research grant applications. Ethics approval is an important process before commencing a research study, and funding provides resources to undertake research. The National Health and Medical Research Council (NHMRC), the peak national funding body for biomedical research, recommends criteria for quality assessment of research and research teams, including: • Significance and/or innovation: potential to increase knowledge about human health, and application of new ideas; • Scientific quality: strengths and weaknesses of the research plan and the experimental design; • Track record in relation to opportunity: standing and skills of the research team, and ability to undertake the project. These quality criteria are useful to consider when designing research projects. Planning research The ‘PICO’ framework helps to ask relevant clinical questions, giving a structure for the hypothesis of a research question in terms of Population, Intervention, Comparison and Outcome. For example, our team recently helped an MBBS Honours student researcher to ask the question: In patients with acute illnesses such as cardiac disease or chronic obstructive pulmonary disease (Population), do weekend admissions (Intervention, or Outcomes of translational research The eventual outcome of biomedical research is to improve the health of the population. Translational research can be thought of as being in two phases 1: the first is ‘benchto-bedside’ in which scientific advances are applied to understanding disease pathogenesis and better ways of diagnosing and treating Dr Ian Yang MBBS, FRACP, PhD, Grad Dip (Clin Epi) Dr Ian Yang is a consultant thoracic physician at The Prince Charles Hospital, and is also an Associate Professor and Head of the Northside Clinical School in the UQ School of Medicine. disease; the second is ‘bedside to clinic’ in which results from clinical trials are translated into clinical practice. It is well-recognised that translational medical research is bidirectional in nature e.g. from bench to bedside, and bedside to bench 2 . There is an inherent cross-fertilisation between basic and clinical sciences, including in respiratory sciences 3. Thus interdisciplinary teams are required to work together to share resources and skills, in order to synergise to address complex human disease questions. Shared knowledge and communication are essential, with clinicians learning the language and techniques of science, and basic scientists acquiring knowledge of clinical research design and aspects of clinical disease. Translational biomedical research enables knowledge from physiology, molecular and cellular biology disciplines to be applied to human disease 4. In this way, there is a directed pathway of applied knowledge from ‘molecules to models to humans’ 4. This is seen particularly in the application of genomics, epigenomics, transcriptomics and proteomics to studying lung diseases 5. For example, our PhD students and research scientists in our team have recently used gene expression microarrays on lung tumour tissue, to study lung cancer outcomes 6-8. These and other studies have identified gene signatures that have predictive ability for susceptibility to lung cancer and risk of recurrence after surgery. Furthermore, other recent studies have shown distinct gene signatures in chronic lung disease such as COPD 9. All of these features of translational research also apply to ‘bedside to clinic’ research that focuses on clinical practice. ORIGINAL ABSTRACT A pilot study into the reproducibility of electrical impedance tomography Lawrence Caruana BPhty, MPhil candidate Caruana L1, 2, Barnett AG2, 3, Tronstad O2,& Fraser JF1, 2 1 The University of Queensland, Brisbane. 2 The Prince Charles Hospital: Critical Care Research Group, Brisbane. 3 Queensland University of Technology, Brisbane. The aim of this study was to assess the reproducibility of electrical impedance tomography, and is a within subject observational design. Five healthy male volunteers were placed in the supine position and connected to the Draeger Medical Electrical Impedance Tomography Evaluation Kit 2 (Lubek, Germany), which uses a 16 electrode array and a pneumotachometer (Ventrak Model No 1550: Novametrix Medical Systems, Wallingford, USA). Concurrent two minute recordings of tidal variations, ventilation distribution and tidal volumes Challenges and opportunities Time and resources are major challenges for any researcher. And of course, the results of any proposed project can’t be predicted ahead of time – the goal is basically to ask relevant questions and then go ahead to answer them in the best way possible. On the other hand, beneficial outcomes for biomedical researchers, including early career researchers, are research training in developing and carrying out research projects; learning new methodologies; skills in communication, team work, time were made in the morning and repeated in the afternoon. Every effort to ensure identical electrode placement was made. The Bland and Altman statistic was used to determine the limits of agreement for the tidal variations, tidal volumes, and ventilation distribution. A Pearson correlation between tidal variations and tidal volumes was used to judge the transferability of the limits of agreement. Descriptive statistics were used to compare actual and predicted tidal volumes, and for comparison to fractal ventilation. Results demonstrated significant correlation between tidal variations and tidal volumes (Pearson correlation = 0.72, p < 0.001), allowing for tidal variations to be judged as in agreement between readings. The tidal volumes showed a coefficient of variation similar to that of fractal ventilation at 26.7%. The ventilation distribution showed significant ‘clustering’ above or below the zero line indicating a lack of agreement. A number of possible causes for