Endoscopic resection of the olfactory cavity
advertisement

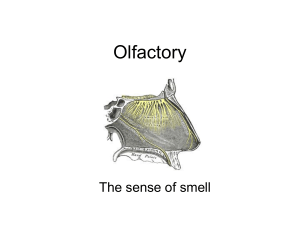
SCIENTIFIC COMMUNICATION Endoscopic resection of the olfactory cavity Roger Jankowski Service O.R.L. et Chirurgie Cervico-Faciale, C.H.U. - Hôpital Central - Nancy ABSTRACT The development or extension of malignant neoplasms into the olfactory cavity of the nasal fossa can be approached by a technique of endoscopic endonasal surgery that we describe in the present article. A complete and carcinologic resection of the olfactory cavity appeared possible in three esthesioneuromas and twenty six adenocarcinomas. The dissection of the mucosa covering the cribriform plate, after section of the olfactory fibers, lead inconstantly to minor CSF leaks that fade most of the times before the end of the procedure. Only one patient needed revision surgery to close a persisting CSF leak. No one developed meningitis after a follow-up of six months to six years. Endoscopic resection of the olfactory cavity represents an innovative technique in the field of endonasal endoscopic surgery. It can be transformed in endoscopic endonasal craniofacial resection, if necessary. (Presented on September 2005 at Congress NOSE, Porto and on Mai 2006 at the Congress of Mexican Society of ENT, Accapulco) (Fr ORL-2007;93:341-346) Key words: Olfactory cleft, Endonasal endoscopic surgery, Malignant neoplasms of the nose and sinuses, Cribriform plate, Conchal lamina of the ethmoïdal bone, Ethmoid. Submitted for publication: Mai 2006 Accepted for publication: November 2007 Corresponding author: Roger Jankowski S e rvice O.R.L. et Chiru rgie Cervico-Fa c i a l e, C . H . U. – Hôpital Central 29 ave nue du Mal de Lat t rede Ta s s i g ny 54035 Nancy Cedex e-mail: r.jankowski@chu-nancy.fr 341 - Fr ORL - 2007 ; 93 Endoscopic resection of the olfactory cavity INTRODUCTION The turbinate wall of the ethmoid [1] and the adjacent part of the nasal septum limits an air-filled narrow and vertical cavity called the olfactory groove [2]. This cavity connects with the nasal fossae via its base and it is closed above by the cribiform plate of the ethmoid bone, behind by the anterior surface of the sphenoid bone, and in front by the roof of the nasal bones. It forms an olfactory air reservoir situated above the nasal fossa through which respiratory airflow occurs. Endoscopic surgery of the olfactory groove has received little attention to date apart from the controversial resection of the middle nasal concha [3] or the resection of inflammatory polyps [4]. The olfactory grove is currently an area that is off-limits for endonasal endoscopic surge ry, particularly its superior part which is in contact with the cribiform plate. The aim of the article is to describe a controlled surgical excision of the olfactory cavity after tumor development or invasion. Detachment of the olfactory mucosa of the cribiform plate after sectioning of olfactory fibres makes this intervention possible. Endoscopic excision of the olfactory cavity appears to be an innovative technique which could be added to the current list of endonasal interventions. Our experience with this technique currently includes three olfactory esthesioneuromas and 26 adenocarcinomas. DESCRIPTION OF THE TECHNIQUE We limit the description to cases of unilateral tumors without intracranial extension at preoperative imaging. The intervention takes place within the standard setting of endonasal endoscopic surgery. The reduction of tumor volume by removing the non-invasive free portion of the tumor in the nasal fossa is usually required to identify the limits of excision of normal tissue. Dissection of the septal wall A healthy region of the septal mucosa is incised at a distance of at least 5 mm from the tumor margins down to the level of bone or cartilage with the aid of a Beaver® lancet. A first incision, parallel to the floor of the nasal fossa, is performed from back to front, a second frontal incision is made from top to bottom to join perpendicularly with the first. The mucosa delineated between these two incisions is raised to the subperichondrial-subperiostal level as far as the posterior edge of vomer and anterior surface of the sphenoid bone behind, and to the cribiform plate above. The olfactory fibres