The Action Of Iliopsoas Muscle In The
advertisement

THE
ACTION
THE
OF
ILIOPSOAS
B. MCKIBBIN,
The
standard
is flexion
anatomical
of the
action,
hip
although
there
(1958)
Basmajian
found
medial
texts
joint.
At
reviewed
1948,
Gray
1949,
same
time
agreement
the
opinion
to be almost
or of lateral
rotation
(Grant
SHEFFIELD,
are unanimous
the
is less
MUSCLE
literature
equally
at the
that
the primary
the
credited
Last
to
long-standing
this
1963).
head
condyles
the
insertion
rotation,
although
attempted
of the
of the
the
that
along
its long
axis
(Fig.
muscle
must
therefore
be very
powerful.
movement
will
iliacus
muscle
rotary
occurs.
controversy
pointed
of the
of the
muscle
rotation
this
might
suggest
of the femur
and
out
that
although
that the pull of the
passes
through
the
9) so that
it lies
give
rise
medial
to medial
Basmajian
by electromyography
1
(1958)
but
he was
2
FIG.
to associate
suggested
not
such
role
pelvis
ofa child with
hip held in the most
increase
in medial
consistently
he
that
functional
FIG.
basis
and
Shortening
it is unlikely
to assess
Radiographs
ofthe
operation,
with the
there
is a considerable
unable
bone
tendon.
psoas
secondary
secondary
action
was one of
texts favour
medial
rotation
It is usually
and medial
location
of the lesser
trochanter
result
in lateral
rotation,
the axis of rotation
and
ofthe
some
in which
the posterior
muscle
would
to the
action
direction
in relation
1956,
NEWBORN
with
divided
as to whether
the
hip.
Most
of the English
Cunningham
THE
ENGLAND
it is usually
about
IN
spina
bifida
and paralytic
dislocation
ofthe
right
hip.
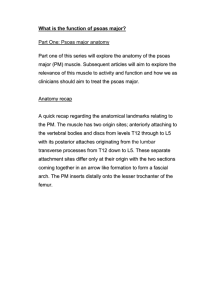
Figure
1-Before
medial
rotation
possible.
Figure
2-After
division
of the psoas
tendon
rotation
possible,
indicated
here by the apparent
increase
in the neckshaft
angle.
The hip is reduced.
electrical
whatever
the
activity
with
anatomical
rotation
action
of
in either
the
direction.
muscle
might
be,
On
this
it had
no
functional
value
as a rotator
of the hip, and he proposed
that
the entire
controversy
be
abandoned.
This attitude
is reflected
in more
recent
editions
of some of the above
reference
works
(Gray
1962, Grant
and Basmajian
1965).
It might
seem that the argument
has degenerated
to the level of anatomical
hair splitting,
but clinical
studies
reveal
that the rotary
action
of the muscle
is of considerable
functional
Thus,
significance.
of medial
paralytic
in
which
well
so
is often
dislocation
of the
the
into
that
L
lay
hip.
in fixed
rotation
conditions
improved
Figure
lateral
and
in which
after
1 shows
rotation.
the
the
its division,
such
Division
dislocation
was
psoas
and
is abnormally
this
a dislocation
of the
reduced
may
the
action
NO.
I,
of
FEBRUARY
the
psoas
1968
becomes
one
of
lateral
rotation.
short
aid
the
resulting
psoas
(Fig.
enabled
2).
the
This
However,
the
range
reduction
from
with caution
because
Somerville
(1959)
pointed
out that when
valgus
of the neck is extreme
the axis of rotation
now runs along
50 B,
VOL.
leg
medial
interpreted
or when
in pathological
rotation
of a
spina
leg
bifida
to
finding
be
must
put
be
the hip is dislocated
the shaft of the bone
improvement
in
161
162
B.
the
range
of medial
rotation
after
psoas
MCKIBBIN
division
is commonly
seen
even
when
the
hip
is not
dislocated
(Figs.
3 and 4) and it is hard
to escape
the conclusion
that the muscle
is a true
lateral
rotator.
This belief
is further
strengthened
by the observation
that during
operative
exposure
of the psoas
from the front the access to it is greatly
facilitated
by flexing
and laterally
rotating
the thigh,
which
causes
the lesser trochanter
to present
more anteriorly
and
off the tendon.
This was recommended
by both
Mustard
(1959)
and by Sharrard
in describing
their respective
operations
of psoas
transplantation.
There
is a conflict
therefore
between
the evidence
from anatomical
and clinical
Because
very
the
clinical
young
children
associated
with
muscle
evidence
it is possible
their
in newborn
the
increase
with
in the most
in the
from
the
difference
It was
decided
during
to anatomical
observations
is attributable
therefore
to
investigate
studies.
operations
on
peculiarities
made
the
action
of the
children.
of a child
hip is held
mostly
that
immaturity.
