Document
advertisement

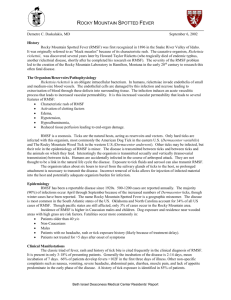
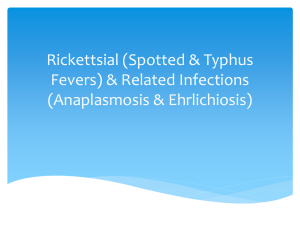
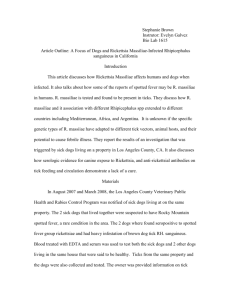
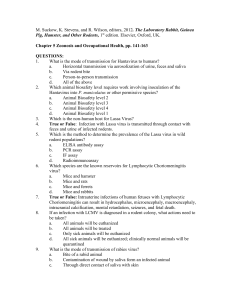
Article #3 CE Canine Rocky Mountain Spotted Fever Rochelle M. Low, DVM Jennifer L. Holm, DVM, DACVECC Angell Animal Medical Center Boston, Massachusetts ABSTRACT: Rocky Mountain spotted fever (RMSF) is an acute, infectious tick-borne disease in dogs. The causative agent of RMSF is Rickettsia rickettsii, a gram-negative bacterium transmitted by ixodid ticks. The most common clinical signs are often nonspecific and include lethargy, anorexia, and fever. Because the primary targets of R. rickettsii are endothelial cells of blood vessels, any organ can be affected, possibly resulting in multiorgan dysfunction. Prompt treatment early in the course of infection may reduce morbidity and mortality associated with RMSF. This article discusses the epidemiology, pathophysiology, diagnosis, and treatment of RMSF in dogs. R ickettsia rickettsii is a gram-negative, obligate intracellular coccobacillus transmitted by hard-bodied ticks that can infect vertebrates, including humans and dogs. Rocky Mountain spotted fever (RMSF) is currently the most common and potentially devastating rickettsial illness in both humans and dogs in the United States. Delayed diagnosis and initiation of treatment have led to a case fatality rate of 2% to 5% in humans.1 The case fatality rate in dogs has not been established, although a recent retrospective study 2 documented a 100% survival rate. However, mortality in one veterinary study was three of five (60%), presumably because of delayed diagnosis and more severe manifestations of disease.3 Greater understanding of the pathophysiology and diagnosis of this disease may enable earlier initiation of therapy and improve prognosis in dogs. Send comments/questions via email editor@CompendiumVet.com or fax 800-556-3288. Visit CompendiumVet.com for full-text articles, CE testing, and CE test answers. COMPENDIUM EPIDEMIOLOGY At least 23 rickettsial species have been described. The Rickettsia genus is divided into four groups: typhus, spotted fever, ehrlichiosis, and bar- 530 tonella.4 Rickettsiae survive in nature by replication in cells of small mammals and arthropods. Rickettsial diseases are important causes of morbidity and mortality worldwide, with an estimated 900 humans afflicted annually in the United States.5 Although RMSF is classified as a reportable disease in humans, the true incidence is believed to be underestimated.6 The primary route of R. rickettsii transmission is tick bites. Transmission requires 5 to 20 hours of tick attachment, making prompt tick removal a priority in preventing RMSF.5 The main tick vector for RMSF in the eastern United States is Dermacentor variabilis, whereas Dermacentor andersonii is the main vector in the western United States and Canada.7,8 Humans and dogs can also become infected through ingestion of an infected tick or direct contamination of a wound by tick feces or secretions from the tick coxial gland. There are no reports of direct transmission between humans and dogs. However, there have been cases of RMSF in humans and dogs living in the same household or geographic area that have been caused by concurrent exposure to infected ticks.9,10 July 2005 Canine Rocky Mountain Spotted Fever CE RMSF occurs in humans and dogs in the United States, Canada, and Central and South America.11,12 The average incubation period of R. rickettsii in both humans and dogs is 1 week, with a reported range of 2 to 14 531 bines with protein S to inactivate factors Va and VIIIa as well as plasminogen activator inhibitor-1 (PAI-1).19 Rickettsial organisms enter endothelial cells through induced phagocytosis. After rickettsial infection, the RMSF in dogs can cause severe vasculitis and