Experimental Gerontology 41 (2006) 1080–1093
www.elsevier.com/locate/expgero
Review
Fracture healing in the elderly patient
Reinhard Gruber
a,b,1
, Hannjörg Koch b,d,f,1, Bruce A. Doll b,c, Florian Tegtmeier b,
Thomas A. Einhorn e, Jeffrey O. Hollinger b,*
a
Department of Oral Surgery, Medical University of Vienna, Austria
Bone Tissue Engineering Center, Carnegie Mellon University, Pittsburgh, USA
c
School of Dental Medicine, University of Pittsburgh, USA
d
Department of Orthopedic Surgery, University of Greifswald, Germany
e
Department of Orthopaedic Surgery, Boston University Medical Center, USA
Department of Orthopaedic Surgery, University of Pittsburgh Medical Center, USA
b
f
Received 14 July 2006; received in revised form 11 September 2006; accepted 12 September 2006
Available online 7 November 2006
Abstract
Clinical experience gives rise to the impression that there are differences in fracture healing in different age groups. It is evident that
fractures heal more efficiently in children than in adults. However, minimal objective knowledge exists to evaluate this assumption.
Temporal, spatial, and cellular quantitative and qualitative interrelationships, as well as signaling molecules and extracellular matrix
have not been comprehensively and adequately elucidated for fracture healing in the geriatric skeleton. The biological basis of fracture healing will provide a context for revealing the pathophysiology of delayed or even impaired bone regeneration in the elderly.
We will summarize experimental studies on age-related changes at the cellular and molecular level that will add to the pathophysiological understanding of the compromised bone regeneration capacity believed to exist in the elderly patient. We will suggest why this
understanding would be useful for therapeutics focused on bone regeneration, in particular fracture healing at an advanced age.
Ó 2006 Elsevier Inc. All rights reserved.
Keywords: Aging; Bone regeneration; Fracture; Osteoporosis; Gerontology; Tissue engineering; Growth factors
1. Fracture susceptibility in the osteoporotic, elderly patient
The physiological process of aging is highly complex at
the molecular, cellular, and systemic levels. The cumulative
effects of this process may lead to cognitive and functional
degenerative outcomes. Clinical observation suggests that
the majority of age-related events are initially constructive,
optimal and conducive to maximized survivability. However, through subtle changes and as a consequence of poorly
understood mechanisms, the fate of the organism stumbles
toward a degenerating finality (Editorial, 2005). ‘The aging
process’ and osteoporosis are two compelling degenerating
changes that have a profound human impact.
*
1
Corresponding author. Tel.: +1 412 268 6498; fax: +1 412 268 8641.
E-mail address: hollinge@cs.cmu.edu (J.O. Hollinger).
These authors contributed equally.
0531-5565/$ - see front matter Ó 2006 Elsevier Inc. All rights reserved.
doi:10.1016/j.exger.2006.09.008
We recognize that not all elderly patients are osteoporotic. Further, an osteoporotic individual may not be
elderly. However, it is generally accepted that if we live
long enough, we will become osteoporotic. Osteoporosis
is the result of progressive catabolic changes, mainly, but
nor exclusively, occurring in the aging skeleton, that cause
an increase in the risk of fracture (Manolagas, 2000; Riggs
and Parfitt, 2005). Fractures following traumatic events
such as falls, which a young individual’s bone would likely
resist, can be the consequence for the elderly, osteoporotic.
In large part due to population demographics and to some
extent as a consequence of the greater amount of physical
activities available for the elderly, there is a compelling
concern about the steady increase in the number of fractures each year. Consequently, the financial burden of
health care becomes more daunting each year, and there
is a commensurate increase in morbidity and mortality
(Cummings and Melton, 2002; Riggs and Melton, 1995).
R. Gruber et al. / Experimental Gerontology 41 (2006) 1080–1093
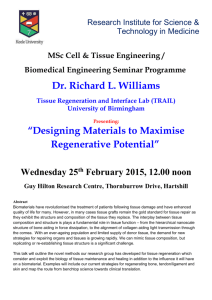
Fig. 1. Fracture susceptibility and therapeutic considerations in the
elderly patient. Demographic observations suggest that lifetime expectations are increasing. Aging is associated with a higher fracture risk and
diminished capacity of bone to heal. Two therapeutic strategies are
possible: one strategy will prevent and partially restore the age-related loss
of bone quality, characteristically applied in osteoporotic patients. The
second strategy is less common and addresses care and management after
a fracture has occurred in the elderly patient. The development of this
strategy should emphasize geriatric bone biology.
The lifetime risk for hip fractures is 17% in Caucasian
women and 6% in Caucasian men from age 50 years
onward (Cummings and Melton, 2002; Wehren, 2003).
Approximately 1.5 million fractures occur annually in the
United States and entail health care costs of about $13.8
billion, with $8.7 billion attributed to the age-related hip
fractures (Ray et al., 1997). Significantly, with the increase
in life expectancy, these estimates will have to be revised
dramatically upwards. The number of men and women
older than 65 years is predicted to increase from 32 million
in 1990 to 69 million in 2050, and 15 million people will be
85 or older. The prevalence of age-related fractures, and in
particular the mortality rates during the first years following hip fractures, will therefore increase over the next decades (Riggs and Melton, 1995). Predictably, the demand
for post-fracture patient management increase over the
next decades. Bone reconstruction procedures are
frequently performed in the older individuals, for example
in oral surgery, to allow stable placement of dental
implants in an augmented bone area (Wang and Boyapati,
2006). Also bone reconstruction following tumor resection
is challenging in the elderly patient (Marx, 2004). Clearly
there is a demand for therapies that take the age-related
changes into consideration (Fig. 1).
2. Therapeutic considerations in the osteoporotic, elderly
patient
Therapies may follow two strategies to address clinical
challenges of the aged skeletal system (Hadley et al., 2005).
One strategy will prevent and may reverse physiological
events that diminish the mechanical and structural integrity
of bone, the bone quality (Seeman and Delmas, 2006). Based
on an increased understanding of bone remodeling, involving osteoblast–osteoclast coupling and cell–hormonal inter-
1081
actions, potent pharmacologic substances such as
bisphosphonates, parathyroid hormone, strontium ranelate
and selective estrogen receptor modulators were developed
that will lower the fracture risk in elderly women and men
(Manolagas, 2000; Riggs and Parfitt, 2005; Rosen, 2005).
Nevertheless, even patients receiving such therapies remain
at risk for fracture (Delmas et al., 2005). Moreover, despite
sophisticated therapeutics and diagnostics, osteoporotic
changes frequently remain undiagnosed and these patients
are at an even higher risk to incur atraumatic fractures
(Gardner et al., 2002; Westesson et al., 2002).
Post-fracture patient management includes education
and physical rehabilitation (Gardner et al., 2005) and nutritional supplementation (Avenell and Handoll, 2005). Postfracture patient management can additionally require invasive treatments such as mechanical stabilization of the fracture ends and bridging of defects with bone grafts
(Stromsoe, 2004). Future strategies to support the repair
process may include cells and signaling molecules, as discussed later in this article. However, in neither of the
post-fracture patient managements, the biology of the aged
skeletal system has been adequately considered. A rational
therapeutic strategy for the aged, mostly osteoporotic
patient must be guided by biology. The authors emphasize
that the pathophysiological mechanisms of impaired bone
healing in the geriatric patient will be the basis for therapy
design and development. Thus, the second strategy to
address care and management of the elderly fracture
patient will emphasize geriatric bone biology to guide
design and development of a rational therapeutic protocol.
3. Current parameters of bone quality predict the fracture
risk but not the regenerative potential
In younger patients, the main etiology of a fracture is
high-energy trauma (Gomberg et al., 1999; Salminen
et al., 2000). Fractures of the femoral neck, vertebrae,
and distal radius as a result of falls and low-energy trauma
occur almost exclusively in the geriatric population, being
the hallmarks of osteoporosis (Cummings and Melton,
2002; Riggs and Melton, 1995). The femoral neck and vertebral bodies have a high percentage of trabecular bone
that is primarily affected by the age-related shift of bone
remodeling towards resorption. In women, a disproportional bone loss of 23–30% trabecular and 5–10% cortical
bone are frequently observed within the first postmenopausal decade. Subsequently, there is a slow phase of trabecular and cortical bone loss in both sexes. Bone quality
parameters have been established to monitor these changes
and to predict the susceptibility of bone to withstand fractures. (Riggs and Parfitt, 2005; Seeman and Delmas, 2006).
Histological analyses of biopsies provide static parameters
such as trabecular size and interconnectivity, and the
dynamic parameters of bone turnover such as the number
and activity of the basic remodeling units (Seeman and
Delmas, 2006). The clinical standard for diagnosis and
treatment of osteoporosis is routinely based only on one
1082
R. Gruber et al. / Experimental Gerontology 41 (2006) 1080–1093
static parameter observed by the radiological method of
bone density measurements (Riggs and Parfitt, 2005; Stokstad, 2005). Histological and radiological methods reflect
the age-related decrease of bone quality and can at least
partially explain the high fracture incidence in the osteoporotic population (Raisz, 2005). In addition, the repair
mechanisms, predictable and uneventful in youth, are compromised with age, as described later in this article. As a
consequence, with increasing age, the likelihood to acquire
fractures goes along with a compromised healing capacity.
However, bone quality parameters that reflect the mechanical stability of bone are likely to be different from those
parameters that provide insights into the regenerative
potential of bone. For example, why should a diminished
structural integrity of trabecular bone be a negative predictor for bone regeneration? Hence, there is an increasing
demand to establish bone quality parameters that can predict the success of bone regeneration. Bone biology can
provide a gate to reach this aim.
4. Clinical situation, morphologic aspects and biomechanical
competency with age-related changes in fracture repair
With increasing age not only the fracture incidence is
increased. In post-fracture management, the overall length
of hospital stay positively correlates with patient age and
older patients may be transferred to a skilled nursing facility and could be discharged earlier from the hospital than
younger individuals (Gomberg et al., 1999; Greatorex,
1988). Moreover, for patients who incur femoral and tibial
shaft fractures (Nilsson and Edwards, 1969; Skak and Jensen, 1988), femoral neck fractures (Nieminen et al., 1981),
floating knee injuries (Hee et al., 2001), and mandibular
fractures (Kawai et al., 1997), there is a significantly higher morbidity rate with elderly patients as compared to
younger individuals. These observations indicate that the
capacity of bone to regenerate slows with advancing age.
As many of the elderly patients have osteoporosis, the
question whether or not the lack of sex steroids negatively
affects the healing process has to be raised. Clinical studies
cannot provide a direct link between the hormone deficiency and the decrease in bone regeneration, as the endocrine status and possible co-morbidities have not been
adequately considered. Even in ovariectomiced rodents,
an accepted osteoporosis model, fracture healing can
either be unimpaired (Cao et al., 2002) or delayed (Meyer
et al., 2001). It thus remains open whether the lack of
estradiol, which is the key signal that causes loss of structural integrity, is also responsible for the compromised
bone regeneration capacity in the elderly.
