Pharmacology review: Drugs that alter blood coagulation
advertisement

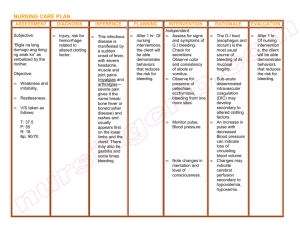
PHARMACOLOGY REVIEW : Drugs that alter blood coagulation Brush up on your knowledge of these potentially life-saving drugs. By Amy M. Karch, RN, MS THE VASCULAR SYSTEM delivers oxygen and nutrients to all body cells and removes waste products from tissues. This closed system functions as a pressure system, with blood flowing continuously from high-pressure to low-pressure areas. Injury of a blood vessel compromises the closed system, causing blood to flow out of the injured vessel (now a low-pressure area). With severe injury to a vessel, the entire circulatory system may be compromised and the patient could die. Blood vessel injuries are common, occurring, for instance, when someone hits the edge of a table, coughs too hard, or falls down. They initiate a series of normal reactions that stops blood flow and maintains balance within the system. The reactions include: • reflex vasoconstriction • platelet aggregation • blood coagulation (clot formation), which causes blood to solidify • clot resolution, which returns blood to the fluid state. In many clinical situations, drugs are used to slow or stop this process, with the goal of preventing tissue damage from the decreased blood flow that occurs when the clotting process cuts off blood supply to an area. This article reviews 26 American Nurse Today the processes the body uses to maintain the cardiovascular system and discusses the mechanisms of action, benefits, and risks of drugs used to alter coagulation. (See Inside the coagulation process.) Indications for drugs that alter coagulation In certain clinical situations—for instance, coronary artery disease, immobility, atrial fibrillation, and joint replacement—interfering with coagulation helps prevent clots that could impede blood flow and cause tissue damage or death. Patients with coronary artery disease, for example, have narrowed vessels. An immobile patient loses the protective massaging of veins caused by muscle fiber contractions; also, CNE: 1.4 contact hours CNE Rx Rx: 1.4 contact hours L EARNING O BJECTIVES 1. Explain the clotting mechanism. 2. Discuss the various drugs that alter blood coagulation. 3. Describe nursing care for patients receiving drugs that alter coagulation. The author and planners of this CNE activity have disclosed no relevant financial relationships with any commercial companies pertaining to this activity. See the last page of the article to learn how to earn CNE credit. Volume 7, Number 11 blood pools and doesn’t return to the heart efficiently. With atrial fibrillation, blood pools in the heart’s auricles and may clot. The artificial parts of a hip or knee replacement initially may damage a blood vessel, leading to clotting. All drugs that alter coagulation interfere with the normal protective reflexes. As a nurse, you need to be aware of the dangers of eliminating these reflexes, which could include serious or even fatal bleeding episodes. Drugs that alter coagulation include platelet inhibitors and anticoagulants. (See Classifying drugs that alter coagulation.) Platelet inhibitors Platelet inhibitors are often the first line of defense in preventing vascular clots; they don’t affect clots that already have formed. These drugs block platelets’ ability to adhere and aggregate to form the platelet plug—the first step in sealing the vascular system and preventing blood loss into body tissues. Current platelet inhibitors include abciximab (ReoPro), anagrelide (Agrylin), aspirin, cilostazol (Pletal), clopidogrel (Plavix), dipyridamole (Persantine), eptifibatide (Integrilin), ticlopidine (Ticlid), ticagrelor (Brilinta), and tirofiban (Aggrastat). These drugs are used to treat cardiovascular diseases in www.AmericanNurseToday.com Inside the coagulation process which vessels become occluded, as well as to maintain venous and arterial grafts and prevent cerebrovascular occlusion. They’re also given as adjuncts to thrombolytic therapy in treating myocardial infarction (MI) and preventing post-MI reinfarction. Ticagrelor, released in 2011, is indicated only to prevent thromboembolic events in acute coronary syndrome. Its black-box warning cites the risk of excessive bleeding and dangers of sudden withdrawal, which can trigger an acute cardiovascular event. Most platelet inhibitors block receptors on platelets to prevent adhesion; anagrelide