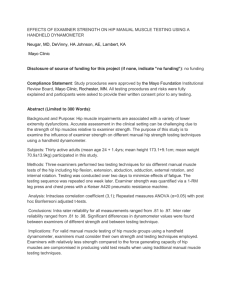
3
FIG.
Radiographs
is derived
slackens
(1964)
amount
4
FIG.
slight
subluxation
of the
rotation
possible.
medial
of medial
rotation
possible
left
hip
who
Figure
and
this
had
spina
bifIda.
4-Immediately
is shown
Figure
after
by an
apparent
3-Before
psoas
operation
division
increase
in
there
the
is an
neck-shaft
angle.
MATERIAL
The
entire
pelvis
infants
who
to
musculo-skeletal
any
had
bilateral
congenital
examination.
The
The
muscles
and
died
were
both
within
positions
with
first
METHODS
associated
weeks
One
child
muscles
of life
was
from
found
were
causes
on
except
for
the
psoas
was not disturbed.
psoas
by pulling
noting
the
tension
and
iliacus
subsequent
and
With the resulting
it in its long axis,
in the
obtained
thought
of the hip and was excluded,
leaving
were dissected
in the fresh condition
removed
while
the
eight
pathology.
dislocation
specimens
the capsule
of the hip joint
to assess
the action
of the
various
femora
the
AND
be
dissection
a total
on the
their
from
to
sixteen
unrelated
to
have
of thirty
hips for
day of necropsy.
conjoined
tendon,
but
preparation
it was possible
and by putting
the hip into
muscle.
RESULTS
In all the
became
flexed
muscle
was
amount
of
specimens,
when
and laterally
tightened
(Fig.
flexion
became
very much
the tendon
round
was
the
psoas
was
pulled
in the
direction
rotated
(Fig.
5).
Again,
when
the hip
6) while
in lateral
rotation
it became
unchanged.
more pronounced
the femur
almost
When
the
limb
was
abducted
(Fig. 7). In this position
like a windlass,
so that
THE
of the
tendon
the
was medially
rotated
slack
provided
that
the
lateral
rotation
hip
the
the
action
medial
rotation
served
to wind
if the muscle
was to contract
in
JOURNAL
OF
BONE
AND
JOINT
SURGERY
THE
this
position
was
most
fully
“
position
.‘
frog
very
ACTION
powerful
relaxed
OF
THE
lateral
ILIOPSOAS
rotation
was in full abduction,
(Fig.
would
flexion
IN THE
result.
and
The
lateral
5-Dissection
5
showing
effect
of traction
position
in
rotation-that
FIG. 6
on the psoas
direction
of its tendon.
The
hip has become
flexed
Figure
6-Dissection
showing
the effect
of internally
hip.
The
iliopsoas
muscle
has
been
rendered
tight
/
which
the
psoas
is, in the so-called
muscle
p
8
FIG.
Figure
7-Dissection
showing
the effect
wound
up round
the upper
end of the
abduction
and external
rotation.
The
iliacus
in the
and
laterally
rotated.
rotating
the extended
by this
manoeuvre.
7
FIG.
163
NEWBORN
8).
FIG.
Figure
MUSCLE
of medial
rotation
on the abducted
hip.
The psoas
femur
and tightened
thereby.
Figure
8-Specimen
iliopsoas
muscle
is at its most
slack
in this position.
portion
as an abductor
can
be seen.
muscle
showing
The
has become
the hip in
role of the
DISCUSSION
is
to
It is clear
from
flex
laterally
and
the foregoing
the trunk
this secondary
becomes
a powerful
lateral
situation
in the adult
hip.
In considering
to account
for the
of rotation
VOL.
50 B,
I,
FEBRUARY
that
hip.
the action
of the
In the anatomical
iliopsoas
muscle
position
with
rotary
action
is weak,
but with the thigh
rotator.
It remains
to attempt
to reconcile
the action
difference
of an adult
NO.
the
rotate
femur
1968
of the
between
has
been
psoas
the
with
adult
constructed
the limb
and the
in the
neonatal
by joining
in the newborn
infant
the thigh
in line with
abducted
the
these findings
anatomical
state.
the
centre
position
In Figure
of the
head
iliopsoas
with the
it is easy
9 the axis
with
the
164
B.
McKIBBIN
centre
of the femoral
well medial
to the
condyles.
This axis passes
lesser
trochanter
so that
the
psoas,
the
which
pulls
trochanter
forward,
must
necessarily
medially
rotate
the limb.