this lack of agreement existed including that regional distribution might be fractal. Electrical impedance tomography tidal variations are reproducible and could be useful in clinically assessing the effects of recruitment manoeuvres or positional changes. Lawrence Caruana completed his physiotherapy degree at the University of Queensland in 1987 and works at The Prince Charles Hospital as an advanced clinician. He is currently a MPhil candidate in the School of Medicine under the supervision of Dr J Fraser. management and leadership; presentation skills (e.g. poster or oral presentation at scientific and clinical meetings); publications in peer-reviewed journals; and satisfaction from discoveries that lead to change in health care practice. Research and teaching are integral parts of clinical practice, and a track record in research and teaching can boost job applications and career advancement. So, if you’re energetic, motivated to be involved in research, and have the desire to learn and discover, it’s time to ask questions! UQ Useful links www.uq.edu.au/research/ Information and resources about research at UQ NHMRC www.nhmrc.gov.au/ Information about the research activities of the NHMRC Nobel Prize for Medicine 2005: Barry Marshall and Robin Warren http ://no b elprize.org/no b el_prizes/ medicine/laureates/2005/ The most recent Australian Nobel Laureates – fascinating videos to watch about how they made their landmark discoveries References 1. Woolf SH. The meaning of translational research and why it matters. JAMA 2008;299(2):211-3. 2. Horig H, Marincola E, Marincola FM. Obstacles and opportunities in translational research. Nat Med 2005;11(7):705-8. 3. Farre R, Dinh-Xuan AT. Translational research in respiratory medicine. Eur Respir J 2007;30(6):1041-2. 4. Sabroe I, Dockrell DH, Vogel SN, Renshaw SA, Whyte MK, Dower SK. Identifying and hurdling obstacles to translational research. Nat Rev Immunol 2007;7(1):77-82. 5. Yang IA, Holloway JW. Asthma: advancing gene-environment studies. Clin Exp Allergy 2007;37(9):1264-6. 6. Larsen JE, Fong KM, Hayward NK. Refining prognosis in non-small-cell lung cancer. N Engl J Med 2007;356(2):190. 7. Larsen JE, Pavey SJ, Bowman R, et al. Gene expression of lung squamous cell carcinoma reflects mode of lymph node involvement. Eur Respir J 2007;30(1):21-5. 8. Larsen JE, Pavey SJ, Passmore LH, et al. Expression profiling defines a recurrence signature in lung squamous cell carcinoma. Carcinogenesis 2007;28(3):760-6. 9. Yang IA, Francis SM. Deconstructing COPD using genomic tools. Respirology 2009;14(3):3137. Investigating the Influence of Temperament and Character on the Rural Medical Workforce Shortage Dr Diann Eley BSc, MSc, PhD Dr Diann Eley is the Director of Research at the Rural Clinical School Research Centre, UQ School of Medicine. d.eley@uq.edu.au Like most research, this work was born out of a problem - specifically, why is it so difficult to get doctors to work in rural and remote areas? 1, 2 The literature reports on several key indicators of rural recruitment and retention such as rural origin, 3 spouse and family influences, positive clinical and lifestyle experiences 4, 5 and more recently the generational factors associated with ‘X’ and ‘Y’. 6 Our research approaches the dilemma of increasing the rural medical workforce by investigating how individual temperament and character traits may provide clues to improve the recruitment and retention of rural doctors. Although acknowledged by anecdotal narrative, the unique personality and lifestyle of doctors in rural and remote locations worldwide has received little attention in the research literature. This is despite its recognition as an entity in itself comprising advanced skill sets different from urban counterparts. Personality is made up of two major components; temperament and character. Temperament is pre-disposition - a configuration of inclinations. Character is disposition - a configuration of habits. Each of us develops the habits appropriate to our temperament but those habits are influenced by the innumerable external factors – good and bad - we are exposed to as we develop. For example; think of your brain as a computer with temperament as its hardware and character as its software. The hardware is the physical base from which character emerges. In other words, temperament is the inborn form of human nature and character, the emergent form which develops through the interaction of temperament and environment. The psychobiological theory of personality underpins the main tool we employ for this work, the Temperament and Character Inventory (TCI) 7. The TCI assesses levels of the seven scales of temperament and character traits. Each trait is multifaceted with high and low descriptors summarized in Table 1. Our research is not about ‘typing’ people or professions. There is no one ‘type’ of person who chooses a profession or to work in a particular location. Instead there are particular combinations of temperament and character traits that predispose individuals to certain areas and interests in life and equip them with the requisite ability to adapt to their decisions. The specific and unique combination of temperament traits, that are mildly heritable, and character traits, which are developmental and influenced by sociocultural learning contribute most strongly to our personalities and influence our choices throughout life. 7, 8 To date, our research findings from samples of rural and urban doctors, medical students and most recently nurses consistently depicts them as highly ‘self directed’ (character), ‘cooperative’ (character) and highly ‘persistent’ (temperament) individuals. In other words, they all possess traits that contribute to a profile that would be expected of successful professionals in the medical sciences. It is interesting and significant that apart from persistence, these are traits of ‘character’, meaning they have developed through maturation and socio-cultural learning. These traits would be familiar to teachers as those of ‘good students’ and high achievers. But although these character traits may be omnipresent within the medical profession – it is the temperament traits that drive the personality, dictates the level of adaptability and provides a unique ‘flavour’ to each individual. 