Mechanics of Breathing
advertisement

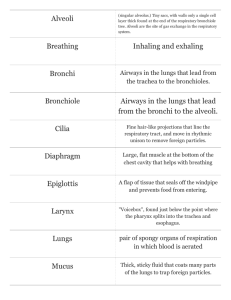
BIOLOGY 12 – RESPIRATORY SYSTEM • RESPIRATION: not just breathing • breathing is just one part of this process • can be divided into 4 areas: Breathing External Respiration Internal Respiration Cellular Respiration the movement of air into and out of the lungs the exchange of O2 and CO2 between the lungs and the BLOOD the exchange of O2 and CO2 between BLOOD and TISSUE FLUID the process which produces ATP in mitochondria --> requires O2 and releases CO2 BREATHING: BRINGING AIR TO THE LUNGS • "INSPIRATION" - breathing air in • "EXPIRATION" - breathing air out 1. Air enters the nasal passages. • Hairs and CILIA trap dust and debris • The air is warmed and moistened. • When we breathe, the GLOTTIS (the opening to the LARYNX ("voice box")) is open, and when we swallow, the EPIGLOTTIS covers the glottis. 3. Air enters the larynx. It is like a triangular box with the Adam's Apple at the front corner. • Elastic ligaments called VOCAL CORDS stretch from the back to the front of the larynx just at the sides of the glottis. Vocal Chord • These cords vibrate when air is expelled past them through the glottis. Glottis This vibrations produce Wide Glottis Narrow Glottis sound. Low Pitch High Pitch 1. 2. 3. 4. 5. 6. 7. 8. 10. 2. The warmed and moistened air passes through the PHARYNX (a common passage for food and air). Respiratory System.doc — Page 1 5. The trachea divides into two BRONCHI, which branch into many smaller passages called bronchioles that extend into the lungs. 6. The bronchioles continue to branch out, and as they do, their walls get thinner and diameter smaller. Each bronchiole ends in sacs called ALVEOLI, which fill up much of the lungs. • There are approximately 300 million alveoli per lung, for a total of 150 m2 of alveolar area (at least Capillary network around alveoli 40 time the area of the skin). • Each alveolar sac is enclosed by a single layer of simple epithelial tissue, which is surrounded by CAPILLARIES carrying deoxygenated blood. GAS EXCHANGE occurs between blood and air in alveoli. • Lungs are enclosed by two pleural membranes. One pleural membrane lines the chest walls, and an inner membrane lines the lung. In between is fluid. This makes for an air-tight seal. INSPIRATION • special ciliated cells at the top recesses of the nasal cavities are scent receptors EXPIRATION Respiratory System.doc — Page 3 4. The air enters the TRACHEA (windpipe). The trachea is held open by cartilaginous rings, and is lined with ciliated mucous membranes. • The cilia beat upward to move up mucus and any dust or particles that were inhaled or accidentally swallowed. Smoking can destroy cilia. • Tracheotomy: an operation in which an incision is made into the trachea below a blockage (and a tube is then inserted). Respiratory System.doc — Page 2 Mechanics of Breathing • What powers breathing? Creating “negative pressure” powers breathing. Negative pressure is EXPIRATION INSPIRATION air pressure that is less (756 mm Hg) than the pressure of the surrounding air (760 mm Hg). This negative pressure is created by increasing the volume inside the thoracic cavity. Air will naturally move in to fill this partial vacuum. The space in the thoracic cavity is made bigger by the CONTRACTION of the diaphragm muscle (this makes it move downward and become less dome shaped). When the diaphragm contracts, the space within lungs increases. • The muscles attached to the ribs, called intercostal muscles, will also CONTRACT when you breathe in. This contraction pulls the ribs up and out, further increasing the space within the thoracic cavity. • The air pressure in the lungs becomes less than the atmospheric pressure. Air naturally rushes into the lungs to fill this natural vacuum. Respiratory System.doc — Page 4 CONTROL OF BREATHING • When the DIAPHRAGM RELAXES, it moves up, and when the INTERCOSTAL MUSCLES RELAX, the ribs move down and inward. This decreases the volume in the thoracic cavity, and air is forced out of the lungs (expiration). • CO2 & H+ IN THE BLOOD control the BREATHING RATE 1. CO2 levels in blood increase as cells continue to produce it - The concentration of CO2 will increase