In the case
of the neonatal
femur,
however,
when the axis of
rotation
is constructed
in the same way it passes
directly
in
very
neck.
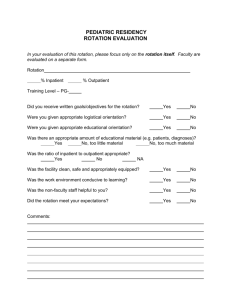
9
FIG.
of rotation.
The axis
of
two
femora
showing
On the left is shown
the
an adult
passes
well
medial
to the
the right
is the femur
from
a newborn
infant.
The axis of rotation
passes
almost
directly
in front
of the lesser
trochanter.
line
of pull
mechanical
Out
is farther
away
from
the
the
with
of rotation
trochanter.
On
lesser
psoas
that
axis
Figure
of the
movement,
a
better
fulfilled
of movement;
axis
is
of
femoral
an
the
oversimpli-
the
action
so that when
it shortens
it
femur
around
the indicated
is very much more obvious
as in Figure
7, for here the
is much altered
in relation
of rotation.
8 also shows
as an abductor
this
it
because
of the
by drawing
a line from
its origin
to
as is commonly
done.
The tendon
is
but winds
in a spiral
manner
round
straight
to
axis
femur.
length
diagrammatically
the neck of the femur
unrolls,
as it were, the
axis of rotation.
This
with the hip abducted
line of pull ofthe
psoas
II
aspect
trochanter
7 shows
insertion
not
the
relative
to represent
of the
its
of
shorter
Figure
fication
Anterior
front
much
This illustration
how the muscle
hip
towards
function
by the
indeed
together
can act
the extreme
which
is
iliacus
portion
in this position
very
of
much
of which
the
it enjoys
a
advantage
at least as great
as that of the gluteal
abductors
themselves.
this confusion
of anatomical
facts
it is desirable
to attempt
to discern
some
purposeful
pattern
in the construction
ofthe
iliopsoas
muscle
complex.
It seems extraordinary
on
the face of it that a muscle
should
have an action
in the newborn
child which
is reversed
by the time it has reached
maturity.
Basmajian
(1958)
dismissed
the problem
by regarding
the
of
secondary
rotary
it operated,
but
maintaining
fixed
action
this
of
that
concentrated,
position.
medial
apply
rotational
It is submitted
have
as of such
cannot
quite
small
to
deformity
the
abducted
has
been
confusion
properly,
on
account
the
arises
out
muscle
position
the
that
in the
abducted
breaks
down
even
in the
in
relation
to
the
axis
adult,
of
because
It
muscle
as a flexor
and lateral
rotator,
trochanter.
It is true that when the
which
accords
limb is adducted
and if the femoral
neck
has a theoretical
medial
or valgus
However,
extremely
poor
that
position
this
actions
to
obscure
plays
congenital
described,
role
in
but
paralytic
dislocation.
A stable
position
effect
as a medial
correspond
with
this
It is important
reduction
into
one
of
Lorenz,
of
dislocation
of a paralytic
two
or
positions,
in abduction,
that
dislocation
abduction,
extension
the
1 and
2).
that
line
be
may
hip
details
and
of
hip
and
medial
can
rotation.
THE
JOURNAL
in favour
muscle
to
reached
advantage
is so
regard
the
where
the muscle
in this position
is
It is unfortunate
which
in
should
not
The
iliopsoas
considerable
should
usually
lateral
texts
location
of the lesser
action
gradually
wanes,
position
of its action
of the
flexion
is
in
anatomical
of the
therefore,
convention
and
psoas
argument
of pull
a lateral
rotator.
ancient
controversy.
the
in the
be discounted.
“
direction
short
anatomical
limb
conventional
anatomical
“
the
is simpler,
of anatomical
of
the
in which
of
with the posterior
this secondary
rotator
the
detail
fact
with
a position
may
the mechanical
the fact that the muscle
is functionally
apology
is offered
for reawakening
this
a vital
leg
short
action.
its functional
should
are normally
No
the
and
is not
rotary
of the
the
rotation.
matter
role
(Figs.
of the
7 shows
not
the
demonstrated
action
Figure
altered
it did
and
largely
the
rotation
profoundly
that
hip,
be fully
the
If the
OF
BONE
muscle
muscle
importance
be achieved
rotation,
all
be allowed
former
AND
in
known.
by putting
so-called
first
position
JOINT
SURGERY
is
THE
chosen
the
psoas
reduction
the danger
rapidly
will
become
OF THE
be at its most
it will be offered
of maintaining
fixed
gluteal
abductors
the iliacus
could
in fixed
ACTION
At
paralysed
and
lateral
MUSCLE
and
while
opportunity
hip in this
in abduction.
be responsible
flexion
slack,
the greatest
a paralysed
also
are
ILIOPSOAS
first
in this
while
the
it will
therefore
this
remainder
seems
of
provide
Sharrard
too long
difficult
of dislocation,
but
the
I 65
NEWBORN
to shorten.
position
for
sight
type
IN THE
no
(1964)
because
obstacle
to explain
Figures
shortened
7 and
muscle
to
pointed
out
the leg may
because
the
8 show
how
holds
the
limb
rotation.