a wide range of clinical manifestations, including fever, ocular lesions, neurologic dysfunction, arthropathy, and edema. days. Most cases occur from April through October, coinciding with peak tick activity.11 In the continental United States, RMSF has been diagnosed in every state except Vermont and Alaska. The incidence of RMSF is actually lower in the Rocky Mountains than in other parts of the country. The highest infection rates in dogs are now in the southeastern United States.2,11 PATHOPHYSIOLOGY R. rickettsii infects vascular endothelial cells, initiating diffuse vasculopathy, a severe perivascular inflammatory response, and microvascular thrombosis.13,14 The pathogenesis of R. rickettsii infection is not completely understood; however, a combination of three mechanisms is described in the recent literature. First, the endothelial cell response to injury leads to promotion of a proinflammatory and prothrombotic state. Second, microvascular thrombosis and endothelial injury cause oxidative stress that leads to cell death. Finally, platelet homeostasis is further affected by immune-mediated platelet destruction.15–17 Endothelial Response to Injury The vascular endothelium is critical in protecting against vascular injury, maintaining blood fluidity, and preventing thrombosis.18 Thrombosis is prevented by production of antiplatelet, anticoagulant, and fibrinolytic factors. The role of the endothelium in preventing thrombosis has recently been reviewed.19 Normal endothelial anticoagulant and fibrinolytic properties are achieved by production of thrombomodulin, protein S, heparin sulfate, tissue factor pathway inhibitor, and tissue plasminogen activator. Thrombomodulin binds to thrombin, and this complex activates protein C, which comJuly 2005 COMPENDIUM surface of the endothelial cell undergoes biochemical changes induced by three possible mechanisms20: • • • Enzymatic effects secondary to rickettsial entry Altered synthesis and expression of cell surface components Expression of rickettsial antigens on the cell surface after infection Studies using human cultured endothelial cells have shown that the host endothelial cell not only sustains damage but also actively responds to intracellular damage.21 This active response to infection by endothelial cells involves altering the expression of several proteins that play an important role in the biochemical and pathologic changes in RMSF.13 In addition, endothelial 532 CE Canine Rocky Mountain Spotted Fever PAI-1 Tissue factor A to pop ntia O2 tic NF-κB O2• GSH 2H2O SOD H2O2 H2O + O2 R. rickettsii Platelets Neutrophil – OH• + OH Normal cell Infected cell Endothelial cell Figure 1. Endothelial cells respond to R. rickettsii infection with increased production of inflammatory and procoagulant proteins, increased platelet and neutrophil adhesion, and expression of antiapoptotic proteins. injury has been shown to exacerbate the inflammatory response with neutrophil activation, increased neutrophil–endothelial adhesion, and increased release of proinflammatory cytokines.11,13,21 Specific endothelial cell changes in RMSF include increased surface adhesiveness to platelets and changes in endothelial cell gene expression, leading to increased production of key proinflammatory and procoagulant proteins, such as PAI-1 and tissue factor21 (Figure 1). PAI-1 quickly inhibits conversion of plasminogen to plasmin and thus is a powerful procoagulant protein.22,23 Another protein released by endothelial cells during R. rickettsii infection is the transcription factor nuclear factor–κB (NF-κB). NF-κB activation has a critical role in protecting cells from apoptosis. It has recently been demonstrated that R. rickettsii exerts an antiapoptotic effect on host cells by increasing NF-κB production, thereby protecting itself by ensuring survival of the host cell. This antiapoptotic