are incorporated within the mucosal layer and do not delay dissection; in contrast progression could be impeded if tumoral invasion of the plane of dissection is discovered at this stage. If the contralateral mucosa of the olfactory cavity is macroscopically normal, it is possible to widen the septal dissection to the point of septal resection; but rather than persisting with the intervention, rather, it is worth reconsidering surgery for bilateral tumors of olfactory cavities. Dissection of internal orbital wall [5] The ethmoid bone is a buffer zone interposed between the olfactory cavity and the internal orbital wall, which offers a margin of tumor dissection when the external or orbital ethmoid cells appear not to be invaded on preoperative imaging. Unciformectomy permits the ex p o s u re of the maxillary ostium, from wh i ch a a large middle meat o t o my is p e r fo rmed from front to back to the palatine bone and f rom bottom to top between the superior edge of the i n fe rior nasal concha and the roof (wh i ch is also the floor of the orbit). The subperiostal dissection of the i n t e rnal wall of the orbit can be perfo rmed from bottom to top from the level of the roof of the maxillary sinus. Advancing the dissection of the compartment of u n c i fo rmcells situated at the anterior- s u p e rior angle of the ethmoid box is fa c i l i t ated by seeking the subperiostal plane ahead of the ethmoid box, on the rising ap o p hysis of the maxillary bone. Sphenoidotomy is p e r fo rmed systemat i c a l ly as it offe rs two points of i n t e rest: it allows the confi rm ation, if re q u i re d, of the l o c ation of the ethmoid roof and the internal wall of the orbit to their posterior parts, and as a result it permits the safe completion of the excision of cells of the anterior-superior angle of the ethmoid box and go o d identification of the cells of Onodi and frequent relief of the optical canal. The bony infra s t ru c t u re of the i n t e rnal wall of the orbit can be also dissected sub-peri o s t i a l lyalong its entire surface in total safe t y. Dissection of the ethmoid roof This starts in normal tissue in contact with the internal wall of the orbit; and is performed subperiosteally from the frontal ostium to the orifice of the sphenoidotomy. The dissection of its internal half can be relaFr ORL - 2007 ; 93 : 342 Endoscopic resection of the olfactory cavity Figure 1: Anatomy of the ceiling of the olfactory groove in sagittal section [10] The ceiling of the olfactory groove presents three segments distinguished by their orienta tion: the anterior oblique segment above and behind formed by the inferior surface of the nasal and frontal bones; a middle horizontal segment formed by the cribiform plate of the ethmoid and the ethmoidal process of the sphenoid; a posterior segment, initially verti cal and then oblique downwards and back wards, formed by anterior surface of the sphe noid to the opening of the sphenoid ostium. tively delicate depending on the presence or absence of tumoral invasion, but when preoperative imaging shows the absence of intracranial extension the technique of endoscopic subperiostal dissection offers a margin of oncologic safety at least comparable with excision using the para-latero-nasal approach. The aim of the dissection of the ethmoid roof is to find the inner surface of Mouret’s conchal plate (Figure 3) along its entire length or in part if it has been destroyed by the tumor. The junction of the ethmoidal roof and the conchal plate is carefully dissected in the subperiosteum. Dissection of the cribriform plate and excision of the olfactory groove If it has not already been performed, the resection of the middle concha is performed at this stage; this facilitates access to the olfactory cavity. With the help of a Beaver® lancet the frontal incision of the septal 343 - Fr ORL - 2007 ; 93 Figure 2: Anatomy of the lateral wall of the right nasal fossa and the turbinate wall of the right ethmoid [1] The turbinate wall of the ethmoid consists of superiorly a continuous bony plate (Mouret’s conchal plate) suspended at the junction of the cribiform plate and the ethmoidal roof, from which it detaches from front to back the middle, inferior and eventually superior turbi