To exclude possible effects of the endocrine status and
co-morbidities, animal models are performed that allow
detailed insights into the age-related changes in fracture
repair. Meyer et al. reported that 6-week-old rats regain
normal bone biomechanics at 4 weeks after a fracture,
26-week-old rats require 10 weeks, and 1-year-old
rats require more than 6 months (Meyer et al., 2001).
Age-related changes in mice include a delay in the onset
of the periosteal reaction, delays in cell differentiation,
decreased bone formation, delayed angiogenic invasion of
cartilage, a protracted period of endochondral ossification,
deceased bone formation and impaired bone remodeling
(Lu et al., 2005). Disrupted regulation of osteogenic differentiation, which is highly associated with blood vessel formation, is likely contributory to impaired fracture healing
(Lu et al., 2005). We assume that these morphologic and
biomechanical aspects from rodent models, may also
account responsible for the compromised bone regeneration capacity of the elderly patient. Underlying these agerelated changes at the cellular and molecular level will help
to guide design and development of a rational therapeutic
protocol. Pathophysiological changes of bone regeneration
in the elderly individual can only be understood when considering the physiology of fracture repair (Fig. 2).
5. Physiology of fracture repair: the spatial and temporal
sequence of the healing phases
Bone fractures result in blood vessel disruption and
tearing, and the ensuing blood clot fills the fracture site,
leading to localized hypoxia and acidosis. Within this
hypoxic and acidified environment, platelets are activated
and release alpha granules into the fibrin-rich extracellular
matrix (ECM). This is the hemostatic ‘blot clot’ that
functions as a depot for signaling molecules involving
chemoattractants for inflammatory cells. Neutrophils,
monocytes, and lymphocytes, appearing consecutively,
and their fibrinolytic activity enable them to migrate into
the extracellular matrix of the blood clot. Blood vessels
also sprout into the blood clot, together with undifferentiated mesenchymal cells forming the granulation tissue.
Mesenchymal progenitors originating from the periosteal
and the endosteal envelopes as well as from the bone marrow can differentiate into osteoblasts. The formation of
woven bone by osteoblasts that spans the fracture defect
leads to the development of the ‘hard callus’. Woven bone
is then remodeled into lamellar bone, a process recapitulating intramembranous bone formation. However, in
unstable fractures and gap defects, blood vessel formation
is either impaired or limited, and mesenchymal progenitor
cells pursue an endochondral pathway. Chondrogenic
cells undergo hypertrophy and mineralize their extracellular matrix. Concurrently, blood vessels penetrate the
chondrogenic tissue bringing chondroclast and mesenchymal progenitors that initiate cartilage replacement with
woven and lamellar bone. Fracture repair without callus
formation is possible when the cutting cones, an interrelated unit of osteoclasts, osteoblasts and blood vessels,
penetrate the fractured bone, permitting direct bone formation across the fracture gap (for review see Barnes
et al., 1999; Bolander, 1992; Hollinger and Wong, 1996;
Schenk and Hunziker, 1994).
Blood clot, granulation tissue, woven bone and cartilage
represent transient tissues that are replaced until mature
R. Gruber et al. / Experimental Gerontology 41 (2006) 1080–1093
1083
Fig. 2. Physiology of fracture repair: the spatial and temporal sequence of the healing phases. Bone regeneration involving fracture repair is a sequential
process that requires a coordinated action of cells, signaling molecules and the extracellular matrices. The sequence of events is initiated by the blood clot
and ends up with lamellar bone. Obviously there is a cascade of events that requires the coordinated action of cells within their environment. New cells are
attracted and respond to local cues causing the final replacement the ‘‘old’’ tissue. This is necessary because each transient tissue has a specific function: the
blood clot provides rapid hemostasis and initiates the healing cascade, granulation tissue can be considered the ‘healing blastema’ formed by the
immigrated mesenchymal cells and the blood capillaries, bending the bow to initiate the following differentiation steps. Cartilage is formed when blood
vessel supply is interrupted by unstable conditions and when oxygen tension is low. Once the cartilage collar provides stable conditions, blood capillaries
can sprout into the matrix and provide osteogenic cells that lay down woven bone. This process is termed endochondral bone formation. Stable conditions
at the defect site allow the differentiation of mesenchymal progenitors into osteoblasts, a process strictly associated with blood vessels and termed
intramembranous ossification. In both cases, woven bone is finally replaced by lamellar bone that has to withstand the functional demands the bone.
Although we have a limited understanding about the molecular mechanisms that drive this sequential process, it is quite obvious that the coordinated
action of mesenchymal cells and the cells that entail blood vessels are key in this process.
lamellar bone is formed. Bone regeneration is therefore a
sequential process associated with a calibrated pattern of
cell phenotypes. Cell calibration involves cell quantity, phenotype and their responsiveness to local parameters that
affect cell function: pH, oxygen tension, the extracellular
matrix and signaling molecules. Moreover, cell arrival
and location at the fracture is neither uniform nor homogeneous. The ‘healing blastema’ is a unique and transitory
ECM that has not been comprehensively studied across
population demographics. The notion of differences in
‘spatial’ and ‘temporal’ organization of the developing callus or ‘healing blastema’ must be acknowledged and studied to improve fracture healing therapeutics.
The spatial and temporal sequence of fracture healing
phases that will involve the ECM and cells first is destructive and second is constructive. The destructive phase of
fracture repair includes the removal of necrotic debris:
the avascular fragments of bone and soft tissues as well
as dead cells. Within 24–36 h post fracture, the constructive
phase begins. The transition between destructive and constructive phases is marked by a temporal stage of hemostasis and inflammation. Subsequent to this stage, are skip
stages: formative and remodeling of the constructive phase.
Clinical observations and animal studies underscore that
with increasing age, temporal progression through phases
is protracted and constituent elements of ECM and cells
quantitatively diminish through time (Claes et al., 2002;
Ekeland et al., 1982; Meyer et al., 2001; Nilsson and
Edwards, 1969). The profound impact of protracted ‘healing time’ and ‘quantitative cellular and ECM disparity’
with advanced age, emphasizes the need to design and
develop rational therapeutic protocols uniquely suited to
patient pathophysiology of the geriatric condition. Therefore, biological guidance must direct rational therapeutic
design and development.
6. Which cell phenotypes and signaling molecules control
fracture healing?
The constructive phase of fracture repair will not occur
without antecedent hemostasis, inflammation and blood
vessel formation. If we assume that fracture healing is a
special version of wound healing, using the established
mouse model, macrophages (Leibovich and Ross, 1975),
but not platelets (Szpaderska et al., 2003), neutrophils
(Simpson and Ross, 1972) and lymphocytes (Park and Barbul, 2004) must be highlighted. It is well known and accepted that wound healing events are driven through cell
activity and co-regulatory interactions among a cascade
of signaling biological mediators. Within the symphony
of this repair sequence, mesenchymal cells respond to chemotactic and mitogenic growth factors such as isoforms of
the platelet-derived growth factor (PDGF)-family (Andrew
et al., 1995; Fujii et al., 1999; Gruber et al., 2004), and
members of the bone morphogenetic protein (BMP)-family
of morphogens. Specifically, BMPs are potent osteochondrogenic differentiation factors (Cho et al., 2002; Kloen
et al., 2003; Onishi et al., 1998). BMP involvement in
fracture healing can be concluded from studies with
BMP-2+/ /BMP-6 / transgenic mice where endochondral, but not intramembranous bone formation was
impaired after femoral midshaft fractures (Kugimiya
et al., 2005). Hepatocyte growth factor can facilitate the
expression of BMP receptors in mesenchymal cells during
the early phase of fracture repair (Imai et al., 2005). Besides
BMPs, also Wnt, and hedgehog signaling may regulate
transcription factors Sox-9, RUNX-2, and osterix required
for osteochondrogenic differentiation during foetal development as well as during post-foetal fracture healing
(Hadjiargyrou et al., 2002; Murakami and Noda, 2000;
Vortkamp et al., 1998). Based upon in vivo models,
1084
R. Gruber et al. / Experimental Gerontology 41 (2006) 1080–1093
vascular endothelial growth factor (VEGF-A) neutralization by antibodies and inhibition of endothelial cell function with TNP-470 diminishes fracture healing (Carano
and Filvaroff, 2003; Hausman et al., 2001; Street et al.,
2002). It is valid, consequently, to underscore blood vessel
formation at the fracture as a pre-eminent key for timely
fracture healing. Additional investigation is warranted on
the inflammatory signaling pathways through tumor necrosis factor (TNF), arachidonic acid metabolites requiring
cyclooxygenase-2 (COX-2) activity (Lehmann et al., 2005;
Simon et al., 2002; Zhang et al., 2002), and nitric oxygen
(NO) synthesis (Baldik et al., 2005) in bone regeneration.
Post-fracture gene array analysis further indicates that
ligands and the corresponding receptors for transforming
growth factor beta molecules (TGF-b), BMPs, insulin-like
growth factors (IGF), and basic fibroblast growth factor
(bFGF) also termed FGF-2, are increasingly expressed,
as are genes associated with transporter activity and energy
derivation (Hadjiargyrou et al., 2002; Li et al., 2005). Using
a mouse model, regulators of osteoclastogenesis receptor
activator of NF-jB ligand (RANKL), osteoprotegerin
(OPG), and macrophage colony stimulating factor (MCSF) were highly expressed immediately post-fracture
(Kon et al., 2001). However, a lack of osteoclasts in the
RANK / mouse did not impair fracture healing (Flick
et al., 2003). Concluding functional roles among a panoply
of cell phenotypes by excluding one phenotype, trivializes a
highly complex interplay of cells whose relationships are in
large mysterious, not having been adequately elucidated.
Therefore, if osteoclastogenesis in the RANK / model
did not impact bone healing, what cell contingency was
evoked to enable unimpeded healing? There are poorly
defined and unidentified contingency healing loops that
govern physiological events in the fracture environment.
Are contingency loops and the redundancies built into adolescent healing are down regulated in the aged skeleton?
7. Age-related changes that may cause compromised bone
regeneration
The effect of aging on cellular and structural changes in
bone was recently summarized to provide insights into the
mechanisms leading the misbalanced bone remodeling
(Carrington, 2005; Kloss and Gassner, 2006). Moreover, a
significant data base on bone biology of fracture healing
has been developed emphasizing normal adult rodents.
However, the fundamental biology and biomechanics for
the aged animal models and its implications on fracture
healing and therapeutic intervention have not been sufficiently explored. Fundamental questions remain open:
what are the biological differences in the fracture healing
process across ages? Are there suitable correlates that may
establish precedence for pathophysiological differences?