9, 10, 11 The most significant findings from our research are that three temperament traits of ‘novelty seeking’, ‘harm avoidance’ and ‘reward dependence’ are integral to identifying differences between various groups. This indeed is an important finding in regards to recruitment and retention efforts. The utility of understanding the temperament and character trait profiles of individuals and groups is that temperament traits, being stable and innate, may be predictive of individuals with similar temperament profiles. For example, identification of the temperament profiles of successful doctors in various roles and practice locations may be indicative (predictive) of the traits conducive to coping in those roles and locations. On the other hand, the developmental nature of character would allow modification or development of those traits through training and education. Both could be of value to educators, recruiters and policy-makers through a better understanding of which traits are most conducive to certain disciplines and their environments. Our data consistently demonstrates that while high levels of core traits; self directedness, cooperativeness and persistence seem to be a prerequisite for success in rural practice, the various levels and combinations of novelty seeking, harm avoidance and reward dependence are most essential to understanding how individuals adapt in their own way to rural medicine. And likewise what separates those who stay and those who leave rural practice i.e. retention issues. There are a myriad of biological, environmental and developmental factors, opportunities and circumstances that influence our decisions in life and make us what we are. There is no one right or wrong trait profile that we could ‘clone’ to alleviate our rural medical workforce shortages. Our research has begun to establish a psychobiological profile of rural doctors. Certainly a better understanding of the temperament and character trait profiles of the professionals who adapt and flourish in the rural environment will provide educators and policy makers with a better comprehension of what it takes to be a ‘rural doc’ and inform the development or modification of training, initiatives and recruitment procedures accordingly. References 1. Wilkinson D. 2000. Inequitable distribution of general practitioners in Australia: Analysis by state and territory using census data. Australian Journal of Rural Health, 8: 87-93. 4. Dunbabin, J., Levitt, L. 2003. Rural origin and rural medical exposure: their impact on the rural and remote medical workforce in Australia. Rural and Remote Health, 3 (online), Available from: http://rrh.deakin.edu.au (Accessed 20 August 2007). 2. Humphreys JS, Jones MP, Jones JA, Mara P. 2002. Workforce retention in rural and remote Australia: determining the factors that influence length of practice. Medical Journal of Australia, 176: 472-476. 5. Eley, D., Baker, P. 2007. Will the Australian Rural Clinical Schools be an effective workforce strategy? Early indications of their positive impact on intern choice and rural career interest. Medical Journal of Australia, 187:166-167. 3. Somers, G.T., Strasser, R., Jolly, B. 2007. What does it take? The influence of rural upbringing and sense of rural background on medical students’ intention to work in a rural environment. Rural and Remote Health, 7: 706 (online), Available from: http://rrh.deakin.edu.au (Accessed 20 August 2007). 6. Twenge JM. 2009. Generational changes and their impact in the classroom: teaching Generation Me. Medical Education, 43: 398-405. 7. Cloninger CR, Svrakic DM, Przbeck TR. Psychobiological model of temperament and character. Archives of General Psychiatry 1993; 50: 975-990. 8. Cloninger CR. Feeling Good 2004, Oxford Univ Press: New York. 9. Eley D, Young L, Shrapnel M. Rural temperament and character: A new perspective on recruitment and retention of rural doctors. Australian Journal of Rural Health 2008; 16, 12-22 10. Eley D, Young L, Prysbeck T. Exploring temperament and character in medical students; a new approach to selection and training to increase the rural workforce. Medical Teacher 1112-2008, 1-6, iFirst. 11. Eley D, Young L, Prysbeck T. Exploring the temperament and character traits of rural and urban doctors; implications for retention of the rural workforce. Journal of Rural Health (USA) 2009, 25; 1: 43-49. Table 1: Temperament and character descriptors TEMPERAMENT is defined as those components of personality that are heritable, developmentally stable, emotion based and not influenced by socio-cultural learning. The four dimensions of Temperament, all of which reflect a heritable bias are: TEMPERAMENT High Scorers Low Scorers Novelty Seeking: NS - observed as exploratory activity in response to novelty, impulsiveness, and extravagance exploratory & curious impulsive, disorderly extravagant & enthusiastic seeks challenge indifferent, reflective frugal & detached orderly & regimented Harm Avoidance: HA - observed as pessimistic worry in anticipation of problems, fear of uncertainty, shyness with strangers, and rapid fatigability worrying & pessimistic fearful & doubtful shy , fatigable indecisive relaxed & optimistic bold & confident outgoing, vigorous opinionated, decisive Reward Dependence: RD- indicates cues of social reward and is observed as sentimentality, social sensitivity, attachment, and dependence on approval by others