effect favors a higher tick rickettsemia. In addition to its antiapoptotic effect, NF-κB activation in RMSF plays a critical role in promoting a prothrombotic state by inducing expression of the procoagulant protein tissue factor.24 Oxidative Injury During normal cellular respiration, oxygen is reduced to water. The metabolism of one molecule of oxygen requires four chemical reduction reactions that lead to production of reactive oxygen species (Figure 2). The COMPENDIUM α-Lipoic acid Normal cell 2H2O Figure 2. Two important intracellular enzymes contribute to antioxidant defense: Glutathione peroxidase (GSH) converts peroxide to water, and superoxide dismutase catalase (SOD) converts peroxide to water and oxygen. (• = free radicals) body normally keeps these free radicals under control by producing antioxidants. However, if production of free radicals exceeds the antioxidant defense mechanism, a condition known as oxidative stress occurs. Oxidative stress leading to lipid peroxidation of cell membranes has been implicated as an important mechanism of cellular injury in numerous diseases, including RMSF.15,17,25 Interaction of R. rickettsii with endothelial tissue leads to generation of reactive oxygen species. Intracellular multiplication of R. rickettsii changes the internal morphology of endothelial cells. Architectural changes in the cytoskeleton of infected cells, such as dilation of membranes of the endoplasmic reticulum and outer nuclear membrane, directly affect the host-cell antioxidant defense system.26 The three enzymatic antioxidants important in normal cellular defense against reactive oxygen species are catalase, glutathione peroxidase, and glucose-6-phosphate dehydrogenase. Activity of these three enzymes is significantly reduced in endothelial cells infected with R. rickettsii.25 Decreased levels of these enzymes make infected endothelial cells vulnerable to oxidative stress. Damage associated with oxidative injury in RMSF is supported by the fact that humans with glucose-6-phosphate dehydrogenase deficiency have a more severe course of infection.27 In addition, experimental studies using cultured human endothelial cells have shown that the level of peroxides (a reactive oxygen species) increases in endothelial cells infected by R. rickettsii.28,29 July 2005 534 CE Canine Rocky Mountain Spotted Fever Figure 3. Anterior uveitis with hyphema in a dog that Figure 4. Hyphema and iris hemorrhage in a dog with tested positive for RMSF. (Courtesy of Dr.William Greentree, Angell Animal Medical Center, Boston, MA) RMSF. (Courtesy of Dr. William Greentree, Angell Animal Medical Center, Boston, MA) Clinical use of exogenous antioxidants and the ability to inhibit down-regulation of endogenous antioxidant enzymes may be critical in ensuring survival of the host cell and ultimately improving the outcome of the disease.26 One study15 recently focused on the antioxidant α-lipoic acid, which is an important constituent of cell membranes. α-Lipoic acid is easily absorbed from the diet and has been proposed as an adjunctive therapy for RMSF. α-Lipoic acid has the capacity to directly bind reactive oxygen species and decrease NF-κB activation.15 role, the presence of elevated platelet-associated IgG titers in sera of infected dogs suggests that antibody coating of platelets is occurring.30 Detection of patients with an immune-mediated component causing platelet destruction in RMSF is important because additional immunosuppressive therapy may be required, especially in the early stages. Immune-Mediated Platelet Destruction Thrombocytopenia is the most consistent (reported in up to 80% of dogs) laboratory finding in canine rickettsial disease.2,30 The mechanism of this rickettsial-induced thrombocytopenia varies with rickettsial species. Historically, thrombocytopenia induced by RMSF has mainly been