Can correlates be exploited for therapeutic potential?
Are there epochal events in fracture healing that require
special emphasis? In the following section, we provide
experimental data on age-related changes at the cellular
and molecular level that will add to the pathophysiological understanding of the compromised bone regeneration
capacity (Fig. 3).
7.1. Local signaling mediators and systemic hormones
Expression levels of genes related to inflammation, osteogenic and chondrogenic differentiation and blood vessel
formation appear to peak at 1–2 weeks after fracture. Significant age-related changes in gene expression at fracture
sites have not been observed. However, expression levels
come to baseline values in adult rats prior to radiographic
union. It is conjectural whether this observation is relevant
to the temporal events of fracture healing (Desai et al.,
2003; Meyer et al., 2006; Meyer et al., 2003). We need to
be mindful that identification of gene expression must ultimately be related to the expression and function of the protein associated with the genes. Whether or not genes are
identified at the healing site must be painstakingly determined through histological analyses and imaging for the
protein they encode.
When serum concentrations of steroids, parathyroid
hormone (PTH), and calcitonin in postmenopausal women
were monitored within a one year period following hip
fracture, only PTH had an age-related increase during the
follow up period (Dubin et al., 1999). Secondary hyperparathyroidism is, however, an age-related phenomenon
that derives from the loss of sex steroid actions on extraskeletal calcium metabolism (Riggs et al., 2002). It remains
unclear whether higher cortisol concentration appearing in
elderly women but not in their younger counterparts following hip fractures impact on fracture healing (Frayn
et al., 1983).
7.2. Mesenchymal progenitor cell – cell number
Mesenchymal progenitor cells are key to bone regeneration. Mesenchymal progenitors undergo chondro-osteogenic differentiation to form cartilage under hypoxic conditions
and bone when blood vessel supply is adequate (Caplan,
1994; Owen and Friedenstein, 1988; Pittenger et al., 1999).
Mesenchymal progenitors are rare within the bone marrow
and can be selected in vitro by adherence to culture dishes.
Their high mitogenic potential allows rapid expansion and
further analysis confirming their multipultipotency. Mesenchymal progenitor cells not only differentiate into osteoblasts and chondrocytes, but also into other cells of the
mesenchymal lineage such as adipocytes and stromal cells
that support osteoclastogenesis. The mature phenotypes
are still considered ‘mesenchymal cells’. The progenitor cells
can be termed ‘mesenchymal stem or progenitor cells’ and
‘bone marrow stromal cells’. The number of colony-forming-unit fibroblasts, which is a rough estimate for the number of mesenchymal progenitors within the bone marrow,
shows an age-related decrease, independent of the species
(Bergman et al., 1996; D’Ippolito et al., 1999; Egrise
et al., 1992; Quarto et al., 1995). Whether or not the number
R. Gruber et al. / Experimental Gerontology 41 (2006) 1080–1093
1085
Fig. 3. Age-related changes that may cause the compromised bone regeneration: clinical observations and animal models indicate that the regenerative
capacity of bone diminishes with age. Histological analysis provide mechanistic insights on the spatial and temporal sequence of the healing phases.
However, we can only speculate about the mechanisms that account responsible for these observation. Current data suggest that with increasing age, the
mesenchymal progenitor cells and the cells required for blood vessel formation are either diminished in number or in their responsiveness to local or even
systemic molecules. General aging phenomenon may provide the underlying causes such as the reduced capacity of the organism to withstand reactive
oxidative stress.
of mesenchymal progenitor cells in the bone marrow
decreases to a level that significantly affects bone regeneration with age is controversial discussed, not only because
when human marrow-derived mesenchymal cells are
selected for the STRO-1 antigen no age-related effects
are observed (Stenderup et al., 2001). Mesenchymal progenitors are also found in the cambium layer of the periosteum and the endosteum. Thinning of the cambium
layer with age diminishes the ability of cartilage, and
likely also bone formation (O’Driscoll et al., 2001). Other
potential sources of mesenchymal cells include muscle
(Bosch et al., 2000), vessel-associated pericytes (Collett
and Canfield, 2005; Doherty et al., 1998), and blood
(Eghbali-Fatourechi et al., 2005). Whether their number
varies with age remains to be determined. It is also
unclear if the age-related shift of mesenchymal cells
toward the adipogenic phenotype at the expense of osteoblast differentiation impact fracture healing (Akune et al.,
2004). Moreover, with increasing age, the ability of mes-
enchymal cells to support osteoclastogenesis, by increasing the ratio of RANKL and OPG may have a guiding
role in the bone healing cascade (Cao et al., 2005).
7.3. Mesenchymal progenitor cell – mitogenic potential
Cell division capacity prior to senescence is lower in
adults than juveniles (Stenderup et al., 2003). The biological significance of a mitogenic decrement for mesenchymal
progenitor cells could lead to a quantitative deficiency and
impaired healing in the elderly. An interesting corollary to
compromised bone healing due to cell insufficiency is the
prospect of in vitro cell expansion that has been reported
to induce aging of mesenchymal progenitor cells (Baxter
et al., 2004). Deducing from this information, another possible problem in the aging patient is that the fewer cells,
forced to undergo cell divisions, may pre-maturely senesce,
thereby decreasing bone healing potential. Cell senescence
and apoptosis are important topics for study in the elderly,
1086
R. Gruber et al. / Experimental Gerontology 41 (2006) 1080–1093
involving the mechanisms of oxidative damage and glycation (Fehrer and Lepperdinger, 2005; Kloss and Gassner,
2006). Telomere shortening is a putative cause for senescence. Telomerase transfection will prolong mesenchymal
progenitor cell life span, enhance osteogenic differentiation
in vitro and bone formation in an immunodeficient mouse
model (Gronthos et al., 2003; Shi et al., 2002). Furthermore, telomerase deficiency impairs differentiation of mesenchymal progenitor cells into chondrocytes and
adipocytes (Liu et al., 2004). Also, serial passaging of
human bone-derived cells, which share gene marker characteristics with marrow-derived mesenchymal cells, will
cause alterations in morphology and cytoskeleton organization, and reduce expression of the transcription factor
RUNX-2 and differentiation markers (Christiansen et al.,
2000; Kassem et al., 1997; Kveiborg et al., 2001; Noth
et al., 2002). Contemporary data suggest that aging is associated with increased senescence of mesenchymal progenitor cells, a process that can negatively affect expansion
and differentiation capacity to the osteochondrogenic lineage during fracture repair.
7.4. Mesenchymal progenitor cell – responsiveness
Periosteum-derived cells from elderly rats respond
more
poorly
to
1,25
dihydroxyvitamin
D3
(1,25(OH)2D3) and transforming growth factor TGF-b
than cells from non-elderly donors (Shiels et al., 2002).
The periosteal-derived cells appear phenotypically indistinguishable from mesenchymal cells. Underscoring this
observation is that human bone-derived cells from younger individuals are more responsive to 1,25(OH)2D3 than
cells from the aged (Martinez et al., 1999). A similar finding has been reported for vitamin D receptor expression
levels (Martinez et al., 2001). Also, an age-dependent
increase of TGF-b receptor number, yet with a lower
ligand affinity, was reported as well (Batge et al., 2000).
These events and other cell-molecular changes may culminate in a negative correlation between DNA synthesis in
response to mitogens and donor age (Kato et al., 1995;
Pfeilschifter et al., 1993). However, mesenchymal progenitor cells isolated from young and adult but not geriatric
rats similarly respond to growth and differentiation factors suggesting that a general age-related impairment of
cellular response to signaling mediators cannot be attributed (Cei et al., 2006). Hence, additional fundamental
research needs to focus on mesenchymal progenitor cells,
their recruitment, mitogenic and differentiation potential,
and signaling responsiveness within fracture healing
microenvironments.
7.5. Blood vessel formation
Chondrogenesis, osteogenesis and angiogenesis occur in
a coordinated, sequenced pattern in skeletal tissue.
Impaired angiogenesis will decrease bone regeneration,
regardless of age. Changes in angiogenesis that occur with
aging have been noted at the molecular, cellular, and physiologic levels of regulation. At the healing fracture, local
VEGF release will herald vessel formation by causing
endothelial cells to migrate at the tips of capillary sprouts
where they proliferate and form tubular structures (Carmeliet, 2000; Ferrara, 1999; Risau, 1997; Yancopoulos et al.,
2000). Chemoattraction of pericytes and smooth muscle
cells help to stabilize capillary network formation and
arborization by a PDGF-BB-controlled process (Hellstrom
et al., 1999; Lindahl et al., 1997). Expression levels of
VEGF splice variants during the early stages of fracture
healing have not been affiliated with aging (Desai et al.,
2003).
The effects of aging on angiogenesis has been summarized elsewhere (Brandes et al., 2005; Edelberg and Reed,
2003; Foreman and Tang, 2003). Overall, a frank decrement in endothelial cells, the hemostatic cascade, neurochemical mediators, and growth factors and their
cognate receptors has been observed. Also alterations
in the structural and regulatory components of the
matrix contiguous to forming vessels in aged tissues
could influence bone healing in elderly patients (Brandes
et al., 2005; Edelberg and Reed, 2003; Foreman and
Tang, 2003). Due to their potential therapeutic impact,
endothelial progenitor cells (EPCs) will be highlighted.
EPCs originating from the hemangioblasts in the bone
marrow will support the blood vessel formation by a
process resembling vasculogenesis during development
(Murasawa and Asahara, 2005; Rafii and Lyden, 2003).
Although EPCs are rare within the blood, they are
increasingly released into the circulation in response to
injury (Gill et al., 2001). Age-related changes in the survival rate and motility, but not in the numbers of circulating EPCs have been reported (Heiss et al., 2005).
However, age is a major limiting factor for mobilization
of EPCs (Scheubel et al., 2003). In vitro studies revealed
that young bone marrow-derived EPCs recapitulated the
cardiac myocyte-induced expression of PDGF-BB,
whereas EPCs from the bone marrow of aging mice
did not express PDGF-BB when cultured in the presence
of cardiac myocytes (Edelberg et al., 2002). Together, the
age-related changes provide mechanistic insights into the
diminished angiogenesis and vasculogenesis in ischemiareperfusion models (Rivard et al., 1999; Shimada et al.,
2004; Swift et al., 1999).
Moreover, cross-sections through the mid-diaphysis of
long bones showed that with age, the blood supply to the
cortex was predominantly from the periosteum in contrast
to the medullary canal in younger conditions. It is unclear
what this observation means and the affect of transcortical
hemodynamics and increased periosteal supply for bone
survival in old age (Bridgeman and Brookes, 1996).
Although there is no direct evidence, decreased blood vessel formation may contribute to the age-related delay of
fracture healing. Therapeutics that support blood vessel
formation will be essential to enhance wound compromised
conditions in the elderly patient.