sentimental & warm dedicated & attached dependent needs to please seeks approval from others practical & cold withdrawn & detached independent not influenced by others socially insensitive Persistence: PS - describes behaviour despite frustration, fatigue and reinforcement. It is observed as industriousness, determination and perfectionism industrious & diligent hard-working ambitious & overachiever perseverant & perfectionist determined inactive & indolent gives up easily un-ambitious underachiever quitting & pragmatist CHARACTER traits reflect personal goals and values and are subject to socio-cultural learning. Each trait quantifies the extent to which an individual displays certain related qualities CHARACTER High Scorers Low Scorers Self Directness: SD - quantifies the extent to which an individual is responsible, reliable, resourceful, goal-oriented and self-confident responsible & reliable purposeful, self accepted resourceful & effective habits congruent with long term goals blaming & unreliable purposeless, self-striving inert & ineffective habits congruent with short term goals Cooperativeness: CO - quantifies the extent to which individuals are cooperative, tolerant, empathic and principled socially tolerant empathic, helpful compassionate, constructive ethical & principled socially intolerant critical, unhelpful revengeful & destructive opportunistic Self Transcendence: ST - quantifies the extent to which individuals conceive themselves in relation to the universe as a whole. It is observed as spirituality, practicality, materialism and modesty wise & patient creative, imaginative self-effacing united with universe modest , humble, spiritual impatient unimaginative proud & lack of humility materialistic practical CALL FOR ABSTRACTS ResNet The UQMS Research Network is now seeking abstracts from medical students for inclusion in future issues of ResNet. Abstracts can be in either of the categories of original research or evidence based medicine. While this particularly suits Honours, Masters and Doctorate research students in the School of Medicine, submissions from students without a research background are strongly encouraged. There is no deadline for abstracts submitted to ResNet. Acceptance for publication will be subject to peerreview process. THE UQMS RESEARCH NETWORK AWARDS UQMSResearch ResNet Category This award is given annually for the best article submitted to ResNet, in either the EBM or original research abstract category. Each article submitted will be judged by a panel for its scientific content, writing style and potential impact. Colloquium Category This award is given for the best oral presentation at the UQMS Research Colloquium. Each presentation is judged for its scientific content, presntation style and accompanying abstract. GUIDELINES FOR AUTHORS 1. Abstracts should be no more than 250 words, and include the following headings (in bold): Background; Aims; Methods; Results; Conclusion. Abstracts outlining a proposed research project will not have a results section. 2. Title should be no more than 20 words. Colloquium 2009 The 2009 UQMS Research Colloquium will be held on the evening of September 30. We are now seeking original research abstracts for either oral or poster presentations. Submissions may be made by any MBBS, MPhil or PhD student within the School of Medicine. The deadline for colloquium abstracts for 2009 is midnight on August 31. Please also indicate whether you would prefer to make an oral or poster presentation. Oral presentations 3. Authors and affiliations must be included beneath the title. 4. Abstracts should use scientific or generic names for products where possible. 5. Any research on human subjects must 15 minutes will be allowed for oral presentations, with 5 minutes for questions. Presentations must be accompanied by powerpoint slides. have been approved by the relevant local Poster presentations the abstract to be reproduced in ResNet. Posters must be no larger than A0 size (841mm x 1189mm). To submit to either ResNet Magazine or the research colloquium, email your abstract as an attachment (word file or rich-text format) with the subject header ‘UQMS Abstract’. Please also include a brief bio paragraph and photo for inclusion with your abstract. institutional ethics committee. 6. Submission of abstract signifies that the author(s) have given permission for Email: m.tuppin@uq.edu.au EBM Corner Visual Loss in Giant Cell Arteritis Background: An elderly male, aged 72, who presented with sudden onset of visual loss in his right eye due to giant cell arteritis (GCA). This raises two immediate point-of-care questions: firstly, what treatment should be initiated; and secondly, what is the prognosis for the sight in his right eye? Clinical Questions: Using the PICO format, these questions could be posed as: 1. In a patient presenting with GCA and visual loss (patient), what are the current treatment guidelines (intervention)? 2. In a patient presenting with GCA and visual loss (patient), and who receives treatment (intervention), what is the prognosis for return of vision (outcome)? Search strategy: A search was performed in Medline Ovid using the fields (“giant cell arteritis” OR “superficial temporal arteritis”).ti. AND Expert Commentary In many conditions of inflammatory disease steroids are assumed to be of benefit, but there is not always a sound or large evidence base to support the nature and size of benefit. For example, in Bell’s palsy the benefit from corticosteroids is modest and only if they are commenced early in the course of disease. Due to the serious implications of visual loss following giant cell arteritis it would be ethically difficult to undertake a RCT without providing steroids to the control group. However, the extant trials are mostly small in size and many are case series rather than prospective cohort