attributed to increased platelet use secondary to vasculitis.2,30 Essentially, damage to the vascular endothelium exposes subendothelial collagen, leading to increased platelet adhesion and aggregation as well as decreased systemic circulation of platelets. Recently, elevated platelet-associated IgG titers were demonstrated in dogs with both experimentally induced and naturally occurring RMSF, suggesting the possibility of immune-mediated platelet destruction in addition to increased use.30 Although an immune component to thrombocytopenia associated with RMSF likely plays only a secondary COMPENDIUM DIAGNOSIS Preliminary diagnosis of RMSF is based on clinical and laboratory findings. Because the clinical and laboratory changes are often vague and nonspecific, a broad differential diagnosis must be considered. Important diagnostic differentials include other tick-borne diseases, immune-mediated thrombocytopenia, systemic lupus erythematosus, sepsis, and neoplasia.5 Clinical Signs In a recent retrospective report 2 of 30 dogs with RMSF, the most common clinical signs were lethargy, anorexia, fever, ocular abnormalities, weight loss, lymphadenomegaly, and edema. Less common clinical signs included arthropathy, cutaneous necrosis, petechiae/ ecchymoses, and myalgia. Dogs with IgM antibody titers of 1:1024 or greater at presentation were more likely to have neurologic dysfunction and skin lesions.2 Ocular manifestations in RMSF occur secondary to vasculitis and are considered useful in the diagnostic July 2005 Canine Rocky Mountain Spotted Fever CE 535 evaluation. Davidson et al31 reported that nine of 11 consecutive dogs with RMSF had ocular involvement. Ocular findings were bilateral in eight of nine dogs and included conjunctival vascular injection (nine dogs), multifocal retinal hemorrhages (seven dogs), anterior uveitis (six dogs; Figure 3), petechial hemorrhages in the iris stroma (two dogs; Figure 4), and bilateral hyphema (one dog). Ocular hemorrhages are the most common ophthalmic sign of RMSF.32 With appropriate treatment, most ocular signs resolved within 2 to 5 days.31 Although the most common cutaneous lesions in RMSF are edema (Figure 5) as well as petechial and ecchymotic hemorrhages, severe dermal necrosis has been reported in four dogs with RMSF. Dermal necrosis occurred in regions in which edema and hemorrhage were most severe, such as the scrotum, pinnae, and limbs.33 Laboratory Findings Laboratory findings in patients with RMSF vary and are nonspecific. Thrombocyte numbers typically drop rapidly but may be normal early in the course of disease.11 In a retrospective study of 30 canine RMSF cases, Gasser et al2 found that 26 of 30 (85%) dogs were thrombocytopenic at initial presentation. Other laboratory abnormalities include increased liver enzymes, azotemia, coagulation abnormalities, leukocytosis, anemia, hypoal- Figure 5. Vasculitis causing severe peripheral edema in a dog with RMSF. RMSF.11,32 Diagnosis can also be demonstrated by a fourfold or greater rise in IgG titer between the acuteand convalescent-phase specimens. These two samples are normally taken 3 to 4 weeks apart.34–36 A positive polymerase chain reaction test for R. rickettsii or a posi- Initial diagnosis of RMSF is based on clinical and laboratory findings and is confirmed with a fourfold rise in acute to convalescent titer to R. rickettsii or a single IgM titer greater than 1:64 at least 7 days after the onset of clinical signs. buminemia, hypercholesterolemia, hyponatremia, and lymphocytic pleocytosis in cerebrospinal fluid.3 Immunofluorescent antibody (IFA) titer is considered the gold standard in diagnosing RMSF. This test is useful in confirming the clinical diagnosis because antibodies to R. rickettsii are rarely detected during the first 7 days of illness.32 The IFA titer can detect IgM and IgG antibodies to