R. Gruber et al. / Experimental Gerontology 41 (2006) 1080–1093
7.6. Transplantation experiments
Approximately 5-fold more bone is formed when total
marrow cells from young mice (compared to their older littermates) are transplanted into either young or old recipients. The age of the recipient has only minor effects with
approximately one third less bone formation in old animals
as compared to younger recipients (Inoue et al., 1997). The
relevance of osteogenic cell quantity in the marrow appears
to correlate with the quantity of ectopic bone formation.
This observation underscores the fact that a threshold
quantity of cells will be responsible for the biological process of fracture and that the bone marrow of young animals is a rich source. The local environment of the
recipient site has a minor impact on the osteogenic capacity
of the transplant.
Intramuscular implantation of demineralized bone
matrix (DBM) and bone marrow caused less calcium and
lower levels of alkaline phosphatase in implants placed into
older rabbits (Strates et al., 1988). In a rat model, calcium
accumulation and expression of alkaline phosphatase
activity in transplanted demineralized bone matrix significantly depressed in a 10- and 16-month-old compared to
1-month-old rats (Nishimoto et al., 1985). Age-related
effects were also observed with recombinant BMP-2 in a
rat model (Matsumoto et al., 2001). When the implant period duration was doubled, 16-month-old rats formed bone
volume equivalent to 3-month-old rats. Moreover, increasing the dose of BMP-2 increased bone formation in older
rats (Fleet et al., 1996). Interestingly, administration of
PTH, prostaglandin E2 (PGE2), or 1,25(OH)2D3 restored
the bone inductive activity of BMP-2 in aged rats (Kabasawa et al., 2003). Overall, these ectopic transplantation
studies imply that mesenchymal progenitor cells and the
local environment may contribute to age-related changes
in bone formation.
7.7. Bone matrix
DBM prepared from younger donors has been reported to be more osteoinductive than preparations from older animals, indicating a possible decrease in BMPs and
additional soluble signals from aged donors (Reddi,
1985). Also, IGF-I and TGF-b concentration in bone
undergoes age-related decreases (Pfeilschifter et al., 1998;
Seck et al., 1998). Further, the age-related decrement in
IGF concentration of binding protein-5 in human cortical
bone has been noted (Nicolas et al., 1995). However,
TGF-b, IGFs and their binding proteins in long-term
bone cell cultures appear to be preserved with age (Bismar
et al., 1999; Pfeilschifter et al., 2000). The importance of
matrix-derived signaling mediators in fracture healing
needs to be a focus for investigative exploration. It is
not clear if the signaling mediators released survive the
acid pH between the osteoclast and the bone matrix. It
is well known, however, that many BMPs and PDGF isoforms are acid stable.
1087
Changes found in skin collagen also occur in bone collagen with aging and may be a causal counterpart to loss of
bone quality in senile osteoporosis (Shuster, 2005). In addition, age-related changes of non-calcified collagen in
human cortical bone have been reported (Wang et al.,
2003). Non-enzymatic glycation-induced cross links of the
collagen might also be a reason for the reduced biomechanical properties of aged bone, in remodeling but also during
bone regeneration (Wang et al., 2003; Zioupos et al., 1999).
7.8. Antioxidants and neutralization of reactive oxygen
species
Factors impairing fracture healing may include the limited capacity of the elderly to neutralize reactive oxygen
species of the respiratory chain. Free radicals produced
by the respiratory chain may cause oxidative damage to
various cellular components which may affect cellular function, also involving cells of the osteogenic and chondrogenic lineage (Carrington, 2005; Kloss and Gassner, 2006).
Antioxidants, vitamins C and E, and the enzymes superoxide dismutase, catalase and glutathione peroxidase may
contribute to bone regeneration. Recent findings suggest
that reactive oxygen species play a role in bone loss following ovariectomy (Lean et al., 2003; Lean et al., 2005). In
animal models, vitamins C and E had a positive effect on
fracture healing (Turk et al., 2004). Similar studies with
regard to impaired fracture healing in geriatric models were
not performed.
8. Therapeutic concepts to increase bone regeneration in the
elderly patient
8.1. Local recombinant signaling molecules
There are currently two signaling mediators approved
by the Food and Drug Administration (FDA) for bone
healing. Recombinant human BMP-2 and BMP-7 are
approved for spinal fusion surgery and treatment of recalcitrant tibial fractures, respectively (Mont et al., 2004; Termaat et al., 2005). Recombinant human PDGF-BB has
received FDA approval to treat diabetic ulcers (Nagai
and Embil, 2002; Smiell et al., 1999) and to stimulate periodontal regeneration (Nevins et al., 2005). Local application of patient-derived platelet-rich plasma can enhance
bone regeneration in compromised situations such as fracture healing in diabetic rats and bone reconstruction following tumor resection (Gandhi et al., 2006; Marx, 2004).
Impaired blood vessel formation may be reversed using
local application of VEGF either alone or together with
BMPs (Huang et al., 2005; Tarkka et al., 2003). The
sequential release of VEGF and PDGF-BB may improve
bone regeneration through stimulating blood vessels and
enhancing their maturation (Richardson et al., 2001).
Similar studies in geriatric animals have not been performed so far. However, the effect of bFGF, TGF-b and
IGF-I were tested in fracture models considering the
1088
R. Gruber et al. / Experimental Gerontology 41 (2006) 1080–1093
(Aaron et al., 2004; Nelson et al., 2003). However, the studies are in preclinical development and do not discriminate
groups on an age basis. Future studies should follow the
concept of Knopp et al. who determined the effect of aging
on the response of rats to intermittent treatment with parathyroid hormone, however with regard to bone remodeling
(Knopp et al., 2005). The effect of systemic growth hormone on fracture healing were determined under the background of old rats (Bak and Andreassen, 1991).
8.3. Cell and gene therapy
Fig. 4. Therapeutic concepts to increase bone regeneration in the elderly
patient. It is a rationally concept to develop strategies based on the
functional understanding of bone regeneration in the elderly. However, we
lack parameters that can predict bone quality with regard to its
regenerative capacity. Ideal would be to promote those parameters that
are diminished with aging. Based on our current knowledge, strategies to
increase cells number, the mitogenic activity, differentiation and matrix
synthesis would be reasonable to develop. The therapies should target
mesenchymal cells and cells required for blood vessel formation and tested
in the relevant animal models.
impaired regenerative capacity with age (Aronson, 2004;
Blumenfeld et al., 2002). BMP-7 can effectively stimulate
fracture repair in both young (3-month-old) and old (18month-old) rats. The effect of rhBMP-7 on the rate of fracture healing was greater in young rats compared to old rats
(Hak et al., 2006). These findings indicate that aging can
diminish the response to a therapeutic intervention such
as with rhBMP-7, nevertheless, geriatric rodents retain
their potential to respond to the therapy. More studies that
follow this design are demanded in the near future. This is
because it does not necessarily mean that if a therapy
works in the young individual, it also stimulates bone
regeneration in the geriatric. On the other hand, if a
therapy that does not provide a benefit in the young,
healthy individual, it may be successfully applied in the
elderly patient (Fig. 4).
Local application of osteogenic cells from bone marrow
and other sources (Cancedda et al., 2003; Caplan and Bruder, 2001) can enhance fracture healing. Moreover, osteogenic cells can provide a microenvironment that favors
blood vessel formation (Gruber et al., 2005). Transplantation of endothelial progenitor cells have the potential to
increase wound healing, similar studies in fracture models
are lacking (Suh et al., 2005). The clinical implementation
of autologous cell therapy may be hampered by the inconvenient ex vivo expansion procedure. Allogeneic cell preparations to treat bone defects is confounded by the
rejection response in vivo (Liu et al., 2006). Gene therapeutic approaches involving transfection of signaling mediators into mesenchymal cells are in preclinical level
development (Doll et al., 2001; Gamradt and Lieberman,
2004). Neither of the therapies was tested for the efficacy
under the impaired conditions of aging.
Even though strategies to increase bone regeneration or
to restore non-healing fractures have reached the level of
clinical trials, their usefulness under the particular conditions of the elderly patient have not specifically been considered. Preclinical studies similar to those that test
influence of age on the effectiveness of rhBMP-7 treatment
in a fracture non-union formation are clinically relevant
and provide the basis for the development of therapeutics
focused on bone regeneration, in particular fracture healing for the elderly (Hak et al., 2006). Nevertheless, the studies are rather based on an empiric approach. We propose to
go one more step further and develop therapies that consider geriatric bone biology to guide design and development
of a rational therapeutic protocol.
8.2. Systemic signaling molecules and biomechanics
9. Conclusion
Systemic application of PTH and agonists of prostaglandin receptors 2 and 4 have been reported to increase
healing of bone defects (Alkhiary et al., 2005; Komatsubara et al., 2005; Li et al., 2003; Nakazawa et al., 2005; Paralkar et al., 2003; Tanaka et al., 2004). Supplementation of
calcium and 1,25(OH)2D3 may have beneficial effects given
vitamin D synthesis decreases with increasing age (Doetsch
et al., 2004). Simvastatin improves fracture healing in mice,
and age-associated impairment of neovascularization
might be a new target of statin therapy (Shimada et al.,
2004; Skoglund et al., 2002). Moreover, stimulation with
physical forces is considered beneficial in fracture healing
The blessing of growing old carries with it the burden of
progressive skeletal degeneration and handicapped bone
regeneration. This statement may be challenged as being
controversial. However, there are supporting, irrefutable
clinical and fundamental data. Rational therapeutic design
requires a biological foundation as a guide. Therapeutics
that will enable elderly patients to overcome the pathophysiological challenges of compromised wound healing
must be based on biology. The parameters that define bone
quality with regard to bone regeneration are multiple and
include the number, life time and responsiveness to local
R. Gruber et al. / Experimental Gerontology 41 (2006) 1080–1093
and systemic factors of mesenchymal progenitors and cells
required for blood vessel formation. It is not clear to which
extent each parameter contributes to the regenerative
cascade. Future strategies should consider both, the
osteogenic and the angiogenic requirements to overcome
the compromised situation in the elderly patient. More
basic, fundamental research is needed to define the temporal, spatial, quantitative and qualitative cellular interrelationships of signaling molecules and extracellular matrix
of fracture healing in the geriatric skeleton, with specific
emphasis of the osteoporotic changes. Pivotal to the comprehensive understanding of fracture healing is a standardized fracture repair model (Gerstenfeld et al., 2005) defined
by functional, molecular and cellular parameters distinguishing relative age and conducted through longitudinal
studies. The pathophysiologically challenged models must
be exploited to elucidate the applied aspects of fracture
healing and to validate therapeutic safety and effectiveness.