studies. Of the first 3 studies chosen to answer the (“amaurosis fugax” OR “vis* loss”).af. AND treatment.af, yielding 70 results. A quick scan of the titles of the first few indicated four articles that were directly relevant – three review articles of giant cell arteritis and its treatment, 1,2,3 and one prognostic study of outcome in patients with visual loss due to GCA.4 nisolone daily for 3 days, followed by oral prednisone. Patients with visual loss from GCA. Unfortunately, visual deterioration still occurred in 27% of eyes within the first week despite corticosteroid treatment, and only 5% had an improvement in both visual acuity and visual field. Results: Based on this point-of-care application of EBM, we concluded that it would be reasonable to admit this patient for intravenous administration of 1g methylprednisolone for three days, followed by a slowly tapering oral prednisolone dose commencing at 60mg. We are also able to commence him on low-dose aspirin as an adjunct to treatment that may help to preserve sight in his other eye. A brief look at the abstracts for the three treatment review articles 1,2,3 gives us a good guide to treatment. Unfortunately, we note that there are no randomized controlled trials specifically looking at CGA patients with ocular complications and comparing treatment modalities. However, all three reviews seem to agree that patients should be admitted to hospital for high-dose intravenous methylprednisolone. Additionally, two articles mention a retrospective study concluding that aspirin appears to decrease the likelihood of stroke or visual loss in GCA, without increasing the complication of bleeding. Other treatments (methotrexate and anti-TNF-a agents) are being trialed but have not yet had their efficacy demonstrated. Application: References: 1. Fraser J, Weyand C, Newman N & Biousse V. The treatment of giant cell arteritis. Reviews in Neurological Diseases (2008); 5(3): 140-52. 2. Hall J. Giant-cell arteritis. Current Opinion in Ophthalmology (2008); 19: 454-460. 3. Wang X, Hu Z & Lu W et al. Giant cell arteritis. Rheumatology International (2008); 29:1-7. The final prognostic study4 was a prospective evaluation of 34 consecutive patients with biopsy proven GCA and visual loss (mean visual acuity was 20/400). All patients were treated with a standard protocol of 1 g intravenous methylpred- 4. Danesh-Meyer H, Savino P & Gamble G. Poor prognosis of visual outcome after visual loss from giant cell arteritis. Ophthalmology (2005); 112(6):1098-103. above clinical question, the second and third are academic reviews rather than systematic reviews, so important studies could potentially have been overlooked. I note that all 3 reviews are dated 2008 – beware rejecting older studies which may actually be of better quality. I fairly quickly located 2 other studies (Hayreh, 2002; Chevalet, 2000) that both found no difference in outcomes at one year between oral and intravenous steroids, although Hayreh, et al. looked at visual recovery rather than prevention. equivocal that IV steroids are better than oral delivery, and due to the inherent dangers of hospitalization, I would prefer to manage such a patient as an outpatient with regular review. A summary of the evidence supports these points. Early treatment probably prevents some visual loss, though we have no evidence for the relative or absolute risk reduction. Once visual loss occurs, there is a very small recovery rate even with steroid treatment. It is 2. Hayreh S, Zimmerman B, Kardon (2002) R. Visual improvement with corticosteroid therapy in giant cell arteritis. Report of a large study and review of literature. Acta Ophthalmol Scand 80(4):355-67 References: 1. Chevalet P, Barrier J. et al (2000) A randomized, multicenter, controlled trial using intravenous pulses of methylprednisolone in the initial treatment of simple forms of giant cell arteritis: a one year followup study of 164 patients. J Rheumatol. Jun;27(6):1484-91 Dr David King ORIGINAL ABSTRACT Fiona Simpson BSc, MBBS candidate A Comparison Of Middle Ear Disease In Indigenous Children In Urban And Rural Communities Simpson F1, Spurling G1,2, Hayman N2 1 University of Queensland 2 Inala Indigenous Health Background: Australian Indigenous children have higher rates of middle ear disease than have been described in any other population in the world. While it is well documented that prevalence is highest in remote communities, there is little research into indigenous children living in an urban environment. Aims: The primary aim of this study is to investigate whether Indigenous children living in an urban environment have similarly high rates of middle ear disease and exposure to risk factors compared to Indigenous children living in a rural environment. Secondary aims of the study include a comparison of severity, as measured by perforation rates; differences in referral rates; and variations in management. Methods: Data was collected opportunistically by administering a Child Health Check to approximately 250 children aged between 0 and 15 yrs who attended the Inala Indigenous Health service between March 2007 and December 2008. This information will be compared to that obtained from Child Heath Checks that were undertaken as part of the Northern Territory Emergency Response Child Health Checks Initiative. This information is available on the Australian Institute of Health and Welfare website. THE UNIVERSITY OF QUEENSLAND CENTRE FOR CLINICAL RESEARCH only translating high quality medical research directly to the patient, but also providing a ready avenue for clinicians to investigate research questions arising from patient care. This joint “bench to bedside” and “bedside to bench” focus, addresses a critical area of unmet need in the early 21st century, not Fiona Simpson completed a Bachelor of Science majoring in Biomedical