prevents platelet formation in the bone marrow. Bleeding (including bleeding caused by toothbrushing and excessive bleeding after injury) is the most common adverse effect. Easy bruising also may occur. Nursing considerations When caring for patients receiving platelet inhibitors, minimize invasive procedures and take other steps to guard against blood loss. Be sure to teach about self-care. Advise them to avoid injury, use a soft-bristled toothbrush, shave with an electric razor, and avoid contact sports. Encourage them to carry or wear Medic-Alert jewelry that alerts healthcare providers to platelet inhibitor use. Stress the importance of telling all healthcare providers they’re taking a platelet inhibitor— especially dentists, surgeons, and others planning an invasive procedure. Caution patients to check with a physician before taking other agents that alter coagulation, including aspirin, nonsteroidal inflammatory drugs, and certain herbs. Emphasize the need to avoid excessive dosages, because no rapid antidote exists for excessive bleeding caused by drug overdose or overreaction. Teach patients about warning signs of excessive blood loss, and advise them to report these immediately. www.AmericanNurseToday.com Platelets Fibrin Collagen Striated muscle After an injury to a blood vessel, the vessel constricts. With a small injury, constriction typically seals the open space, allowing blood to flow and helping the vessel to heal. A larger injury exposes endothelial cells lining the vessel to blood flowing through it, causing platelets to adhere to the injured area. When a platelet adheres, it releases chemicals that attract more platelets, in turn drawing even more platelets to the area in a process called platelet aggregation. Consequently, a platelet plug forms. In some cases, this is enough to seal the leak and keep pressures stable while the vessel heals. In more severe injuries, the vessel wall injury activates Hagemann factor, a clotting factor. Activated Hagemann factor triggers activation of other clotting factors, initiating the clotting cascade. The cascade ends in conversion of prothrombin to thrombin; activated thrombin initiates clot formation. All clotting factors are made in the liver and require vitamin K for their formation. Calcium is the catalyst that speeds the clotting cascade. Activated thrombin breaks down fibrinogen into fibrin. An insoluble protein, fibrin forms a clot at the site. The change of blood from fluid to solid form stops blood flow in the vessel. In this process, called the intrinsic process, a clot forms within the vessel. A similar process, the extrinsic process, occurs in blood that has leaked out of the vessel at the injury site. This process produces a seal within the vessel, along with a seal outside the vessel. While this allows the vessel wall to seal and heal, it could interrupt blood flow to tissues beyond that point, causing ischemia or even cell death. When Hagemann factor is activated and triggers the clotting cascade, it also causes plasminogen conversion to plasmin. Plasmin dissolves fibrin and returns blood to the fluid state. This is the body’s clot-dissolving mechanism. Plasminogen, made in the liver, also is activated by such conditions as stress, fever, and various enzymes. This process protects against the harmful effects of clot formation. Anticoagulants Although commonly called blood thinners, anticoagulants don’t actually thin the blood. Like platelet inhibitors, they don’t dissolve clots that have already formed but they can prevent formation of new clots. In patients with clots, deep vein thrombosis, or occluded vessels that have caused an MI or a stroke, clot prevention is crucial, because new clot formation may compound the patient’s problem. Anticoagulants fall into two categories— injectable and oral. Injectable anticoagulants These agents act rapidly to directly block formation of thrombin from prothombin. Clotting changes occur November 2012 American Nurse Today 27 rapidly after injection. Injectable anticoagulants in current use include antithrombin III (Thrombate III), argatroban (Acova), bivalirudin (Angiomax), desirudin (Iprivask), fondaparinux (Arixtra), heparin (generic), and the low-molecularweight heparins dalteparin (Fragmin) and enoxaparin (Lovenox). Indications for injectable anticoagulants include acute treatment and prevention of venous thrombosis and pulmonary embolism, treatment of atrial fibrillation