R. rickettsii. IgG levels take 2 to 3 weeks to rise after infection and may not decline for 3 to 5 months, whereas the IgM titer usually increases before the IgG titer and declines 6 to 8 weeks after infection. Thus a single IFA titer of 64 or more for IgM, with appropriate clinical signs, is considered diagnostic of July 2005 tive immunofluorescence result from a skin biopsy is also considered diagnostic, but these results are neither timely nor practical in most clinical settings.36 TREATMENT The primary therapeutic goals for RMSF include early, appropriate antibiotic therapy and supportive care, such as intravenous fluids, to prevent organ dysfunction. In addition, adjunct treatments such as corticosteroids, anticoagulants, and antioxidants can be considered. Early antibiotic administration may prevent development of severe thrombosis and dermal lesions as well as ultimately improve the outcome.11,16,32 COMPENDIUM 536 CE Canine Rocky Mountain Spotted Fever Antibiotics proven to be effective against experimental R. rickettsii infection in dogs include tetracycline and its semisynthetic derivative doxycycline, certain fluoroquinolones (i.e., enrofloxacin, trovafloxacin), and chloramphenicol.37–39 In these experimental studies, therapy for 7 days was shown to be sufficient. Doxycycline is the drug of choice in dogs because treating ehrlichiosis (i.e., another rickettsial infection with similar clinical signs) with fluoroquinolones has proven ineffective.40 Although doxycycline is considered less likely to cause dis- promising results in its ability to directly bind reactive oxygen species and protect cell membranes.15 Preventing tick-borne disease in dogs is extremely important.11,36 No vaccines are currently available for administration in dogs. The only effective means of preventing RMSF are avoidance of tick bites and prompt removal of attached ticks.34 Suggested preventive measures include avoiding tick-infested areas between April and October, wearing protective clothing, applying appropriate insect repellants to both humans and pets, Although RMSF is not directly transmitted from animals to humans, dogs can harbor the organism and may increase the chance of human exposure. coloration of teeth than is tetracycline, some authors advocate administering chloramphenicol in young animals to avoid this potential problem.38,39 Administering antiinflammatory or immunosuppressive corticosteroid therapy is controversial, especially in cases with ocular involvement and hematologic abnormalities such as anemia and thrombocytopenia. It is recommended that ocular lesions involving the posterior segment (i.e., chorioretinitis, retinal hemorrhage/ detachment) should be treated with systemic steroids, whereas topical steroids should be used to treat anterior uveitis or hyphema. 31 Because immune-mediated destruction of platelets is likely a component in thrombocytopenia associated with RMSF and a primary diagnostic differential in many cases, immunosuppressive therapy may be warranted.32,41 An experimental study41 in dogs showed that concurrent use of prednisone at antiinflammatory or immunosuppressive doses along with doxycycline did not worsen the severity of R. rickettsii infection. However, the authors of this study caution against extrapolating these results to dogs with severe RMSF because the experimentally induced disease was considered mild to moderate in severity.41 Other treatments proposed in humans with RMSF include use of anticoagulants and antioxidants, but information is limited. If diffuse evidence of microthrombi is suspected clinically, mini doses of heparin have been advocated by some authors.42,43 Clinical administration of antioxidants in patients with RMSF to limit free radical damage is currently an active area of study. As mentioned earlier, α-lipoic acid has shown COMPENDIUM checking animals and