Science at UQ in 2006, and is currently in 3rd year medicine. Her honours research project is under the supervision of Dr G Spurling. Conclusions: The results of this research will improve our understanding of the difference in health in indigenous Profile Piece The University of Queensland Centre for Clinical Research (UQCCR) is a new Faculty of Health Sciences centre pivotally located on the Herston campus, alongside Australia’s largest teaching hospital. UQCCR’s mission is to embed clinical research at the interface between the laboratory and the patient bedside, by fostering innovation in clinical research, and translating basic and applied research into more effective outcomes for patients. children in urban and rural communities. It is essential that health care practices and health interventions are appropriate for the target community, therefore an understanding of whether the same factors influence health in Indigenous children, regardless of location, is necessary. This information can provide a basis for improvements in clinical practice and for wider health interventions in the community that aim to improve the health status of Indigenous children. Our research is organised along four primary themes: Molecular and Cellular Pathology, Clinical Neuroscience, Tissue Inflammation and Injury Repair, and Clinical Outcomes and Clinical Trials. Work in stem cell research and perinatal medicine link these areas as central cross-cutting themes. Molecular and Cellular Pathology Research investigating breast, prostate, oral and skin cancer will develop a better understanding of the links between pathological changes at the molecular and cellular level and the clinical expression of the disease seen at the bedside. Research groups led by Professor Sunil Lakhani, Professor Martin Lavin, Professor ‘Frank’ Gardiner and A/Prof Camile Farah are paving the way for development of novel or improved diagnostic technologies, and better methods of treatment. Tissue Inflammation and Injury Repair Inflammation is a fundamental part of many diseases and a prime target for therapeutic interventions. Professor Nicholas Fisk, Professor David Paterson and A/Professor Kiarash Khosrotehrani’s tissue inflammation and injury repair research program links basic research on inflammation and repair with new approaches to treating inflammation and promoting repair. This research includes a focus on a range of injuries such as infection, burns, fractures and arthritis, as well as damage caused by genetic and autoimmune diseases. BOOK REVIEW • Brain development/injury/rescue • Signal Processing • Fetal Movement • Gene expression in the brain in pregnancy in rats Introdution To Research In The Health Sciences. 5th edition. • Immune responses in human stroke Polgar S & Thomas S • Genetic factors predisposing to human inflammatory neuropathy Clinical Neuroscience This program works on developing and evaluating new modes of diagnosis and treatment of brain disorders, particularly dementia, stroke, movement disorders, and brain injury in adults and babies. Research includes the areas of neuroimmunology, neuropharmacology, neuroimaging and neuroprotection. Research groups are led by Professor David Pow, Dr Judith Greer, A/ Professor Pamela McCombe, Professor Paul Colditz, Dr David Copland, A/Professor Stephen Rose and Professor Peter Silburn. Clinical Outcomes and Clinical Trials Clinical trials are intrinsic to our mission of delivering the benefits of new medical research to patients. UQCCR’s location alongside one of Australia’s largest hospitals optimises opportunities to conduct intensive investigation of how patients respond to new treatments and modes of diagnosis. The Centre will grow clinical trials research particularly focusing on ambulatory Phase Two – Early Phase Three trials and develop new databases to monitor health outcomes. Potential RHD projects UQCCR is committed to training translational researchers and clinical scientists and a number of projects for PhD studies are offered on the following topics. • Pharmacotherapy for aphasia • Mapping the neural mechanisms of language treatment in aphasia • Neurophysiological markers of language recovery in acute stroke • Influence of deep brain stimulation on language in Parkinson’s disease • Potential language markers of depression and dementia in Parkinson’s disease • ERP indices of developmental reading and language disorders and treatment • Perinatal Research • Rate of loss of motor neurones in the SOD1 model of ALS • Generation of new cortical atlases based on functional connectivity information acquired using MR diffusion tractography. • Investigating the relationship between white matter lesion (WML) load, cortical atrophy and aging. • Development of novel methods to quantitatively measure white matter injury and endogenous reorganisation / recovery mechanisms associated with stroke and hypoxic injury in neonates. • Development of novel MRI markers of early treatment response in patients with brain tumours. • Investigating novel fMRI and MR diffusion tractography technology to improve neurosurgical planning for patients with brain tumours. • Cancer association with reduced fetal stem cell microchimerism • Fetal stem cell transplantation • Maximising homing and engraftment of stem cells for bone repair • Development of novel segmentation and cortical mantle extraction techniques for the neonate brain. Our UQCCR Research staff and academics are happy to advise or offer any further information. Visit our website for contact details www.uqccr.uq.edu.au or phone the centre on 07 3346 6555. Professor Nicholas Fisk Description According to the publisher Elsevier, the fifth edition of An Introduction to Research in the Health Sciences has two overall aims. 1) To introduce the fundamental principles of research methodology and explain how these principles are applied for conducting research in the health sciences. 