Acknowledgements
Partial funding for this review is from NIH R01DE13018-02 (JOH) and the Oesterreichische Nationalbank
#10905 (RG).
References
Aaron, R.K., Ciombor, D.M., Simon, B.J., 2004. Treatment of nonunions
with electric and electromagnetic fields. Clin. Orthop. Relat. Res., 21–
29.
Akune, T., Ohba, S., Kamekura, S., Yamaguchi, M., Chung, U.I.,
Kubota, N., Terauchi, Y., Harada, Y., Azuma, Y., Nakamura, K.,
Kadowaki, T., Kawaguchi, H., 2004. PPARgamma insufficiency
enhances osteogenesis through osteoblast formation from bone marrow progenitors. J. Clin. Invest. 113, 846–855.
Alkhiary, Y.M., Gerstenfeld, L.C., Krall, E., Westmore, M., Sato, M.,
Mitlak, B.H., Einhorn, T.A., 2005. Enhancement of experimental
fracture-healing by systemic administration of recombinant human
parathyroid hormone (PTH 1-34). J. Bone Joint Surg. Am. 87, 731–741.
Andrew, J.G., Hoyland, J.A., Freemont, A.J., Marsh, D.R., 1995.
Platelet-derived growth factor expression in normally healing human
fractures. Bone 16, 455–460.
Aronson, J., 2004. Modulation of distraction osteogenesis in the aged rat
by fibroblast growth factor. Clin. Orthop. Relat. Res., 264–283.
Avenell, A., Handoll, H.H., 2005. Nutritional supplementation for hip
fracture aftercare in older people. Cochrane Database Syst Rev, 18,
CD001880.
Bak, B., Andreassen, T.T., 1991. The effect of growth hormone on fracture
healing in old rats. Bone 12, 151–154.
Baldik, Y., Diwan, A.D., Appleyard, R.C., Ming Fang, Z., Wang, Y.,
Murrell, G.A., 2005. Deletion of iNOS gene impairs mouse fracture
healing. Bone 37, 32–36.
Barnes, G.L., Kostenuik, P.J., Gerstenfeld, L.C., Einhorn, T.A., 1999.
Growth factor regulation of fracture repair. J. Bone Miner. Res. 14,
1805–1815.
Batge, B., Feydt, A., Gebken, J., Klein, H., Notbohm, H., Muller, P.K.,
Brinckmann, J., 2000. Age-related differences in the expression of
receptors for TGF-beta in human osteoblast-like cells in vitro. Exp.
Clin. Endocrinol. Diabetes 108, 311–315.
Baxter, M.A., Wynn, R.F., Jowitt, S.N., Wraith, J.E., Fairbairn, L.J.,
Bellantuono, I., 2004. Study of telomere length reveals rapid aging of
human marrow stromal cells following in vitro expansion. Stem Cells
22, 675–682.
1089
Bergman, R.J., Gazit, D., Kahn, A.J., Gruber, H., McDougall, S., Hahn,
T.J., 1996. Age-related changes in osteogenic stem cells in mice. J.
Bone Miner. Res. 11, 568–577.
Bismar, H., Kloppinger, T., Schuster, E.M., Balbach, S., Diel, I., Ziegler,
R., Pfeilschifter, J., 1999. Transforming growth factor beta (TGF-beta)
levels in the conditioned media of human bone cells: relationship to
donor age, bone volume, and concentration of TGF-beta in human
bone matrix in vivo. Bone 24, 565–569.
Blumenfeld, I., Srouji, S., Lanir, Y., Laufer, D., Livne, E., 2002.
Enhancement of bone defect healing in old rats by TGF-beta and
IGF-1. Exp. Gerontol. 37, 553–565.
Bolander, M.E., 1992. Regulation of fracture repair by growth factors.
Proc. Soc. Exp. Biol. Med. 200, 165–170.
Bosch, P., Musgrave, D.S., Lee, J.Y., Cummins, J., Shuler, T., Ghivizzani,
T.C., Evans, T., Robbins, T.D., Huard, J., 2000. Osteoprogenitor cells
within skeletal muscle. J. Orthop. Res. 18, 933–944.
Brandes, R.P., Fleming, I., Busse, R., 2005. Endothelial aging. Cardiovasc
Res. 66, 286–294.
Bridgeman, G., Brookes, M., 1996. Blood supply to the human femoral
diaphysis in youth and senescence. J. Anat. 188 (Pt 3), 611–621.
Cancedda, R., Bianchi, G., Derubeis, A., Quarto, R., 2003. Cell therapy
for bone disease: a review of current status. Stem Cells 21, 610–619.
Cao, Y., Mori, S., Mashiba, T., Westmore, M.S., Ma, L., Sato, M.,
Akiyama, T., Shi, L., Komatsubara, S., Miyamoto, K., Norimatsu, H.,
2002. Raloxifene, estrogen, and alendronate affect the processes of
fracture repair differently in ovariectomized rats. J. Bone Miner. Res.
17, 2237–2246.
Cao, J.J., Wronski, T.J., Iwaniec, U., Phleger, L., Kurimoto, P.,
Boudignon, B., Halloran, B.P., 2005. Aging increases stromal/osteoblastic cell-induced osteoclastogenesis and alters the osteoclast precursor pool in the mouse. J. Bone Miner. Res. 20, 1659–1668.
Caplan, A.I., 1994. The mesengenic process. Clin Plast Surg. 21, 429–435.
Caplan, A.I., Bruder, S.P., 2001. Mesenchymal stem cells: building blocks
for molecular medicine in the 21st century. Trends Mol. Med. 7, 259–
264.
Carano, R.A., Filvaroff, E.H., 2003. Angiogenesis and bone repair. Drug
Discov. Today 8, 980–989.
Carmeliet, P., 2000. Mechanisms of angiogenesis and arteriogenesis. Nat.
Med. 6, 389–395.
Carrington, J.L., 2005. Aging bone and cartilage: cross-cutting issues.
Biochem. Biophys. Res. Commun. 328, 700–708.
Cei, S., Kandler, B., Fugl, A., Gabriele, M., Hollinger, J.O., Watzek, G.,
Gruber, R., 2006. Bone marrow stromal cells of young and adult rats
respond similarly to platelet-released supernatant and bone morphogenetic protein-6 in vitro. J. Periodontol. 77, 699–706.
Cho, T.J., Gerstenfeld, L.C., Einhorn, T.A., 2002. Differential temporal
expression of members of the transforming growth factor beta
superfamily during murine fracture healing. J. Bone. Miner Res. 17,
513–520.
Christiansen, M., Kveiborg, M., Kassem, M., Clark, B.F., Rattan, S.I.,
2000. CBFA1 and topoisomerase I mRNA levels decline during
cellular aging of human trabecular osteoblasts. J. Gerontol. A. Biol.
Sci. Med. Sci. 55, B194–B200.
Claes, L., Grass, R., Schmickal, T., Kisse, B., Eggers, C., Gerngross, H.,
Mutschler, W., Arand, M., Wintermeyer, T., Wentzensen, A., 2002.
Monitoring and healing analysis of 100 tibial shaft fractures. Langenbecks Arch. Surg. 387, 146–152.
Collett, G.D., Canfield, A.E., 2005. Angiogenesis and pericytes in the
initiation of ectopic calcification. Circ. Res. 96, 930–938.
Cummings, S.R., Melton, L.J., 2002. Epidemiology and outcomes of
osteoporotic fractures. Lancet 359, 1761–1767.
Delmas, P.D., Rizzoli, R., Cooper, C., Reginster, J.Y., 2005. Treatment
of patients with postmenopausal osteoporosis is worthwhile. The
position of the International Osteoporosis Foundation. Osteoporos
Int. 16, 1–5.
Desai, B.J., Meyer, M.H., Porter, S., Kellam, J.F., Meyer Jr., R.A., 2003.
The effect of age on gene expression in adult and juvenile rats following
femoral fracture. J. Orthop. Trauma. 17, 689–698.
1090
R. Gruber et al. / Experimental Gerontology 41 (2006) 1080–1093
D’Ippolito, G., Schiller, P.C., Ricordi, C., Roos, B.A., Howard, G.A.,
1999. Age-related osteogenic potential of mesenchymal stromal stem
cells from human vertebral bone marrow. J. Bone Miner. Res. 14,
1115–1122.
Doetsch, A.M., Faber, J., Lynnerup, N., Watjen, I., Bliddal, H.,
Danneskiold-Samsoe, B., 2004. The effect of calcium and vitamin D3
supplementation on the healing of the proximal humerus fracture: a
randomized placebo-controlled study. Calcif. Tissue Int. 75, 183–188.
Doherty, M.J., Ashton, B.A., Walsh, S., Beresford, J.N., Grant, M.E.,
Canfield, A.E., 1998. Vascular pericytes express osteogenic potential
in vitro and in vivo. J. Bone Miner. Res. 13, 828–838.
Doll, B., Sfeir, C., Winn, S., Huard, J., Hollinger, J., 2001. Critical aspects
of tissue-engineered therapy for bone regeneration. Crit. Rev.
Eukaryot. Gene Expr. 11, 173–198.
Dubin, N.H., Monahan, L.K., Yu-Yahiro, J.A., Michael, R.H., Zimmerman, S.I., Hawkes, W., Hebel, J.R., Fox, K.M., Magaziner, J., 1999.
Serum concentrations of steroids, parathyroid hormone, and calcitonin in postmenopausal women during the year following hip fracture:
effect of location of fracture and age. J. Gerontol. A Biol. Sci. Med.
Sci. 54, M467–M473.
Edelberg, J.M., Reed, M.J., 2003. Aging and angiogenesis. Front Biosci. 8,
S1199–S1209.
Edelberg, J.M., Tang, L., Hattori, K., Lyden, D., Rafii, S., 2002. Young
adult bone marrow-derived endothelial precursor cells restore agingimpaired cardiac angiogenic function. Circ. Res. 90, E89–E93.
Editorial, 2005. Aging research comes of age (featuring 11 reviews on
various aspects of aging research). Cell 120, 435.
Eghbali-Fatourechi, G.Z., Lamsam, J., Fraser, D., Nagel, D., Riggs, B.L.,
Khosla, S., 2005. Circulating osteoblast-lineage cells in humans. N.
Engl. J. Med. 352, 1959–1966.
Egrise, D., Martin, D., Vienne, A., Neve, P., Schoutens, A., 1992. The
number of fibroblastic colonies formed from bone marrow is decreased
and the in vitro proliferation rate of trabecular bone cells increased in
aged rats. Bone 13, 355–361.
Ekeland, A., Engesoeter, L.B., Langeland, N., 1982. Influence of age on
mechanical properties of healing fractures and intact bones in rats.
Acta Orthop. Scand. 53, 527–534.
Fehrer, C., Lepperdinger, G., 2005. Mesenchymal stem cell aging. Exp.
Gerontol..