with embolization, prevention of clotting in blood samples and in dialysis and venous tubing, and diagnosis and treatment of disseminated intravascular coagulation. Nursing considerations. Be aware that in patients with excessive bleeding caused by anticoagulants, protamine sulfate can be injected as a rapid antidote to restore clotting activity. This drug directly reacts with thrombin, freeing it up to allow clots to form. Also, know that several serious to fatal medication errors have occurred when patients have inadvertently received two anticoagulants at the same time. Such errors are possible when, for instance, a hospital patient is put on a protocol that uses an anticoagulant and then is transferred to another unit, where she receives an anticoagulant from a different protocol. Warnings, labels, and effective communication among nurses at transfer points can help prevent this problem. The major drawback of injectable anticoagulants is that they must be injected. Some patients may be discharged on low-molecular-weight heparin to inject themselves; be sure to teach them proper injection technique and proper disposal of needles and syringes. Advise patients that they must have their blood tested frequently to check crucial coagulation indices. Whole blood clotting 28 American Nurse Today Classifying drugs that alter coagulation Drugs that affect blood coagulation fall into two main categories— platelet inhibitors and anticoagulants. Platelet inhibitors • abciximab (ReoPro) • anagrelide (Agrylin) • aspirin • cilostazol (Pletal) • clopidogrel (Plavix) • dipyridamole (Persantine) • eptifibatide (Integrilin) • ticagrelor (Brilinta) • ticlopidine (Ticlid) • tirofiban (Aggrastat) Anticoagulants Anticoagulants may be injectable or oral. Injectable anticoagulants • antithrombin III (Thrombate III) • argatroban (Acova) • bivalirudin (Angiomax) • dalteparin (Fragmin) • desirudin (Iprivask) • enoxaparin (Lovenox) • fondaparinux (Arixtra) • heparin Oral anticoagulants • dabigatran (Pradaxa) • rivaroxaban (Xarelto) • warfarin (Coumadin) time must be maintained at 2.5 to 3 times the control value, or activated partial thromboplastin time (APTT) must be maintained at 1.5 to 3 times the control value. Be sure to provide other protective measures and cover the same teaching topics as for patients receiving platelet inhibitors. Oral anticoagulants Previously, warfarin (Coumadin) was the only oral anticoagulant available. In recent years, two new oral anticoagulants have been approved by the Food and Drug Administration. Dabigatran (Pradaxa) Volume 7, Number 11 is a direct thrombin inhibitor; rivaroxaban (Xarelto) inhibits activated thrombin. Both stop the coagulation process. Warfarin. Warfarin blocks the liver’s use of vitamin K to produce clotting factors. It’s commonly prescribed for chronic conditions that might involve problems with clot formation, such as coronary artery disease, atrial fibrillation, knee or hip replacement, and immobility. However, warfarin has several disadvantages. For one, it takes time to deplete already-formed clotting factors; clot formation may not decrease until 48 to 72 hours after warfarin therapy begins. Also, if the patient receives too much warfarin and is bleeding, no precise antidote exists. Although vitamin K can be injected to trigger the liver to resume making clotting factors, clotting activity may not return for 48 to 72 hours. In severe overdose and bleeding, blood products containing clotting factors may be given to stop the bleeding; however, the liver still needs time to restore a normal level of clotting factors. Traditionally, warfarin was the only oral anticoagulant patients could take at home. In light of its www.AmericanNurseToday.com slowness in halting clot formation, warfarin therapy usually is started while the patient is still receiving an injectable anticoagulant; the latter drug is withdrawn when warfarin kicks in. Also, warfarin may interact with many other drugs and certain herbal supplements. What’s more, its effects may be altered by changes in the liver or in vitamin K production by the normal intestinal flora. (See Herbs and other supplements that increase bleeding risk.) Patients on warfarin need to have frequent blood tests to evaluate its effectiveness and allow dosage adjustment, if needed. The desired prothrombin time (PT) is 1.5 to 2.5 times the control value; the desired International Normalized Ratio (INR) is 2 to 3. If