2) To demonstrate how evidence produced through research is applied to solving problems in everday health care. Review This introductory text is great for anyone contemplating research within health sciences and doesn’t quite know how to go about it. The book is divided into 7 key sections that effectively outline the research process from start to finish: • The scientific method • Research planning • Research designs • Data collection • Descriptive statistics • Inferential statistics • Dissemination and critical evaluation of research Throughout the text, the emphasis on writing is placed firmly on the application of key concepts to research. This is in contrast to some other texts that get caught up in providing too much detail on the statistical analysis and not enough on designing the research project. The result is a book that delivers what it primarily set out to achieve – an introduction to research. The key strength of this book is that it effectively discusses the entire research process in a minimum of pages, allowing it to be read in a very short period of time. There is also some discussion of basic descriptive statistics for those who have not studied this at a tertiary level. Those who have might also find it a useful and succinct summary of some of the main concepts. Finally, there is some brief discussion of choosing the appropriate statistical test for analyzing data. Again, this would be most useful for people who have not studied more advanced tests at a tertiary level, or for those who are only likely to be using simple tests in their research project. An interesting feature of this book is the inclusion of qualitative research methodologies in research in health sciences. There has also been some attempt at integrating this into the wider research framework of using combined methodologies to approach a research problem. However, as the emphasis of the text is still firmly biased towards quantitative research, the main use of this discussion would be to get budding researchers to at least think about qualitative methodologies in their research. It would certainly be nice to see further development of the qualitative paradigms in future editions of the text. Strengths: • Well written, easy to read and understand in a short period of time • Good, simple introduction to the use of statistical analysis in research • Introduces the concept of pragmatism – the combined use of qualitative and quantitative methodologies in solving problems • Includes a chapter on qualitative research in health sciences • Discusses how to critically evaluate the literature, and introduces systematic reviews and meta-analyses • Inclusion of questions and answers at the end of each chapter to allow the reader to test their understanding of the key concepts presented Weaknesses: • Does not discuss more advanced statistical techniques such as survival analysis and logistic regression • Sections discussing qualitative research could be further developed Conclusion: This book provides an extremely useful starting point for any student or clinician without a solid grounding in the research process and who is about to enter into a research project. It would particularly suit any student who is contemplating pursuing an honours project as part of their medical degree. Bibliographic Details Paperback, 344 pages Publication date: NOV-2007 ISBN-13: 978-0-443-07429-5 Imprint: CHURCHILL LIVINGSTONE, ELSEVIER The Last Word Qualitative Research in EBM The use of qualitative data in the practice of evidence based medicine presents a number of issues, such as its scientific validity as well as its practical reliability in being able to predict how patients will respond in a clinical or other settings. Indeed, as data, they represent what and how people think, usually as a process, not necessarily as a simple response to a stimulus at one point in time, the way EBM’s quantitative data sets measure, under particular conditions (symptoms and diseases), the body’s response to an intervening stimulus (treatment) of some kind. Qualitative data, whether elicited from a sociologist’s semi-structured interviews with people or from ethnographic research where an anthropologist, embedded in an isolated community for a year or more, describes everything seen, heard, felt, tasted or smelled as data, are concerned with people’s expressive lives. They are a kind of data that, even in the social sciences, sometimes has a difficult time defending their usefulness. Not because they aren’t useful. But such a defence is usually against those who do not appreciate the difference between explanation of peoples’ behaviours as distinct from understanding their behaviours and their perceptions of others’ behaviours as something that has a particular meaning to them, a meaning probably quite different from the meaning you or I would attribute to it. EBM libraries now have a growing set of qualitative studies that are ranked in value according to some very well developed principles that even social scientists could do well to adopt. However, I am not sure that ranking them according to some type of qualitative validity or any such other ill-conceived and misleading term, is all that useful. This is because, concerned as qualitative data collection methods usually are with people’s expressive lives, they are continually picking up unpredictable directions in which people’s eternally Dr Mark Schubert PhD Dr Mark Schubert is a lecturer with the School of Population Health. He holds a PhD in the field of anthropology at the University of Queensland in 2008. creative awareness can send people’s responses and behaviours. A qualitative study, based on observation and semistructured interviews, of how terminally ill patients’ relatives respond to such news in one setting