Ferrara, N., 1999. Vascular endothelial growth factor: molecular and
biological aspects. Curr. Top Microbiol. Immunol. 237, 1–30.
Fleet, J.C., Cashman, K., Cox, K., Rosen, V., 1996. The effects of aging on
the bone inductive activity of recombinant human bone morphogenetic
protein-2. Endocrinology 137, 4605–4610.
Flick, L.M., Weaver, J.M., Ulrich-Vinther, M., Abuzzahab, F., Zhang,
X., Dougall, W.C., Anderson, D., O’Keefe, R.J., Schwarz, E.M., 2003.
Effects of receptor activator of NFkappaB (RANK) signaling blockade on fracture healing. J. Orthop. Res. 21, 676–684.
Foreman, K.E., Tang, J., 2003. Molecular mechanisms of replicative
senescence in endothelial cells. Exp. Gerontol. 38, 1251–1257.
Frayn, K.N., Stoner, H.B., Barton, R.N., Heath, D.F., Galasko, C.S.,
1983. Persistence of high plasma glucose, insulin and cortisol concentrations in elderly patients with proximal femoral fractures. Age
Ageing 12, 70–76.
Fujii, H., Kitazawa, R., Maeda, S., Mizuno, K., Kitazawa, S., 1999.
Expression of platelet-derived growth factor proteins and their
receptor alpha and beta mRNAs during fracture healing in the normal
mouse. Histochem. Cell Biol. 112, 131–138.
Gamradt, S.C., Lieberman, J.R., 2004. Genetic modification of stem cells
to enhance bone repair. Ann. Biomed. Eng. 32, 136–147.
Gandhi, A., Doumas, C., O’Connor, J.P., Parsons, J.R., Lin, S.S., 2006.
The effects of local platelet rich plasma delivery on diabetic fracture
healing. Bone 38, 540–546.
Gardner, M.J., Flik, K.R., Mooar, P., Lane, J.M., 2002. Improvement in
the undertreatment of osteoporosis following hip fracture. J. Bone
Joint Surg. Am., 1342–1348.
Gardner, M.J., Brophy, R.H., Demetrakopoulos, D., Koob, J., Hong, R.,
Rana, A., Lin, J.T., Lane, J.M., 2005. Interventions to improve
osteoporosis treatment following hip fracture. A prospective, randomized trial. J. Bone Joint Surg. Am. 87, 3–7.
Gerstenfeld, L.C., Wronski, T.J., Hollinger, J.O., Einhorn, T.A., 2005.
Application of histomorphometric methods to the study of bone
repair. J. Bone Miner. Res. 20, 1715–1722.
Gill, M., Dias, S., Hattori, K., Rivera, M.L., Hicklin, D., Witte, L.,
Girardi, L., Yurt, R., Himel, H., Rafii, S., 2001. Vascular trauma
induces rapid but transient mobilization of VEGFR2(+)AC133(+)
endothelial precursor cells. Circ. Res. 88, 167–174.
Gomberg, B.F., Gruen, G.S., Smith, W.R., Spott, M., 1999. Outcomes in
acute orthopaedic trauma: a review of 130,506 patients by age. Injury
30, 431–437.
Greatorex, I.F., 1988. Proximal femoral fractures: an assessment of the
outcome of health care in elderly people. Commun. Med. 10, 203–210.
Gronthos, S., Chen, S., Wang, C.Y., Robey, P.G., Shi, S., 2003.
Telomerase accelerates osteogenesis of bone marrow stromal stem
cells by upregulation of CBFA1, osterix, and osteocalcin. J. Bone
Miner. Res. 18, 716–722.
Gruber, R., Karreth, F., Kandler, B., Fuerst, G., Rot, A., Fischer, M.B.,
Watzek, G., 2004. Platelet-released supernatants increase migration
and proliferation, and decrease osteogenic differentiation of bone
marrow-derived mesenchymal progenitor cells under in vitro conditions. Platelets 15, 29–35.
Gruber, R., Kandler, B., Holzmann, P., Vogele-Kadletz, M., Losert, U.,
Fischer, M.B., Watzek, G., 2005. Bone marrow stromal cells can
provide a local environment that favors migration and formation of
tubular structures of endothelial cells. Tissue Eng. 11, 896–903.
Hadjiargyrou, M., Lombardo, F., Zhao, S., Ahrens, W., Joo, J., Ahn, H.,
Jurman, M., White, D.W., Rubin, C.T., 2002. Transcriptional profiling of bone regeneration. Insight into the molecular complexity of
wound repair. J. Biol. Chem. 277, 30177–30182.
Hadley, E.C., Lakatta, E.G., Morrison-Bogorad, M., Warner, H.R.,
Hodes, R.J., 2005. The future of aging therapies. Cell 120, 557–567.
Hak, D.J., Makino, T., Niikura, T., Hazelwood, S.J., Curtiss, S., Reddi,
A.H., 2006. Recombinant human BMP-7 effectively prevents nonunion in both young and old rats. J. Orthop. Res. 24, 11–20.
Hausman, M.R., Schaffler, M.B., Majeska, R.J., 2001. Prevention of
fracture healing in rats by an inhibitor of angiogenesis. Bone 29, 560–
564.
Hee, H.T., Wong, H.P., Low, Y.P., Myers, L., 2001. Predictors of
outcome of floating knee injuries in adults: 89 patients followed for 2–
12 years. Acta. Orthop. Scand. 72, 385–394.
Heiss, C., Keymel, S., Niesler, U., Ziemann, J., Kelm, M., Kalka, C.,
2005. Impaired progenitor cell activity in age-related endothelial
dysfunction. J. Am. Coll. Cardiol. 45, 1441–1448.
Hellstrom, M., Kalen, M., Lindahl, P., Abramsson, A., Betsholtz, C.,
1999. Role of PDGF-B and PDGFR-beta in recruitment of vascular
smooth muscle cells and pericytes during embryonic blood vessel
formation in the mouse. Development 126, 3047–3055.
Hollinger, J., Wong, M.E., 1996. The integrated processes of hard tissue
regeneration with special emphasis on fracture healing. Oral. Surg.
Oral. Med. Oral. Pathol. Oral. Radiol. Endod. 82, 594–606.
Huang, Y.C., Kaigler, D., Rice, K.G., Krebsbach, P.H., Mooney, D.J.,
2005. Combined angiogenic and osteogenic factor delivery enhances
bone marrow stromal cell-driven bone regeneration. J. Bone Miner.
Res. 20, 848–857.
Imai, Y., Terai, H., Nomura-Furuwatari, C., Mizuno, S., Matsumoto, K.,
Nakamura, T., Takaoka, K., 2005. Hepatocyte growth factor contributes to fracture repair by upregulating the expression of BMP
receptors. J. Bone Miner. Res. 20, 1723–1730.
Inoue, K., Ohgushi, H., Yoshikawa, T., Okumura, M., Sempuku, T.,
Tamai, S., Dohi, Y., 1997. The effect of aging on bone formation in
porous hydroxyapatite: biochemical and histological analysis. J. Bone
Miner. Res. 12, 989–994.
Kabasawa, Y., Asahina, I., Gunji, A., Omura, K., 2003. Administration of
parathyroid hormone, prostaglandin E2, or 1-alpha,25-dihydroxyvitamin D3 restores the bone inductive activity of rhBMP-2 in aged rats.
DNA Cell Biol. 22, 541–546.
R. Gruber et al. / Experimental Gerontology 41 (2006) 1080–1093
Kassem, M., Ankersen, L., Eriksen, E.F., Clark, B.F., Rattan, S.I., 1997.
Demonstration of cellular aging and senescence in serially passaged
long-term cultures of human trabecular osteoblasts. Osteoporos Int. 7,
514–524.
Kato, H., Matsuo, R., Komiyama, O., Tanaka, T., Inazu, M., Kitagawa,
H., Yoneda, T., 1995. Decreased mitogenic and osteogenic responsiveness of calvarial osteoblasts isolated from aged rats to basic
fibroblast growth factor. Gerontology 41 (Suppl. 1), 20–27.
Kawai, T., Murakami, S., Hiranuma, H., Sakuda, M., 1997. Radiographic
changes during bone healing after mandibular fractures. Br. J. Oral
Maxillofac. Surg. 35, 312–318.
Kloen, P., Di Paola, M., Borens, O., Richmond, J., Perino, G., Helfet,
D.L., Goumans, M.J., 2003. BMP signaling components are expressed
in human fracture callus. Bone 33, 362–371.
Kloss, F.R., Gassner, R., 2006. Bone and aging: effects on the maxillofacial skeleton. Exp. Gerontol. 41, 123–129.
Knopp, E., Troiano, N., Bouxsein, M., Sun, B.H., Lostritto, K.,
Gundberg, C., Dziura, J., Insogna, K., 2005. The effect of aging on
the skeletal response to intermittent treatment with parathyroid
hormone. Endocrinology 146, 1983–1990.
Komatsubara, S., Mori, S., Mashiba, T., Nonaka, K., Seki, A., Akiyama,
T., Miyamoto, K., Cao, Y., Manabe, T., Norimatsu, H., 2005. Human
parathyroid hormone (1–34) accelerates the fracture healing process of
woven to lamellar bone replacement and new cortical shell formation
in rat femora. Bone 36, 678–687.
Kon, T., Cho, T.J., Aizawa, T., Yamazaki, M., Nooh, N., Graves, D.,
Gerstenfeld, L.C., Einhorn, T.A., 2001. Expression of osteoprotegerin,
receptor activator of NF-kappaB ligand (osteoprotegerin ligand) and
related proinflammatory cytokines during fracture healing. J. Bone
Miner. Res. 16, 1004–1014.
Kugimiya, F., Kawaguchi, H., Kamekura, S., Chikuda, H., Ohba, S.,
Yano, F., Ogata, N., Katagiri, T., Harada, Y., Azuma, Y., Nakamura,
K., Chung, U.I., 2005. Involvement of endogenous bone morphogenetic protein (BMP)2 and BMP6 in bone formation. J. Biol. Chem.
280, 35704–35712.
Kveiborg, M., Rattan, S.I., Clark, B.F., Eriksen, E.F., Kassem, M., 2001.
Treatment with 1,25-dihydroxyvitamin D3 reduces impairment of
human osteoblast functions during cellular aging in culture. J. Cell
Physiol. 186, 298–306.
Lean, J.M., Davies, J.T., Fuller, K., Jagger, C.J., Kirstein, B., Partington,
G.A., Urry, Z.L., Chambers, T.J., 2003. A crucial role for thiol
antioxidants in estrogen-deficiency bone loss. J. Clin. Invest. 112, 915–
923.
Lean, J.M., Jagger, C.J., Kirstein, B., Fuller, K., Chambers, T.J., 2005.