a drug is added to or removed from the patient’s regimen, warfarin dosage may need to be adjusted. As with any drug used to alter coagulation, be sure to provide education and support. Dabigatran. This drug was approved in 2010 for prevention of stroke and blood clots in patients with nonvalvular atrial fibrillation. Rather than affecting clotting-factor formation, it inhibits activation of a clotting factor, which stops the clotting cascade. Dabigatran has become the drug of choice for preventing clots in patients with chronic nonvalvular atrial fibrillation. It interacts with few drugs and its effects aren’t altered directly by liver function changes, so patients don’t need frequent blood testing to guide dosages. Because its half-life is 12 to 17 hours, the drug’s effects linger after the patient stops taking it. Teach patients to use all tablets within 60 days of opening the bottle. Instruct them to swallow tablets whole without cutting, crushing, or chewing. Advise them to protect the drug from humidity and light exposure. Because no antidote exists, caution patients to stay alert for signs and symptoms of exceswww.AmericanNurseToday.com Herbs and other supplements that increase bleeding risk The following herbs and supplements may increase the bleeding risk, especially in patients receiving drugs that alter coagulation: • angelica • cat’s claw • chamomile • chondroitin • feverfew • garlic • ginkgo • goldenseal • grape seed extract • green leaf tea • horse chestnut seed • psyllium • fish oil • vitamin E • turmeric. sive bleeding, such as excessive bruising, easy bleeding from minor injuries, and bleeding from toothbrushing. Stress that they shouldn’t stop taking the drug suddenly, because cardiovascular problems could result. Rivaroxaban. This drug was approved in 2011 to prevent deep vein thrombosis after knee or hip replacement surgery and to reduce stroke risk in patients with nonvalvular atrial fibrillation. It affects clot formation by inhibiting activated clotting factor. It has a shorter half-life than dabigatran (5 to 9 hours), so it clears from the body faster and its effects don’t last as long. No specific antidote exists. Caution patients not to stop taking rivaroxaban suddenly because this may cause sudden reversal of effects, triggering a stroke. Inform them that combining rivaroxaban with other drugs or herbs that af- fect coagulation could lead to excessive bleeding. Ensuring patient safety Patient safety is a major concern for patients receiving drugs that affect coagulation because they’re at risk for excessive bleeding. Take the following measures to protect patients from injury and minimize invasive procedures: • Help consolidate required blood withdrawals so the patient has fewer chances to bleed. • Clearly document in the chart that the patient is on this drug, to alert other caregivers that invasive procedures could lead to blood loss. • Use compression dressings over areas that could bleed. • Check all drugs and supplements the patient is taking for their potential to alter coagulation, which could lead to more bleeding • At least once during each shift, November 2012 American Nurse Today 29 Photo courtesy of MedicAlert® Foundation assess patients carefully for signs and symptoms of bleeding. • Evaluate clotting-test results to help determine the drug’s therapeutic dosage, if appropriate. • To help prevent or check for possible interactions, ask patients about all drugs, herbs, and other supplements they’re taking. Education is important for patients receiving these drugs. (See Crucial nursing care and patient education.) Be sure to teach them how and when to take the prescribed drug, and make sure they understand safety measures to prevent bleeding. * Crucial nursing care and patient education When caring for patients receiving drugs that alter coagulation, limit invasive procedures, apply prolonged pressure to puncture sites and wounds, and guard against activities that may cause bleeding. Evaluate for therapeutic drug effects and monitor for adverse effects that could put the patient at risk, such as hypersensitivity reactions, gastric hemorrhage, and bleeding. Monitor clotting tests to ensure therapeutic drug effects and decrease adverse effects. • For patients receiving warfarin, prothrombin time should be 1.5 to 2.5 times the control value, or the International Normalized Ratio (INR) should be 2 to 3. • For patients receiving heparin, whole blood