nates, which between them demarcate the meatuses of the name. Figure 3: Mouret’s conchal plate continues above the cribriform plate as the lateral plate of the intracranial olfactory groove which makes the junction with the roof of the lateral mass of the ethmoid. mucosa is prolonged diagonally under the nasal bone, then outside on the rising apophysis of the maxilla coming down to the level of the resection line of the middle concha. The detachment of the mucosa from the inferior surface of the nasal bone and the maxillary apophysis is Endoscopic resection of the olfactory cavity Figure 4: Anatomy of the endocranial surface of the cribriform plate [2] Foramina of the cribriform plate allow the p a s s age of the olfa c t o ry nerves, with the exception of two orifices situated at its ante rior extremity: the ethmoidal groove, which is situated opposite to the apophysis of the cris ta galli; ethmoidal foramen which is located outside of the ethmoidal groove allows the passage of the internal nasal nerve, a branch of optic nerve, which accompanies the ante rior ethmoidal artery in its path and separates from it later at the internal orifice of the ante rior ethmoidal canal to follow the ethmoidal groove and rejoin the ethmoid foramen. performed in the subperiosteum to rejoin the subperichondrial plane of detachment on the septum. The subperiostial dissection of the anterior oblique segment of the ceiling of the olfactory groove (Figure 1) does not present any difficulty; arrival at the cribiform plate (Figure 4) is indicated by the emergence across the ethmoid of the internal nasal nerve which arises as a resistant cord preventing the progress of submucosal detachment. After section of this nerve using a curved micro-scissors the detachment of the mucosa of the cribriform plate is again easy for one to two millimetres, the point where the first olfactory fibres are encountered. The extension of dura mater of the ethmoid groove (Figure 4) does not seem often affect the inferior surface of the cribriform plate, as it has never been an obstacle to the progression of the mucosal detachment or the source of a CSF leak. The olfactory fibres are much thinner than the internal nasal nerve and can be arranged 2 randomly or in two rows which emerge on the inferior surface of the cribriform plate, one internal row in contact with the septum and an external row along Mouret’s conchal plate (Figure 4). The olfactory fibres are easily cut or pulled with a sharp Blakesley forceps, which does not in general lead to an endoscopically visible CSF leak. However, pulling seems to be a gre ater risk for a CSF leak due to connections between olfa c t o ry fibres and the meninges. The detachment of the mucosa on the inferior surface of the cribriform plate does not present any resistance in areas apart from the emergence of the olfactory fibres and progresses easily at the rate they are sectioned to the level of the septum-cribriform plate junction. The section of Mouret’s conchal plate (Figure 2) from the cribriform plate is facilitated if it is fractured before by internal dislocation, this dislocation reveals the olfactory fibres and it is sufficient to cut these in order to detach the conchal plate step by step from front to back. Meanwhile, it is necessary to keep in mind from the scan images of the patient, that the ethmoidal roof is situated above the plane of the cribriform plate, particularly in front. Fracturing by internal dislocation of the lateral plate (figure3) leads to intracranial damage with not only a CSF leak but also the risk of a haematoma in case of an associated lesion of the ethmoidal artery. The dissection of the cribriform plate ends behind by meeting the anterior sphenoidal surface. In favourable cases, the olfatory cavity excision could be performed in one piece. Perioperative wound-dressing and care In the absence of a visible CSF leak the cribriform plate and ethmoidal roof are coated with 2 ml of biological glue to which a compress of Surgicel ® is applied. The cavity does not receive any other packing. The patient can leave the department after 48 hours of perfused antibiotic prophylaxis (the protocol is copied from that of neurinoma surgery). Postoperative care is that of endonasal surgery, and the