Hydrogen peroxide is essential for estrogen-deficiency bone loss and
osteoclast formation. Endocrinology 146, 728–735.
Lehmann, W., Edgar, C.M., Wang, K., Cho, T.J., Barnes, G.L., Kakar,
S., Graves, D.T., Rueger, J.M., Gerstenfeld, L.C., Einhorn, T.A.,
2005. Tumor necrosis factor alpha (TNF-alpha) coordinately regulates
the expression of specific matrix metalloproteinases (MMPS) and
angiogenic factors during fracture healing. Bone 36, 300–310.
Leibovich, S.J., Ross, R., 1975. The role of the macrophage in wound
repair. A study with hydrocortisone and antimacrophage serum. Am.
J. Pathol. 78, 71–100.
Li, M., Ke, H.Z., Qi, H., Healy, D.R., Li, Y., Crawford, D.T.,
Paralkar, V.M., Owen, T.A., Cameron, K.O., Lefker, B.A., Brown,
T.A., Thompson, D.D., 2003. A novel, non-prostanoid EP2 receptor-selective prostaglandin E2 agonist stimulates local bone formation and enhances fracture healing. J. Bone Miner. Res. 18, 2033–
2042.
Li, X., Quigg, R.J., Zhou, J., Ryaby, J.T., Wang, H., 2005. Early signals
for fracture healing. J. Cell Biochem. 95, 189–205.
Lindahl, P., Johansson, B.R., Leveen, P., Betsholtz, C., 1997. Pericyte loss
and microaneurysm formation in PDGF-B-deficient mice. Science 277,
242–245.
Liu, L., DiGirolamo, C.M., Navarro, P.A., Blasco, M.A., Keefe, D.L.,
2004. Telomerase deficiency impairs differentiation of mesenchymal
stem cells. Exp. Cell Res. 294, 1–8.
1091
Liu, H., Kemeny, D.M., Heng, B.C., Ouyang, H.W., Melendez, A.J., Cao,
T., 2006. The immunogenicity and immunomodulatory function of
osteogenic cells differentiated from mesenchymal stem cells. J. Immunol. 176, 2864–2871.
Lu, C., Miclau, T., Hu, D., Hansen, E., Tsui, K., Puttlitz, C., Marcucio,
R.S., 2005. Cellular basis for age-related changes in fracture repair. J.
Orthop. Res. 23, 1300–1307.
Manolagas, S.C., 2000. Birth and death of bone cells: basic regulatory
mechanisms and implications for the pathogenesis and treatment of
osteoporosis. Endocr. Rev. 21, 115–137.
Martinez, M.E., Medina, S., Sanchez, M., Del Campo, M.T., Esbrit, P.,
Rodrigo, A., Martinez, P., Sanchez-Cabezudo, M.J., Moreno, I.,
Garces, M.V., Munuera, L., 1999. Influence of skeletal site of origin
and donor age on 1,25(OH)2D3-induced response of various osteoblastic markers in human osteoblastic cells. Bone 24, 203–209.
Martinez, P., Moreno, I., De Miguel, F., Vila, V., Esbrit, P., Martinez,
M.E., 2001. Changes in osteocalcin response to 1,25-dihydroxyvitamin
D(3) stimulation and basal vitamin D receptor expression in human
osteoblastic cells according to donor age and skeletal origin. Bone 29,
35–41.
Marx, R.E., 2004. Platelet-rich plasma: evidence to support its use. J. Oral.
Maxillofac. Surg. 62, 489–496.
Matsumoto, A., Yamaji, K., Kawanami, M., Kato, H., 2001. Effect of
aging on bone formation induced by recombinant human bone
morphogenetic protein-2 combined with fibrous collagen membranes
at subperiosteal sites. J. Periodontal. Res. 36, 175–182.
Meyer Jr., R.A., Tsahakis, P.J., Martin, D.F., Banks, D.M., Harrow,
M.E., Kiebzak, G.M., 2001. Age and ovariectomy impair both the
normalization of mechanical properties and the accretion of mineral by
the fracture callus in rats. J. Orthop. Res. 19, 428–435.
Meyer Jr., R.A., Meyer, M.H., Tenholder, M., Wondracek, S., Wasserman, R., Garges, P., 2003. Gene expression in older rats with delayed
union of femoral fractures. J. Bone Joint Surg. Am., 1243–1254.
Meyer Jr., R.A., Desai, B.R., Heiner, D.E., Fiechtl, J., Porter, S., Meyer,
M.H., 2006. Young, adult, and old rats have similar changes in mRNA
expression of many skeletal genes after fracture despite delayed healing
with age. J. Orthop. Res. 24, 1933–1944.
Mont, M.A., Ragland, P.S., Biggins, B., Friedlaender, G., Patel, T., Cook,
S., Etienne, G., Shimmin, A., Kildey, R., Rueger, D.C., Einhorn, T.A.,
2004. Use of bone morphogenetic proteins for musculoskeletal
applications. An overview. J. Bone Joint Surg. Am. 86-A (Suppl. 2),
41–55.
Murakami, S., Noda, M., 2000. Expression of Indian hedgehog during
fracture healing in adult rat femora. Calcif. Tissue Int. 66, 272–276.
Murasawa, S., Asahara, T., 2005. Endothelial progenitor cells for
vasculogenesis. Physiology (Bethesda) 20, 36–42.
Nagai, M.K., Embil, J.M., 2002. Becaplermin: recombinant platelet
derived growth factor, a new treatment for healing diabetic foot ulcers.
Expert Opin. Biol. Ther. 2, 211–218.
Nakazawa, T., Nakajima, A., Shiomi, K., Moriya, H., Einhorn, T.A.,
Yamazaki, M., 2005. Effects of low-dose, intermittent treatment
with recombinant human parathyroid hormone (1–34) on chondrogenesis in a model of experimental fracture healing. Bone 37, 711–
719.
Nelson, F.R., Brighton, C.T., Ryaby, J., Simon, B.J., Nielson, J.H.,
Lorich, D.G., Bolander, M., Seelig, J., 2003. Use of physical forces in
bone healing. J. Am. Acad. Orthop. Surg. 11, 344–354.
Nevins, M., Giannobile, W.V., McGuire, M.K., Kao, R.T., Mellonig,
J.T., Hinrichs, J.E., McAllister, B.S., Murphy, K.S., McClain, P.K.,
Nevins, M.L., Paquette, D.W., Han, T.J., Reddy, M.S., Lavin, P.T.,
Genco, R.J., Lynch, S.E., 2005. Platelet-derived growth factor
stimulates bone fill and rate of attachment level gain: results of a
large multicenter randomized controlled trial. J. Periodontol. 76, 2205–
2215.
Nicolas, V., Mohan, S., Honda, Y., Prewett, A., Finkelman, R.D.,
Baylink, D.J., Farley, J.R., 1995. An age-related decrease in the
concentration of insulin-like growth factor binding protein-5 in human
cortical bone. Calcif. Tissue Int. 57, 206–212.
1092
R. Gruber et al. / Experimental Gerontology 41 (2006) 1080–1093
Nieminen, S., Nurmi, M., Satokari, K., 1981. Healing of femoral neck
fractures; influence of fracture reduction and age. Ann. Chir. Gynaecol. 70, 26–31.
Nilsson, B.E., Edwards, P., 1969. Age and fracture healing: a statistical
analysis of 418 cases of tibial shaft fractures. Geriatrics 24, 112–117.
Nishimoto, S.K., Chang, C.H., Gendler, E., Stryker, W.F., Nimni, M.E.,
1985. The effect of aging on bone formation in rats: biochemical and
histological evidence for decreased bone formation capacity. Calcif.
Tissue Int. 37, 617–624.
Noth, U., Osyczka, A.M., Tuli, R., Hickok, N.J., Danielson, K.G., Tuan,
R.S., 2002. Multilineage mesenchymal differentiation potential of
human trabecular bone-derived cells. J. Orthop. Res. 20, 1060–1069.
O’Driscoll, S.W., Saris, D.B., Ito, Y., Fitzimmons, J.S., 2001. The
chondrogenic potential of periosteum decreases with age. J. Orthop.
Res. 19, 95–103.
Onishi, T., Ishidou, Y., Nagamine, T., Yone, K., Imamura, T., Kato, M.,
Sampath, T.K., ten Dijke, P., Sakou, T., 1998. Distinct and overlapping patterns of localization of bone morphogenetic protein (BMP)
family members and a BMP type II receptor during fracture healing in
rats. Bone 22, 605–612.
Owen, M., Friedenstein, A.J., 1988. Stromal stem cells: marrow-derived
osteogenic precursors. Ciba Found Symp. 136, 42–60.
Paralkar, V.M., Borovecki, F., Ke, H.Z., Cameron, K.O., Lefker, B.,
Grasser, W.A., Owen, T.A., Li, M., DaSilva-Jardine, P., Zhou, M.,
Dunn, R.L., Dumont, F., Korsmeyer, R., Krasney, P., Brown, T.A.,
Plowchalk, D., Vukicevic, S., Thompson, D.D., 2003. An EP2
receptor-selective prostaglandin E2 agonist induces bone healing.
Proc. Natl. Acad. Sci. USA 100, 6736–6740.
Park, J.E., Barbul, A., 2004. Understanding the role of immune regulation
in wound healing. Am. J. Surg. 187, 11S–16S.
Pfeilschifter, J., Diel, I., Pilz, U., Brunotte, K., Naumann, A., Ziegler, R.,
1993. Mitogenic responsiveness of human bone cells in vitro to
hormones and growth factors decreases with age. J. Bone Miner. Res.
8, 707–717.
Pfeilschifter, J., Diel, I., Scheppach, B., Bretz, A., Krempien, R.,
Erdmann, J., Schmid, G., Reske, N., Bismar, H., Seck, T., Krempien,
B., Ziegler, R., 1998. Concentration of transforming growth factor
beta in human bone tissue: relationship to age, menopause, bone
turnover, and bone volume. J. Bone Miner. Res. 13, 716–730.
Pfeilschifter, J., Diel, I., Kloppinger, T., Bismar, H., Schuster, E.M.,
Balbach, S., Ziegler, R., Baylink, D., Mohan, S., 2000. Concentrations
of insulin-like growth factor (IGF)-I, -II, and IGF binding protein-4,
and -5 in human bone cell conditioned medium do not change with
age. Mech. Ageing Dev. 117, 109–114.
Pittenger, M.F., Mackay, A.M., Beck, S.C., Jaiswal, R.K., Douglas, R.,
Mosca, J.D., Moorman, M.A., Simonetti, D.W., Craig, S., Marshak,
D.R., 1999. Multilineage potential of adult human mesenchymal stem
cells. Science 284, 143–147.
Quarto, R., Thomas, D., Liang, C.T., 1995. Bone progenitor cell deficits
and the age-associated decline in bone repair capacity. Calcif. Tissue
Int. 56, 123–129.