Immobilisation
in the extended
medially
rotated
position
on the other
hand
means
that
psoas
is tightened,
so that if it should
be abnormally
short
it may be impossible
to get
thigh
into enough
extension
and medial
rotation
to make
reduction
possible
unless
the
the
the
psoas
is divided
as in the child illustrated
in Figures
1 and 2. If the hip can be immobilised
in this position
without
dividing
the psoas
it has less opportunity
for shortening.
It should
be made
clear that, although
the secondary
actions
of the iliopsoas
muscle
are
of considerable
significance
in the mechanism
of deformity
it cannot
be taken
to mean
that
they are of functional
significance
in normal
use.
Because
the muscle
is capable
of laterally
rotating
the abducted
information
we have
thigh
does
about
normal
Keagy,
Bergan
Brumlik
and
not imply
function
1966),
and
that it is ever used for this
derives
from electromyography
this
suggests
that
the
muscle
purpose.
The only
(Basmajian
1958;
serves
as a flexor
only.
SUMMARY
1 . Dissections
of the newborn
child revealed
that the psoas
muscle
is a lateral
rotator
of the
hip in all positions
but that this secondary
action
is much
stronger
when the limb is abducted.
2. It has also been shown
that the iliacus
portion
of the muscle
can contribute
towards
the
completion
of abduction
3. An attempt
has been
of the
4.
muscle
The
in the
clinical
movement.
made to reconcile
these
with
facts
the
accepted
concept
of the
action
adult.
significance
is discussed.
Grateful
thanks
are extended
to Dr J. L. Emery,
the Department
of Pathology,
Children’s
who kindly provided
the pathological
material,
and to Mr G. E. Swan of the Photographic
Hospital,
Department,
Sheffield,
Royal
London:
Oxford
London:
Oxford
Sheffield.
Infirmary,
REFERENCES
J. V. (1958):
BASMAJIAN,
D.
CUNNINGHAM,
University
Electromyography
of Iliopsoas.
Textbook
J. (1951):
J. (1964):
D.
University
GRANT,
J. C.
B. (1948):
J. C.
B.,
London:
Textbook
A Method
and
ofAnatomy.
J. V. (1965):
BASMAJIAN,
E. & S.
Livingstone
Limited.
GRAY,
H.
(1949):
Gray’s
Anatomy.
Edited
H.
(1962):
Gray’s
Anatomy.
Edited
BRUMLIK,
J., and
R. D.,
Journal
Joint
W.
W.
the Hip.
SOMERVILLE,
50 B,
Record,
Edited
edition.
Edited
Anatomy,
41-B,
J. W.
Journal
E. W.
NO.
Regional
I
,
Follow-up
A
Fourth
edition.
London
Grant’s
Method
ofAnatomy.
by T. B. Johnston
by D. V. Davies
J. J. (1966):
BERGAN,
and Joint
T. (1959):
Surgery,
SHARRARD,
VOL.
ofBone
R. J. (1963):
MUSTARD,
Tenth
ofAnatomy.
GRAY,
LAST,
edition.
132, 127.
by J. C. Brash.
by G. J. Romanes.
Press.
GRANT,
Man.
Ninth
Press.
CUNNINGHAM,
KEAGY,
Anatomical
ofAnatomy.
Surgery,
and
48-A,
Applied.
Study
Direct
Seventh
and J. Whillis.
and F. Davies.
Electromyography
1377.
Third edition.
of Iliopsoas
: Bailli#{232}re,Tindall
Transfer
London
for
Hip
edition.
& Cox.
Edinburgh
London:
Longmans.
London:
Longmans.
of the Psoas Major
: J. & A. Churchill
Instability.
Journal
and
Muscle
in
Ltd.
of Bone
and
289.
(1964):
Posterior
Iliopsoas
of Bone and Joint Surgery,
(1959):
FEBRUARY
Paralytic
1968
Dislocation
Transplantation
in the Treatment
of Paralytic
46-B, 426.
of the Hip. Journal of Bone and Joint Surgery,
Dislocation
41-B,
279.
of