surgical intervention is integrated into a protocol of combined care adapted to the tumor pathology. The management of a visible CSF leak is handled using classical filling techniques. DISCUSSION The excision of malignant sinus tumors by the endoscopic endonasal ap p ro a ch remains controversial. Fr ORL - 2007 ; 93 : 344 Endoscopic resection of the olfactory cavity Figure 5: Endoscopic view of the left operative cavity at the end of an excision. Figure 6: MRI appearance of an adenocarcinoma of the left olactory groove (a) and postoperative follow up after one year (b). a Rsm = Resection of septal mucosa; Fs = Frontal sinus; Cp = Cribiform plate; Te = Roof of the ethmoid; Sph = Sphenoid; Po = Wall of the orbit b CSF flow in seven patients, of whom six had spontaneous drying in intra-operative period. None of the patients had postoperative meningitis after a followup period of between 6 months and 6 years. All were irradiated. CONCLUSION The recent publication by Goffart et al [6] in 78 patients and that of Lund et al [7] in 49 patients, however, seriously strengthen the arguments in favour of an endoscopic approach: the follow-up periods of 3 to 5 years are at least equal to those published for external approaches. Our experience also shows promising results, although the endoscopic approach has mostly permitted us to identify limiting factor for this approach, which is the dissection of the tumor developed in or extending to the olfactory groove. The aim of this publication is not to report our oncologic results as our series is too small and without sufficient follow-up for the majority of our patients. The object is to present an innovative surgical approach for the excision of malignant tumors that have developed in or extending to the olfactory groove, but without endocranial invasion. Our technique could be completed, if necessary, according to intra-operative findings regarding intracranial invasion, by endoscopic resection of the skull base [8,9]. The excision of the olfactory cavity does not increase surgical trauma and does not modify classical operative results of ethmoidal surgery. Several of our patients who had advanced age or fragile general health have tolerated the procedure without difficulties. Only one of our patients had a CSF leak, which required a second surgery. The section of olfactory fibres has lead to visible 345 - Fr ORL - 2007 ; 93 The dissection of the cribriform plate and the excision of the olfactory cavity by the endoscopic endonasal approach could be performed using a codified surgical protocol that was not accompanied by particular neuro-meningeal risk. This technique necessitates, however, solid experience in endonasal endoscopic surgery and the respect of rules of medical management of malignant tumors in keeping with a multi-disciplinary approach. REFERENCES 1. Bodino C, Jankowski R, Grignon B, JimenezChobillon A, Braun M. Surgical anatomy of the turbinal wall of the ethmoidal laby rinth. Rhinology. 2004;42:73-80. 2. Rouvière H. Anatomie humaine. Paris: Masson. 1974. 3. Kennedy DW. Middle turbinate resection: evaluating the issues-should we resect normal middle turbinates? Arch Otolaryngol Head Neck Surg. 1998;124:107. 4. Masaki M, Tanaka Y. Nasal polyps in the olfactory cleft. Laryngoscope. 1998;108:1243-1246. 5. Ja n kowski R. La nasalisation. In: Fre che C, Fontanel J, Peynegre R, editors. La polypose n a s o - s i nu s i e n n e. Pa ris: Soc Fr ORL et CCF. 2000:246-255. Endoscopic resection of the olfactory cavity 6. Goffart Y, Jorissen M, Daele J, et al. Minimally invasive endoscopic management of malignant sinonasal tumours. Acta Otorhinolaryngol Belg. 2000;54:221-232. 7. Lund V, Howa rd DJ, Wei WI. Endoscopic resection of malignant tumors of the nose and sinuses. Am J Rhinol. 2007;21:89-94. 8. Castelnuovo PG, Belli E, Bignami M, Battaglia P, Sberze F, Tomei G. Endoscopic nasal and anterior craniotomy resection for malignant nasoethmoid tumors involving the anterior skull base. Skull Base. 2006;16:15-18. 9. Yuen AP, Fung CF, Hung KN. Endoscopic cranionasal resection of anterior skull base tumor. Am J Otolaryngol. 1997;18:431-433. 10. Legent F, Perlmuter L, Vandenbrouck C. Cahiers d'anatomie ORL, 3ème édition ed. Paris: Masson. 1981:133. Fr ORL - 2007 ; 93 : 346