children daily for attached ticks if in endemic areas, removing garden refuse, keeping lawns mowed, avoiding tall grass, and promptly removing attached ticks.11,37,44 We refer readers to a recent review45 of tick repellants and more detailed information on preventing tick-borne disease. CONCLUSION RMSF is the most common rickettsial disease in dogs in the United States. Damage to the vascular endothelium, oxidative injury, and immune-mediated platelet destruction are all believed to contribute to the pathophysiology of RMSF. Common clinical signs include lethargy, anorexia, fever, ocular abnormalities, lymphadenomegaly, and edema. Tentative diagnosis is based on clinical signs and history, whereas a definitive diagnosis is obtained via IFA titer. A single IgM titer greater than 1:64 or a fourfold rise in acute to convalescent IgG titer confirms a diagnosis of RMSF. Treatment recommendations include appropriate antibiotic therapy and supportive care to prevent multiorgan dysfunction. Adjunct treatments to consider include anticoagulant, antioxidant, and/or immunosuppressive therapy. The prognosis is good if patients are treated early in the course of the disease. REFERENCES 1. Paddock CD, Holman RC, Krebs JW, et al: Assessing the magnitude of fatal Rocky Mountain spotted fever in the United States: Comparison of two national data sources. Am J Trop Med Hygiene 67(4):349–354, 2002. 2. Gasser AM, Birkenheuer AJ, Breitschwerdt EB: Canine Rocky Mountain spotted fever: A retrospective study of 30 cases. JAAHA 37:41–48, 2001. July 2005 Canine Rocky Mountain Spotted Fever CE 537 3. Rutgers C, Kowalski J, Cole CR, et al: Severe Rocky Mountain spotted fever in five dogs. JAVMA 21:361–369, 1985. Rickettsia rickettsii–induced transcriptional activation of the host endothelial cell. Infect Immunol 67(12):6418–6423, 1999. 4. Brouqui P: Tropical animal and human rickettsial infections. Med Trop 57(3 suppl):23–27, 1997. 25. Devamanoharan PS, Santucci LA, Hong J, et al: Infection of human endothelial cells by Rickettsia rickettsii causes a significant reduction in the levels of key enzymes involved in protection against oxidative injury. Infect Immunol 62(6):2619–2621, 1994. 5. Thorner AR: Rocky Mountain spotted fever. State of the art clinical article. Clin infect Dis 27:1353–1360, 1998. 6. Talan DA, Moran GJ: Update on emerging infections: News from the CDC. Ann Emerg Med 32(5):537–539, 2000. 7. Hinrichsen VL, Whitworth UG, Breitschwerdt EB, et al: Assessing the association between the geographic distribution of deer ticks and seropositivity rates to various tick-transmitted disease organisms in dogs. JAVMA 218(7): 1092–1097, 2001. 8. Walker DH: Tick-transmitted infectious disease in the United States. Annu Rev Pub Health 19:237–269, 1998. 9. Jones TF, Allen SC, Paddock CD, et al: Family cluster of Rocky Mountain spotted fever. Clin Infect Dis 28:853–859, 1999. 10. Paddock CD, Brenner O, Vaid C, et al: Short report: Concurrent Rocky Mountain spotted fever in a dog and its owner. Am J Trop Med Hyg 66(2): 197–199, 2002. 11. Sexton DJ, Kaye KS: Rocky Mountain spotted fever. Med Clin North Am 86(2):351–360, 2002. 12. Heymann WR: Rickettsial diseases of the skin. Clin Dermatol 14:237–242, 1996. 13. Shi R, Simpson-Haidaris J, Lerner NB, et al: Transcriptional regulation of endothelial cell tissue factor expression during Rickettsia rickettsii infection: Involvement of the transcription factor NF-κB. Infect Immunol 1070–1075, 1998. 14. Kwitkowski VE: Infectious disease emergencies in primary care. Lippincott’s Primary Care Pract 3(1):108–125, 1999. 15. Eremeeva MA, Silverman DJ: Effects of the antioxidant α-lipoic acid on human umbilical vein endothelial cells infected with Rickettsia rickettsii. Infect Immunol 2290–2299, 1998. 16. Walker DH: Rocky Mountain spotted fever: A seasonal alert. Clin Infect Dis 20:1111–1117, 1995. 