clotting time should be 2.5 to 3 times the control value, or the activated partial thromboplastin time should be 1.5 to 3 times the control value. For patients on dabigatran or rivaroxaban, be aware that blood tests aren’t available to evaluate effectiveness. If your patient stops or starts a drug that alters coagulation, ask about other drugs or herbal supplements he or she is taking, because these could cause an interaction. Make sure all healthcare providers know the patient’s receiving the anticoagulant (especially at transfer points) and that the patient’s medical record clearly indicates this information. Essential teaching points Educate patients about the drug regimen and required safety measures. Advise them to use only a soft-bristled toothbrush and an electric razor. If they will be discharged on the drug, teach them how and when to administer it and (with an injectable drug) how to prepare, administer, and dispose of the drug, needles, and syringes. Advise patients using dabigatran or rivaroxaban how to store the drug properly. Instruct them to use it within 60 days of opening the bottle. Caution them not to stop taking the drug suddenly and to make sure they always have enough tablets on hand so they don’t run out. Also teach the patient: • the importance of carrying or wearing Medical Alert jewelry • when to return for blood tests to monitor drug effects • which other drugs, herbs, and other supplements to avoid • the importance of telling all healthcare providers they’re taking this drug • what to watch for and report, including prolonged bleeding, easy bruising, and changes in urine or stool color. 30 American Nurse Today Volume 7, Number 11 Selected references Brunton L, Chabner B, Knollman B. Goodman and Gilman’s The Pharmacological Basis of Therapeutics. 12th ed. New York: McGraw-Hill; 2010. Facts & Comparisons. Drug Facts and Comparisons 2012. 66th ed. Philadelphia: Lippincott Williams & Wilkins; 2011. Hankey GJ, Eikelboom JW. Dabigatran etexilate: a new oral thrombin inhibitor. Circulation. 2011 Apr 5;123:1436-50. Karch AM. 2012 Lippincott’s Nursing Drug Guide. Philadelphia: Lippincott Williams & Wilkins; 2011. Karch AM. Focus on Nursing Pharmacology. 6th ed. Philadelphia: Lippincott Williams & Wilkins; 2012. Mitke M. New alternative to warfarin may help reduce stroke in patients with AF. JAMA. 2011 Jan 5:305(1):25-6. Porth CM. Pathophysiology: Concepts of Altered Health States. 8th ed. Philadelphia: Lippincott Williams & Wilkins; 2010. Price MJ, Berger PB, Teirstein et al; GRAVITAS Investigators. Standard- vs high-dose clopidogrel based on platelet function testing after percutaneous coronary intervention: the GRAVITAS randomized trial. JAMA. 2011 Mar 16:305(11):1079-105. Shimoli V, Gage BF. Cost-effectiveness of dabigatran for stroke prophylaxis in atrial fibrillation. Circuation. 2011:123:2562-70. Streiff MB, Haut ER. The CMS ruling on venous thromboembolism after total knee or hip arthroplasty: weighing risks and benefits. JAMA. 2009 Mar 11:301(10):1063-5. Amy M. Karch is an associate professor of clinical nursing at the University of Rochester School of Nursing in Rochester, New York. www.AmericanNurseToday.com POST-TEST • Pharmacology review: Drugs that alter blood coagulation Earn contact hour credit online at www.americannursetoday.com/ContinuingEducation.aspx (ANT121101) Instructions To take the post-test for this article and earn contact hour credit, please go to www.AmericanNurseToday.com/ContinuingEducation.aspx. Simply use your Visa or MasterCard to pay the processing fee. (ANA members $15; nonmembers $20.) Once you’ve successfully passed the post-test and completed the evaluation form, you’ll be able to print out your certificate immediately. Provider accreditation The American Nurses Association’s Center for Continuing Education and Professional Development is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center’s Commission on Accreditation. ANCC Provider Number 0023. Contact hours: 1.4, Rx contact hours: 1.4. ANA’s Center for Continuing Education and Professional Development is approved by the California Board of Registered Nursing, Provider Number CEP6178. Post-test passing score is 75%. Expiration: 12/31/14 ANA Center for Continuing Education and Professional Development’s ac- Please mark the correct answer online. 1. Which of the following is among the first reactions to a blood vessel injury? a. Prothrombin is converted to thrombin. b. A blood clot forms. c. The blood vessel dilates. d. The blood vessel constricts. 