until they reach a threshold level 2. Chemoreceptors in arteries detect the increased CO2 & H+ levels 3. chemoreceptors send a signal to a breathing center in the MEDULLA OBLONGATA of the brain(it detects the rising levels of CO2 and H+, but not affected by low O2 levels) - also chemoreceptors in the carotid bodies(in carotid arteries), and in the aortic bodies(in aorta) that respond primarily to H+ concentration, but also to the level of carbon dioxide and oxygen in the blood(these bodies communicate with respiratory center) 4. medulla oblongata sends a nerve impulse to the diaphragm & muscles in the rib cage 5. diaphragm contracts & lowers, while the rib cage moves up Respiratory System.doc — Page 5 6. air flows into alveoli, & alveolar walls expand & stretch 7. Stretch Receptors in the alveoli walls detect this stretching 8. nerves in alveoli send signal to brain to inhibit the medulla oblongata from sending its message to the diaphragm and rib muscles to contract (they therefore stop contracting) 9. diaphragm relaxes, & moves upward, resuming its original shape -rib cage relaxes & moves downward & inward & air is forced out the lungs • Thus, CO2 levels in blood regulate breathing rate. Therefore, it is better to not give pure oxygen to a patient to get breathing going (should be a mixture of oxygen and carbon dioxide) • Average human breathes in, on average, 500 ml of air per breath (tidal volume) • vital capacity: maximum that can be breathed in per breath (averages about 3000-6000 ml.) Respiratory System.doc — Page 6 • other part of this air is stuck in bronchioles and doesn’t get to the alveoli. ( "Dead Air Space") • residual air: air that remains in lungs after expiration (about 1000 ml) CONDITIONING OF INHALED AIR On its journey into alveoli, the air is: 1. Cleansed of Debris: - nose hairs & mucous in nasal passageways - mucous lining & cilia of trachea and bronchi 2. Adjusted to Body Temperature. - the more contact it has with moist tissues that are 37 C, closer the temperature of the inhaled air gets to 37 C. - by time the air gets to alveoli, it has same temperature as surrounding tissue 3. Adjusted to 100% Humidity: - inhaled air becomes saturated with water • only ~350 cc of the 500 cc normally breathed in actually gets down deep enough to reach the alveoli Respiratory System.doc — Page 7 Respiratory System.doc — Page 8 SPECIALIZATION OF THE ALVEOLI Alveoli are specialized for gas exchange with the blood: 1. very numerous: a great surface area for the diffusion of gases 2. very thin walls: are only one-cell thick which aids in gas diffusion because there is very little resistance 3. have a coating of lipoproteins on their inner surface(SURFACTANT): helps to maintain surface tension thus preventing them from collapsing and sticking together during exhalation 4. supplied with stretch receptors: are nerve endings that are sensitive to stretch 5. kept moist: ensures that gas exchange is possible. If they dried out, efficient diffusion would be impossible 6. have a very rich blood supply from the pulmonary capillaries to ensure maximum gas diffusion EXTERNAL RESPIRATION: • the exchange of gases between the air in the alveoli and the blood in pulmonary capillaries • exchange of gases is by diffusion alone (high concentration to low concentration) capillaries (blood) Alveoli (lung) [O2] low high [CO2] high low • Carbon dioxide is moved in the blood in three forms a) HHb – reduced hemoglobin (H+ ions) b) HbCO2 - carbaminohemoglobin c) HCO3 – - bicarbonate ion • As O2–poor blood enters the arteriole end of the pulmonary capillary, conditions in the lungs that allow the hemoglobin to drop H+ and CO2 and then pick up O2 are a pH of 7.4 and a temperature of 37 C. • CO2 that is dropped off by the hemoglobin (HbCO2) simply diffuses out of the blood and into the alveoli • The HHb drops off the H+ ions which then joins with HCO3- to form H2CO3 (carbonic acid). In order to maintain the pH of the blood this acid can not remain in the blood. The enzyme carbonic anhydrase converts Respiratory System.doc — Page 9 the carbonic acid into CO2 and H2O. These molecules then diffuse out of the blood and into the alveoli • As CO2 is leaving the blood there