17. Silverman DJ, Santucci LA: Potential for free radical–induced lipid peroxidation as a cause of endothelial cell injury in Rocky Mountain spotted fever. Infect Immunol 56(12):3110–3115, 1988. 18. Bombeli T, Karsan A, Tait JF, et al: Apoptotic vascular endothelial cells become procoagulant. Blood 89(7):2429–2442, 1997. 19. Good LI, Manning AM: Thromboembolic disease: Physiology of hemostasis and pathophysiology of thrombosis. Compend Contin Educ Pract Vet 25(9): 650–659, 2003. 20. Elghetany MT, Walker DH: Hemostatic changes in Rocky Mountain spotted fever and Mediterranean spotted fever. Am J Clin Pathol 112:159–168, 1999. 21. Clifton DR, Goss RA, van Antwerp D, et al: NF-κB–dependent inhibition of apoptosis is essential for host cell survival during Rickettsia rickettsii infection. Proc Natl Acad Sci 95:4646–4651, 1998. 22. Shi RJ, Simpson-Haidaris PJ, Marder VJ, et al: Increased expression of plasminogen activator inhibitor-1 in R. ricketsii–infected endothelial cells. Thromb Haemost 75(4):600–606, 1996. 23. Drancourt M, Alessi M, Levy P-Y, et al: Secretion of tissue-type plasminogen activator and plasminogen activator inhibitor by Rickettsia conorii– and Rickettsia rickettsii–infected cultured endothelial cells. Infect Immunol 58(8):2459–2463, 1990. 24. Sahni SK, Turpin LC, Brown T, et al: Involvement of protein kinase C in July 2005 26. Rydkina E, Sahni A, Silverman DJ, et al: Rickettsia rickettsii infection of cultured human endothelial cells induces heme oxygenase 1 expression. Infect Immunol 70(8):4045–4052, 2002. 27. Abuhammour W, Salman R: Rocky Mountain spotted fever from pediatrics/ infectious diseases. Emerg Med J 2(10), 2001. 28. Eremeeva ME, Silverman DJ: Rickettsia rickettsii infection of the EA.hy 926 endothelial cell line: Morphological response to infection and evidence for oxidative injury. Microbiology 144:2037–2048, 1998. 29. Hong JE, Santucci LA, Tian X, et al: Superoxide dismutase-dependent, catalase-sensitive peroxides in human endothelial cells infected by Rickettsia rickettsii. Infect Immunol 66(4):1293–1298, 1998. 30. Grindem CB, Breitschwerdt EB, Perkins PC, et al: Platelet-associated immunoglobulin (antiplatelet antibody) in canine Rocky Mountain spotted fever and ehrlichiosis. JAAHA 35:56–61, 1999. 31. Davidson MG, Breitschwerdt EB, Nasisse MP, et al: Ocular manifestations of RMSF in dogs. JAVMA 194(6):777–781, 1998. 32. Stiles J: Canine rickettsial infections. Vet Clin North Am Small Anim Pract 30(5):1144–1148, 2000. 33. Weiser IB, Greene CE: Dermal necrosis associated with Rocky Mountain spotted fever in four dogs. JAVMA 195(12):1756–1758, 1989. 34. Buckingham SC: Rocky Mountain spotted fever: A review for the pediatrician. Pediatr Ann 31:3, 2002. 35. La Scola B, Raoult D: Laboratory diagnosis of rickettsioses: Current approaches to diagnosis of old and new rickettsial diseases. J Clin Microbiol 35(11):2715–2722, 1997. 36. Warner RD, Marsh WW: Rocky Mountain spotted fever. JAVMA 221(10): 1413–1417, 2002. 37. Rolain JM, Maurin M, Raoult D: In vitro susceptibilities of 27 rickettsiae to 13 antimicrobials. Antimicrob Agents Chemother 42(7):1537–1541, 1998. 38. Purvis JJ, Edwards MS: Doxycycline use for rickettsial disease in pediatric patients. Pediatr Infect Dis J 19(9):871–874, 2000. 39. Breitschwerdt EB, Papich MG, Hegarty BC, et al: Efficacy of doxycycline, azithromycin or trovafloxacin for treatment of experimental Rocky Mountain spotted fever in dogs. Antimicrob Agents Chemother 43(4):813–821, 1999. 40. Neer TM, Eddlestone SM, Gaunt SD, Corstvet RE: Efficacy of enrofloxacin for the treatment of experimentally induced Ehrlichia canis infection: J Vet Intern Med 13(5):501–504, 1999. 41. Breitschwerdt EB, Davidson MG, Hegarty BC, et al: Prednisolone at antiinflammatory or immunosuppressive dosages in conjunction with doxycycline does not potentiate the severity of R. rickettsii infection in dogs: Antimicrob Agents Chemother 41(1):141–147, 1997. 