2. Which statement about Hagemann factor is correct? a. It is activated when a minor injury to the vessel wall occurs. b. It is activated when a more severe injury to the vessel wall occurs. c. It stops the clotting cascade. d. It converts thrombin to prothrombin. 3. During the extrinsic process of blood coagulation: a. a seal forms outside the injured blood vessel. b. platelet aggregation occurs. c. thrombin breaks up fibrinogen. d. the clotting cascade is activated. 4. What is the role of plasmin in blood coagulation? a. It converts vitamin K to fibrinogen. b. It converts fibrin to plasminogen. c. It dissolves the Hagemann factor. d. It dissolves fibrin. 5. You admit a patient with atrial fibrillation who is taking clopidogrel. You explain to the student nurse accompanying you that this drug: a. stimulates receptors to prevent adhesion. b. is an anticoagulant. c. blocks receptors on platelets to prevent adhesion. d. is a blood thinner. www.AmericanNurseToday.com CNE: 1.4 contact hours Rx: 1.4 contact hours CNE Rx credited provider status refers only to CNE activities and does not imply that there is real or implied endorsement of any product, service, or company referred to in this activity nor of any company subsidizing costs related to the activity. This CNE activity does not include any unannounced information about off-label use of a product for a purpose other than that for which it was approved by the Food and Drug Administration (FDA). The planners of this CNE activity have disclosed no relevant financial relationships with any commercial companies pertaining to this CNE. P URPOSE / GOAL To provide nurses with the information they need to better manage patients who are receiving drugs that alter blood coagulation L EARNING O BJECTIVES 1. Explain the clotting mechanism. 2. Discuss the various medications that alter blood coagulation. 3. Describe nursing care for patients receiving drugs that alter coagulation. 6. Which drug may cause cardiovascular problems if discontinued suddenly? a. Enoxaparin b. Cilostazol c. Dabigatran d. Bivalirudin 7. To prevent formation of a new blood clot, which drug might be prescribed? a. Abciximab b. Eptifibatide c. Tirofiban d. Bivalirudin 8. Your patient with deep vein thrombosis is receiving an injectable anticoagulant. You explain to the patient that the drug works by: a. directly blocking formation of prothrombin from thrombin. b. directly blocking formation of thrombin from prothombin. c. dissolving the clot. d. thinning the blood. 9. Which agent is a rapid antidote that may be given when an anticoagulant causes excessive bleeding? a. Ticlopidine b. Dipyridamole c. Protamine sulfate d. Potassium sulfate 10. Your patient just started receiving heparin because of a pulmonary embolism. Which laboratory test result would concern you? a. Activated partial thromboplastin time (APTT) of 2 times the control value b. APTT of 4 times the control value c. Whole blood clotting time (WBCT) of 2.5 times the control value d. WBCT of 3 times the control value 11. Which statement about a rapid antidote for excessive bleeding caused by overdose or overreaction to platelet inhibitors is accurate? a. No rapid antidote exists for this situation. b. Vitamin K can be used as a rapid antidote. c. A rapid antidote is contraindicated in patients with myocardial infarction. d. A rapid antidote is contraindicated in patients with atrial fibrillation. 12. Which drug would you expect the physician to order for a patient with disseminated intravascular coagulation? a. Warfarin b. Dabigatran c. Aspirin d. Heparin 13. Your patient on warfarin experiences minor abnormal bleeding. Which vitamin may be given to stimulate the liver to start making clotting factors? a. Vitamin A b. Vitamin B c. Vitamin D d. Vitamin K 14. Your patient on warfarin therapy describes his activities at home. Which statement would concern you? a. “I stopped taking the garlic pills I used to take.” b. “I drink chamomile tea every evening to relax.” c. “I’m using a soft-bristled toothbrush.” d. “I’m shaving with an electric razor.” 15. Which of the following is a correct instruction for a patient taking rivaroxaban? a. Don’t suddenly stop taking the drug. b. Take it with chondroitin to increase effectiveness. c. Use the drug within 30 days. d. It is acceptable to skip 5 days. November 2012 American Nurse Today 31