is room for the hemoglobin to carry oxygen as HbO2 (oxyhemoglobin). This O2 rich blood leaves the capillaries and enters the pulmonary venules (and veins) and heads back to the heart. Respiratory System.doc — Page 10 • The CO2 and H2O enter the capillaries by diffusion. In order to move the CO2 and H2O we must reassemble them. The H2O and CO2 combine to form H2CO3 (carbonic acid) which is then converted into H+ ions and HCO3-. The H+ is picked up by hemoglobin and becomes HHb. The HCO3- stays in the blood and travels in this form. A small percentage of CO2 joins with Hb and travels as HbCO2. These three forms of CO2 leave the capillary bed through the venule end and return to the heart. ⇒ INTERNAL RESPIRATION: • the exchange of O2 and CO2 between BLOOD in the systemic capillaries and TISSUE FLUID. • O2-rich blood enters the arteriole end of a systemic capillary bed. The Hb releases the O2 allowing it to diffuse into the tissues based on the conditions at the cellular level. • The conditions in the systemic capillaries that signal the Hb to drop the O2 and pick up the H+ is a pH of 7.38 and a temperature of 38 C. • The O2 that diffuses in to the tissues is used for cellular respiration. The products of cellular respiration are ATP, CO2, and H2O. The latter two are waste products and must be removed from the cell. Respiratory System.doc — Page 11 Note: Hemoglobin combines with the excess H+ that this reaction produces. That way, blood pH remains constant. You could say that Hemoglobin acts like a buffer. RESPIRATORY DISORDERS 1. Common Cold: Caused by viral infection. About 150 viruses are known to cause colds. • Mild symptoms: sore throat, watery mucusy nasal discharge. • No Cure -- treat symptoms. Antihistamines, decongestants, ASA, rest. 2. Influenza: a more severe viral infection. • Symptoms include fevers, aches, cold symptoms. Vaccines have been developed, but the virus is constantly mutating into new forms. Over 20,000,000 people died in a flu epidemic in 1919-20. Respiratory System.doc — Page 12 3. Bronchitis: usually caused by viral infection of nasal cavities that spreads to bronchi and causes a secondary bacterial infection. • In acute bronchitis, there is heavy mucoid discharge, coughing. • Chronic bronchitis is not usually due to bacterial infection, but rather to chronic irritation of bronchial lining (leads to degeneration of lining, loss of cilia). Chronic bronchitis is usually due to smoking. • Treatment for acute bronchitis is antibiotics and rest. 4. Pneumonia: caused by bacteria or viruses which infect lungs. The lobes of the lungs fill up with mucus and pus. • Many AIDS patients die of Pneumocystis carinii infection. • Treatment is antibiotics (if bacterial), hospitalization. 5. Emphysema: most often caused by smoking. • Deteriorating bronchioles ----> alveoli cut off. This leads to ballooning of lungs due to trapped air. The trapped air causes the alveoli to rupture. • Symptoms include coughing, sluggishness, heart racing. The heart and brain starve for oxygen. May lead to a heart condition. • Hard to treat: often surgical removal of some lung tissue helps. 6. Tuberculosis: caused by tubercle bacteria. Can detect with a skin test, X-Rays. • If the bacilli invade lungs, cells the invaders with capsule called tubercles (a defense mechanism). This may kill sufferer. Respiratory System.doc — Page 13 • Treatment: quarantine, antibiotics, other drugs. 7. Lung Cancer: Smoking is the #1 cause! (see text). • Lung cancer is a progressive disease --> early detection is important. Progress of disease: 1. Lungs exposed to carcinogenic irritants. 2. Bronchial cells thicken, callus, cilia die. 3. "Atypical" cells start appearing in thickened lining ("in situ" cancer). 4. Some of these cells break loose and penetrate other tissues (= metastasis). This is the point where true cancer begins. 5. Tumor(s) grow, tubes become blocked, lung collapses, secondary infections can occur. • Treatment: chemotherapy, surgery, pneumonectomy (remove lung). Smoking Risks (a partial list): • lung cancer • bronchitis/emphysema • larynx cancer • peptic ulcers • bladder cancer • reduced lifespan • pancreas • weak immune system cancer Respiratory System.doc — Page 14