42. Davi G, Giammarresi C, Vigneri S, et al: Demonstration of Rickettsia conorii–induced coagulative and platelet activation in vivo in patients with MSF. Thromb Haemost 4(2):631–634, 1995. 43. Silverman DJ, Santucci LA, Sekeyova Z: Heparin protects endothelial cells infected by Rickettsia rickettsii. Infect Immunol 59(12):4505–4510, 1991. 44. Wilson ME: Prevention of tick-borne diseases. Med Clin North Am 86(2):219–233, 2002. 45. Kidd L, Breitschwerdt EB: Transmission times and prevention of tick-borne diseases in dogs. Compend Contin Educ Pract Vet 25(10):742–751. COMPENDIUM 538 CE Canine Rocky Mountain Spotted Fever ARTICLE #3 CE TEST This article qualifies for 2 contact hours of continuing education credit from the Auburn University College of Veterinary Medicine. Subscribers may purchase individual CE tests or sign up for our annual CE program. Those who wish to apply this credit to fulfill state relicensure requirements should consult their respective state authorities regarding the applicability of this program. To participate, fill out the test form inserted at the end of this issue or take CE tests online and get real-time scores at CompendiumVet.com. 1. Normal endothelial cell functions do not include a. maintenance of vascular tone. b. transport of nutrients across the endothelium. c. maintenance of a thromboresistant surface. d. secretion of von Willebrand factor. e. secretion of antithrombin. 2. Which statement regarding transcription factor NF-κB is incorrect? a. It is critical in protecting endothelial cells from apoptosis in patients with RMSF. b. It normally resides in the endothelial cell cytoplasm as an active pool. c. It induces the expression of tissue factor in patients infected with R. rickettsii. d. It is a common response of the host cell to a variety of infectious agents. e. none of the above 3. The three enzymatic antioxidants in the body are a. catalase, selenium, and glutathione peroxidase. b. ascorbic acid, selenium, and catalase. c. glucose-6-phosphate dehydrogenase, catalase, and selenium. d. catalase, glutathione peroxidase, and glucose-6-phosphate dehydrogenase. e. ascorbic acid, selenium, and iron. 4. Which statement regarding R. rickettsii is incorrect? a. It is an arthropod-associated bacterium. b. It is a gram-negative obligate intracellular bacterium. c. Its primary targets are endothelial cells of small vessels and lymphocytes. d. It cannot be directly transmitted between animals and humans. e. none of the above 5. The average incubation of R. rickettsii in humans and dogs is a. 14 days. b. 1 to 3 days. c. longer than 30 days. COMPENDIUM CE d. 7 days. e. 12 hours. 6. Endothelial cell changes in patients with RMSF do not include a. increased surface adhesiveness to platelets. b. production of the procoagulant protein PAI-1. c. increased production of tissue factor. d. down-regulation of NF-κB. e. none of the above 7. A single IFA titer of 64 or more for _____, with appropriate clinical signs, is diagnostic of RMSF. a. IgG b. IgA c. IgG or IgA d. IgM e. IFA titers must be higher than 128 to be clinically significant. 8. Which antibiotic has not been proven to be effective in treating RMSF? a. doxycycline b. trovafloxacin c. chloramphenicol d. enrofloxacin e. ampicillin 9. Which of the following is ineffective in preventing tick-borne disease? a. vaccination b. prompt removal of attached ticks c. wearing protective clothing to avoid tick bites d. avoiding tick-infested areas during peak tick season e. none of the above 10. Thrombocytopenia associated with RMSF is not attributed to a. increased platelet use secondary to vasculitis. b. immune-mediated platelet destruction. c. bone marrow suppression. d. a and b e. none of the above Test answers now available at CompendiumVet.com July 2005