Rafii, S., Lyden, D., 2003. Therapeutic stem and progenitor cell
transplantation for organ vascularization and regeneration. Nat.
Med. 9, 702–712.
Raisz, L.G., 2005. Clinical practice. Screening for osteoporosis. N. Engl. J.
Med. 353, 164–171.
Ray, N.F., Chan, J.K., Thamer, M., Melton 3rd, L.J., 1997. Medical
expenditures for the treatment of osteoporotic fractures in the United
States in 1995: report from the National Osteoporosis Foundation. J.
Bone Miner. Res. 12, 24–35.
Reddi, A.H., 1985. Age-dependent decline in extracellular matrix-induced
local bone differentiation. Isr. J. Med. Sci. 21, 312–313.
Richardson, T.P., Peters, M.C., Ennett, A.B., Mooney, D.J., 2001.
Polymeric system for dual growth factor delivery. Nat. Biotechnol. 19,
1029–1034.
Riggs, B.L., Melton 3rd, L.J., 1995. The worldwide problem of
osteoporosis: insights afforded by epidemiology. Bone 17, 505S–
511S.
Riggs, B.L., Parfitt, A.M., 2005. Drugs used to treat osteoporosis: the
critical need for a uniform nomenclature based on their action on bone
remodeling. J. Bone. Miner. Res. 20, 177–184.
Riggs, B.L., Khosla, S., Melton 3rd, L.J., 2002. Sex steroids and the
construction and conservation of the adult skeleton. Endocr. Rev. 23,
279–302.
Risau, W., 1997. Mechanisms of angiogenesis. Nature 386, 671–674.
Rivard, A., Fabre, J.E., Silver, M., Chen, D., Murohara, T., Kearney, M.,
Magner, M., Asahara, T., Isner, J.M., 1999. Age-dependent impairment of angiogenesis. Circulation 99, 111–120.
Rosen, C.J., 2005. Clinical practice. Postmenopausal osteoporosis. N.
Engl. J. Med. 353, 595–603.
Salminen, S.T., Pihlajamaki, H.K., Avikainen, V.J., Bostman, O.M., 2000.
Population based epidemiologic and morphologic study of femoral
shaft fractures. Clin. Orthop., 241–249.
Schenk, R.K., Hunziker, E.B., 1994. Histologic and ultrastructural
features of fracture healing. In: Brighton, C.T., Friedlaender, G.,
Lane, J.M., (Eds.), Bone Formation and Repair. Rosemont, Illinois,
American Academy of Orthopaedic Surgeons 23, pp. 117–146.
Scheubel, R.J., Zorn, H., Silber, R.E., Kuss, O., Morawietz, H., Holtz, J.,
Simm, A., 2003. Age-dependent depression in circulating endothelial
progenitor cells in patients undergoing coronary artery bypass
grafting. J. Am. Coll. Cardiol. 42, 2073–2080.
Seck, T., Scheppach, B., Scharla, S., Diel, I., Blum, W.F., Bismar, H.,
Schmid, G., Krempien, B., Ziegler, R., Pfeilschifter, J., 1998. Concentration of insulin-like growth factor (IGF)-I and -II in iliac crest bone
matrix from pre- and postmenopausal women: relationship to age,
menopause, bone turnover, bone volume, and circulating IGFs. J.
Clin. Endocrinol. Metab. 83, 2331–2337.
Seeman, E., Delmas, P.D., 2006. Bone quality – the material and
structural basis of bone strength and fragility. N. Engl. J. Med. 354,
2250–2261.
Shiels, M.J., Mastro, A.M., Gay, C.V., 2002. The effect of donor age on
the sensitivity of osteoblasts to the proliferative effects of TGF(beta)
and 1,25(OH(2)) vitamin D(3). Life Sci. 70, 2967–2975.
Shi, S., Gronthos, S., Chen, S., Reddi, A., Counter, C.M., Robey, P.G.,
Wang, C.Y., 2002. Bone formation by human postnatal bone marrow
stromal stem cells is enhanced by telomerase expression. Nat.
Biotechnol. 20, 587–591.
Shimada, T., Takeshita, Y., Murohara, T., Sasaki, K., Egami, K.,
Shintani, S., Katsuda, Y., Ikeda, H., Nabeshima, Y., Imaizumi, T.,
2004. Angiogenesis and vasculogenesis are impaired in the precociousaging klotho mouse. Circulation 110, 1148–1155.
Shuster, S., 2005. Osteoporosis, a unitary hypothesis of collagen loss in
skin and bone. Med. Hypotheses 65, 426–432.
Simon, A.M., Manigrasso, M.B., O’Connor, J.P., 2002. Cyclo-oxygenase
2 function is essential for bone fracture healing. J. Bone Miner. Res.
17, 963–976.
Simpson, D.M., Ross, R., 1972. The neutrophilic leukocyte in wound
repair a study with antineutrophil serum. J. Clin. Invest. 51, 2009–
2023.
Skak, S.V., Jensen, T.T., 1988. Femoral shaft fracture in 265 children.
Log-normal correlation with age of speed of healing. Acta Orthop.
Scand. 59, 704–707.
Skoglund, B., Forslund, C., Aspenberg, P., 2002. Simvastatin improves
fracture healing in mice. J. Bone Miner. Res. 17, 2004–2008.
Smiell, J.M., Wieman, T.J., Steed, D.L., Perry, B.H., Sampson, A.R.,
Schwab, B.H., 1999. Efficacy and safety of becaplermin (recombinant
human platelet-derived growth factor-BB) in patients with nonhealing,
lower extremity diabetic ulcers: a combined analysis of four randomized studies. Wound Repair Regen. 7, 335–346.
Stenderup, K., Justesen, J., Eriksen, E.F., Rattan, S.I., Kassem, M., 2001.
Number and proliferative capacity of osteogenic stem cells are
maintained during aging and in patients with osteoporosis. J. Bone
Miner. Res. 16, 1120–1129.
Stenderup, K., Justesen, J., Clausen, C., Kassem, M., 2003. Aging is
associated with decreased maximal life span and accelerated senescence
of bone marrow stromal cells. Bone 33, 919–926.
R. Gruber et al. / Experimental Gerontology 41 (2006) 1080–1093
Stokstad, E., 2005. Bone quality fills holes in fracture risk. Science 308,
1580.
Strates, B.S., Stock, A.J., Connolly, J.F., 1988. Skeletal repair in the aged:
a preliminary study in rabbits. Am. J. Med. Sci. 296, 266–269.
Street, J., Bao, M., deGuzman, L., Bunting, S., Peale Jr., F.V., Ferrara, N.,
Steinmetz, H., Hoeffel, J., Cleland, J.L., Daugherty, A., van Bruggen, N.,
Redmond, H.P., Carano, R.A., Filvaroff, E.H., 2002. Vascular endothelial growth factor stimulates bone repair by promoting angiogenesis
and bone turnover. Proc. Natl. Acad. Sci. USA 99, 9656–9661.
Stromsoe, K., 2004. Fracture fixation problems in osteoporosis. Injury 35,
107–113.
Suh, W., Kim, K.L., Kim, J.M., Shin, I.S., Lee, Y.S., Lee, J.Y., Jang,
H.S., Lee, J.S., Byun, J., Choi, J.H., Jeon, E.S., Kim, D.K., 2005.
Transplantation of endothelial progenitor cells accelerates dermal
wound healing with increased recruitment of monocytes/macrophages
and neovascularization. Stem Cells 23, 1571–1578.
Swift, M.E., Kleinman, H.K., DiPietro, L.A., 1999. Impaired wound
repair and delayed angiogenesis in aged mice. Lab. Invest. 79, 1479–
1487.
Szpaderska, A.M., Egozi, E.I., Gamelli, R.L., DiPietro, L.A., 2003. The
effect of thrombocytopenia on dermal wound healing. J. Invest.
Dermatol. 120, 1130–1137.
Tanaka, M., Sakai, A., Uchida, S., Tanaka, S., Nagashima, M.,
Katayama, T., Yamaguchi, K., Nakamura, T., 2004. Prostaglandin
E2 receptor (EP4) selective agonist (ONO-4819.CD) accelerates bone
repair of femoral cortex after drill-hole injury associated with local
upregulation of bone turnover in mature rats. Bone 34, 940–948.
Tarkka, T., Sipola, A., Jamsa, T., Soini, Y., Yla-Herttuala, S., Tuukkanen, J., Hautala, T., 2003. Adenoviral VEGF-A gene transfer induces
angiogenesis and promotes bone formation in healing osseous tissues.
J. Gene Med. 5, 560–566.
1093
Termaat, M.F., Den Boer, F.C., Bakker, F.C., Patka, P., Haarman, H.J.,
2005. Bone morphogenetic proteins. Development and clinical efficacy
in the treatment of fractures and bone defects. J. Bone Joint Surg. Am.
87, 1367–1378.
Turk, C., Halici, M., Guney, A., Akgun, H., Sahin, V., Muhtaroglu, S.,
2004. Promotion of fracture healing by vitamin E in rats. J. Int. Med.
Res. 32, 507–512.
Vortkamp, A., Pathi, S., Peretti, G.M., Caruso, E.M., Zaleske, D.J.,
Tabin, C.J., 1998. Recapitulation of signals regulating embryonic bone
formation during postnatal growth and in fracture repair. Mech. Dev.
71, 65–76.
Wang, H.L., Boyapati, L., 2006. ‘‘PASS’’ principles for predictable bone
regeneration. Implant Dent. 15, 8–17.
Wang, X., Li, X., Shen, X., Agrawal, C.M., 2003. Age-related changes of
noncalcified collagen in human cortical bone. Ann. Biomed. Eng. 31,
1365–1371.
Wehren, L.E., 2003. The epidemiology of osteoporosis and fractures in
geriatric medicine. Clin. Geriatr. Med. 19, 245–258.
Westesson, P.L., Lee, R.K., Ketkar, M.A., Lin, E.P., 2002.
Underdiagnosis and undertreatment of osteoporosis. Lancet 360,
1891.
Yancopoulos, G.D., Davis, S., Gale, N.W., Rudge, J.S., Wiegand, S.J.,
Holash, J., 2000. Vascular-specific growth factors and blood vessel
formation. Nature 407, 242–248.
Zhang, X., Schwarz, E.M., Young, D.A., Puzas, J.E., Rosier, R.N.,
O’Keefe, R.J., 2002. Cyclooxygenase-2 regulates mesenchymal cell
differentiation into the osteoblast lineage and is critically involved in
bone repair. J. Clin. Invest. 109, 1405–1415.
Zioupos, P., Currey, J.D., Hamer, A.J., 1999. The role of collagen in the
declining mechanical properties of aging human cortical bone. J.
Biomed. Mater. Res. 45, 108–116.