may reliably predict how such relatives will respond in another; but, there again, it may not. This is not because the qualitative method and its resulting data are no good, but simply because human beings are eternally, creatively aware and unpredictable, including medical practitioners. The power of creative awareness is not just in its making of unpredictable behaviour. All you have to is read Viktor Frankl’s account of survival in concentration camps, not being a result of better food or health care, but whether or not people actually even had a vision of their lives after liberation; a vision out of creative awareness. Even an anthropologist, who has read every other study of a village or region that will be their next focus of study, can find themselves quite naked and clueless once the village of study is reached. I once went on a project armed with an idea based on what I understood was happening in a region and also with all the relevant studies under my belt; but then, after one day in the location, realised the people into whose lives I had moved were not concerned with what I thought they had been at all. The study changed completely. Then there is that other factor in every social process – you. You do not stand outside the creative awarenesses of those with whose issues you deal and diseases you treat; you are a part of their very responses to these, just as in social science research activities, the very presence of a researcher can have an effect on the very people under study in a manner analogical to what the observer effect or Heisenberg uncertainty principle attempts to describe. For confirmation of this, why not take a look at Robert Rosenthal’s studies of the effect of teachers’, psychologists’, medical practitioners’ and other interveners’ attitudes and conduct and communication modes on the outcomes for students, clients, patients and others whose lives are being helped. This does not mean that qualitative studies in EBM collections should not be consulted. They should. However, like any field anthropologist, you must be aware that any patient consultation episode can be as exploratory as the anthropologist’s field work; and, if the best advice I can give to anthropologists is to listen, listen, listen …… be quiet and without resistance, give the people you seek to portray your own agency as a human being, so that you can stand-under them, then such advice is as important to you as future medical practitioners. Why? ……….as medical practitioners you will listen to and have interaction daily with more people over your careers than most anthropologists ever will. Research Classifieds Journal Club Clubs & groups Want to keep up with the literature? Interested in forming a journal club in your local clinical school? Just email your details along with your preferred location and special interest group (eg surgery, medicine, paediatrics) to the UQMS Research Network, and we will provide you with the necessary contacts and guides. UQCCR Open Day Events The UQCCR is holding an open day on the 25th September, and is definitely worth checking out. Between 10am-2pm there will be building tours, presentations by group leaders and supervisors, and lunch provided. Registration for catering and a chance to win an iPod is online via: www.uqccr.uq.edu.au Also check the article in this issue outlining potential PhD topics within the UQCCR. Research Assistant Positions Sorry! There are no research assistant positions available at the moment, but please check again in the next issue! Subjects Needed Exercise & the prevention of oesophageal cancer The EPOC study aims to determine if exercise can help prevent the development of oesophageal cancer, and is currently recruiting male subjects with Barrett’s Oesophagus. Goodlife Health Clubs Brisbane in conjunction with UQ Sport are providing free 6 month gym memberships to all participants randomised to the ‘exercise’ group of this study. The EPOC study is also supported by a Queensland Health – Health Practitioners grant. Details: b.winzer@uq.edu.au Attitudes, mood & decision making Individuals for a lab-based study on attitudes, mood and decision-making at St Lucia campus. This research may contain death-related concepts that some may find confronting. Details: clinton.knight@uqconnect.edu.au Tennis Elbow People who have experienced tennis elbow pain for at least six weeks. Details: tenniselbow@uq.edu.au or ext. 54692 Chronic neck pain Males/females (18-45 years) with chronic neck pain to undertake one supervised exercise session and undergo a MRI exam of their neck. There is no cost to the participant and no side-effects from the MRI. The study will be at The Wesley Hospital. Volunteers reimbursed for participation. Details:Dr James Elliott; 3365 4529 (Office). Type 2 Diabetes People with Type 2 diabetics but not achieving adequate blood sugars control on least 1.5g/day metformin (Diabex, Diaformin) only and close to needing insulin. Trial of new additional therapy which promotes weight loss and may help control blood sugars before Insulin is needed. Details: d.colquhoun@uq.edu.au or Lara Petelin, 3876 5688. Whiplash Injury People aged 18-65 with current neck pain following whiplash injury incurred during a motor vehicle accident three months to two years ago, to participate in a study investigating the effects of dry-needling, exercise and advice. Each included participant receives $60 towards travel & time for each assessment (five in total over one year). Details: s.valentin@uq.edu.au. Carpal Tunnel Syndrome Patients with carpal tunnel syndrome to participate in a clinical trial evaluating non-surgical interventions. Details: carpaltunnel@uq.edu.au or ext. 54692 Advertising in the ResNet Research Classifieds is free! To advertise here, please contact the ResNet team. m.tuppin@uq.edu.au UQMS Research Network www.uqms.org